Association of Testosterone-Related Dietary Pattern with Testicular Function among Adult Men: A Cross-Sectional Health Screening Study in Taiwan

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants Recruitments
2.2. Clinical and Biochemical Data Measurements
2.3. Dietary Pattern Assessments and Other Covariates
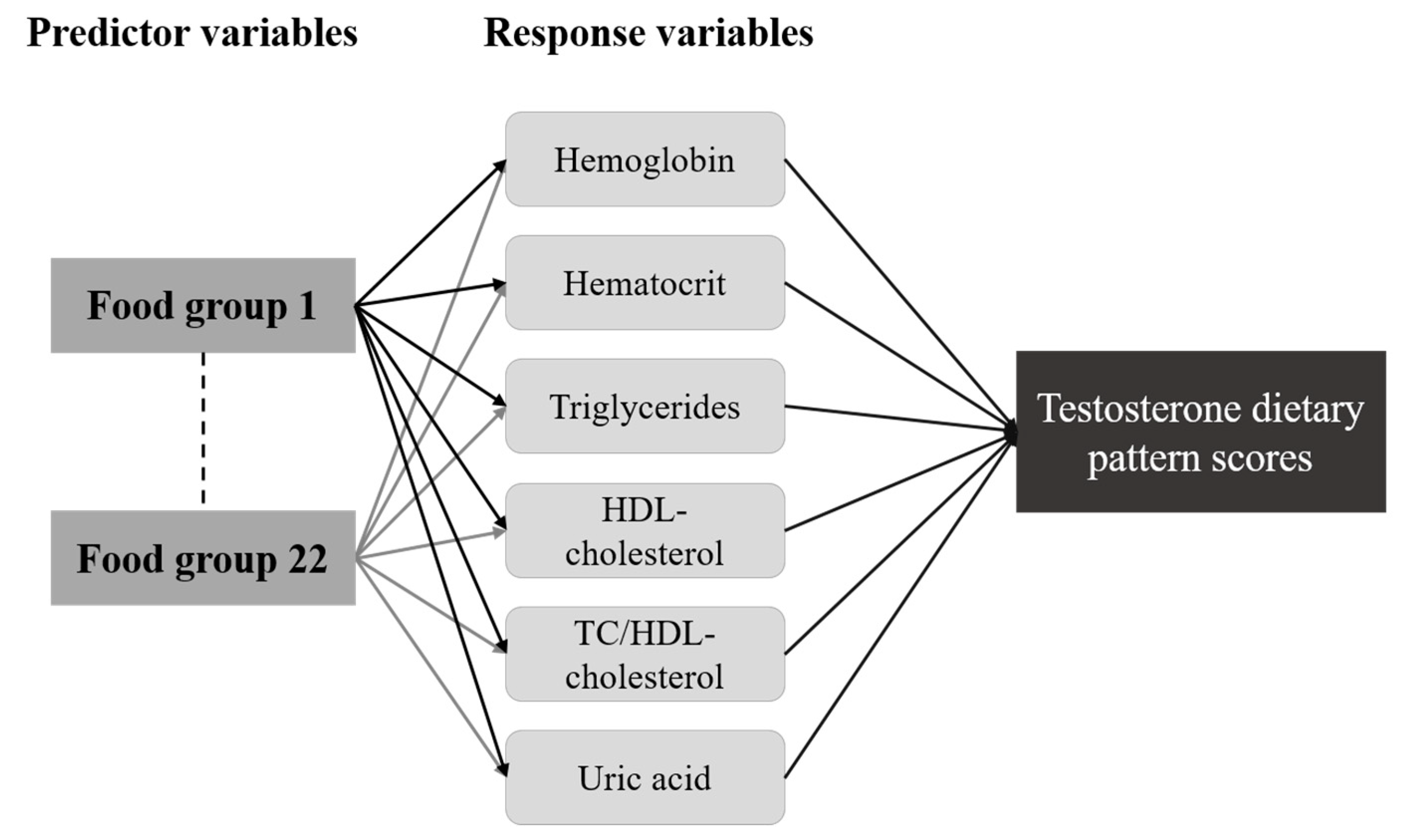
2.4. Data Analysis
3. Results
3.1. Characteristics of Study Participants According to Nutritional Status
3.2. Association of Serum Testosterone with Selected Biochemical Data
3.3. Testosterone-Related Dietary Pattern
3.4. Association of Dietary Pattern with Sex Hormone and Sperm Parameters in Men
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amory, J.K.; Bremner, W.J. Regulation of testicular function in men: Implications for male hormonal contraceptive development. J. Steroid Biochem. 2003, 85, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Pantalone, K.M.; Faiman, C. Male hypogonadism: More than just a low testosterone. Clevel. Clin. J. Med. 2012, 79, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Tilbrook, A.J.; Clarke, I.J. Negative feedback regulation of the secretion and actions of gonadotropin-releasing hormone in males. Biol. Reprod. 2001, 64, 735–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, L.; Stanton, P.; de Kretser, D.M. Endocrinology of the male reproductive system and spermatogenesis. In Endotext [Internet]; MDText. com, Inc.: South Dartmouth, MA, USA, 2017. [Google Scholar]
- Levine, H.; Jorgensen, N.; Martino-Andrade, A.; Mendiola, J.; Weksler-Derri, D.; Mindlis, I.; Pinotti, R.; Swan, S.H. Temporal trends in sperm count: A systematic review and meta-regression analysis. Hum. Reprod. Update 2017, 23, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.C.; Tajar, A.; Pye, S.R.; Silman, A.J.; Finn, J.D.; O’Neill, T.W.; Bartfai, G.; Casanueva, F.; Forti, G.; Giwercman, A.; et al. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: The European Male Aging Study. J. Clin. Endocrinol. Metab. 