Young Children’s Sugar-Sweetened Beverage Consumption and 5-Year Change in BMI: Lessons Learned from the Timing of Consumption


Abstract
:1. Introduction
2. Materials and Methods
2.1. GECKO Drenthe Birth Cohort and Study Population
2.2. Data Collection
2.2.1. Anthropometrics
2.2.2. Parental Information
2.2.3. Food Pattern Questionnaire
2.3. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. SSB, BMI-z, and Overweight
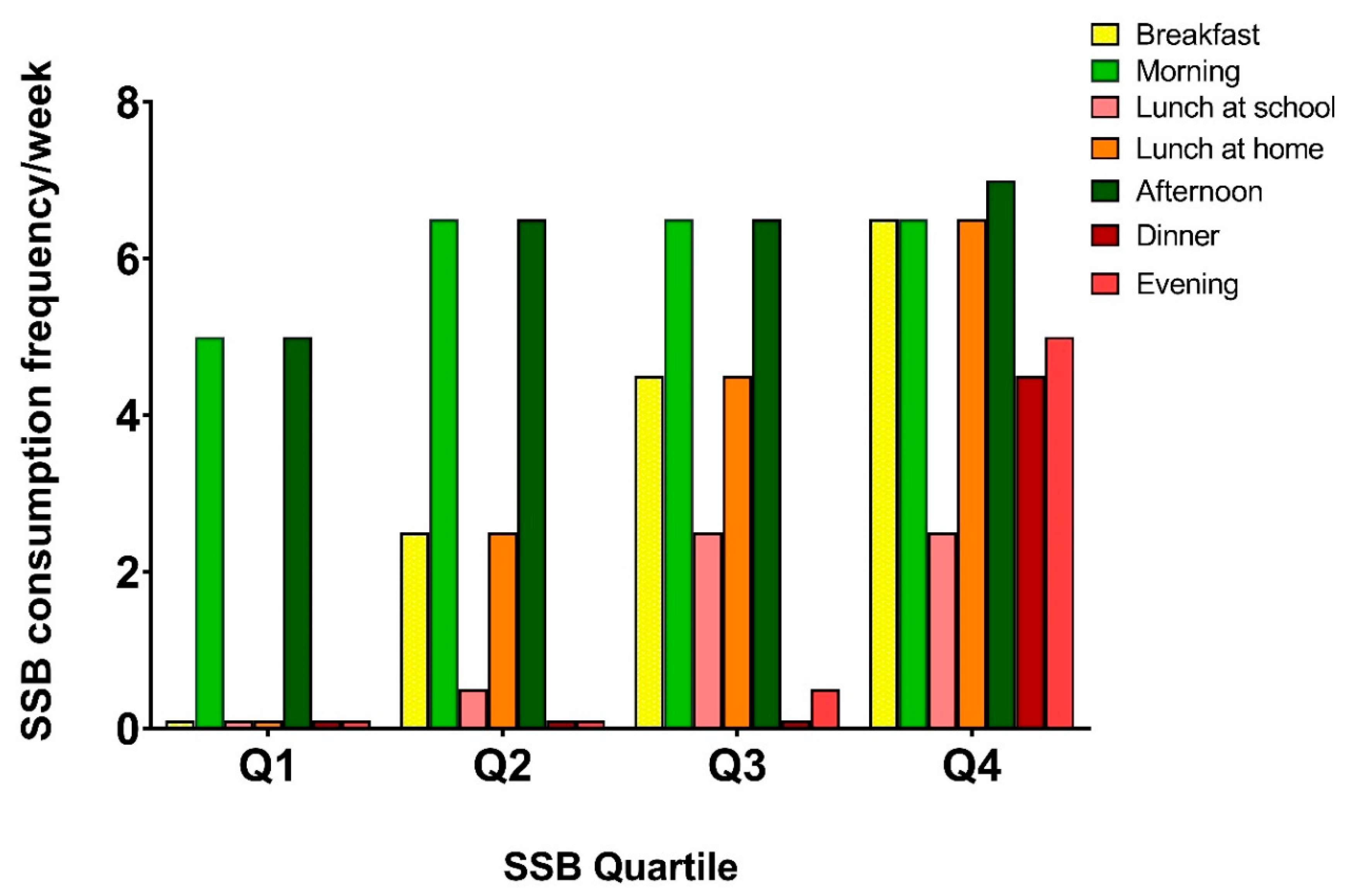
3.3. SSB Consumption Patterns
4. Discussion
5. Conclusions
Implications for Future Research and Policies
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
References
- De Onis, M.; Blössner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [Green Version]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood obesity: Causes, consequences, and management. Pediatr. Clin. 2015, 62, 821–840. [Google Scholar]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-related consequences of childhood obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas-Garcia, E.J.; Evans, C.E.L.; Prestwich, A.; Sykes-Muskett, B.J.; Hooson, J.; Cade, J.E. Interventions to reduce consumption of sugar-sweetened beverages or increase water intake: Evidence from a systematic review and meta-analysis. Obes. Rev. 2017, 18, 1350–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, A.A.; Jomaa, L.; Kahale, L.A.; Adair, P.; Pine, C. Effectiveness of behavioral interventions to reduce the intake of sugar-sweetened beverages in children and adolescents: A systematic review and meta-analysis. Nutr. Rev. 2017, 76, 88–107. [Google Scholar] [CrossRef]
- Dimeglio, D.P.; Mattes, R.D. Liquid versus solid carbohydrate: Effects on food intake and body weight. Int. J. Obes. 2000, 24, 794–800. [Google Scholar] [CrossRef] [Green Version]
- De Graaf, C. Why liquid energy results in overconsumption. Proc. Nutr. Soc. 2011, 70, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.C.; Bleich, S.N.; Gortmaker, S.L. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988–2004. Pediatrics 2008, 121, e1604–e1614. [Google Scholar] [CrossRef]
- van Rossum, C.T.M.; Buurma-Rethans, E.J.M.; Vennemann, F.B.C.; Beukers, M.; Brants, H.A.M.; de Boer, E.J.; Ocké, M.C. The diet of the Dutch: Results of the first two years of the Dutch National Food Consumption Survey 2012–2016. In RIVM Letter Report 2016–0082; Bilthoven: National Institute for Public Health and the Environment: Utrecht, The Netherlands, 2016. [Google Scholar]
