
The Nutritional Status of Long-Term Institutionalized Older Adults Is Associated with Functional Status, Physical Performance and Activity, and Frailty

 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
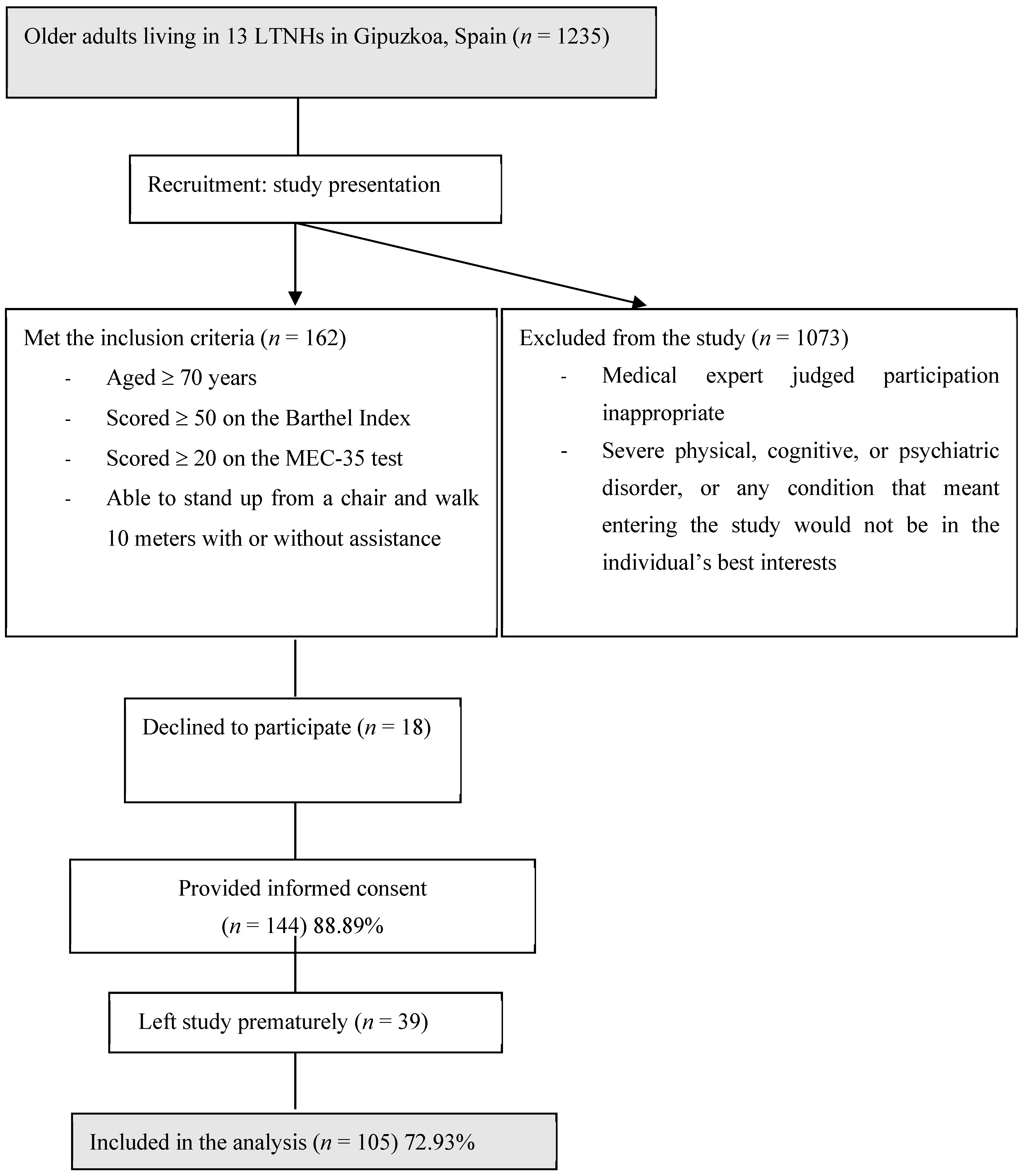
2.1. Study Design and Participants
2.2. Variables Measured
2.3. Statistical Analysis
3. Results
4. Discussion
5. Strength of the Study
6. Limitations of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salva, A.; Coll-Planas, L.; Bruce, S.; De Groot, L.; Andrieu, S.; Abellan, G.; Vellas, B.; The Task Force on Nutrition and Ageing of the IAGG and the IANA. Nutritional Assessment of Residents in Long-Term Care Facilities (LTCFs): Recommendations of the Task Force on Nutrition and Ageing of the IAGG European Region and the IANA. J. Nutr. Health Aging 2009, 13, 475–483. [Google Scholar] [CrossRef]
- Mathewson, S.L.; Azevedo, P.S.; Gordon, A.L.; Phillips, B.E.; Greig, C.A. Overcoming protein-energy malnutrition in older adults in the residential care setting: A narrative review of causes and interventions. Ageing Res. Rev. 2021, 70, 101401. [Google Scholar] [CrossRef]
- Clegg, M.E.; Williams, E.A. Optimizing nutrition in older people. Maturitas 2018, 112, 34–38. [Google Scholar] [CrossRef]
- Brownie, S. Why are elderly individuals at risk of nutritional deficiency? Int. J. Nurs. Pract. 2006, 12, 110–118. [Google Scholar] [CrossRef]
- Kiesswetter, E.; Colombo, M.G.; Meisinger, C.; Peters, A.; Thorand, B.; Holle, R.; Ladwig, K.H.; Schulz, H.; Grill, E.; Diekmann, R.; et al. Malnutrition and Related Risk Factors in Older Adults from Different Health-Care Settings: An Enable Study. Public Health Nutr. 2020, 23, 446–456. [Google Scholar] [CrossRef] [Green Version]
- Roberts, C.E.; Phillips, L.H.; Cooper, C.L.; Gray, S.; Allan, J.L. Effect of Different Types of Physical Activity on Activities of Daily Living in Older Adults: Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2017, 25, 653–670. [Google Scholar] [CrossRef] [Green Version]
- Motamed-Jahromi, M.; Kaveh, M.H. Effective Interventions on Improving Elderly’s Independence in Activity of Daily Living: A Systematic Review and Logic Model. Front. Public Health 2021, 8, 516151. [Google Scholar] [CrossRef] [PubMed]
- Glass, N.L.; Bellettiere, J.; Jain, P.; LaMonte, M.J.; La Croix, A.Z.; Women’s Health Initiative. Evaluation of Light Physical Activity Measured by Accelerometry and Mobility Disability during a 6-Year Follow-Up in Older Women. JAMA Netw. Open 2021, 4, e210005. [Google Scholar] [CrossRef] [PubMed]
- Stattin, K.; Michaelsson, K.; Larsson, S.C.; Wolk, A.; Byberg, L. Leisure-Time Physical Activity and Risk of Fracture: A Cohort Study of 66,940 Men and Women. J. Bone Miner. Res. 2017, 32, 1599–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, R.M.; Reynolds, C.F. Management of Depression in Older Adults: A Review. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef]
