
Content Validation of a Chrononutrition Questionnaire for the General and Shift Work Populations: A Delphi Study

 , , , and
, , , and
Abstract
:1. Introduction
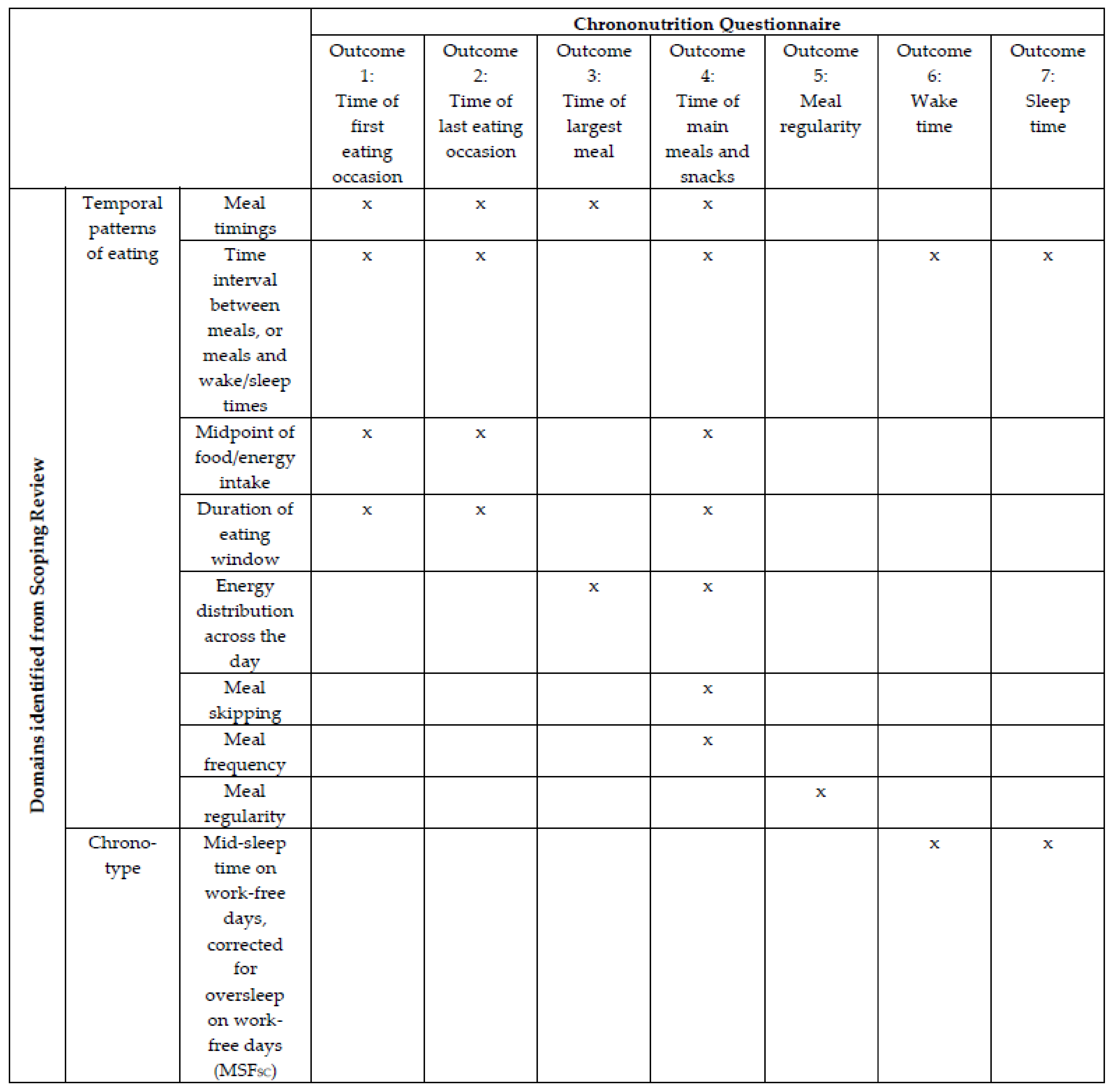
Development of a Chrononutrition Questionnaire
2. Materials and Methods
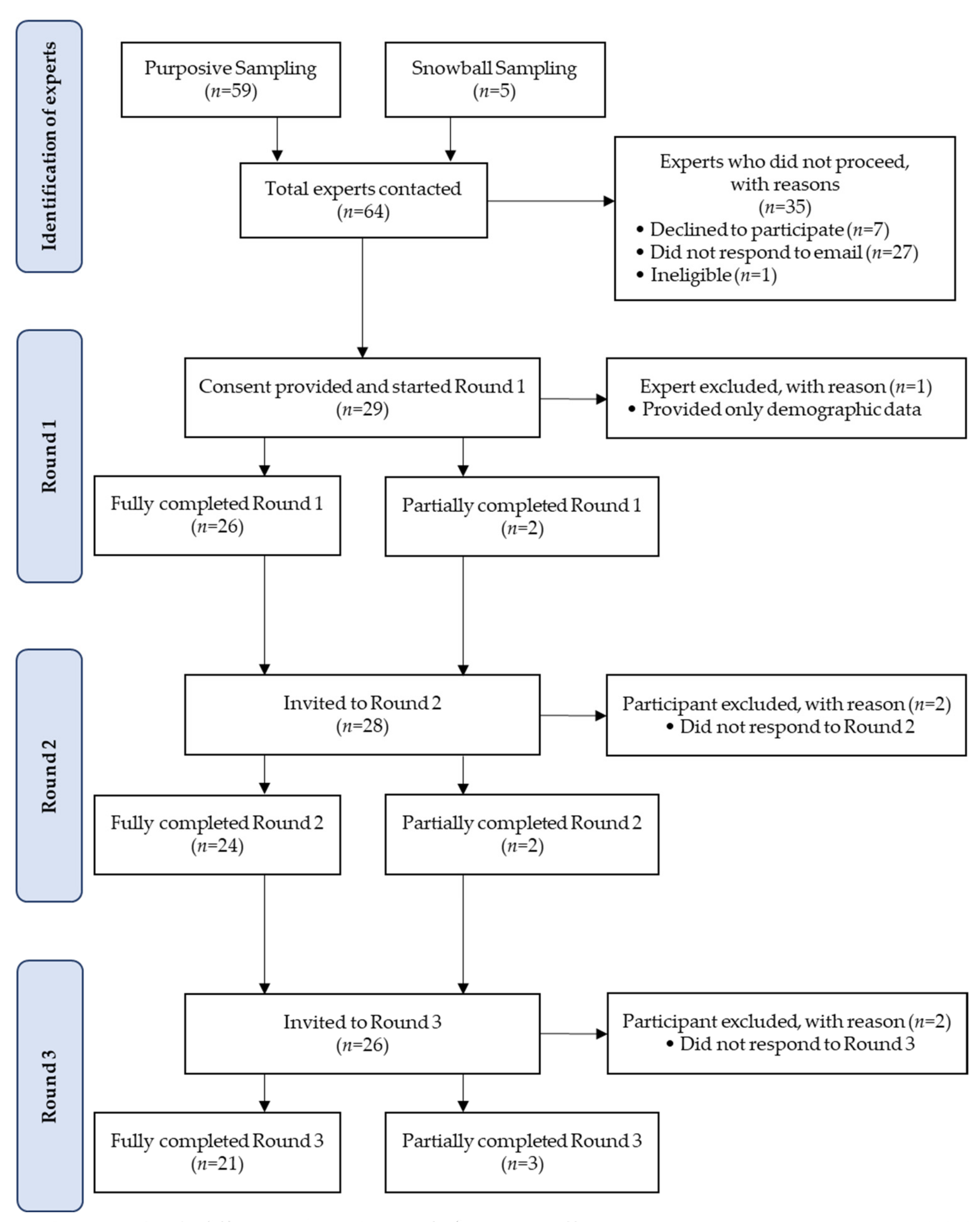
2.1. Recruitment
2.2. Data Collection and Management
2.3. Data Analysis
3. Results
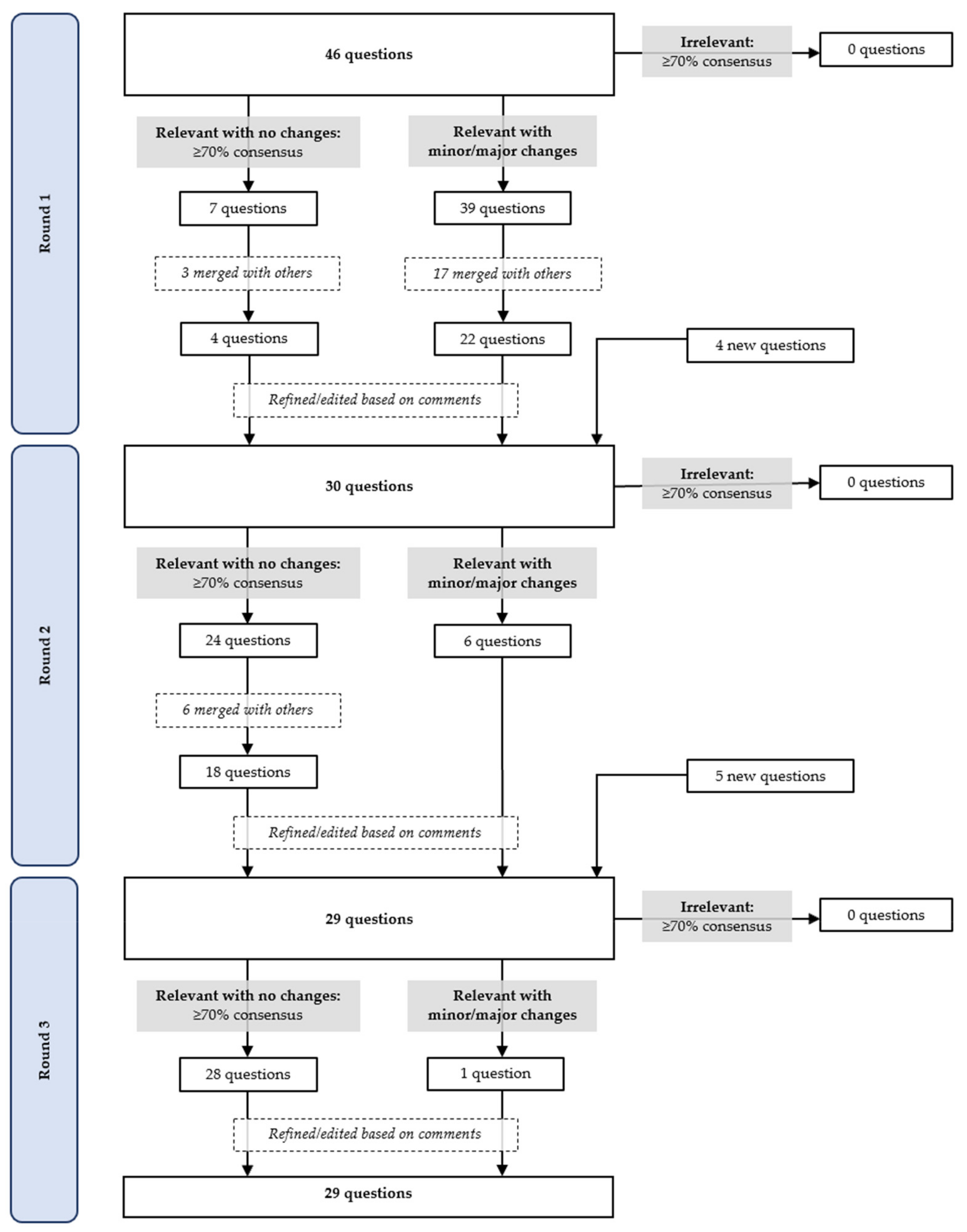
