Association of Circulating Trimethylamine N-Oxide and Its Dietary Determinants with the Risk of Kidney Graft Failure: Results of the TransplantLines Cohort Study

 ,
,  , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Dietary Intake Assessment
2.3. Laboratory Measurements
2.4. Clinical Endpoint
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Cross-Sectional Analyses
3.3. Longitudinal Analyses
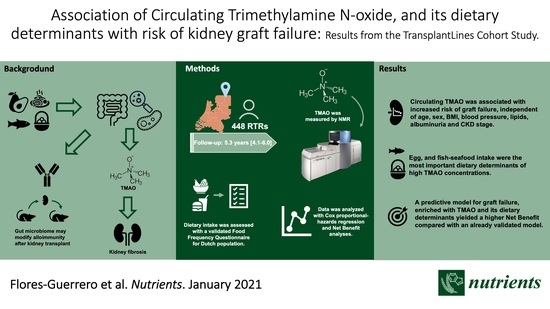
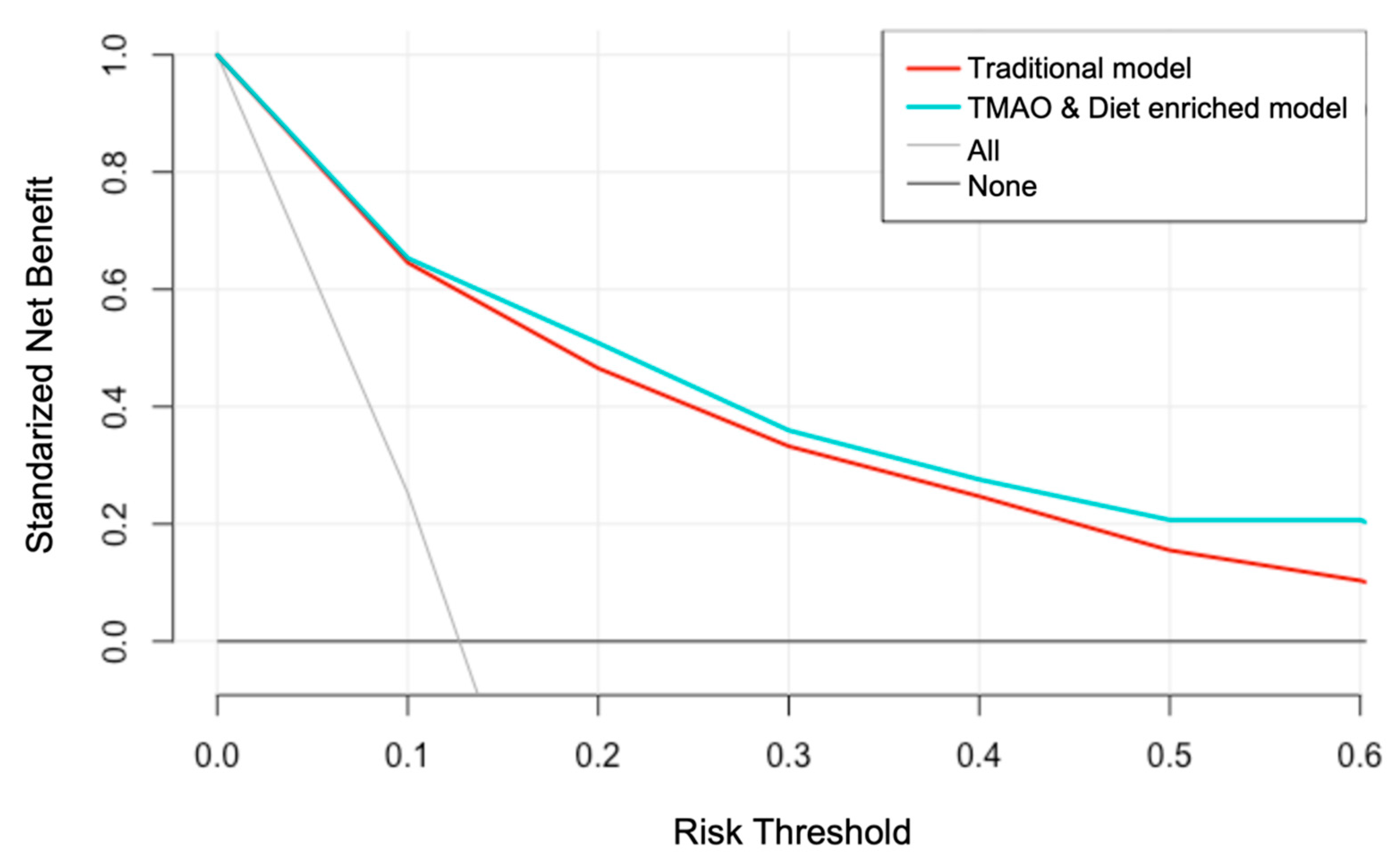
3.4. Clinical Utility of TMAO and Diet Assessment
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Axelrod, D.A.; Schnitzler, M.A.; Xiao, H.; Irish, W.; Tuttle-Newhall, E.; Chang, S.H.; Kasiske, B.L.; Alhamad, T.; Lentine, K.L. An economic assessment of contemporary kidney transplant practice. Am. J. Transplant. 2018, 18, 1168–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormick, F.; Held, P.J.; Chertow, G.M. The terrible toll of the kidney shortage. J. Am. Soc. Nephrol. 2018, 29, 2775–2776. [Google Scholar] [CrossRef] [PubMed]
- Lamb, K.E.; Lodhi, S.; Meier-Kriesche, H.U. Long-term renal allograft survival in the United States: A critical reappraisal. Am. J. Transplant. 2011, 11, 450–462. [Google Scholar] [CrossRef]
- Jardine, A.G.; Hartmann, A.; Holdaas, H. Long-term renal allograft survival: A quiet revolution. Kidney Int. 2018, 94, 853–855. [Google Scholar] [CrossRef]
- Vickers, A.J.; Van Calster, B.; Steyerberg, E.W. Net benefit approaches to the evaluation of prediction models, molecular markers, and diagnostic tests. BMJ 2016, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, H.C.; Graves, D.J. Natural methylamine osmolytes, trimethylamine N-oxide and betaine, increase tau-induced polymerization of microtubules. Biochem. Biophys. Res. Commun. 1998, 250, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Lee, J.; Hsu, J.; Su, M.M.; Wu, Y.; Lin, T.; Lan, C.; Hwang, J.; Lin, L. Myocardial adipose deposition and the development of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, ejhf.1617. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Wang, Z.; Shrestha, K.; Borowski, A.G.; Wu, Y.; Troughton, R.W.; Klein, A.L.; Hazen, S.L. Intestinal microbiota-dependent phosphatidylcholine metabolites, diastolic dysfunction, and adverse clinical outcomes in chronic systolic heart failure. J. Card. Fail. 2015, 21, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Pelletier, C.C.; Croyal, M.; Ene, L.; Aguesse, A.; Billon-Crossouard, S.; Krempf, M.; Lemoine, S.; Guebre-Egziabher, F.; Juillard, L.; Soulage, C.O. Elevation of trimethylamine-N-oxide in chronic kidney disease: Contribution of decreased glomerular filtration rate. Toxins 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Gruppen, E.G.; Garcia, E.; Connelly, M.A.; Jeyarajah, E.J.