Reducing the Burden of Anemia and Neural Tube Defects in Low- and Middle-Income Countries: An Analysis to Identify Countries with an Immediate Potential to Benefit from Large-Scale Mandatory Fortification of Wheat Flour and Rice

 , ,
, ,
Abstract
:1. Introduction
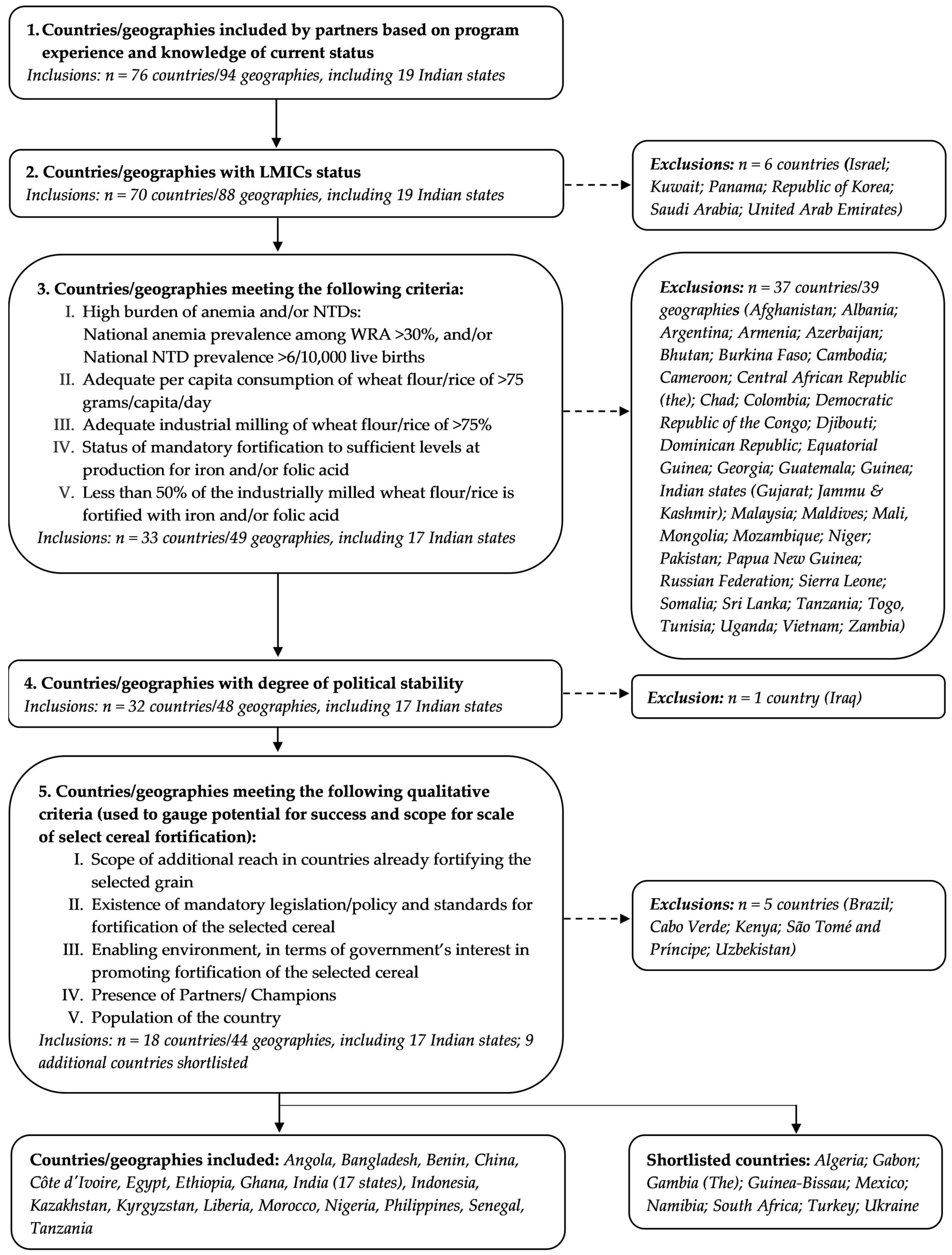
2. Materials and Methods
2.1. Estimation Method for Number of Anemia Cases Prevented in Eligible Countries
2.2. Estimation Method for Number of Folic Acid-Preventable NTDs Prevented and Child Deaths Averted in Eligible Countries:
2.3. Estimation Method for Number of DALYs Averted and the Economic Value of Health Benefits of Fortification at Scale
3. Results
3.1. Number of Cases of Anemia Prevented among WRA
3.2. Number of Cases of NTD Prevented and Under-Five Deaths Averted
3.3. Value of Morbidity and Mortality Averted
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Indian State | People Reached (Millions) | Cases of Anemia in WRA Averted | Cases of NTDs Averted | Child Deaths Averted | DALYs Averted | Economic Value of DALYs Averted (in USD $ m) |
|---|---|---|---|---|---|---|
| Andhra Pradesh | 25.1 | 1,282,143 | 943 | 874 | 100,154 | 260 |
| Assam | 16.4 | 639,396 | 816 | 757 | 72,946 | 172 |
| Bihar | 56.2 | 2,882,247 | 2364 | 2193 | 240,692 | 612 |
| Chhattisgarh | 13.5 | 539,333 | 800 | 742 | 68,509 | 157 |
| Haryana | 13.2 | 702,042 | 617 | 572 | 61,084 | 153 |
| Himachal Pradesh | 3.5 | 158,175 | 117 | 108 | 12,472 | 33 |
| Jharkhand | 17.6 | 975,552 | 806 | 748 | 81,499 | 206 |
| Karnataka | 31.4 | 1,195,893 | 1266 | 1174 | 120,029 | 293 |
| Kerala | 16.8 | 490,413 | 580 | 538 | 54,086 | 131 |
| Madhya Pradesh | 38.8 | 1,732,766 | 1691 | 1569 | 163,140 | 403 |
| Maharashtra | 57.4 | 2,341,889 | 2084 | 1933 | 208,893 | 527 |
| Orissa | 21.6 | 934,548 | 798 | 740 | 80,870 | 205 |
| Punjab | 14.1 | 640,540 | 481 | 446 | 51,056 | 133 |
| Rajasthan | 36.9 | 1,466,494 | 1946 | 1805 | 171,827 | 401 |
| Tamil Nadu | 36.4 | 1,701,949 | 1093 | 1013 | 123,627 | 331 |
| Uttar Pradesh | 107.8 | 4,800,876 | 4085 | 3788 | 413,783 | 1049 |
| West Bengal | 46.4 | 2,465,850 | 1519 | 1409 | 173,436 | 466 |
| TOTAL (17 states) | 553.1 | 24,950,107 | 22,006 | 20,410 | 2,198,103 | 5532 |
| Country/ Region | Monetized DALYs ($ Millions) | ||
|---|---|---|---|
| 0% Discount Rate | 3% Discount Rate | 5% Discount Rate | |
| Angola | 676.75 | 383.2 | 303.4 |
| Bangladesh | 1042.42 | 593.7 | 486.3 |
| Benin | 91.26 | 63.5 | 56.1 |
| China | 29,863.50 | 20,298.0 | 18,150.7 |
| Côte d’Ivoire | 110.28 | 93.4 | 88.6 |
| Egypt | 1284.55 | 699.3 | 559.0 |
| Ethiopia | 214.26 | 140.7 | 121.9 |
| Ghana | 214.88 | 146.7 | 128.7 |
| India (17 states) | 8669.83 | 531.5 | 4756.8 |
| Indonesia | 286.79 | 195.6 | 173.6 |
| Kazakhstan | 430.41 | 370.1 | 356.0 |
| Kyrgyzstan | 20.77 | 17.4 | 16.6 |