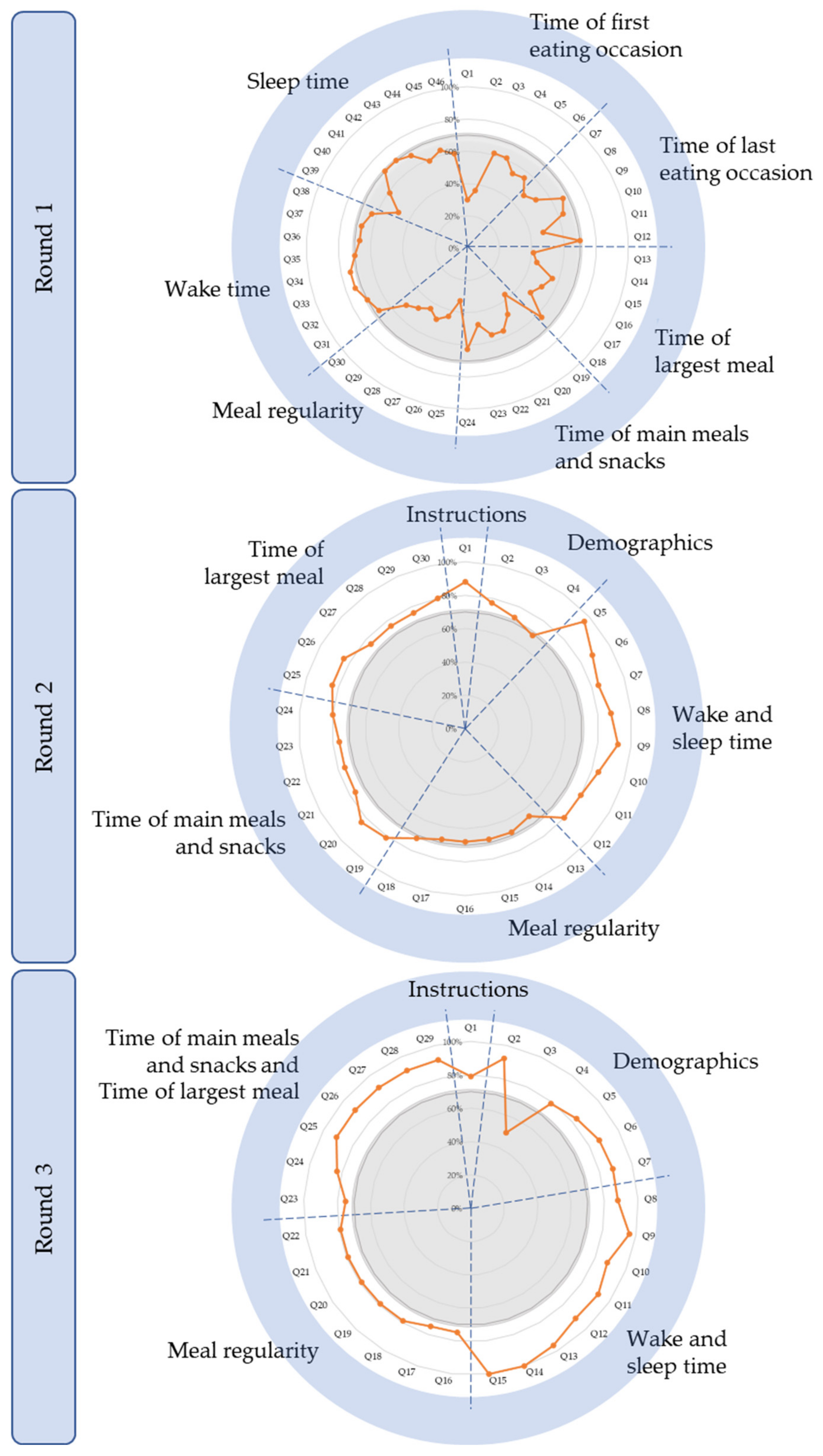
3.1. Delphi Round 1
3.2. Delphi Round 2
3.3. Delphi Round 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poggiogalle, E.; Jamshed, H.; Peterson, C.M. Circadian regulation of glucose, lipid, and energy metabolism in humans. Metabolism 2018, 84, 11–27. [Google Scholar] [CrossRef] [Green Version]
- Allada, R.; Bass, J. Circadian Mechanisms in Medicine. N. Engl. J. Med. 2021, 384, 550–561. [Google Scholar] [CrossRef]
- Johnston, J.D.; Ordovás, J.M.; Scheer, F.A.; Turek, F.W. Circadian Rhythms, Metabolism, and Chrononutrition in Rodents and Humans. Adv. Nutr. 2016, 7, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Baron, K.G.; Reid, K.J. Circadian misalignment and health. Int. Rev. Psychiatry 2014, 26, 139–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, C.J.; Purvis, T.E.; Hu, K.; Scheer, F.A. Circadian misalignment increases cardiovascular disease risk factors in humans. Proc. Natl. Acad. Sci. USA 2016, 113, E1402–E1411. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Australian Labour Market Statistics. Available online: https://www.abs.gov.au/ausstats/[email protected]/featurearticlesbyCatalogue/5461A9DAE97FF759CA2578C300153388?OpenDocument (accessed on 16 June 2021).