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. TMAO is Associated with Mortality: Impact of Modestly Impaired Renal Function. Sci. Rep. 2017, 7, 13781. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; Dugar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L.; et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013, 19, 576–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canyelles, M.; Tondo, M.; Cedó, L.; Farràs, M.; Escolà-Gil, J.C.; Blanco-Vaca, F. Trimethylamine N-oxide: A link among diet, gut microbiota, gene regulation of liver and intestine cholesterol homeostasis and HDL function. Int. J. Mol. Sci. 2018, 19, 3228. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, J.R.; House, J.A.; Ocque, A.J.; Zhang, S.; Johnson, C.; Kimber, C.; Schmidt, K.; Gupta, A.; Wetmore, J.B.; Nolin, T.D.; et al. Serum Trimethylamine-N-Oxide is Elevated in CKD and Correlates with Coronary Atherosclerosis Burden. J. Am. Soc. Nephrol. 2016, 27, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomlinson, J.A.P.; Wheeler, D.C. The role of trimethylamine N-oxide as a mediator of cardiovascular complications in chronic kidney disease. Kidney Int. 2017, 92, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Shafi, T.; Powe, N.R.; Meyer, T.W.; Hwang, S.; Hai, X.; Melamed, M.L.; Banerjee, T.; Coresh, J.; Hostetter, T.H. Trimethylamine n-oxide and cardiovascular events in hemodialysis patients. J. Am. Soc. Nephrol. 2017, 28, 321–331. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Singer, J.; Kwan, T.K.; Loh, Y.W.; Wang, C.; Tan, J.; Li, Y.J.; Lai, S.W.C.; Macia, L.; Alexander, S.I.; et al. Gut microbial metabolites induce donor-specific tolerance of kidney allografts through induction of T regulatory cells by short-chain fatty acids. J. Am. Soc. Nephrol. 2020, 31, 1445–1461. [Google Scholar] [CrossRef]
- Tang, W.H.W.; Wang, Z.; Kennedy, D.J.; Wu, Y.; Buffa, J.A.; Agatisa-Boyle, B.; Li, X.S.; Levison, B.S.; Hazen, S.L. Gut microbiota-dependent trimethylamine N-oxide (TMAO) pathway contributes to both development of renal insufficiency and mortality risk in chronic kidney disease. Circ. Res. 2014, 116, 448–455. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [CrossRef] [PubMed] [Green Version]