| Liberia | 8.68 | 5.6 | 4.8 |
| Morocco | 448.41 | 309.9 | 278.3 |
| Nigeria | 3220.71 | 2363.9 | 2112.4 |
| Philippines | 864.40 | 536.7 | 457.1 |
| Senegal | 79.11 | 64.1 | 60.3 |
| Tajikistan | 34.57 | 28.6 | 27.2 |
| Total | 47.6 B | 31.8 B | 28.1 B |
| Indian State | Monetized DALYs ($ millions) | ||
|---|---|---|---|
| 0% Discount Rate | 3% Discount Rate | 5% Discount Rate | |
| Andhra Pradesh | 394.76 | 260.3 | 227.2 |
| Assam | 288.1 | 171.7 | 142.9 |
| Bihar | 949.14 | 612 | 528.7 |
| Chhattisgarh | 270.73 | 156.7 | 128.6 |
| Haryana | 240.95 | 153 | 131.3 |
| Himachal Pradesh | 49.16 | 32.5 | 28.4 |
| Jharkhand | 321.41 | 206.4 | 178 |
| Karnataka | 473.71 | 293.2 | 248.6 |
| Kerala | 213.5 | 130.8 | 110.3 |
| Madhya Pradesh | 643.72 | 402.5 | 343 |
| Maharashtra | 823.89 | 526.6 | 453.2 |
| Orissa | 318.92 | 205.1 | 177 |
| Punjab | 201.24 | 132.7 | 115.7 |
| Rajasthan | 678.75 | 401.2 | 332.7 |
| Tamil Nadu | 486.96 | 331.1 | 292.6 |
| Uttar Pradesh | 1631.79 | 1049.20 | 905.4 |
| West Bengal | 683.09 | 466.5 | 413 |
| TOTAL | 8.7 B | 5.5 B | 4.8 B |
| Country/Region | Benefit-Cost Ratio | |||||
|---|---|---|---|---|---|---|
| 0% Discount Rate | 3% Discount Rate | 5% Discount Rate | ||||
| At 1× Unit Cost | At 3× Unit Cost | At 1× Unit Cost | At 3× Unit Cost | At 1× Unit Cost | At 3× Unit Cost | |
| Angola | 202.79 | 67.60 | 114.81 | 38.27 | 90.93 | 30.31 |
| Bangladesh | 19.49 | 6.50 | 11.10 | 3.70 | 9.09 | 3.03 |
| Benin | 24.04 | 8.01 | 16.74 | 5.58 | 14.78 | 4.93 |
| China | 62.82 | 20.94 | 42.70 | 14.23 | 38.18 | 12.73 |
| Côte d’Ivoire | 24.32 | 8.11 | 20.60 | 6.87 | 19.54 | 6.51 |
| Egypt | 39.20 | 13.07 | 21.34 | 7.11 | 17.06 | 5.69 |
| Ethiopia | 6.85 | 2.28 | 4.50 | 1.50 | 3.90 | 1.30 |
| Ghana | 28.97 | 9.66 | 19.78 | 6.59 | 17.35 | 5.78 |
| India (17 states) | 42.37 | 14.12 | 27.03 | 9.01 | 23.25 | 7.75 |
| Indonesia | 31.67 | 10.56 | 21.61 | 7.20 | 19.17 | 6.39 |
| Kazakhstan | 70.63 | 23.54 | 60.74 | 20.25 | 58.42 | 19.47 |
| Kyrgyzstan | 9.90 | 3.30 | 8.32 | 2.77 | 7.93 | 2.64 |
| Liberia | 8.43 | 2.81 | 5.46 | 1.82 | 4.68 | 1.56 |
| Morocco | 37.40 | 12.47 | 25.85 | 8.62 | 23.22 | 7.74 |
| Nigeria | 79.57 | 26.52 | 58.40 | 19.47 | 52.19 | 17.40 |
| Philippines | 28.94 | 9.65 | 17.97 | 5.99 | 15.30 | 5.10 |
| Senegal | 15.03 | 5.01 | 12.19 | 4.06 | 11.47 | 3.82 |
| Tajikistan | 11.93 | 3.98 | 9.89 | 3.30 | 9.39 | 3.13 |
| TOTAL | 51.40 | 17.13 | 34.41 | 11.47 | 30.41 | 10.14 |
| MEDIAN | 28.96 | 9.65 | 20.19 | 6.73 | 17.20 | 5.73 |
| RANGE | 6.9–202.8 | 2.3–67.6 | 4.5–114.8 | 1.5–38.3 | 3.9–90.9 | 1.3–30.3 |
| Country/Region | Benefit-Cost Ratio | |||||
|---|---|---|---|---|---|---|
| 0% Discount Rate | 3% Discount Rate | 5% Discount Rate | ||||
| At 1× Unit Cost | At 3× Unit Cost | At 1× Unit Cost | At 3× Unit Cost | At 1× Unit Cost | At 3× Unit Cost | |