- Wyse, C.A.; Celis Morales, C.A.; Graham, N.; Fan, Y.; Ward, J.; Curtis, A.M.; Mackay, D.; Smith, D.J.; Bailey, M.E.S.; Biello, S.; et al. Adverse metabolic and mental health outcomes associated with shiftwork in a population-based study of 277,168 workers in UK biobank. Ann. Med. 2017, 49, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Adan, A. Chronotype, 2nd ed.; Elsevier Ltd.: Amsterdam, The Netherlands, 2015; pp. 568–573. [Google Scholar] [CrossRef]
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social jetlag: Misalignment of biological and social time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef]
- Fabbian, F.; Zucchi, B.; De Giorgi, A.; Tiseo, R.; Boari, B.; Salmi, R.; Cappadona, R.; Gianesini, G.; Bassi, E.; Signani, F.; et al. Chronotype, gender and general health. Chronobiol. Int. 2016, 33, 863–882. [Google Scholar] [CrossRef]
- Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Mat Ludin, A.F. The association between chronotype and dietary pattern among adults: A scoping review. Int. J. Environ. Res. Public Health 2019, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- De Assis, M.A.; Kupek, E.; Nahas, M.V.; Bellisle, F. Food intake and circadian rhythms in shift workers with a high workload. Appetite 2003, 40, 175–183. [Google Scholar] [CrossRef]
- Shaw, E.; Dorrian, J.; Coates, A.M.; Leung, G.K.W.; Davis, R.; Rosbotham, E.; Warnock, R.; Huggins, C.E.; Bonham, M.P. Temporal pattern of eating in night shift workers. Chronobiol. Int. 2019, 36, 1613–1625. [Google Scholar] [CrossRef]
- Sato, M.; Nakamura, K.; Ogata, H.; Miyashita, A.; Nagasaka, S.; Omi, N.; Yamaguchi, S.; Hibi, M.; Umeda, T.; Nakaji, S.; et al. Acute effect of late evening meal on diurnal variation of blood glucose and energy metabolism. Obes. Res. Clin. Pract. 2011, 5, e169–e266. [Google Scholar] [CrossRef]
- Lopez-Minguez, J.; Saxena, R.; Bandín, C.; Scheer, F.A.; Garaulet, M. Late dinner impairs glucose tolerance in MTNR1B risk allele carriers: A randomized, cross-over study. Clin. Nutr. 2018, 37, 1133–1140. [Google Scholar] [CrossRef]
- Bonham, M.P.; Kaias, E.; Zimberg, I.; Leung, G.K.W.; Davis, R.; Sletten, T.L.; Windsor-Aubrey, H.; Huggins, C.E. Effect of night time eating on postprandial triglyceride metabolism in healthy adults: A systematic literature review. J. Biol. Rhythm. 2019, 34, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Gan, Y.; Yang, C.; Tong, X.; Sun, H.; Cong, Y.; Yin, X.; Li, L.; Cao, S.; Dong, X.; Gong, Y.; et al. Shift work and diabetes mellitus: A meta-analysis of observational studies. Occup. Environ. Med. 2015, 72, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Merikanto, I.; Lahti, T.; Puolijoki, H.; Vanhala, M.; Peltonen, M.; Laatikainen, T.; Vartiainen, E.; Salomaa, V.; Kronholm, E.; Partonen, T. Associations of chronotype and sleep with cardiovascular diseases and type 2 diabetes. Chronobiol. Int. 2013, 30, 470–477. [Google Scholar] [CrossRef]
- Roenneberg, T.; Allebrandt, K.V.; Merrow, M.; Vetter, C. Social jetlag and obesity. Curr. Biol. 2012, 22, 939–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vyas, M.V.; Garg, A.X.; Iansavichus, A.V.; Costella, J.; Donner, A.; Laugsand, L.E.; Janszky, I.; Mrkobrada, M.; Parraga, G.; Hackam, D.G. Shift work and vascular events: Systematic review and meta-analysis. BMJ Br. Med. J. 2012, 345, e4800. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, A.; Bechtold, D.A.; Pot, G.K.; Johnston, J.D. Chrono-nutrition: From molecular and neuronal mechanisms to human epidemiology and timed feeding patterns. J. Neurochem. 2021, 157, 53–72. [Google Scholar] [CrossRef]