- Van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Joosten, M.M.; Gans, R.O.B.; Navis, G.; Bakker, S.J.L. Dietary acid load and metabolic acidosis in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1811–1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feunekes, I.J.; Van Staveren, W.A.; Graveland, F.; De Vos, J.; Burema, J. Reproducibility of a semiquantitative food frequency questionnaire to assess the intake of fats and cholesterol in the Netherlands. Int. J. Food Sci. Nutr. 1995, 46, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Van Den Berg, E.; Engberink, M.F.; Brink, E.J.; Van Baak, M.A.; Gans, R.O.B.; Navis, G.; Bakker, S.J.L. Dietary protein, blood pressure and renal function in renal transplant recipients. Br. J. Nutr. 2013, 109, 1463–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dullaart, R.P.F.; Garcia, E.; Jeyarajah, E.; Gruppen, E.G.; Connelly, M.A. Plasma phospholipid transfer protein activity is inversely associated with betaine in diabetic and non-diabetic subjects. Lipids Health Dis. 2016, 15, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A. Estimating GFR Using the CKD Epidemiology Collaboration (CKD-EPI) Creatinine Equation: More Accurate GFR Estimates, Lower CKD Prevalence Estimates, and Better Risk Predictions. Am. J. Kidney Dis. 2010, 55, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Eckardt, K.U.; Dorman, N.M.; Christiansen, S.L.; Hoorn, E.J.; Ingelfinger, J.R.; Inker, L.A.; Levin, A.; Mehrotra, R.; Palevsky, P.M.; et al. Nomenclature for kidney function and disease: Report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2020, 97, 1117–1129. [Google Scholar] [CrossRef]
- Montgomery, D.C.; Peck, E.A.; Vining, G.G. Introduction to Linear Regression Analysis, 5th ed.; John Wiley & Sons, Incorporated: Hoboken, NJ, USA, 2012; ISBN 9780470542811. [Google Scholar]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Statistics for Biology and Health; Springer: New York, NY, USA, 2000; ISBN 978-1-4419-3161-0. [Google Scholar]
- Shabir, S.; Halimi, J.M.; Cherukuri, A.; Ball, S.; Ferro, C.; Lipkin, G.; Benavente, D.; Gatault, P.; Baker, R.; Kiberd, B.; et al. Predicting 5-year risk of kidney transplant failure: A prediction instrument using data available at 1 year posttransplantation. Am. J. Kidney Dis. 2014, 63, 643–651. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B.; D’Agostino, R.B.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef]
- Wang, Z.; Bergeron, N.; Levison, B.S.; Li, X.S.; Chiu, S.; Jia, X.; Koeth, R.A.; Li, L.; Wu, Y.; Tang, W.H.W.; et al. Impact of chronic dietary red meat, white meat, or non-meat protein on trimethylamine N-oxide metabolism and renal excretion in healthy men and women. Eur. Heart J. 2019, 40, 583–594. [Google Scholar] [CrossRef]