- Murri, M.B.; Ekkekakis, P.; Menchetti, M.; Neviani, F.; Trevisani, F.; Tedeschi, S.; Latessa, P.M.; Nerozzi, E.; Ermini, G.; Zocchi, D.; et al. Physical Exercise for Late-Life Depression: Effects on Symptom Dimensions and Time Course. J. Affect. Disord. 2018, 230, 65–70. [Google Scholar] [CrossRef]
- Moraes, H.S.; Silveira, H.S.; Oliveira, N.A.; Matta Mello Portugal, E.; Araujo, N.B.; Vasques, P.E.; Bergland, A.; Santos, T.M.; Engedal, K.; Coutinho, E.S.; et al. Is Strength Training as Effective as Aerobic Training for Depression in Older Adults? A Randomized Controlled Trial. Neuropsychobiology 2020, 79, 141–149. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef] [Green Version]
- Tarazona-Santabalbina, F.J.; Gomez-Cabrera, M.C.; Perez-Ros, P.; Martinez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Manas, L.; Vina, J. A Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, H.; Rezola-Pardo, C.; Echeverria, I.; Iturburu, M.; Gil, S.M.; Yanguas, J.J.; Irazusta, J.; Rodriguez-Larrad, A. Physical Activity and Fitness are Associated with Verbal Memory, Quality of Life and Depression among Nursing Home Residents: Preliminary Data of a Randomized Controlled Trial. BMC Geriatr. 2018, 18, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Saghafi-Asl, M.; Vaghef-Mehrabany, E. Comprehensive Comparison of Malnutrition and its Associated Factors between Nursing Home and Community Dwelling Elderly: A Case-Control Study from Northwestern Iran. Clin. Nutr. ESPEN 2017, 21, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Tay, L.B.; Chua, M.P.; Tay, E.L.; Chan, H.N.; Mah, S.M.; Latib, A.; Wong, C.Q.; Ng, Y.S. Multidomain Geriatric Screen and Physical Fitness Assessment Identify Prefrailty/Frailty and Potentially Modifiable Risk Factors in Community-Dwelling Older Adults. Ann. Acad. Med. Singap. 2019, 48, 171–180. [Google Scholar] [PubMed]
- Aspell, N.; Laird, E.; Healy, M.; Lawlor, B.; O’Sullivan, M. Vitamin D Deficiency is Associated with Impaired Muscle Strength and Physical Performance in Community-Dwelling Older Adults: Findings from the English Longitudinal Study of Ageing. Clin. Interv. Aging 2019, 14, 1751–1761. [Google Scholar] [CrossRef] [Green Version]
- Ge, L.; Yap, C.W.; Heng, B.H. Association of Nutritional Status with Physical Function and Disability in Community-Dwelling Older Adults: A Longitudinal Data Analysis. J. Nutr. Gerontol. Geriatr. 2020, 39, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Izawa, S.; Enoki, H.; Hasegawa, J.; Hirose, T.; Kuzuya, M. Factors Associated with Deterioration of Mini Nutritional Assessment-Short Form Status of Nursing Home Residents during a 2-Year Period. J. Nutr. Health Aging 2014, 18, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Vandewoude, M.F.J.; van Wijngaarden, J.P.; De Maesschalck, L.; Luiking, Y.C.; Van Gossum, A. The Prevalence and Health Burden of Malnutrition in Belgian Older People in the Community or Residing in Nursing Homes: Results of the NutriAction II Study. Aging Clin. Exp. Res. 2019, 31, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, K.A.; Meskers, C.G.M.; Trappenburg, M.C.; Verlaan, S.; Reijnierse, E.M.; Whittaker, A.C.; Maier, A.B. Malnutrition is Associated with Dynamic Physical Performance. Aging Clin. Exp. Res. 2020, 32, 1085–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corcoran, M.P.; Nelson, M.E.; Sacheck, J.M.; Reid, K.F.; Kirn, D.; Fielding, R.A.; Chui, K.K.H.; Folta, S.C. Efficacy of an Exercise and Nutritional Supplement Program on Physical Performance and Nutritional Status in Older Adults with Mobility Limitations Residing at Senior Living Facilities. J. Aging Phys. Act. 2017, 25, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Hernandez Morante, J.J.; Gomez Martinez, C.; Morillas-Ruiz, J.M. Dietary Factors Associated with Frailty in Old Adults: A Review of Nutritional Interventions to Prevent Frailty Development. Nutrients 2019, 11, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni Lochlainn, M.; Cox, N.J.; Wilson, T.; Hayhoe, R.P.G.; Ramsay, S.E.; Granic, A.; Isanejad, M.; Roberts, H.C.; Wilson, D.; Welch, C.; et al. Nutrition and Frailty: Opportunities for Prevention and Treatment. Nutrients 2021, 13, 2349. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone Singh, M.A.; Bernstein, M.A.; Ryan, A.D.; O’Neill, E.F.; Clements, K.M.; Evans, W.J. The effect of oral nutritional supplements on habitual dietary quality and quantity in frail elders. J. Nutr. Health Aging 2000, 4, 5–12. [Google Scholar]
- Smoliner, C.; Norman, K.; Scheufele, R.; Hartig, W.; Pirlich, M.; Lochs, H. Effects of Food Fortification on Nutritional and Functional Status in Frail Elderly Nursing Home Residents at Risk of Malnutrition. Nutrition 2008, 24, 1139–1144. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales Asín, F.; Fernando Pascual, L.; Montañés, J.Á.; Aznar, S. Revalidación Y Normalización Del Mini-Examen Cognoscitivo (Primera Versión En Castellano Del Mini-Mental Status Examination) En La Población General Geriátrica. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Assessing the Nutritional Status of the Elderly: The Mini Nutritional Assessment as Part of the Geriatric Evaluation. Nutr. Rev. 1996, 54, S59. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a Combined Comorbidity Index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults (US). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998. [Google Scholar]
- Wade, D.T.; Collin, C. The Barthel ADL Index: A Standard Measure of Physical Disability? Int. Disabil. Stud. 1988, 10, 64–67. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. Ser. A 2000, 55, M221–M231. [Google Scholar] [CrossRef] [Green Version]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The Sit-to-Stand Muscle Power Test: An Easy, Inexpensive and Portable Procedure to Assess Muscle Power in Older People. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef]
- Bohannon, R.W. Reference Values for the Timed Up and Go Test: A Descriptive Meta-Analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Fess, E. Clinical Assessment Recommendations. American society of hand therapists. Grip Strength 1981, 1, 6–8. [Google Scholar]