2008, 93, 2737–2745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Y.F.; Feng, Q.; Ge, Z.Y.; Guo, Y.; Zhou, F.; Zhang, K.S.; Wang, X.W.; Lu, W.H.; Liang, X.W.; Gu, Y.Q. Obesity impairs male fertility through long- term effects on spermatogenesis. BMC Urol. 2018, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, T.K.; Gottschau, M.; Madsen, J.O.B.; Andersson, A.M.; Lassen, T.H.; Skakkebaek, N.E.; Swan, S.H.; Priskorn, L.; Juul, A.; Jorgensen, N. Habitual alcohol consumption associated with reduced semen quality and changes in reproductive hormones; a cross-sectional study among 1221 young Danish men. BMJ Open 2014, 4. [Google Scholar] [CrossRef]
- Bundhun, P.K.; Janoo, G.; Bhurtu, A.; Teeluck, A.R.; Soogund, M.Z.S.; Pursun, M.; Huang, F. Tobacco smoking and semen quality in infertile males: A systematic review and meta-analysis. BMC Public Health 2019, 19. [Google Scholar] [CrossRef]
- Danielewicz, A.; Morze, J.; Przybylowicz, M.; Przybylowicz, K.E. Association of the Dietary Approaches to Stop Hypertension, Physical Activity, and Their Combination with Semen Quality: A Cross-Sectional Study. Nutrients 2020, 12, 39. [Google Scholar] [CrossRef] [Green Version]
- Nassan, F.L.; Jensen, T.K.; Priskorn, L.; Halldorsson, T.I.; Chavarro, J.E.; Jorgensen, N. Association of Dietary Patterns With Testicular Function in Young Danish Men. JAMA Netw. Open 2020, 3. [Google Scholar] [CrossRef] [Green Version]
- Jurewicz, J.; Radwan, M.; Sobala, W.; Radwan, P.; Bochenek, M.; Hanke, W. Dietary Patterns and Their Relationship With Semen Quality. Am. J. Mens Health 2018, 12, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Salas-Huetos, A.; Bullo, M.; Salas-Salvado, J. Dietary patterns, foods and nutrients in male fertility parameters and fecundability: A systematic review of observational studies. Hum. Reprod. Update 2017, 23, 371–389. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Schulze, M.B. Evaluating dietary patterns: The role of reduced rank regression. Curr. Opin. Clin. Nutr. 2016, 19, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Department of Health Executive Yuan (Taiwan). Identification, Evaluation, and Treatment of Overweight and Obesity in Adults in Taiwan; Department of Health Executive Yuan: Taipei, Taiwan, 2003.