- De Filippis, F.; Pellegrini, N.; Vannini, L.; Jeffery, I.B.; La Storia, A.; Laghi, L.I.; Serrazanetti, D.; Di Cagno, R.; Ferrocino, I.; Lazzi, C.; et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut 2016, 65, 1812–1821. [Google Scholar] [CrossRef]
- Manor, O.; Zubair, N.; Conomos, M.P.; Xu, X.; Rohwer, J.E.; Krafft, C.E.; Lovejoy, J.C.; Magis, A.T. A Multi-omic Association Study of Trimethylamine N-Oxide. Cell Rep. 2018, 24, 935–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thøgersen, R.; Rasmussen, M.K.; Sundekilde, U.K.; Goethals, S.A.; Van Hecke, T.; Vossen, E.; De Smet, S.; Bertram, H.C. Background diet influences TMAO concentrations associated with red meat intake without influencing apparent hepatic TMAO-related activity in a porcine model. Metabolites 2020, 10, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rufibach, K. Use of Brier score to assess binary predictions. J. Clin. Epidemiol. 2010, 63, 938–939. [Google Scholar] [CrossRef] [PubMed]
- Assel, M.; Sjoberg, D.D.; Vickers, A.J. The Brier score does not evaluate the clinical utility of diagnostic tests or prediction models. Diagnostic Progn. Res. 2017, 1, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickers, A.J.; Cronin, A.M.; Gönen, M. A simple decision analytic solution to the comparison of two binary diagnostic tests. Stat. Med. 2013, 32, 1865–1876. [Google Scholar] [CrossRef] [Green Version]
- Hunink, M.G.M.; Weinstein, M.C.; Wittenberg, E.; Drummond, M.F.; Pliskin, J.S.; Wong, J.B.; Glasziou, P.P. Decision Making in Health and Medicine; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Bain, M.A.; Faull, R.; Fornasini, G.; Milne, R.W.; Evans, A.M. Accumulation of trimethylamine and trimethylamine-N-oxide in end-stage renal disease patients undergoing haemodialysis. Nephrol. Dial. Transplant. 2006, 21, 1300–1304. [Google Scholar] [CrossRef] [Green Version]
- Treberg, J.R.; Driedzic, W.R. Elevated levels of trimethylamine oxide in deep-sea fish: Evidence for synthesis and intertissue physiological importance. J. Exp. Zool. 2002, 293, 39–45. [Google Scholar] [CrossRef]
- Miller, C.A.; Corbin, K.D.; Da Costa, K.A.; Zhang, S.; Zhao, X.; Galanko, J.A.; Blevins, T.; Bennett, B.J.; O’Connor, A.; Zeisel, S.H. Effect of egg ingestion on trimethylamine-N-oxide production in humans: A randomized, controlled, dose-response study. Am. J. Clin. Nutr. 2014, 100, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Ramezani, A.; Raj, D.S. The gut microbiome, kidney disease, and targeted interventions. J. Am. Soc. Nephrol. 2014, 25, 657–670. [Google Scholar] [CrossRef] [Green Version]