- Hauer, K.; Lord, S.R.; Lindemann, U.; Lamb, S.E.; Aminian, K.; Schwenk, M. Assessment of Physical Activity in Older People with and without Cognitive Impairment. J. Aging Phys. Act. 2011, 19, 347–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; Brien, W.L.O.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O. Compendium of Physical Activities: An Update of Activity Codes and MET Intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Theou, O. Using the Clinical Frailty Scale in Allocating Scarce Health Care Resources. Can. Geriatr. J. 2020, 23, 210–215. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. The Tilburg Frailty Indicator: Psychometric Properties. J. Am. Med. Dir. Assoc. 2010, 11, 344–355. [Google Scholar] [CrossRef]
- Piglowska, M.; Guligowska, A.; Kostka, T. Nutritional Status Plays More Important Role in Determining Functional State in Older People Living in the Community than in Nursing Home Residents. Nutrients 2020, 12, 42. [Google Scholar] [CrossRef] [PubMed]
- Caçador, C.; Teixeira-Lemos, E.; Oliveira, J.; Pinheiro, J.; Mascarenhas-Melo, F.; Ramos, F. The Relationship between Nutritional Status and Functional Capacity: A Contribution Study in Institutionalised Portuguese Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 3789. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Stephan, B.; Rosano, A.; Molfino, A.; Poggiogalle, E.; Lenzi, A.; Siervo, M.; Muscaritoli, M. What are the Risk Factors for Malnutrition in Older-Aged Institutionalized Adults? Nutrients 2020, 12, 2857. [Google Scholar] [CrossRef] [PubMed]
- Jerez-Roig, J.; de Brito Macedo Ferreira, L.M.; Torres de Araújo, J.R.; Costa Lima, K. Functional Decline in Nursing Home Residents: A Prognostic Study. PLoS ONE 2017, 12, e0177353. [Google Scholar] [CrossRef]
- López-Contreras, M.; Torralba, C.; Zamora, S.; Pérez-Llamas, F. Nutrition and Prevalence of Undernutrition Assessed by Different Diagnostic Criteria in Nursing Homes for Elderly People. J. Hum. Nutr. Diet. 2012, 25, 239–246. [Google Scholar] [CrossRef] [PubMed]
- de Medeiros, M.M.D.; de Figueredo, O.M.C.; Pinheiro, M.A.; de Oliveira, L.F.S.; Wanderley, R.L.; Cavalcanti, Y.W.; Garcia, R.C.M.R. Factors Associated with the Overlap of Frailty and Nutrition in Institutionalized Older Adults: A Multicenter Study. Arch. Gerontol. Geriatr. 2020, 90, 104150. [Google Scholar] [CrossRef]
- Onder, G.; Carpenter, I.; Finne-Soveri, H.; Gindin, J.; Frijters, D.; Henrard, J.C.; Nikolaus, T.; Topinkova, E.; Tosato, M.; Liperoti, R. Assessment of Nursing Home Residents in Europe: The Services and Health for Elderly in Long TERm Care (SHELTER) Study. BMC Health Serv. Res. 2012, 12, 1–10. [Google Scholar] [CrossRef]
- Kojima, G. Prevalence of Frailty in Nursing Homes: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2015, 16, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Faxen-Irving, G.; Luiking, Y.; Gronstedt, H.; Franzen, E.; Seiger, A.; Vikstrom, S.; Wimo, A.; Bostrom, A.M.; Cederholm, T. Do Malnutrition, Sarcopenia and Frailty Overlap in Nursing-Home Residents? J. Frailty Aging 2021, 10, 17–21. [Google Scholar]