- Millar, L.; Rowland, M.; Nichols, B.; Swinburn, C.; Bennett, H.; Skouteris, H.; Allender, S. Relationship between raised BMI and sugar sweetened beverage and high fat food consumption among children. Obesity 2014, 22, 96–103. [Google Scholar] [CrossRef]
- Lim, S.; Zoellner, J.M.; Lee, J.M.; Burt, B.A.; Sandretto, A.M.; Sohn, W.; Ismail, A.I.; Lepkowski, J.M. Obesity and sugar-sweetened beverages in African-American preschool children: A longitudinal study. Obesity 2009, 17, 1262–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBoer, M.D.; Scharf, R.J.; Demmer, R.T. Sugar-sweetened beverages and weight gain in 2-to 5-year-old children. Pediatrics 2013, 132, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ruyter, J.C.; Olthof, M.R.; Seidell, J.C.; Katan, M.B. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N. Engl. J. Med 2012, 367, 1397–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercammen, K.A.; Frelier, J.M.; Lowery, C.M.; McGlone, M.E.; Ebbeling, C.B.; Bleich, S.N. A systematic review of strategies to reduce sugar-sweetened beverage consumption among 0-year to 5-year olds. Obes. Rev. 2018, 19, 1504–1524. [Google Scholar] [CrossRef]
- L’Abée, C.; Sauer, P.J.J.; Damen, M.; Rake, J.P.; Cats, H.; Stolk, R.P. Cohort profile: The GECKO Drenthe study, overweight programming during early childhood. Int. J. Epidemiol. 2008, 37, 486–489. [Google Scholar] [CrossRef] [Green Version]
- de Jong, E.; Visscher, T.L.S.; HiraSing, R.A.; Heymans, M.W.; Seidell, J.C.; Renders, C.M. Association between TV viewing, computer use and overweight, determinants and competing activities of screen time in 4- to 13-year-old children. Int. J. Obes. 2013, 37, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Koning, M.; de Jong, A.; de Jong, E.; Visscher, T.L.S.; Seidell, J.C.; Renders, C.M. Agreement between parent and child report of physical activity, sedentary and dietary behaviours in 9–12-year-old children and associations with children’s weight status. BMC Psychol. 2018, 6, 14. [Google Scholar] [CrossRef]
- World Health Organization, Fact Sheet Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 29 April 2020).