- Bunnapradist, S.; Neri, L.; Wong, W.; Lentine, K.L.; Burroughs, T.E.; Pinsky, B.W.; Takemoto, S.K.; Schnitzler, M.A. Incidence and Risk Factors for Diarrhea Following Kidney Transplantation and Association with Graft Loss and Mortality. Am. J. Kidney Dis. 2008, 51, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.R.; Magruder, M.; Zhang, L.; Westblade, L.F.; Satlin, M.J.; Robertson, A.; Edusei, E.; Crawford, C.; Ling, L.; Taur, Y.; et al. Gut microbiota dysbiosis and diarrhea in kidney transplant recipients. Am. J. Transplant. 2019, 19, 488–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostidis, S.; Bank, J.R.; Soonawala, D.; Nevedomskaya, E.; Kooten, C.; Mayboroda, O.A.; Fijter, J.W. Urinary metabolites predict prolonged duration of delayed graft function in DCD kidney transplant recipients. Am. J. Transplant. 2019, 19, 110–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Skeans, M.A.; Peng, Y.; Weinhandl, E.D. A simple tool to predict outcomes after kidney transplant. Am. J. Kidney Dis. 2010, 56, 947–960. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 448) | Tertile 1 (n = 147) (<3.93 μmol/L) | Tertile 2 (n = 149) (3.93 to 8.07 μmol/L) | Tertile 3 (n = 152) (>8.07 μmol/L) | p-Value |
|---|---|---|---|---|---|
| Men, n (%) | 238 (53.1%) | 70 (47.6%) | 79 (53.0%) | 89 (58.6%) | 0.17 |
| Age, year | 52.71 (13.09) | 50.32 (13.14) | 53.43 (12.64) | 54.32 (13.23) | 0.02 |
| BMI, kg/m2 | 26.41 (4.79) | 26.47 (5.01) | 26.14 (4.37) | 26.63 (4.97) | 0.67 |
| SBP, mmHg | 135.85 (17.56) | 135.25 (15.58) | 134.47 (17.55) | 137.77 (19.24) | 0.24 |
| DBP, mmHg | 81.86 (10.95) | 82.35 (10.49) | 81.50 (10.85) | 81.73 (11.54) | 0.79 |
| Heart Rate, bpm | 67.97 (11.67) | 68.20 (11.58) | 68.03 (11.63) | 67.69 (11.86) | 0.93 |
| Glucose, mmol/L | 5.20 (4.70, 5.90) | 5.30 (4.80, 5.70) | 5.15 (4.70, 5.90) | 5.30 (4.70, 6.00) | 0.69 |
| TG, mmol/L | 1.88 (0.94) | 1.80 (0.91) | 1.89 (1.01) | 1.95 (0.89) | 0.21 |
| TC, mmol/L | 5.12 (1.14) | 5.18 (1.15) | 5.11 (1.19) | 5.07 (1.08) | 0.72 |
| HDL-C, mmol/L | 1.37 (0.46) | 1.47 (0.48) | 1.35 (0.44) | 1.31 (0.46) | 0.01 |
| HbA1c, % | 5.80 (5.50, 6.10) | 5.80 (5.45, 6.25) | 5.70 (5.40, 6.00) | 5.80 (5.50, 6.10) | 0.32 |
| TMAO, μmol/L | 5.66 (3.08, 11.20) | 2.41 (1.44, 3.06) | 5.62 (4.82, 6.69) | 15.09 (11.08, 22.11) | <0.001 |
| eGFR, mL/min/1.73 m2 | 49.93 (19.38) | 62.12 (16.70) | 49.35 (15.58) | 38.71 (18.23) | <0.001 |
| CKD stage, n (%) | <0.001 | ||||
| G1 | 12 (2.7%) | 8 (5.4%) | 2 (1.3%) | 2 (1.3%) | |
| G2 | 125 (27.9%) | 72 (49.0%) | 38 (25.5%) | 15 (9.9%) | |