- Al Snih, S.; Ottenbacher, K.J.; Markides, K.S.; Kuo, Y.; Eschbach, K.; Goodwin, J.S. The Effect of Obesity on Disability Vs Mortality in Older Americans. Arch. Intern. Med. 2007, 167, 774–780. [Google Scholar] [CrossRef] [Green Version]
- Winter, J.E.; MacInnis, R.J.; Wattanapenpaiboon, N.; Nowson, C.A. BMI and all-Cause Mortality in Older Adults: A Meta-Analysis. Am. J. Clin. Nutr. 2014, 99, 875–890. [Google Scholar] [CrossRef] [Green Version]
- Bosello, O.; Vanzo, A. Obesity Paradox and Aging. Eat. Weight Disord. 2021, 26, 27–35. [Google Scholar] [CrossRef]
- Atkins, J.L.; Wannamathee, S.G. Sarcopenic Obesity in Ageing: Cardiovascular Outcomes and Mortality. Br. J. Nutr. 2020, 124, 1102–1113. [Google Scholar] [CrossRef]
- Liu, W.; Chen, S.; Jiang, F.; Zhou, C.; Tang, S. Malnutrition and Physical Frailty among Nursing Home Residents: A Cross-Sectional Study in China. J. Nutr. Health Aging 2020, 24, 500–506. [Google Scholar] [CrossRef]
- Urquiza, M.; Fernandez, N.; Arrinda, I.; Sierra, I.; Irazusta, J.; Rodriguez Larrad, A. Nutritional Status is Associated with Function, Physical Performance and Falls in Older Adults Admitted to Geriatric Rehabilitation: A Retrospective Cohort Study. Nutrients 2020, 12, 2855. [Google Scholar] [CrossRef]
- Aparicio-Ugarriza, R.; Luzardo-Socorro, R.; Palacios, G.; Bibiloni, M.M.; Argelich, E.; Tur, J.A.; Gonzalez-Gross, M. What is the Relationship between Physical Fitness Level and Macro- and Micronutrient Intake in Spanish Older Adults? Eur. J. Nutr. 2019, 58, 1579–1590. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lengele, L.; Moehlinger, P.; Bruyere, O.; Locquet, M.; Reginster, J.Y.; Beaudart, C. Association between Changes in Nutrient Intake and Changes in Muscle Strength and Physical Performance in the SarcoPhAge Cohort. Nutrients 2020, 12, 3485. [Google Scholar] [CrossRef] [PubMed]
- Martinikorena, I.; Martinez-Ramirez, A.; Gomez, M.; Lecumberri, P.; Casas-Herrero, A.; Cadore, E.L.; Millor, N.; Zambom-Ferraresi, F.; Idoate, F.; Izquierdo, M. Gait Variability Related to Muscle Quality and Muscle Power Output in Frail Nonagenarian Older Adults. J. Am. Med. Dir. Assoc. 2016, 17, 162–167. [Google Scholar] [CrossRef]
- Foldvari, M.; Clark, M.; Laviolette, L.C.; Bernstein, M.A.; Kaliton, D.; Castaneda, C.; Pu, C.T.; Hausdorff, J.M.; Fielding, R.A.; Singh, M.A.F. Association of Muscle Power with Functional Status in Community-Dwelling Elderly Women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M192–M199. [Google Scholar] [CrossRef] [PubMed]
- Kozicka, I.; Kostka, T. Handgrip Strength, Quadriceps Muscle Power, and Optimal Shortening Velocity Roles in Maintaining Functional Abilities in Older Adults Living in a Long-Term Care Home: A 1-Year Follow-Up Study. Clin. Interv. Aging 2016, 11, 739–747. [Google Scholar] [CrossRef] [Green Version]