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Muga, M.A.; Owili, P.O.; Hsu, C.Y.; Rau, H.H.; Chao, J.C.J. Association between Dietary Patterns and Cardiovascular Risk Factors among Middle-Aged and Elderly Adults in Taiwan: A Population-Based Study from 2003 to 2012. PLoS ONE 2016, 11, e0157745. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, K.; Schulze, M.B.; Schienkiewitz, A.; Nothlings, U.; Boeing, H. Application of a new statistical method to derive dietary patterns in nutritional epidemiology. Am. J. Epidemiol. 2004, 159, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Paduch, D.A.; Brannigan, R.E.; Fuchs, E.F.; Kim, E.D.; Marmar, J.L.; Sandlow, J.I. The laboratory diagnosis of testosterone deficiency. Urology 2014, 83, 980–988. [Google Scholar] [CrossRef]
- Bachman, E.; Travison, T.G.; Basaria, S.; Davda, M.N.; Guo, W.; Li, M.; Connor Westfall, J.; Bae, H.; Gordeuk, V.; Bhasin, S. Testosterone induces erythrocytosis via increased erythropoietin and suppressed hepcidin: Evidence for a new erythropoietin/hemoglobin set point. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 725–735. [Google Scholar] [CrossRef]
- Roy, C.N.; Snyder, P.J.; Stephens-Shields, A.J.; Artz, A.S.; Bhasin, S.; Cohen, H.J.; Farrar, J.T.; Gill, T.M.; Zeldow, B.; Cella, D.; et al. Association of Testosterone Levels With Anemia in Older Men: A Controlled Clinical Trial. JAMA Intern. Med. 2017, 177, 480–490. [Google Scholar] [CrossRef]
- Shin, Y.S.; You, J.H.; Cha, J.S.; Park, J.K. The relationship between serum total testosterone and free testosterone levels with serum hemoglobin and hematocrit levels: A study in 1221 men. Aging Male 2016, 19, 209–214. [Google Scholar] [CrossRef]
- Chung, T.H.; Kwon, Y.J.; Lee, Y.J. High triglyceride to HDL cholesterol ratio is associated with low testosterone and sex hormone-binding globulin levels in Middle-aged and elderly men. Aging Male 2020, 23, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Grosman, H.; Rosales, M.; Fabre, B.; Nolazco, C.; Mazza, O.; Berg, G.; Mesch, V. Association between testosterone levels and the metabolic syndrome in adult men. Aging Male 2014, 17, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Yassin, A.; Haider, A.; Haider, K.S.; Caliber, M.; Doros, G.; Saad, F.; Garvey, W.T. Testosterone Therapy in Men With Hypogonadism Prevents Progression From Prediabetes to Type 2 Diabetes: Eight-Year Data From a Registry Study. Diabetes Care 2019, 42, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.M.; Kelly, D.M.; Jones, T.H. Testosterone and insulin resistance in the metabolic syndrome and T2DM in men. Nat. Rev. Endocrinol. 2013, 9, 479–493. [Google Scholar] [CrossRef]