| G3a | 115 (25.7%) | 41 (27.9%) | 47 (31.5%) | 27 (17.8%) | |
| G3b | 128 (28.6%) | 25 (17.0%) | 47 (31.5%) | 56 (36.8%) | |
| G4 | 62 (13.8%) | 1 (0.7%) | 15 (10.1%) | 46 (30.3%) | |
| G5 | 6 (1.3%) | 0 (0.0%) | 0 (0.0%) | 6 (3.9%) | |
| UAE, mg/24 h | 43.97 (11.75, 207.12) | 37.70 (9.62, 177.82) | 30.55 (8.48, 108.65) | 90.03 (16.54, 384.67) | <0.001 |
| Current smokers, n (%) | 56 (13.2%) | 15 (11.1%) | 16 (11.3%) | 25 (17.0%) | 0.24 |
| Alcohol consumption, g/day | 2.20 (0.04, 10.47) | 2.01 (0.03, 11.33) | 2.49 (0.06, 9.65) | 2.62 (0.03, 10.33) | 0.94 |
| Total energy intake, kcal/day | 2138.61 (613.46) | 2204.56 (558.62) | 2137.56 (650.91) | 2072.21 (626.80) | 0.21 |
| Egg intake, g/day | 8.93 (4.46, 14.29) | 8.93 (4.46, 14.29) | 7.14 (4.46, 14.29) | 8.93 (7.14, 14.29) | 0.25 |
| Vegetable intake, g/day | 107.00 (71.50, 147.90) | 110.71 (81.69, 144.21) | 112.67 (72.81, 156.02) | 95.75 (65.83, 140.15) | 0.10 |
| Fruit intake, g/day | 105.43 (49.71, 191.53) | 90.11 (39.63, 178.02) | 123.79 (53.07, 212.64) | 99.43 (52.71, 191.41) | 0.25 |
| Fiber intake, g/day | 20.86 (16.32, 26.39) | 21.07 (15.88, 27.15) | 21.47 (17.93, 28.23) | 19.95 (15.28, 25.29) | 0.08 |
| Fish and sea food intake, g/day | 10.81 (4.42, 18.71) | 9.94 (3.89, 17.07) | 10.69 (4.68, 16.93) | 14.87 (4.68, 22.96) | 0.02 |
| Meat intake, g/day | 83.82 (60.95, 100.30) | 84.06 (59.58, 102.90) | 80.51 (64.76, 98.25) | 84.60 (59.92, 99.49) | 0.86 |
| Transplant vintage, year | 4.95 (1.59, 11.54) | 4.88 (1.79, 10.26) | 4.08 (1.31, 10.58) | 6.14 (1.76, 14.43) | 0.09 |
| Preemptive, n (%) | 69 (17.5%) | 28 (20.9%) | 26 (20.3%) | 15 (11.3%) | 0.07 |
| Living donor, n (%) | 158 (35.3%) | 62 (42.2%) | 57 (38.3%) | 39 (25.7%) | 0.007 |
| HLA-A,-B broad antigen mismatch, n (%) | 0.99 | ||||
| 0 | 94 (22.8%) | 29 (21.6%) | 32 (22.7%) | 33 (23.9%) | |
| 1 | 97 (23.5%) | 35 (26.1%) | 33 (23.4%) | 29 (21.0%) | |
| 2 | 151 (36.6%) | 48 (35.8%) | 51 (36.2%) | 52 (37.7%) | |
| 3 | 46 (11.1%) | 14 (10.4%) | 16 (11.3%) | 16 (11.6%) | |
| 4 | 25 (6.1%) | 8 (6.0%) | 9 (6.4%) | 8 (5.8%) | |
| HLA-DR broad antigen mismatch, n (%) | 0.49 | ||||
| 0 | 175 (42.6%) | 60 (45.1%) | 55 (39.0%) | 60 (43.8%) | |
| 1 | 192 (46.7%) | 60 (45.1%) | 66 (46.8%) | 66 (48.2%) | |
| 2 | 44 (10.7%) | 13 (9.8%) | 20 (14.2%) | 11 (8.0%) | |
| Tacrolimus, n (%) | 68 (17.2%) | 17 (12.7%) | 22 (17.2%) | 29 (21.8%) | 0.14 |
| Cyclosporine, n (%) | 173 (43.8%) | 48 (35.8%) | 60 (46.9%) | 65 (48.9%) | 0.07 |
| Azathioprine, n (%) | 72 (18.2%) | 21 (15.7%) | 17 (13.3%) | 34 (25.6%) | 0.02 |
| Mycophenolic acid, n (%) | 262 (66.3%) | 98 (73.1%) | 90 (70.3%) | 74 (55.6%) | 0.005 |