- Bonnefoy, M.; Jauffret, M.; Jusot, J.F. Muscle Power of Lower Extremities in Relation to Functional Ability and Nutritional Status in very Elderly People. J. Nutr. Health Aging 2007, 11, 223–228. [Google Scholar]
- Abizanda, P.; Lopez, M.D.; Garcia, V.P.; Estrella Jde, D.; da Silva Gonzalez, A.; Vilardell, N.B.; Torres, K.A. Effects of an Oral Nutritional Supplementation Plus Physical Exercise Intervention on the Physical Function, Nutritional Status, and Quality of Life in Frail Institutionalized Older Adults: The ACTIVNES Study. J. Am. Med. Dir. Assoc. 2015, 16, e9–e439. [Google Scholar] [CrossRef] [Green Version]
- Phu, S.; Boersma, D.; Duque, G. Exercise and Sarcopenia. J. Clin. Densitom. 2015, 18, 488–492. [Google Scholar] [CrossRef]
- Rus, G.E.; Porter, J.; Brunton, A.; Crocker, M.; Kotsimbos, Z.; Percic, J.; Polzella, L.; Willet, N.; Huggins, C.E. Nutrition Interventions Implemented in Hospital to Lower Risk of Sarcopenia in Older Adults: A Systematic Review of Randomised Controlled Trials. Nutr. Diet. 2020, 77, 90–102. [Google Scholar] [CrossRef]
- Marshall, R.N.; Smeuninx, B.; Morgan, P.T.; Breen, L. Nutritional Strategies to Offset Disuse-Induced Skeletal Muscle Atrophy and Anabolic Resistance in Older Adults: From Whole-Foods to Isolated Ingredients. Nutrients 2020, 12, 1533. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.Y.; Huang, K.S.; Chen, K.M.; Chou, C.P.; Tu, Y.K. Exercise, Nutrition, and Combined Exercise and Nutrition in Older Adults with Sarcopenia: A Systematic Review and Network Meta-Analysis. Maturitas 2021, 145, 38–48. [Google Scholar] [CrossRef]
- Valentini, A.; Federici, M.; Cianfarani, M.A.; Tarantino, U.; Bertoli, A. Frailty and Nutritional Status in Older People: The Mini Nutritional Assessment as a Screening Tool for the Identification of Frail Subjects. Clin. Interv. Aging 2018, 13, 1237–1244. [Google Scholar] [CrossRef] [Green Version]
- Artaza-Artabe, I.; Saez-Lopez, P.; Sanchez-Hernandez, N.; Fernandez-Gutierrez, N.; Malafarina, V. The Relationship between Nutrition and Frailty: Effects of Protein Intake, Nutritional Supplementation, Vitamin D and Exercise on Muscle Metabolism in the Elderly. A Systematic Review. Maturitas 2016, 93, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zuniga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and Interventions for Sarcopenia in Ageing Adults: A Systematic Review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Lopez, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodriguez-Villamil, J.L.; Millan-Calenti, J.C. Nutritional Determinants of Frailty in Older Adults: A Systematic Review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [Green Version]
- Zupo, R.; Castellana, F.; Bortone, I.; Griseta, C.; Sardone, R.; Lampignano, L.; Lozupone, M.; Solfrizzi, V.; Castellana, M.; Giannelli, G.; et al. Nutritional Domains in Frailty Tools: Working Towards an Operational Definition of Nutritional Frailty. Ageing Res. Rev. 2020, 64, 101148. [Google Scholar] [CrossRef] [PubMed]