- Wan, H.; Zhang, K.; Wang, Y.Y.; Chen, Y.; Zhang, W.; Xia, F.Z.; Zhang, Y.P.; Wang, N.J.; Lu, Y.L. The Associations Between Gonadal Hormones and Serum Uric Acid Levels in Men and Postmenopausal Women with Diabetes. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, F.B.; Jiang, B.R.; Cang, Z.; Wang, N.J.; Han, B.; Li, Q.; Chen, Y.; Chen, Y.C.; Xia, F.Z.; Zhai, H.L.; et al. Serum Uric Acid Is Associated with Erectile Dysfunction: A Population-Based Cross-Sectional Study in Chinese Men. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, W.; Zheng, R.D.; Xu, S.H.; Fan, Y.F.; Sun, H.P.; Liu, C. Association between Sex Hormone and Blood Uric Acid in Male Patients with Type 2 Diabetes. Int. J. Endocrinol. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.Y.; Chou, Y.C.; Chao, J.C.J.; Hsu, C.Y.; Cha, T.L.; Tsao, C.W. The Association between Dietary Patterns and Semen Quality in a General Asian Population of 7282 Males. PLoS ONE 2015, 10, e0134224. [Google Scholar] [CrossRef]
- Schulze, M.B.; Martinez-Gonzalez, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food based dietary patterns and chronic disease prevention. BMJ Brit. Med. J. 2018, 361. [Google Scholar] [CrossRef] [Green Version]
- Afeiche, M.; Williams, P.L.; Mendiola, J.; Gaskins, A.J.; Jorgensen, N.; Swan, S.H.; Chavarro, J.E. Dairy food intake in relation to semen quality and reproductive hormone levels among physically active young men. Hum. Reprod. 2013, 28, 2265–2275. [Google Scholar] [CrossRef]
- Afeiche, M.C.; Bridges, N.D.; Williams, P.L.; Gaskins, A.J.; Tanrikut, C.; Petrozza, J.C.; Hauser, R.; Chavarro, J.E. Dairy intake and semen quality among men attending a fertility clinic. Fertil. Steril. 2014, 101, 1280–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giahi, L.; Mohammadmoradi, S.; Javidan, A.; Sadeghi, M.R. Nutritional modifications in male infertility: A systematic review covering 2 decades. Nutr. Rev. 2016, 74, 118–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afeiche, M.C.; Williams, P.L.; Gaskins, A.J.; Mendiola, J.; Jorgensen, N.; Swan, S.H.; Chavarro, J.E. Meat Intake and Reproductive Parameters Among Young Men. Epidemiology 2014, 25, 323–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afeiche, M.C.; Gaskins, A.J.; Williams, P.L.; Toth, T.L.; Wright, D.L.; Tanrikut, C.; Hauser, R.; Chavarro, J.E. Processed Meat Intake Is Unfavorably and Fish Intake Favorably Associated with Semen Quality Indicators among Men Attending a Fertility Clinic. J. Nutr. 2014, 144, 1091–1098. [Google Scholar] [CrossRef]
- Morgan, D.H.; Ghribi, O.; Hui, L.; Geiger, J.D.; Chen, X.S. Cholesterol-enriched diet disrupts the blood-testis barrier in rabbits. Am. J. Physiol. Endocrinol. Metab. 2014, 307, E1125–E1130. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Yan, M.; Cao, Z.; Li, X.; Zhang, Y.; Shi, J.; Feng, G.H.; Peng, H.; Zhang, X.; Zhang, Y.; et al. Sperm tsRNAs contribute to intergenerational inheritance of an acquired metabolic disorder. Science 2016, 351, 397–400. [Google Scholar] [CrossRef] [Green Version]
- Natt, D.; Kugelberg, U.; Casas, E.; Nedstrand, E.; Zalavary, S.; Henriksson, P.; Nijm, C.; Jaderquist, J.; Sandborg, J.; Flinke, E.; et al. Human sperm displays rapid responses to diet. PLoS Biol. 2019, 17, e3000559. [Google Scholar] [CrossRef] [Green Version]
- Nassan, F.L.; Chavarro, J.F.; Tanrikut, C. Diet and men’s fertility: Does diet affect sperm quality? Fertil. Steril. 2018, 110, 570–577. [Google Scholar] [CrossRef] [Green Version]