| Andhra Pradesh | 42.44 | 14.15 | 27.99 | 9.33 | 24.42 | 8.14 |
| Assam | 47.62 | 15.87 | 28.37 | 9.46 | 23.62 | 7.87 |
| Bihar | 45.62 | 15.21 | 29.41 | 9.8 | 25.41 | 8.47 |
| Chhattisgarh | 54.2 | 18.07 | 31.37 | 10.46 | 25.74 | 8.58 |
| Haryana | 49.44 | 16.48 | 31.4 | 10.47 | 26.94 | 8.98 |
| Himachal Pradesh | 38.2 | 12.73 | 25.27 | 8.42 | 22.08 | 7.36 |
| Jharkhand | 49.35 | 16.45 | 31.69 | 10.56 | 27.33 | 9.11 |
| Karnataka | 40.77 | 13.59 | 25.23 | 8.41 | 21.39 | 7.13 |
| Kerala | 34.3 | 11.43 | 21.01 | 7 | 17.73 | 5.91 |
| Madhya Pradesh | 44.81 | 14.94 | 28.02 | 9.34 | 23.87 | 7.96 |
| Maharashtra | 38.79 | 12.93 | 24.8 | 8.27 | 21.34 | 7.11 |
| Orissa | 39.98 | 13.33 | 25.72 | 8.57 | 22.19 | 7.4 |
| Punjab | 38.61 | 12.87 | 25.45 | 8.48 | 22.2 | 7.4 |
| Rajasthan | 49.76 | 16.59 | 29.41 | 9.8 | 24.39 | 8.13 |
| Tamil Nadu | 36.15 | 12.05 | 24.58 | 8.19 | 21.73 | 7.24 |
| Uttar Pradesh | 40.92 | 13.64 | 26.31 | 8.77 | 22.7 | 7.57 |
| West Bengal | 39.77 | 13.26 | 27.16 | 9.05 | 24.05 | 8.02 |
| TOTAL | 42.37 | 14.12 | 27.03 | 9.01 | 23.25 | 7.75 |
| MEDIAN | 40.92 | 13.64 | 27.16 | 9.05 | 23.62 | 7.87 |
| RANGE | 34.3–54.2 | 11.4–18.1 | 21–31.7 | 7–10.6 | 17.7–27.3 | 5.9–9.1 |
References
- Petry, N.; Olofin, I.; Hurrell, R.F.; Boy, E.; Wirth, J.P.; Moursi, M.; Donahue Angel, M.; Rohner, F. The proportion of anemia associated with iron deficiency in low, medium, and high human development index countries: A systematic analysis of national surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Prevalence of Anaemia in 2011; World Health Organization: Geneva, Switzerland, 2015; Available online: https://www.who.int/nutrition/publications/micronutrients/global_prevalence_anaemia_2011/en/ (accessed on 7 June 2020).
- Blencowe, H.; Kancherla, V.; Moorthie, S.; Darlison, W.; Modell, B. Estimates of global and regional prevalence of neural tube defects for 2015: A systematic analysis. Ann. N. Y. Acad. Sci. 2018, 1414, 31–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botto, L.D.; Moore, C.A.; Khoury, M.J.; Erickson, J.D. Neural-tube defects. N. Engl. J. Med. 1999, 341, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Crider, K.S.; Devine, O.; Hao, L.; Dowling, N.F.; Li, S.; Molloy, A.M.; Li, Z.; Zhu, J.; Berry, R.J. Population red blood cell folate concentrations for prevention of neural tube defects: Bayesian model. BMJ 2014, 349, g4554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horton, S.; Alderman, H.; Rivera, J.A. Copenhagen Consensus 2008 Challenge Paper: Hunger and Malnutrition, Draft. Denmark: Copenhagen Consensus Center. Copenhagen Consensus Center, 2008. Available online: https://www.copenhagenconsensus.com/sites/default/files/CP_Malnutrition_and_Hunger_-_Horton.pdf (accessed on 8 December 2020).