- Echeverria, I.; Amasene, M.; Urquiza, M.; Labayen, I.; Anaut, P.; Rodriguez-Larrad, A.; Irazusta, J.; Besga, A. Multicomponent Physical Exercise in Older Adults After Hospitalization: A Randomized Controlled Trial Comparing Short- Vs. Long-Term Group-Based Interventions. Int. J. Environ. Res. Public. Health. 2020, 17, 666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.M.; Christensen, A.G.; Hansen, B.S.; Damsbo-Svendsen, S.; Moller, T.K. Multidisciplinary Nutritional Support for Undernutrition in Nursing Home and Home-Care: A Cluster Randomized Controlled Trial. Nutrition 2016, 32, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Pillard, F.; Klapouszczak, A.; Reynish, E.; Thomas, D.; Andrieu, S.; Riviere, D.; Vellas, B. Exercise Program for Nursing Home Residents with Alzheimer’s Disease: A 1-Year Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2007, 55, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Maltais, M.; Rolland, Y.; Hay, P.E.; Armaingaud, D.; Cestac, P.; Rouch, L.; de Souto Barreto, P. The Effect of Exercise and Social Activity Interventions on Nutritional Status in Older Adults with Dementia Living in Nursing Homes: A Randomised Controlled Trial. J. Nutr. Health Aging 2018, 22, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Senior, H.E.; Henwood, T.R.; Beller, E.M.; Mitchell, G.K.; Keogh, J.W. Prevalence and Risk Factors of Sarcopenia among Adults Living in Nursing Homes. Maturitas 2015, 82, 418–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensson, L.; Ek, A.C.; Unosson, M. Individually Adjusted Meals for Older People with Protein-Energy Malnutrition: A Single-Case Study. J. Clin. Nurs. 2001, 10, 491–502. [Google Scholar] [CrossRef]
- Allen, V.J.; Methven, L.; Gosney, M.A. Use of Nutritional Complete Supplements in Older Adults with Dementia: Systematic Review and Meta-Analysis of Clinical Outcomes. Clin. Nutr. 2013, 32, 950–957. [Google Scholar] [CrossRef]
- Papadopoulou, S.K. Sarcopenia: A Contemporary Health Problem among Older Adult Populations. Nutrients 2020, 12, 1293. [Google Scholar] [CrossRef]
- Franzke, B.; Neubauer, O.; Cameron-Smith, D.; Wagner, K.H. Dietary Protein, Muscle and Physical Function in the very Old. Nutrients 2018, 10, 935. [Google Scholar] [CrossRef] [Green Version]
- Bosaeus, I.; Rothenberg, E. Nutrition and Physical Activity for the Prevention and Treatment of Age-Related Sarcopenia. Proc. Nutr. Soc. 2016, 75, 174–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, H.; Fukushima, H.; Miwa, Y.; Shiraki, M.; Gomi, I.; Saito, M.; Mawatari, K.; Kobayashi, H.; Kato, M.; Moriwaki, H. A Longitudinal Study on the Nutritional State of Elderly Women at a Nursing Home in Japan. Intern. Med. 2006, 45, 1113–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poehlman, E.T.; Dvorak, R.V. Energy Expenditure, Energy Intake, and Weight Loss in Alzheimer Disease. Am. J. Clin. Nutr. 2000, 71, 650S–655S. [Google Scholar] [CrossRef] [Green Version]