- Oostingh, E.C.; Steegers-Theunissen, R.P.M.; de Vries, J.H.M.; Laven, J.S.E.; Koster, M.P.H. Strong adherence to a healthy dietary pattern is associated with better semen quality, especially in men with poor semen quality. Fertil. Steril. 2017, 107. [Google Scholar] [CrossRef] [Green Version]
- Chavarro, J.E.; Toth, T.L.; Sadio, S.M.; Hauser, R. Soy food and isoflavone intake in relation to semen quality parameters among men from an infertility clinic. Hum. Reprod. 2008, 23, 2584–2590. [Google Scholar] [CrossRef]
- Beaton, L.K.; McVeigh, B.L.; Dillingham, B.L.; Lampe, J.W.; Duncan, A.M. Soy protein isolates of varying isoflavone content do not adversely affect semen quality in healthy young men. Fertil. Steril. 2010, 94, 1717–1722. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.Y.; Chen, Y.C.; Lin, P.; Shih, C.K.; Bai, C.H.; Yuan, K.C.; Lee, S.Y.; Chang, J.S. Testosterone-Associated Dietary Pattern Predicts Low Testosterone Levels and Hypogonadism. Nutrients 2018, 10, 1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Total (n = 3283) | Nutritional Status | pa | |
|---|---|---|---|---|
| Normal (n = 1756) | Overweight/Obese (n = 1527) | |||
| Age | <0.001 | |||
| <30 year | 1130 (34.4) | 643 (36.6) | 487 (31.9) | |
| 31–40 year | 1527 (46.5) | 828 (47.2) | 699 (45.8) | |
| >41 year | 626 (19.1) | 285 (16.2) | 341 (22.3) | |
| Smoker | 0.001 | |||
| No | 2035 (62.0) | 1135 (64.6) | 900 (58.9) | |
| Yes | 1248 (38.0) | 621 (35.4) | 627 (41.1) | |
| Alcoholic drinker | 0.02 | |||
| No | 2584 (78.7) | 1410 (80.3) | 1174 (76.9) | |
| Yes | 699 (21.3) | 346 (19.7) | 353 (23.1) | |
| Physical activity | 0.28 | |||
| None/light | 1844 (56.2) | 971 (55.3) | 873 (57.2) | |
| Moderate/intense | 1439 (43.8) | 785 (44.7) | 654 (42.8) | |
| BMI, kg/m2 | 24.1 ± 3.4 | 21.7 ± 1.7 | 26.8 ± 2.7 | <0.001 |
| Leukocytes, 103/μL | 6.2 ± 1.5 | 5.9 ± 1.5 | 6.5 ± 1.5 | <0.001 |
| Neutrophil/lymphocyte ratio | 1.8 ± 0.8 | 1.7 ± 0.8 | 1.8 ± 0.8 | 0.003 |
| Erythrocytes, 106/μL | 5.2 ± 0.4 | 5.1 ± 0.4 | 5.2 ± 0.4 | <0.001 |
| Hemoglobin, g/dL | 15.4 ± 1.0 | 15.3 ± 0.9 | 15.4 ± 1.0 | <0.001 |
| Hematocrit, % | 45.7 ± 2.8 | 45.5 ± 2.7 | 45.9 ± 2.8 | <0.001 |
| Fasting glucose, mmol/L | 5.5 ± 0.7 | 5.4 ± 0.5 | 5.6 ± 0.8 | <0.001 |
| Triglycerides, mmol/L | 1.4 ± 0.8 | 1.1 ± 0.6 | 1.6 ± 1.0 | <0.001 |
| Total cholesterol, mmol/L | 5.0 ± 0.9 | 4.9 ± 0.8 | 5.2 ± 0.9 | <0.001 |
| HDL-cholesterol, mmol/L | 1.3 ± 0.3 | 1.4 ± 0.3 | 1.3 ± 0.3 | <0.001 |
| LDL-cholesterol, mmol/L | 3.1 ± 0.8 | 3.0 ± 0.8 | 3.2 ± 0.8 | <0.001 |
| TC/HDL-cholesterol ratio | 3.9 ± 1.0 | 3.6 ± 0.9 | 4.2 ± 1.0 | <0.001 |
| Creatinine, μmol/L | 95.3 ± 10.8 | 94.9 ± 10.7 | 95.8 ± 10.9 | 0.02 |
| eGFR, mL/min/1.73 m2 | 90.2 ± 13.0 | 91.1 ± 12.9 | 89.2 ± 13.1 | <0.001 |
| C-reactive protein, nmol/L | 19.7 ± 32.8 | 16.4 ± 29.0 | 23.5 ± 36.3 | <0.001 |
| Iron, μmol/L | 18.7 ± 6.3 | 18.8 ± 6.4 | 18.5 ± 6.2 | 0.13 |
| TIBC, μmol/L | 55.7 ± 8.0 | 55.0 ± 7.7 | 56.5 ± 8.3 | 0.07 |