- Keats, E.C.; Neufeld, L.; Garrett, G.S.; Mbuya, M.N.M.; Bhutta, Z.A. Improved micronutrient status and health outcomes in low- and middle-income countries following large-scale fortification: Evidence from a systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 10, 1093–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, L.; de Benoist, B.; Dary, O.; Hurrel, R. (Eds.) Guidelines on Food Fortification with Micronutrients; World Health Organization; Food and Agriculture Organization: Geneva, Switzerland, 2006. [Google Scholar]
- The Food Fortification Initiative. Flour Fortification with Iron, Folic Acid, Vitamin B12, Vitamin A, and Zinc: Proceedings of the Second Technical Workshop on Wheat Flour Fortification; The Food Fortification Initiative: Atlanta, GA, USA, 2018; Available online: https://static1.squarespace.com/static/5e1df234eef02705f5446453/t/5f8dbd4dca01f45f6cc66113/1603124605613/FNB2010.pdf (accessed on 14 January 2021).
- Zimmerman, S.; Baldwin, R.; Codling, K.; Hindle, P.; Montgomery, S.; Pachon, H.; Maberly, G. Mandatory policy: Most successful way to maximize fortification’s effect on vitamin and mineral deficiency. Indian J. Commun. Health 2014, 26, 369–374. [Google Scholar]
- Atta, C.A.; Fiest, K.M.; Frolkis, A.D.; Jette, N.P.T.; St Germaine-Smith, C.; Rajapakse, T.; Kaplan, G.G.; Metcalfe, A. Global birth prevalence of spina bifida by folic acid fortification status: A systematic review and meta-analysis. Am. J. Public Health 2016, 106, e124–e134. [Google Scholar] [CrossRef]
- Global Fortification Data Exchange (GFDx). Available online: https://fortificationdata.org (accessed on 15 June 2020).
- The Food Fortification Initiative: Fortify to Address Sustainable Development Goals. Available online: https://www.ffinetwork.org/world (accessed on 15 June 2020).
- World Health Organization. Number of Countries Categorized by Public Health Significance of Anemia; World Health Organization: Geneva, Switzerland, 2008; Available online: https://www.who.int/vmnis/anaemia/prevalence/anaemia_data_status_t4/en/ (accessed on 7 December 2020).
- World Health Organization: Recommendations on Wheat and Maize Flour Fortification. Available online: https://www.who.int/nutrition/publications/micronutrients/wheat_maize_fort.pdf?ua=1 (accessed on 7 December 2020).
- The Food Fortification Initiative. Country Profiles. Available online: https://www.ffinetwork.org/country-profiles (accessed on 15 June 2020).
- World Health Organization. Maternal, Newborn, Child and Adolescent Health and Ageing; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- UNICEF. State of the World’s Children 2019. Available online: https://www.unicef.org/media/63016/file/SOWC-2019.pdf (accessed on 7 December 2020).
- Castillo-Lancellotti, C.; Tur, J.A.; Uauy, R. Impact of folic acid fortification of flour on neural tube defects: A systematic review. Public Health Nutr. 2013, 16, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Cortes, F.; Mellado, C.; Pardo, R.A.; Villarroel, L.A.; Hertrampf, E. Wheat flour fortification with folic acid: Changes in neural tube defects rates in Chile. Am. J. Med. Genet. A 2012, 158A, 1885–1890. [Google Scholar] [CrossRef] [PubMed]
- De Wals, P.; Tairou, F.; Van Allen, M.I.; Uh, S.H.; Lowry, R.B.; Sibbald, B.; Evans, J.A.; Van den Hof, M.C.; Zimmer, P.; Crowley, M.; et al. Reduction in neural-tube defects after folic acid fortification in Canada. N. Engl. J. Med. 2007, 357, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayed, A.R.; Bourne, D.; Pattinson, R.; Nixon, J.; Henderson, B. Decline in the prevalence of neural tube defects following folic acid fortification and its cost-benefit in South Africa. Birth. Defects Res. A Clin. Mol. Teratol. 2008, 82, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, L.J.; Mai, C.T.; Edmonds, L.D.; Shaw, G.M.; Kirby, R.S.; Hobbs, C.A.; Sever, L.E.; Miller, L.A.; Meaney, F.J.; Levitt, M. Prevalence of spina bifida and anencephaly during the transition to mandatory folic acid fortification in the United States. Teratology 2002, 66, S40–S43. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Disability Weights; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2018; Available online: http://ghdx.healthdata.org/record/ihme-data/gbd-2017-disability-weights (accessed on 15 November 2020).
- World Health Organization. Global Health Observatory Data Repository; Prevalence of Anaemia in Women of Reproductive Age; WHO: Geneva, Switzerland, 2017; Available online: https://apps.who.int/gho/data/view.main.ANAEMIAWOMENPREVANEMIAREG?lang=en. (accessed on 15 November 2020).