- Fredriks, A.M.; van Buuren, S.; Burgmeijer, R.J.; Meulmeester, J.F.; Beuker, R.J.; Brugman, E.; Roede, M.J.; Verloove-Vanhorick, S.P.; Wit, J.M. Continuing positive secular growth change in the Netherlands 1955–1997. Pediatr. Res. 2000, 47, 316–323. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Carlson, J.A.; Crespo, N.C.; Sallis, J.F.; Patterson, R.E.; Elder, J.P. Dietary-related and physical activity-related predictors of obesity in children: A 2-year prospective study. Child Obes. 2012, 8, 110–115. [Google Scholar] [CrossRef]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Is sugar-sweetened beverage consumption associated with increased fatness in children? Nutrition 2007, 23, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Bucher, D.T.S. Sugar-sweetened beverages and obesity among children and adolescents: A review of systematic literature reviews. Child Obes. 2015, 11, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Dubois, L.; Farmer, A.; Girard, M.; Peterson, K. Regular sugar-sweetened beverage consumption between meals increases risk of overweight among preschool-aged children. J. Am. Diet. Assoc. 2007, 107, 924–934. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Rangan, A.; Allman-Farinelli, M.; Rohde, J.F.; Olsen, N.J.; Heitmann, B.L. Replacing sugary drinks with milk is inversely associated with weight gain among young obesity-predisposed children. Br. J. Nutr. 2015, 114, 1448–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kromhout, D.; Spaaij, C.J.K.; de Goede, J.; Weggemans, R.M. The 2015 Dutch food-based dietary guidelines. Eur. J. Clin. Nutr. 2016, 70, 69–78. [Google Scholar] [CrossRef]
- Patrick, H.; Nicklas, T.A. A review of family and social determinants of children’s eating patterns and diet quality. J. Am. Coll. Nutr. 2005, 24, 82–92. [Google Scholar] [CrossRef]
- Gibbs, H.D.; Kennett, A.R.; Kerling, E.H.; Yu, Q.; Gajewski, B.; Ptomey, L.T.; Sullivan, D.K. Assessing the nutrition literacy of parents and its relationship with child diet quality. J. Nutr. Educ. Behav. 2016, 48, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Blissett, J. Relationships between parenting style, feeding style and feeding practices and fruit and vegetable consumption in early childhood. Appetite 2011, 57, 826–831. [Google Scholar] [CrossRef]
- Katz, D.L.; Katz, C.S.; Treu, J.A.; Reynolds, J.; Njike, V.; Walker, J.; Smith, E.; Michael, J. Teaching healthful food choices to elementary school students and their parents: The Nutrition Detectives™ Program. J. Sch. Health 2011, 81, 21–28. [Google Scholar] [CrossRef]
- von Philipsborn, P.; Stratil, J.M.; Burns, J.; Busert, L.K.; Pfadenhauer, L.M.; Polus, S.; Holzapfel, C.; Hauner, H.; Rehfuess, E. Environmental interventions to reduce the consumption of sugar-sweetened beverages and their effects on health. Cochrane Database Syst. Rev. 2019, 6, CD012292. [Google Scholar] [CrossRef]