| Transferrin saturation, % | 45.0 ± 21.7 | 45.0 ± 21.8 | 45.0 ± 21.8 | 0.98 |
| Ferritin, μg/L | 240.7 ± 151.6 | 226.0 ± 128.5 | 252.9 ± 167.6 | 0.07 |
| Uric acid, mmol/L | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | <0.001 |
| FSH, IU/L | 4.6 ± 5.4 | 4.6 ± 7.0 | 4.6 ± 3.7 | 0.96 |
| LH, IU/L | 3.3 ± 2.2 | 3.4 ± 2.7 | 3.2 ± 1.7 | 0.54 |
| Testosterone, nmol/L | 17.5 ± 6.0 | 19.3 ± 6.1 | 15.8 ± 5.4 | <0.001 |
| E2, pmol/L | 90.3 ± 32.8 | 88.4 ± 30.7 | 91.8 ± 34.3 | 0.16 |
| SC, 106/mL | 46.6 ± 25.4 | 47.8 ± 25.8 | 45.0 ± 24.9 | 0.01 |
| TSM, % | 67.1 ± 11.6 | 67.2 ± 11.6 | 67.0 ± 11.6 | 0.81 |
| PRM, % | 48.3 ± 14.8 | 48.3 ± 14.7 | 48.3 ± 14.8 | 0.92 |
| NSM, % | 67.0 ± 13.3 | 67.4 ± 13.3 | 66.4 ± 13.3 | 0.09 |
| Variables | Model 1 a | Model 2 b | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | P | β | 95% CI | p | |
| Leukocytes, 103/μL | 0.04 | −0.17, 0.25 | 0.69 | −0.03 | −0.24, 0.18 | 0.77 |
| Neutrophil/lymphocyte ratio | −0.29 | −0.66, 0.08 | 0.12 | −0.28 | −0.64, 0.07 | 0.12 |
| Erythrocytes, 106/μL | 0.40 | −0.35, 1.15 | 0.30 | 0.47 | −0.26, 1.20 | 0.21 |
| Hemoglobin, g/dL | 0.61 | 0.29, 0.93 | <0.001 | 0.57 | 0.25, 0.89 | <0.001 |
| Hematocrit, % | 0.18 | 0.07, 0.29 | 0.002 | 0.17 | 0.06, 0.28 | 0.002 |
| Fasting glucose, mmol/L | −0.94 | −1.31, 0.58 | <0.001 | −0.93 | −1.29, −0.56 | <0.001 |
| Triglycerides, mmol/L | −0.82 | −1.16, −0.48 | <0.001 | −0.84 | −1.18, −0.50 | <0.001 |
| Total cholesterol, mmol/L | 0.18 | −0.18, 0.54 | 0.33 | 0.18 | −0.18, 0.53 | 0.33 |
| HDL-cholesterol, mmol/L | 3.86 | 2.73, 5.00 | <0.001 | 3.58 | 2.45, 4.71 | <0.001 |
| LDL-cholesterol, mmol/L | 0.12 | −0.26, 0.50 | 0.52 | 0.14 | −0.23, 0.51 | 0.47 |
| TC/HDL-cholesterol ratio | −0.84 | −1.21, −0.48 | <0.001 | −0.78 | −1.15, −0.42 | <0.001 |
| Creatinine, μmol/L | 0.03 | −0.00, 0.06 | 0.07 | 0.02 | −0.01, 0.05 | 0.19 |
| eGFR, mL/min/1.73 m2 | −0.03 | −0.06, 0.00 | 0.07 | −0.02 | −0.05, 0.01 | 0.22 |
| C-reactive protein, nmol/L | −0.01 | −0.02, 0.00 | 0.17 | −0.01 | −0.01, 0.01 | 0.35 |
| Iron, μmol/L | −0.02 | −0.07, 0.03 | 0.47 | −0.04 | −0.09, 0.01 | 0.14 |
| TIBC, μmol/L | −0.06 | −0.16, 0.04 | 0.27 | −0.06 | −0.16, 0.04 | 0.24 |
| Transferrin saturation, % | 0.01 | −0.03, 0.04 | 0.78 | 0.00 | −0.04, 0.04 | 0.98 |
| Ferritin, μg/L | 0.00 | −0.00, 0.00 | 0.77 | 0.00 | −0.00, 0.00 | 0.66 |
| Uric acid, mmol/L | −9.15 | −13.81, −4.49 | <0.001 | −10.77 | −15.31, −6.22 | <0.001 |
| FSH, IU/L | −0.11 | −0.19, −0.04 | 0.004 | −0.12 | −0.19, −0.04 | 0.002 |
| LH, IU/L | −0.05 | −0.23, 0.13 | 0.60 | −0.07 | −0.25, 0.11 | 0.44 |
| E2, pmol/L | 0.05 | 0.04, 0.06 | <0.001 | 0.05 | 0.04, 0.06 | <0.001 |
| Explained Variation (%) | Factor Loading a | |
|---|---|---|
| Predictor food groups | ||
| Milk | 26.43 | −0.47 |
| Dairy products | 5.48 | −0.21 |
| Innards organs | 16.12 | 0.37 |
| Legumes or beans products | 6.19 | −0.23 |
| Dark or leafy vegetables | 6.44 | −0.23 |
| Rice or flour products cooked in oil | 11.56 | 0.31 |
| Deep-fried foods | 8.78 | 0.27 |