| Prednisolone dose, mg/day | 10.00 (7.50, 10.00) | 10.00 (7.50, 10.00) | 10.00 (7.50, 10.00) | 10.00 (7.50, 10.00) | 0.42 |
| Statins, n (%) | 233 (52.0%) | 70 (47.6%) | 73 (49.0%) | 90 (59.2%) | 0.09 |
| Diuretics, n (%) | 177 (39.5%) | 47 (32.0%) | 55 (36.9%) | 75 (49.3%) | 0.007 |
| Univariable Regression | Multivariable Regression | |||
|---|---|---|---|---|
| Variable | β (95% CI) | p-Value | β (95% CI) | p-Value |
| Sex, male, yes | 0.02 (−0.17, 0.21) | 0.83 | — | — |
| Age, year | 0.03 (−0.06, 0.12) | 0.54 | — | — |
| BMI, kg/m2 | 0.06 (−0.04, 0.15) | 0.24 | — | — |
| SBP, mm Hg | 0.06 (−0.03, 0.15) | 0.21 | 0.15 (0.03, 0.27) | 0.01 |
| DBP, mm Hg | −0.05 (−0.14, 0.05) | 0.32 | −0.13 (−0.25, −0.02) | 0.03 |
| Heart rate, bpm | 0.03 (−0.07, 0.12) | 0.56 | — | — |
| Glucose, mmol/L | 0.02 (−0.08, 0.11) | 0.72 | — | — |
| TG, mmol/L | 0.03 (−0.06, 0.12) | 0.53 | — | — |
| TC, mmol/L | −0.09 (−0.19, 0.00) | 0.05 | −0.15 (−0.24, −0.06) | 0.001 |
| HDL-C, mmol/L | −0.12 (−0.21, −0.02) | 0.01 | — | — |
| HbA1C, % | 0.02 (−0.08, 0.11) | 0.71 | — | — |
| eGFR, mL/min/1.73 m2 | −0.29 (−0.38, −0.20) | <0.001 | −0.28 (−0.36, −0.19) | <0.001 |
| CKD stage, yes | ||||
| G2 | 0.01 (−0.56, 0.57) | 0.99 | — | — |
| G3a | 0.10 (−0.47, 0.67) | 0.74 | — | — |
| G3b | 0.46 (−0.10, 1.00) | 0.11 | — | — |
| G4 | 0.88 (0.29, 1.50) | 0.003 | — | — |
| G5 | 1.00 (0.02, 1.90) | 0.04 | — | — |
| UAE, mg/24 h | 0.08 (−0.01, 0.17) | 0.08 | — | — |
| Current smoking, yes | 0.10(−0.19, 0.39) | 0.49 | — | — |
| Alcohol consumption, g/day | −0.04 (−0.13, 0.05) | 0.39 | — | — |
| Total energy intake, kcal/day | −0.07 (−0.16, 0.02) | 0.12 | — | — |
| Egg intake, g/day | 0.03 (−0.06, 0.11) | 0.57 | 0.09 (0.01, 0.18) | 0.03 |
| Vegetable intake, g/day | −0.07 (−0.16, 0.01) | 0.10 | — | — |
| Fruit intake, g/day | −0.04 (−0.13, 0.04) | 0.33 | — | — |
| Vegetable and Fruit intake, g/day | −0.07 (−0.16, 0.02) | 0.13 | — | — |
| Fiber intake, g/day | −0.08 (−0.17, 0.01) | 0.06 | −0.14 (−0.22, −0.05) | 0.002 |
| Fish and Seafood intake, g/day | 0.15 (0.06, 0.24) | <0.001 | 0.12 (0.03,0.21) | 0.01 |
| Meat intake, g/day | −0.01 (−0.09, 0.08) | 0.89 | — | — |
| Transplant vintage, year | 0.01 (−0.08, 0.10) | 0.84 | — | — |
| Preemptive, yes | −0.23 (−0.47, 0.00) | 0.05 | — | — |
| Living donor, yes | −0.24 (−0.43, −0.05) | 0.02 | −0.08 (−0.17, 0.00) | 0.06 |
| HLA-A,-B broad antigen mismatch, yes | ||||
| 1 | −0.12 (−0.41, 0.16) | 0.39 | — | — |
| 2 | 0.04 (−0.22, 0.30) | 0.75 | — | — |
| 3 | 0.05 (−0.31, 0.40) | 0.80 | — | — |