- Bartelink, N.H.M.; Van Assema, P.; Kremers, S.P.J.; Savelberg, H.H.C.M.; Oosterhoff, M.; Willeboordse, M. van Schayck O.C.P.; Winkens B.; Jansen M.W.J. Can the Healthy Primary School of the Future offer perspective in the ongoing obesity epidemic in young children? A Dutch quasi-experimental study. BMJ Open 2019, 9, e030676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartelink, N.H.M.; van Assema, P.; Kremers, S.P.J.; Savelberg, H.H.C.M.; Oosterhoff, M.; Willeboordse, M.; van Schayck, O.C.P.; Winkens, B.; Jansen, M.W.J. One- and two-year effects of the healthy primary school of the future on children’s dietary and physical activity behaviours: A quasi-experimental study. Nutrients 2019, 11, 689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.D.; Hou, T.; Hu, F.B.; Rimm, E.B.; Spiegelman, D.; Willett, W.C.; Mozaffarian, D.A. A comparison of different methods for evaluating diet, physical activity, and long-term weight gain in 3 prospective cohort studies. J. Nutr. 2015, 145, 2527–2534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaddoe, V.W.; Mackenbach, J.P.; Moll, H.A.; Steegers, E.A.; Tiemeier, H.; Verhulst, F.C.; Witteman, J.C.M.; Hofman, A. The generation r study: Design and cohort profile. Eur. J. Epidemiol. 2006, 21, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, T.N.; Nohr, E.A.; Frydenberg, M. Selection by socioeconomic factors into the Danish National Birth Cohort. Eur. J. Epidemiol. 2010, 25, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total (N = 1257) | Q1 (N = 313) | Q2 (N = 311) | Q3 (N = 325) | Q4 (N = 308) | p-Value | |
|---|---|---|---|---|---|---|
| Child Characteristics | ||||||
| Gender | 0.499 | |||||
| Boy | 632 (50.3) | 148 (47.3) | 159 (51.1) | 161 (49.5) | 164 (53.2) | |
| Girl | 625 (49.7) | 165 (52.7) | 152 (48.9) | 164 (50.5) | 144 (46.8) | |
| Daily SSB consumption frequency | 3.1 [2.3–4.2] | 1.9 [1.5–2.0] | 2.7 [2.5–2.9] | 3.6 [3.4–3.9] | 4.9 [4.6–5.5] | <0.001 |
| Age at FPQ assessment (years) | 6.0 ± 0.3 | 6.0 ± 0.3 | 6.0 ± 0.3 | 6.0 ± 0.3 | 6.1 ± 0.3 | 0.018 |
| BMI-z score age 5/6 years (SD) | 0.3 ± 0.8 | 0.3 ± 0.8 | 0.2 ± 0.8 | 0.2 ± 0.8 | 0.3 ± 0.9 | 0.412 |
| Age at BMI measurement age 5/6 (years) | 5.8 ± 0.3 | 5.8 ± 0.3 | 5.8 ± 0.3 | 5.8 ± 0.3 | 5.8 ± 0.3 | 0.540 |
| BMI-z score age 10/11 years (SD) | 0.2 ± 1.1 | 0.2 ± 1.0 | 0.2 ± 1.1 | 0.2 ± 1.0 | 0.4 ± 1.1 | 0.249 |
| Age at BMI measurement age 10/11 (years) | 10.6 ± 0.4 | 10.6 ± 0.4 | 10.6 ± 0.4 | 10.6 ± 0.4 | 10.7 ± 0.4 | 0.001 |
| Overweight * prevalence at age 5/6 | 132 (10.5) | 34 (10.9) | 35 (11.3) | 28 (8.6) | 35 (11.4) | 0.622 |
| Overweight * prevalence at age 10/11 | 214 (17.0) | 40 (12.8) | 54 (17.4) | 50 (15.4) | 70 (22.7) | 0.009 |
| Parental Characteristics | ||||||
| Age of father at birth (years) | 34.4 ± 4.7 | 35.0 ± 4.7 | 34.7 ± 4.8 | 34.3 ± 4.8 | 33.8 ± 4.5 | 0.021 |
| Age of mother at birth (years) | 31.6 ± 4.1 | 32.0 ± 4.0 | 31.9 ± 3.9 | 31.6 ± 4.2 | 31.0 ± 4.2 | 0.023 |
| BMI of father at birth (kg/m2) | 25.4 ± 3.2 | 25.4 ± 3.3 | 25.5 ± 3.1 | 25.3 ± 3.2 | 25.7 ± 3.3 | 0.150 |
| BMI of mother at birth (kg/m2) | 24.7 ± 4.7 | 24.3 ± 4.5 | 24.7 ± 4.9 | 25.1 ± 4.8 | 24.8 ± 4.5 | 0.107 |