| Preserved vegetables, processed meat, or fish | 8.44 | 0.27 |
| Dipping sauce | 9.24 | 0.28 |
| Total explained variation (%) | 29.65 | |
| Respond biomarkers | ||
| Hemoglobin | 1.91 | |
| Hematocrit | 1.86 | |
| Triglycerides | 1.11 | |
| HDL-cholesterol | 0.68 | |
| TC/HDL-cholesterol ratio | 1.76 | |
| Uric acid | 1.26 | |
| Total explained variation in biomarkers (%) | 2.72 | |
| Dietary Pattern Quartiles | Testosterone, nmol/L | FSH, IU/L | LH, IU/L | E2, pmol/L | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 β (95% CI) | Model 2 β (95% CI) | Model 1 β (95% CI) | Model 2 β (95% CI) | Model 1 β (95% CI) | Model 2 β (95% CI) | Model 1 β (95% CI) | Model 2 β (95% CI) | |
| Pooled (n = 3283) | ||||||||
| Q1 (low) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Q2 (mild) | 0.24 (−0.69, 1.16) | 0.02 (−0.91, 0.95) | 0.23 (−0.83, 1.31) | 0.17 (−0.91, 1.24) | −0.09 (−0.53, 0.35) | −0.13 (−0.58, 0.31) | 3.37 (−3.11, 9.85) | 3.54 (−2.96, 10.06) |
| Q3 (moderate) | −0.68 (−1.61, 0.24) | −0.69 (−1.60, 0.22) | 0.68 (−0.45, 1.81) | 0.59 (−0.55, 1.73) | 0.11 (−0.36, 0.58) | 0.05 (−0.42, 0.52) | 1.64 (−5.22, 8.51) | 1.41 (−5.51, 8.32) |
| Q4 (high) | −0.91 (−1.77, −0.06) * | −0.89 (−1.73, −0.05) * | 0.11 (−0.98, 1.21) | −0.04 (−1.17, 1.09) | 0.12 (−0.34, 0.57) | 0.01 (−0.45, 0.48) | 0.09 (−6.55, 6.74) | −0.56 (−7.38, 6.27) |
| Normal (n = 1756) | ||||||||
| Q1 (low) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Q2 (mild) | −0.88 (−2.30, 0.55) | −1.03 (−2.44, 0.39) | −0.25 (−2.29, 1.79) | −0.47 (−2.53, 1.58) | −0.30 (−1.09, 0.49) | −0.42 (−1.21, 0.36) | −2.72 (−11.76, 6.32) | −2.21 (−11.33, 6.92) |
| Q3 (moderate) | −1.14 (−2.55, 0.27) | −1.08 (−2.47, 0.31) | 1.22 (−0.99, 3.44) | 1.06 (−1.21, 3.32) | −0.18 (−1.04, 0.67) | −0.35 (−1.22, 0.51) | −2.00 (−11.80, 7.80) | −2.66 (−12.70, 7.39) |
| Q4 (high) | −1.47 (−2.76, −0.19) * | −1.48 (−2.72, −0.24) * | −0.25 (−2.42, 1.92) | −0.42 (−2.65, 1.80) | 0.05 (−0.78, 0.89) | −0.13 (−0.98, 0.72) | −4.60 (−14.21, 5.00) | −5.73 (−15.60, 4.14) |
| Overweight/obese (n = 1527) | ||||||||
| Q1 (low) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Q2 (mild) | 1.10 (−0.10, 2.31) | 0.86 (−0.35, 2.08) | 0.64 (−0.34, 1.62) | 0.59 (−0.40−1.58) | 0.09 (−0.40, 0.57) | 0.07 (−0.42, 0.56) | 3.50 (−5.61, 12.60) | 3.46 (−5.96, 12.87) |
| Q3 (moderate) | −0.28 (−1.49, 0.93) | −0.26 (−1.45, 0.93) | 0.25 (−0.78, 1.28) | 0.16 (−0.88, 1.19) | 0.29 (−0.22, 0.79) | 0.25 (−0.26, 0.76) | 3.68 (−5.87, 13.22) | 3.76 (−5.86, 13.38) |
| Q4 (high) | −0.35 (−1.48, 0.79) | −0.23 (−1.34, 0.88) | 0.38 (−0.60, 1.37) | 0.17 (−0.85, 1.18) | 0.17 (−0.31, 0.65) | 0.08 (−0.42, 0.57) | 8.68 (−0.45, 17.82) | 8.57 (−0.64, 17.79) |
| Dietary Pattern Quartiles | SC, 106/mL | TSM, % | PRM, % | NSM, % | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 β (95% CI) | Model 2 β (95% CI) | Model 1 β (95% CI) | Model 2 β (95% CI) | Model 1 β (95% CI) | Model 2 β (95% CI) | Model 1 β (95% CI) | Model 2 β (95% CI) | |
| Pooled (n = 3283) | ||||||||