| 4 | −0.16 (−0.60, 0.29) | 0.48 | — | — |
| HLA-DR broad antigen mismatch, yes | ||||
| 1 | 0.08 (−0.12, 0.29) | 0.43 | — | — |
| 2 | 0.07 (−0.26, 0.41) | 0.66 | — | — |
| Tacrolimus, yes | 0.31 (0.08, 0.54) | 0.009 | — | — |
| Cyclosporine, yes | −0.01 (−0.19, 0.17) | 0.92 | — | — |
| Azathioprine, yes | 0.15 (−0.08, 0.38) | 0.19 | — | — |
| Mycophenolic acid, yes | −0.16 (−0.35, 0.03) | 0.09 | — | — |
| Prednisolone dose, mg/day | −0.01 (−0.10, 0.09) | 0.89 | — | — |
| Statins, yes | 0.02 (−0.17, 0.21) | 0.83 | — | — |
| Diuretics, yes | 0.23 (0.04, 0.42) | 0.02 | — | — |
| TMAO Per 1 SD Increment | Tertile 1 (0.21–3.92) | Tertile 2 (3.93–8.07) | Tertile 3 (8.07–154.3) | ||||
|---|---|---|---|---|---|---|---|
| Participants, n | 448 | 147 | 149 | 152 | |||
| Events, n | 58 | 6 | 14 | 38 | |||
| HR [95% CI] | p-value | HR [95% CI] | p-value | HR [95% CI] | p-value | ||
| Crude Model | 2.22 [1.73; 2.84] | <0.001 | (ref) | 2.41 [0.93; 6.27] | 0.07 | 7.62 [3.22; 18.03] | <0.001 |
| Model 1 | 2.20 [1.73; 2.80] | <0.001 | (ref) | 2.54 [0.97; 6.62] | 0.06 | 8.17 [3.44; 19.43] | <0.001 |
| Model 2 | 2.27 [1.64; 3.14] | <0.001 | (ref) | 1.73 [0.60; 4.95] | 0.31 | 5.41 [2.17; 13.48] | <0.001 |
| Model 3 | 1.39 [1.01; 1.91] | 0.04 | (ref) | 2.06 [0.75; 5.70] | 0.16 | 3.01 [1.10; 8.26] | 0.03 |
| Model 4 | 2.86 [2.13; 3.83] | <0.001 | (ref) | 2.02 [0.73; 5.57] | 0.17 | 9.15 [3.79; 22.04] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores-Guerrero, J.L.; Osté, M.C.J.; Baraldi, P.B.; Connelly, M.A.; Garcia, E.; Navis, G.; Bakker, S.J.L.; Dullaart, R.P.F. Association of Circulating Trimethylamine N-Oxide and Its Dietary Determinants with the Risk of Kidney Graft Failure: Results of the TransplantLines Cohort Study. Nutrients 2021, 13, 262. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010262
Flores-Guerrero JL, Osté MCJ, Baraldi PB, Connelly MA, Garcia E, Navis G, Bakker SJL, Dullaart RPF. Association of Circulating Trimethylamine N-Oxide and Its Dietary Determinants with the Risk of Kidney Graft Failure: Results of the TransplantLines Cohort Study. Nutrients. 2021; 13(1):262. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010262
Chicago/Turabian StyleFlores-Guerrero, Jose L., Maryse C. J. Osté, Paula B. Baraldi, Margery A. Connelly, Erwin Garcia, Gerjan Navis, Stephan J. L. Bakker, and Robin P. F. Dullaart. 2021. "Association of Circulating Trimethylamine N-Oxide and Its Dietary Determinants with the Risk of Kidney Graft Failure: Results of the TransplantLines Cohort Study" Nutrients 13, no. 1: 262. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010262