- Diekmann, R.; Winning, K.; Uter, W.; Kaiser, M.J.; Sieber, C.C.; Volkert, D.; Bauer, J.M. Screening for Malnutrition among Nursing Home Residents—A Comparative Analysis of the Mini Nutritional Assessment, the Nutritional Risk Screening, and the Malnutrition Universal Screening Tool. J. Nutr. Health Aging 2013, 17, 326–331. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Sample, n = 105 | |
|---|---|
| Women, n (%) | 57 (54.3) |
| Men, n (%) | 48 (45.7) |
| Age, n (%) | |
| 70–80 years | 23 (21.9) |
| 80–90 years | 46 (43.8) |
| >90 years | 36 (34.3) |
| MNA, n (%) | |
| Normal nutritional status | 78 (74.2) |
| Risk of malnutrition | 26 (24.8) |
| Malnutrition | 1 (1.0) |
| Charlson index (score ≥ 0) | 6.42 ± 1.86 |
| BMI (kg·m−2) | 29.28 ± 4.60 |
| Normal weight, n (%) | 17 (16.7) |
| Overweight, n (%) | 42 (41.2) |
| Obesity, n (%) | 42 (41.2) |
| Morbid obesity, n (%) | 1 (1) |
| Barthel Index (range 0–100) | 79.17 ± 16.61 |
| Handgrip strength (Kg) | 18.72 ± 7.61 |
| Timed Up and Go (s) | 27.05 ± 19.75 |
| SPPB (range 0–12) | 6.90 ± 2.86 |
| Absolute muscle power (W) | 149.78 ± 72.11 |
| APAFOP score | 25.29 ± 1.09 |
| Fried’s frailty phenotype (range 0–5) | 2.54 ± 1.38 |
| Not frail, n (%) | 45 (42.9) |
| Frail, n (%) | 60 (57.1) |
| Rockwood Clinical Frailty Scale (range 0–9) | 3.93 ± 1.41 |
| Not frail, n (%) | 92 (87.6) |
| Frail, n (%) | 13 (12.4) |
| Tilburg Frailty Indicator (range 0–15) | 4.42 ± 3.16 |
| Not frail, n (%) | 55 (52.4) |
| Frail, n (%) | 50 (47.6) |
| β | Standardized β | p-Value | R2 | |
|---|---|---|---|---|
| Intercept | 0.003 | 0.998 | 0.314 | |
| BMI (kg·m−2) | 0.150 | 0.301 | 0.002 | |
| Barthel Index score | 0.050 | 0.220 | 0.039 | |
| APAFOP score | 0.746 | 0.386 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mugica-Errazquin, I.; Zarrazquin, I.; Seco-Calvo, J.; Gil-Goikouria, J.; Rodriguez-Larrad, A.; Virgala, J.; Arizaga, N.; Matilla-Alejos, B.; Irazusta, J.; Kortajarena, M. The Nutritional Status of Long-Term Institutionalized Older Adults Is Associated with Functional Status, Physical Performance and Activity, and Frailty. Nutrients 2021, 13, 3716. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113716
Mugica-Errazquin I, Zarrazquin I, Seco-Calvo J, Gil-Goikouria J, Rodriguez-Larrad A, Virgala J, Arizaga N, Matilla-Alejos B, Irazusta J, Kortajarena M. The Nutritional Status of Long-Term Institutionalized Older Adults Is Associated with Functional Status, Physical Performance and Activity, and Frailty. Nutrients. 2021; 13(11):3716. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113716
Chicago/Turabian StyleMugica-Errazquin, Itxaso, Idoia Zarrazquin, Jesús Seco-Calvo, Javier Gil-Goikouria, Ana Rodriguez-Larrad, Janire Virgala, Nagore Arizaga, Beatriz Matilla-Alejos, Jon Irazusta, and Maider Kortajarena. 2021. "The Nutritional Status of Long-Term Institutionalized Older Adults Is Associated with Functional Status, Physical Performance and Activity, and Frailty" Nutrients 13, no. 11: 3716. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113716