- ICF. The DHS Program STATcompiler. Funded by USAID. 2012. Available online: http://www.statcompiler.com (accessed on 15 November 2020).
- Robinson, L.A.; Hammitt, J.K.; Cecchini, M.; Chalkidou, K.; Claxton, K.; Cropper, M.; Eozenou, P.H.; de Ferranti, D.; Deolalikar, A.N.; Guanais, F.; et al. Reference Case Guidelines for Benefit-Cost Analysis in Global Health and Development. Boston 2019. Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/2447/2019/05/BCA-Guidelines-May-2019.pdf (accessed on 7 December 2020).
- Bill and Melinda Gates Foundation and NICE International. Methods for Economic Evaluation Project (MEEP). In The Gates Reference Case. What It Is, Why It’s Important, and How to Use It; National Institute for Clinical Excellence: Abingdon, UK, 2014. [Google Scholar]
- Viscusi, W.K.; Masterman, C.J. Income Elasticities and Global Values of a Statistical Life. J. Benef. Cost Anal. 2017, 8, 226–250. Available online: https://static1.squarespace.com/static/5be33b0efcf7fdd77c7823be/t/5be9f13021c67c13124b3a77/1542058289675/361_Income_Elasticity_of_Global_Values_of_a_Statistical_Life.pdf (accessed on 15 November 2020). [CrossRef] [Green Version]
- Scott, N.; Delport, D.; Hainsworth, S.; Pearson, R.; Morgan, C.; Huang, S.; Akuoku, J.; Piwoz, E.; Shekar, M.; Levin, C.; et al. Ending malnutrition in all its forms requires scaling up proven nutrition interventions and much more: A 129-country analysis. BMC Med. 2020, 18, 356. [Google Scholar] [CrossRef] [PubMed]
- Government of the Federal Democratic Republic of Ethiopia: Assessment of Feasibility and Potential Benefits of Food Fortification in Ethiopia. 2011. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.659.5929&rep=rep1&type=pdf (accessed on 7 December 2020).
- Berihu, B.A.; Welderufael, A.L.; Berhe, Y.; Magana, T.; Mulugeta, A.; Asfaw, S.; Gebreselassie, K. High burden of neural tube defects in Tigray, Northern Ethiopia: Hospital-based study. PLoS ONE 2018, 13, e0206212. [Google Scholar] [CrossRef] [PubMed]
- Horton, S.; Shekar, M.; McDonald, C.; Mahal, A.; Brooks, J.K. Scaling Up Nutrition: What Will It Cost? Directions in Development Series; World Bank: Washington, DC, USA, 2010. [Google Scholar]
- Shekar, M.; Kakietek, J.; Dayton Eberwein, J.; Walters, D. An Investment Framework for Nutrition: Reaching the Global Targets for Stunting, Anemia, Breastfeeding, and Wasting; The World Bank: Washington DC, USA, 2017. [Google Scholar]
- Horton, S.; Mannar, V.; Wesley, A. Micronutrient Fortification (Iron and Salt Iodization) Edited by Copenhagen Consensus. 2008. Available online: https://www.copenhagenconsensus.com/sites/default/files/bpp_fortification.pdf (accessed on 7 December 2020).
- Osendarp, S.J.M.; Martinez, H.; Garrett, G.S.; Neufeld, L.M.; De-Regil, L.M.; Vossenaar, M.; Darnton-Hill, I. Large-scale food fortification and biofortification in low- and middle-income countries: A review of programs, trends, challenges, and evidence gaps. Food Nutr. Bull. 2018, 39, 315–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, H.; Weakland, A.P.; Bailey, L.B.; Botto, L.D.; De-Regil, L.M.; Brown, K. Improving maternal folate status to prevent infant neural tube defects: Working group conclusions and a framework for action. Ann. N. Y. Acad. Sci. 2018, 1414, 5–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| No. | Country | Anemia among WRA and/or NTD Prevalence | Wheat Flour | Rice | |||
|---|---|---|---|---|---|---|---|
| Per Capita Consumption | % Availability of Industrially Milled Grains | Per Capita Consumption | % Availability of Industrially Milled Grains | ||||
| >30% Anemia Prevalence among Nonpregnant WRA | >6 NTDs /10,000 Live Births (LBs) | ≥75 g/c/day | ≥75% (Considering Imports to Be Industrially Milled) | ≥75 g/c/day | ≥75% (Considering Imports to Be Industrially Milled) | ||
| Source: Most recent Demographic Health Surveys/National Micronutrient Surveys/WHO Global Observatory 2016 | Source: Blencowe 2018 estimates (personal communication) | Source: Global Fortification Data Exchange (GFDx) | Source: FFI Country Profile January 2020 | Source: Global Fortification Data Exchange (GFDx) | Source: FFI Country Profile January 2020 | ||
| 1 | Angola | 47.7% | 15.3 | 112 | 100% | ||
| 2 | Bangladesh | 26% | 32.0 | 48 | 73% ** | 470 | 60% ** |
| 3 | Benin | 57.7% | 15.3 | 146 | 83% | ||
| 4 | China | 26.4% | 19.4 | 174 | 89% | 214 | 90% |
| 5 | Côte d’Ivoire | 53.7% | 9.9 | 174 | 30% ** | ||
| 6 | Egypt | 25.2% | 17.5 | 402 | 100% | ||
| 7 | Ethiopia | 23.6% | 15.3 | 86 | 55% ** | ||
| 8 | Ghana | 42.4% | 15.3 | 88 | 53% ** | ||
| 9 | India (17 states) * | 53.1% | 30.0 | 140 | * | 184 | * |