| Paternal education level | <0.001 | |||||
| Low | 485 (38.6) | 98 (31.3) | 111 (35.7) | 133 (40.9) | 143 (46.4) | |
| Middle | 346 (27.5) | 85 (27.2) | 86 (27.7) | 85 (26.2) | 90 (29.2) | |
| High | 426 (33.9) | 130 (41.5) | 114 (36.7) | 107 (32.9) | 75 (24.4) | |
| Maternal education level | <0.001 | |||||
| Low | 356 (28.3) | 57 (18.2) | 75 (24.1) | 102 (31.4) | 122 (39.6) | |
| Middle | 395 (31.4) | 99 (31.6) | 94 (30.2) | 101 (31.1) | 101 (32.8) | |
| High | 506 (40.3) | 157 (50.2) | 142 (45.7) | 122 (37.5) | 85 (27.6) | |
| Maternal smoking during pregnancy | 155 (12.3) | 25 (8.0) | 30 (9.6) | 42 (12.9) | 58 (18.8) | <0.001 |
| Model | SSB Quartile | β | 95% CI | p-Value |
|---|---|---|---|---|
| 1 | Q2 | 0.155 | 0.042; 0.267 | 0.007 |
| Q3 | 0.098 | −0.013; 0.209 | 0.083 | |
| Q4 | 0.180 | 0.068; 0.293 | 0.002 | |
| 2 | Q2 | 0.149 | 0.037; 0.262 | 0.009 |
| Q3 | 0.094 | −0.017; 0.205 | 0.097 | |
| Q4 | 0.177 | 0.064; 0.290 | 0.002 | |
| 3 | Q2 | 0.122 | 0.014; 0.230 | 0.026 |
| Q3 | 0.065 | −0.042; 0.172 | 0.236 | |
| Q4 | 0.158 | 0.048; 0.267 | 0.005 | |
| 4 | Q2 | 0.122 | 0.014; 0.229 | 0.027 |
| Q3 | 0.066 | −0.041; 0.174 | 0.227 | |
| Q4 | 0.160 | 0.050; 0.271 | 0.004 |
| Model | Q1 | Q2 | Q3 | Q4 | p-Logistic |
|---|---|---|---|---|---|
| 1 | 1 (REF) | 1.95 (1.05; 3.61) | 2.06 (1.13; 3.77) | 2.72 (1.51; 4.92) | 0.012 |
| 2 | 1 (REF) | 2.57 (1.33; 4.98) | 2.34 (1.23; 4.46) | 3.18 (1.68; 6.00) | 0.004 |
| 3 | 1 (REF) | 2.36 (1.20; 4.67) | 2.18 (1.12; 4.23) | 3.14 (1.63; 6.04) | 0.008 |
| 4 | 1 (REF) | 2.30 (1.15; 4.57) | 2.13 (1.09; 4.17) | 3.12 (1.60; 6.07) | 0.010 |
| Q1 | Q2 | Q3 | Q4 | p-Trend | |
|---|---|---|---|---|---|
| Breakfast | 31.3% | 67.2% | 86.8% | 98.1% | <0.001 |
| Morning | 90.4% | 97.7% | 98.8% | 99.4% | <0.001 |
| Lunch at school * | 46.5% | 78.1% | 83.8% | 95.2% | <0.001 |
| Lunch at home | 31.6% | 70.7% | 90.5% | 98.1% | <0.001 |
| Afternoon | 93.6% | 96.8% | 99.4% | 99.7% | <0.001 |
| Dinner | 17.3% | 32.2% | 50.5% | 72.4% | <0.001 |
| Evening | 22.4% | 39.5% | 56.0% | 81.2% | <0.001 |
| Total | 99.0% | 100.0% | 100.0% | 100.0% | 0.030 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinke, P.C.; Blijleven, K.A.; Luitjens, M.H.H.S.; Corpeleijn, E. Young Children’s Sugar-Sweetened Beverage Consumption and 5-Year Change in BMI: Lessons Learned from the Timing of Consumption. Nutrients 2020, 12, 2486. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082486
Vinke PC, Blijleven KA, Luitjens MHHS, Corpeleijn E. Young Children’s Sugar-Sweetened Beverage Consumption and 5-Year Change in BMI: Lessons Learned from the Timing of Consumption. Nutrients. 2020; 12(8):2486. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082486
Chicago/Turabian StyleVinke, Petra C., Karlien A. Blijleven, Milou H. H. S. Luitjens, and Eva Corpeleijn. 2020. "Young Children’s Sugar-Sweetened Beverage Consumption and 5-Year Change in BMI: Lessons Learned from the Timing of Consumption" Nutrients 12, no. 8: 2486. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082486