| Q1 (low) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Q2 (mild) | −0.43 (−3.48, 2.62) | −0.37 (−3.46, 2.72) | 0.87 (−0.56, 2.29) | 0.89 (−0.53, 2.32) | 0.24 (−1.59, 2.06) | 0.24 (−1.58, 2.06) | −0.72 (−2.36, 0.91) | −0.69 (−2.32, 0.94) |
| Q3 (moderate) | −2.24 (−5.3, 0.83) | −2.21 (−5.28, 0.87) | −0.20 (−1.60, 1.20) | −0.20 (−1.60, 1.20) | 0.32 (−1.46, 2.11) | 0.33 (−1.46, 2.12) | −0.55 (−2.16, 1.05) | −0.48 (−2.07, 1.12) |
| Q4 (high) | −5.54 (−8.67, −2.42) ** | −5.55 (−8.68, −2.41) ** | −0.41 (−1.80, 0.98) | −0.63 (−2.03, 0.78) | 0.05 (−1.73, 1.83) | −0.17 (−1.97, 1.62) | −2.57 (−4.16, −0.98) ** | −2.22 (−3.83, −0.62) * |
| Normal (n = 1756) | ||||||||
| Q1 (low) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Q2 (mild) | 0.55 (−3.57, 4.66) | 0.78 (−3.39, 4.95) | 1.00 (−0.88, 2.88) | 1.04 (−0.84, 2.93) | 0.78 (−1.62, 3.19) | 0.85 (−1.55, 3.25) | −0.55 (−2.72, 1.61) | −0.60 (−2.75, 1.55) |
| Q3 (moderate) | −1.99 (−6.09, 2.11) | −1.97 (−6.08, 2.14) | −0.93 (−2.76, 0.91) | −0.92 (−2.77, 0.92) | −0.02 (−2.37, 2.33) | 0.06 (−2.29, 2.41) | −0.57 (−2.69, 1.54) | −0.57 (−2.68, 1.53) |
| Q4 (high) | −4.52 (−8.72, −0.31) * | −4.61 (−8.82, −0.40) * | 0.18 (−1.66, 2.02) | −0.08 (−1.94, 1.79) | −0.19 (−2.55, 2.16) | −0.55 (−2.94, 1.83) | −2.23 (−4.35, −0.11) * | −1.64 (−3.77, 0.49) |
| Overweight/obese (n = 1527) | ||||||||
| Q1 (low) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Q2 (mild) | −1.50 (−6.06, 3.06) | −1.81 (−6.43, 2.81) | 0.72 (−1.47, 2.91) | 0.71 (−1.48, 2.90) | 0.32 (−2.41, 3.04) | 0.29 (−2.47, 3.04) | −0.98 (−3.48, 1.52) | −0.91 (−3.42, 1.59) |
| Q3 (moderate) | −2.24 (−6.89, 2.40) | −2.31 (−6.96, 2.35) | 0.84 (−1.33, 3.00) | 0.81 (−1.36, 2.98) | 0.77 (−2.01, 3.54) | 0.74 (−2.04, 3.52) | −0.47 (−2.94, 2.00) | −0.36 (−2.83, 2.12) |
| Q4 (high) | −6.73 (−11.42, −2.03) ** | −6.73 (−11.44, −2.02) ** | −1.11 (−3.24, 1.01) | −1.30 (−3.45, 0.85) | −0.48 (−3.29, 2.33) | −0.52 (−3.32, 2.29) | −3.02 (−5.44, −0.59) * | −2.90 (−5.35, −0.44) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurniawan, A.-L.; Hsu, C.-Y.; Chao, J.C.-J.; Paramastri, R.; Lee, H.-A.; Lai, P.-C.; Hsieh, N.-C.; Wu, S.-F.V. Association of Testosterone-Related Dietary Pattern with Testicular Function among Adult Men: A Cross-Sectional Health Screening Study in Taiwan. Nutrients 2021, 13, 259. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010259
Kurniawan A-L, Hsu C-Y, Chao JC-J, Paramastri R, Lee H-A, Lai P-C, Hsieh N-C, Wu S-FV. Association of Testosterone-Related Dietary Pattern with Testicular Function among Adult Men: A Cross-Sectional Health Screening Study in Taiwan. Nutrients. 2021; 13(1):259. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010259
Chicago/Turabian StyleKurniawan, Adi-Lukas, Chien-Yeh Hsu, Jane C-J Chao, Rathi Paramastri, Hsiu-An Lee, Pao-Chin Lai, Nan-Chen Hsieh, and Shu-Fang Vivienne Wu. 2021. "Association of Testosterone-Related Dietary Pattern with Testicular Function among Adult Men: A Cross-Sectional Health Screening Study in Taiwan" Nutrients 13, no. 1: 259. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010259