| 10 | Indonesia | 26% | 13.1 | 70 ** | 100% | ||
| 11 | Kazakhstan | 30.7% | 9.9 | 253 | 100% | ||
| 12 | Kyrgyzstan | 35.2% | 9.9 | 354 | 85% | ||
| 13 | Liberia | 44.5% | 15.3 | 260 | 49% ** | ||
| 14 | Morocco | 36.9% | 17.5 | 492 | 100% | ||
| 15 | Nigeria | 57.8% | 15.3 | 77 | 47% ** | ||
| 16 | Philippines | 11.8% | 13.1 | 63 ** | 100% | ||
| 17 | Senegal | 54.1% | 9.9 | 198 | 68% ** | ||
| 18 | Tajikistan | 41.1% | 9.9 | 358 | 60% ** | ||
| A. Strong political will and/or reach opportunity | |
| Bangladesh and India | The governments of Bangladesh and India have demonstrated strong political will for fortification through the adoption of voluntary fortification of wheat flour and rice, and the countries are committed to the integration of these fortified vehicles into national social safety net programs. This presents an immediate opportunity to reach the most vulnerable populations at scale. India has the largest number of pregnancies in the world affected by NTDs and presents an opportunity to reach 400 million people with fortified wheat flour/rice. |
| China | 330,000 pregnancies are affected by NTDs each year; this is 13% of the global total and second only to India in the number of pregnancies affected [3]. With such a significant burden, there is high potential in China to prevent NTDs through folic acid fortification. |
| Côte d’Ivoire | The government is leading the way in the West Africa region by considering the introduction and scale-up of rice fortification, including fortification of imported rice that constitutes ~30% of total rice available for consumption [16]. |
| Egypt | Egypt is yet another case exhibiting strong political support and potential for expansive reach. The government is currently working to restart the country’s social safety net wheat flour fortification program with interest in expanding it into the open market. Fortified wheat flour provided through the social safety net program alone would reach over 73 million vulnerable people. If fortified wheat flour was provided through both the social safety net program and the open market, 90% of the population would be reached (Food Fortification Initiative, personal communication). |
| Ethiopia | Although only 55% of Ethiopia’s wheat flour is milled industrially and the coverage of fortifiable wheat flour in Ethiopia is only 28% [31], this country was included due to the relatively large population of Ethiopia (104.9 million) and high rate of NTDs (130 per 10,000 births) [32]. Coverage of only 28% in this country means that almost 30 million people can be reached with fortified foods. Additionally, the government has adopted voluntary fortification of wheat flour, exhibiting strong political will to address micronutrient deficiencies through fortification. Lastly, there are multiple champions to support fortification of wheat flour with folic acid in the country. |
| B. Opportunity for fortifying imports | |
| Angola Bangladesh Benin Côte d’Ivoire Ghana Indonesia Liberia Philippines Senegal | Imported wheat flour and/or rice remain a dominant staple, presenting an opportunity for feasible and effective grain fortification in half of the eligible countries (9 out of 18). By mandating fortification of imported wheat flour/rice, these countries could reap large public health benefits while facilitating an enabling environment for other countries in the region seeking similar mandates. A considerable proportion of wheat flour that is available for consumption is imported in Angola (>90%), Philippines, (>90%), Indonesia (>90%), and Bangladesh (>70%). The same holds true for rice in Benin (>90%), Senegal (>70%), Côte d’Ivoire (>50%), Ghana (>50%), and Liberia (>50%). |
| Nigeria | Nigeria consumes more rice than any other country in Africa and, although only ~37% of the rice available for consumption is imported [16], the large population (190.8 million), high burden of anemia among women of reproductive age (47%), and high prevalence of neural tube defects (15/10,000 live births) make it a tremendous opportunity for rice fortification. |
| C. Support required due to technical limitations and constrained resources (market, economic, and behavior) | |
| KazakhstanKyrgyzstanMoroccoPhilippinesTajikistan | Kazakhstan, Kyrgyzstan, Morocco, Philippines, and Tajikistan have all expressed strong political will by legislating fortification of wheat flour. While Tajikistan is the newest country to legislate wheat flour fortification in 2018 and would benefit from support, suboptimal implementation of the legislation in Kazakhstan, Kyrgyzstan, Morocco, and the Philippines is hindering the achievement of optimal health impact in these countries. Support for the industry to adequately fortify wheat flour and for the government to enforce monitoring and compliance to the national fortification standards in these countries will go a long way in ensuring a sustainable wheat flour fortification intervention. In the Philippines, simply adding folic acid to the already-existing wheat flour/rice fortification standards and enforcing its implementation will help the country address the high burden of NTDs. |
| No. | Eligible Country | Wheat Flour Fortification | |||||
|---|---|---|---|---|---|---|---|
| Legislation | Iron | Folic Acid (ppm) | |||||
| Level (ppm) | Compound Indicated in Standard | Level (ppm) as Per Global Recommendation for Country’s Cereal Grain Consumption | Level (ppm) | Level (ppm) as Per Global Recommendation for Country’s Cereal Grain Consumption | |||
| 1 | Angola * | Unknown | No fortification standard | 40 as NaFeEDTA *** 60 as FF/FS *** | No fortification standard | 2.6 | |
| 2 | Bangladesh ** | Unknown | 55 | Not specified | 40 as NaFeEDTA *** 60 as FF/FS *** | 2 | 5 |
| 3 | China * | Voluntary 2012 | 20 | No information | 20 as NaFeEDTA *** 30 as FF/FS *** 60 as EI *** | 2 | 1.3 |
| 4 | Egypt * | Unknown | No fortification standard | 15 as NaFeEDTA *** 20 as FF/FS *** 40 as EI *** | No fortification standard | 1 | |
| 5 | Ethiopia ** | Voluntary 2017 | 30 40 | NaFeEDTA *** FF *** | 40 as NaFeEDTA *** 60 as FF/FS *** | 2 | 2.6 |
| 6 | India (6 states) **# | Voluntary 2018 | 14–21.25 28–42.5 | NaFeEDTA *** FS/FF/EI/FC/FP/FB/FL *** | 20 as NaFeEDTA *** | 0.075-0.125 | 1.3 |
| 7 | Indonesia ** | Mandatory 2001 | 50 | NaFeEDTA/FF/FS *** | 40 as NaFeEDTA *** 60 as FF/FS *** | 2 | 5 |
| 8 | Kazakhstan * | Mandatory 2005 | 55 | - | 20 as NaFeEDTA *** 30 as FF/FS *** 60 as EI *** | 1.4 | 1.3 |
| 9 | Kyrgyzstan * | Mandatory 2009 | No fortification standard | 15 as NaFeEDTA *** 20 as FF/FS *** 40 as EI *** | No fortification standard | 1 | |
| 10 | Morocco * | Mandatory 2005 | 45 | No information | 15 as NaFeEDTA *** 20 as FF/FS *** 40 as EI *** | 1.53 | 1 |
| 11 | Philippines * | Mandatory 2000 | 87.5 | No information | 40 as NaFeEDTA *** 60 as FF/FS *** | 0 | 5 |
| 12 | Tajikistan * | Mandatory 2019 | No fortification standard | 15 as NaFeEDTA *** 20 as FF/FS *** 40 as EI *** | No fortification standard | 1 | |
| No. | Eligible Country | Rice Fortification | |||||
|---|---|---|---|---|---|---|---|
| Legislation | Iron | Folic Acid (ppm) | |||||
| Level (ppm) | Compound Indicated in Standard | Level (ppm) as Per Global Recommendation for Country’s Cereal Grain Consumption | Level (ppm) | Level (ppm) as Per Global Recommendation for Country’s Cereal Grain Consumption | |||
| 1 | Bangladesh ** | Voluntary 2015 | 60 | Micronized ferric pyrophosphate | 70 as micronized ferric pyrophosphate | 1.7 | 1 |
| 2 | Benin * | None | No fortification standard | 120 as micronized ferric pyrophosphate | No fortification standard | 2.6 | |
| 3 | China * | None | No fortification standard | 70 as micronized ferric pyrophosphate | No fortification standard | 1.3 | |
| 4 | Côte d’Ivoire | None | No fortification standard | 70 as micronized ferric pyrophosphate | No fortification standard | 1.3 | |
| 5 | Ghana * | None | No fortification standard | 120 as micronized ferric pyrophosphate | No fortification standard | 2.6 | |
| 6 | India (11 states) # | Voluntary 2018 | 28–42.5 14–21.25 | Ferric pyrophosphateNaFeEDTA | 70 as micronized ferric pyrophosphate | 0.075–0.125 | 1.3 |
| 7 | Liberia * | None | No fortification standard | 70 as micronized ferric pyrophosphate | No fortification standard | 1.3 | |
| 8 | Nigeria * | None | No fortification standard | 120 as micronized ferric pyrophosphate | No fortification standard | 2.6 | |
| 9 | Senegal ** | None | No fortification standard | 70 as micronized ferric pyrophosphate | No fortification standard | 1.3 | |
| No. | Eligible Country | Wheat Flour | Rice | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Proportion of Industrially Milled Wheat Flour Available Post Harvest/Processing Available for consumption (%)—To Achieve Scale | Total Industrially Milled Wheat Flour Available Post Harvest/Processing Available for Consumption (MT) | Proportion of Industrially Milled Wheat Flour Available That Is Already Fortified (%) | Total Industrially Milled Wheat Flour Available That Is Already Fortified (MT) | Proportion of Industrially Milled Wheat Flour Available with Potential to be Fortified (%) | Total Industrially Milled Wheat Flour Available with Potential to be Fortified (MT) | Proportion of Industrially Milled Rice Available Post Harvest/Processing Available for Consumption (%)—To Achieve Scale | Total Industrially Milled Rice Available Post Harvest/Processing Available for Consumption (MT) | Proportion of Industrially Milled rice Available That Is Already Fortified (%) | Total Industrially Milled Rice Available That Is Already Fortified (MT) | Proportion of Industrially Milled Rice Available with Potential to be Fortified (%) | Total Industrially Milled Rice Available with Potential to be Fortified (MT) | ||
| 1 | Angola | 70% | 368,972 | 0% | - | 70% | 368,972 | ||||||
| 2 | Bangladesh | 55% | 2,559,890 | 0.5% | 25,599 | 54.5% | 2,534,291 | * | 750,000 | 2% | 15,000 | * | 735,000 |
| 3 | Benin | 97% | 1,374,002 | 0% | - | 97% | 1,374,002 | ||||||
| 4 | China | 63% | 80,697,739 | 1% | 806,977 | 62% | 79,890,761 | 90% | 113,060,636 | 0% | - | 90% | 113,060,636 |
| 5 | Côte d’Ivoire | 40% | 779,045 | 0% | - | 40% | 779,045 | ||||||
| 6 | Egypt | 70% | 13,782,824 | 0% | - | 70% | 13,782,824 | ||||||
| 7 | Ethiopia | 48% | 2,654,994 | 0% | - | 48% | 2,654,994 | ||||||
| 8 | Ghana | 65% | 644,328 | 0% | - | 65% | 644,328 | ||||||
| 9 | India (17 states) | * | 12,853,149 | 0% | - | * | 12,853,149 | * | 20,330,033 | 0% | - | * | 20,330,033 |
| 10 | Indonesia | 70% | 4,813,060 | 61% | 4,187,362 | 9% | 625,698 | ||||||
| 11 | Kazakhstan | 70% | 4,943,239 | 29% | 2,026,728 | 41% | 2,916,511 | ||||||
| 12 | Kyrgyzstan | 63% | 838,878 | 4% | 58,721 | 59% | 780,157 | ||||||
| 13 | Liberia | 62% | 264,208 | 0% | - | 62% | 264,208 | ||||||
| 14 | Morocco | 70% | 6,656,713 | 0% | - | 70% | 6,656,713 | ||||||
| 15 | Nigeria | 54% | 3,076,626 | 0% | - | 54% | 3,076,626 | ||||||
| 16 | Philippines | 70% | 1,857,509 | 0% | - | 70% | 1,857,509 | ||||||
| 17 | Senegal | 80% | 1,035,376 | 0% | - | 80% | 1,035,376 | ||||||
| 18 | Tajikistan | 56% | 1,023,695 | 0% | - | 56% | 1,023,695 | ||||||
| Total | 133,050,662 | 7,105,387 | 125,945,275 | 141,314,254 | 15,000 | 141,299,254 | |||||||
| Country | Number of People Reached (Millions) | Cases of Anemia in WRA Averted | Cases of NTDs Averted | Child Deaths Averted | DALYs Averted | Economic Value of DALYs Averted (in Millions of USD) |
|---|---|---|---|---|---|---|
| Angola | 9.0 | 365,698 | 816 | 769 | 57,522 | 383 |
| Bangladesh | 144.6 | 3,194,605 | 4154 | 3857 | 369,392 | 594 |
| Benin | 10.3 | 503,202 | 375 | 354 | 38,998 | 64 |
| China | 1284.8 | 28,831,810 | 14,037 | 11,681 | 1,701,396 | 20,298 |
| Côte d’Ivoire | 12.3 | 559,521 | 142 | 134 | 26,294 | 93 |
| Egypt | 88.6 | 1,896,955 | 2077 | 1783 | 161,352 | 699 |
| Ethiopia | 84.5 | 1,695,531 | 1397 | 1315 | 140,088 | 141 |
| Ghana | 20.0 | 722,468 | 531 | 499 | 54,008 | 147 |
| India (17 states) | 553.1 | 24,950,107 | 22,006 | 20,410 | 2,198,103 | 5532 |
| Indonesia | 24.5 | 540,840 | 312 | 274 | 35,071 | 196 |
| Kazakhstan | 16.5 | 429,785 | 62 | 53 | 16,768 | 370 |
| Kyrgyzstan | 5.7 | 169,646 | 36 | 29 | 7666 | 17 |
| Liberia | 2.8 | 105,235 | 92 | 87 | 8555 | 6 |
| Morocco | 32.4 | 1,016,226 | 547 | 454 | 66,193 | 310 |
| Nigeria | 109.4 | 5,374,530 | 3731 | 3519 | 362,564 | 2364 |
| Philippines | 80.7 | 809,657 | 1089 | 954 | 102,517 | 537 |
| Senegal | 14.2 | 653,907 | 171 | 161 | 32,183 | 64 |
| Tajikistan | 7.8 | 273,501 | 61 | 47 | 11,371 | 29 |
| Total | 2.5 B | 72.1 M | 51,636 | 46,378 | 5.4 M | 31.84 B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kancherla, V.; Chadha, M.; Rowe, L.; Thompson, A.; Jain, S.; Walters, D.; Martinez, H. Reducing the Burden of Anemia and Neural Tube Defects in Low- and Middle-Income Countries: An Analysis to Identify Countries with an Immediate Potential to Benefit from Large-Scale Mandatory Fortification of Wheat Flour and Rice. Nutrients 2021, 13, 244. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010244
Kancherla V, Chadha M, Rowe L, Thompson A, Jain S, Walters D, Martinez H. Reducing the Burden of Anemia and Neural Tube Defects in Low- and Middle-Income Countries: An Analysis to Identify Countries with an Immediate Potential to Benefit from Large-Scale Mandatory Fortification of Wheat Flour and Rice. Nutrients. 2021; 13(1):244. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010244
Chicago/Turabian StyleKancherla, Vijaya, Manpreet Chadha, Laura Rowe, Andrew Thompson, Sakshi Jain, Dylan Walters, and Homero Martinez. 2021. "Reducing the Burden of Anemia and Neural Tube Defects in Low- and Middle-Income Countries: An Analysis to Identify Countries with an Immediate Potential to Benefit from Large-Scale Mandatory Fortification of Wheat Flour and Rice" Nutrients 13, no. 1: 244. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010244