- Almoosawi, S.; Vingeliene, S.; Gachon, F.; Voortman, T.; Palla, L.; Johnston, J.D.; Van Dam, R.M.; Darimont, C.; Karagounis, L.G. Chronotype: Implications for epidemiologic studies on chrono-nutrition and cardiometabolic health. Adv. Nutr. 2019, 10, 30–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regmi, P.; Heilbronn, L.K. Time-Restricted Eating: Benefits, Mechanisms, and Challenges in Translation. iScience 2020, 23, 101161. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K. Meal timing and frequency: Implications for cardiovascular disease prevention: A scientific statement from the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- Boateng, G.; Neilands, T.; Frongillo, E.; Melgar-Quinonez, H.; Young, S. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research:A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Phoi, Y.Y.; Rogers, M.; Bonham, M.P.; Dorrian, J.; Coates, A.M. A scoping review of chronotype and temporal patterns of eating of adults: Tools used, findings, and future directions. Nutr. Res. Rev. 2021, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T. Having trouble typing? What on earth is chronotype? J. Biol. Rhythm. 2015, 30, 487–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juda, M.; Vetter, C.; Roenneberg, T. The Munich ChronoType Questionnaire for Shift-workers (MCTQShift). J. Biol. Rhythm. 2013, 28, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Goodman, C.M. The Delphi technique: A critique. J. Adv. Nurs. 1987, 12, 729–734. [Google Scholar] [CrossRef]
- Freitas, Â.; Santana, P.; Oliveira, M.; Almendra, R. Indicators for evaluating European population health: A Delphi selection process. BMC Public Health 2018, 18, 557. [Google Scholar] [CrossRef]
- von der Gracht, H.A. Consensus measurement in Delphi studies: Review and implications for future quality assurance. Technol. Forecast. Soc. Chang. 2012, 79, 1525–1536. [Google Scholar] [CrossRef]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [CrossRef] [Green Version]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef] [Green Version]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Keeney, S.; Hasson, F.; McKenna, H. Consulting the oracle: Ten lessons from using the Delphi technique in nursing research. J. Adv. Nurs. 2006, 53, 205–212. [Google Scholar] [CrossRef]
- Keeney, S.; McKenna, H.; Hasson, F. The Delphi Technique in Nursing and Health Research; John Wiley & Sons, Incorporated: Chicester, UK, 2011. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Lynn, R.M. Determination and Quantification Of Content Validity. Nurs. Res. 1986, 35, 382–386. [Google Scholar] [CrossRef]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]
- Rayens, M.K.; Hahn, E.J. Building Consensus Using the Policy Delphi Method. Policy Politics Nurs. Pract. 2000, 1, 308–315. [Google Scholar] [CrossRef]
- Veziari, Y.; Kumar, S.; Leach, M. The development of a survey instrument to measure the barriers to the conduct and application of research in complementary and alternative medicine: A Delphi study. BMC Complementary Altern. Med. 2018, 18, 335. [Google Scholar] [CrossRef]
- Grant, J.S.; Davis, L.L. Selection and use of content experts for instrument development. Res. Nurs. Health 1997, 20, 269–274. [Google Scholar] [CrossRef]
- Antcliff, D.; Keeley, P.; Campbell, M.; Oldham, J.; Woby, S. The development of an activity pacing questionnaire for chronic pain and/or fatigue: A Delphi technique. Physiotherapy 2013, 99, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Marot, L.P.; Rosa, D.E.; Lopes, T.d.V.C.; Moreno, C.R.d.C.; Crispim, C.A. Eating Duration throughout a Rotating Shift Schedule: A Case Study. J. Am. Coll. Nutr. 2021, 40, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Zeron-Rugerio, M.F.; Longo-Silva, G.; Hernaez, A.; Ortega-Regules, A.E.; Cambras, T.; Izquierdo-Pulido, M. The elapsed time between dinner and the midpoint of sleep is associated with adiposity in young women. Nutrients 2020, 12, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Q.; Garaulet, M.; Scheer, F. Meal timing and obesity: Interactions with macronutrient intake and chronotype. Int. J. Obes. 2019, 43, 1701–1711. [Google Scholar] [CrossRef] [PubMed]
- Kutsuma, A.; Nakajima, K.; Suwa, K. Potential Association between Breakfast Skipping and Concomitant Late-Night-Dinner Eating with Metabolic Syndrome and Proteinuria in the Japanese Population. Scientifica 2014, 2014, 253581. [Google Scholar] [CrossRef]
- Zitting, K.-M.; Vujovic, N.; Yuan, R.K.; Isherwood, C.M.; Medina, J.E.; Wang, W.; Buxton, O.M.; Williams, J.S.; Czeisler, C.A.; Duffy, J.F. Human Resting Energy Expenditure Varies with Circadian Phase. Curr. Biol. 2018, 28, 3685–3690.e3683. [Google Scholar] [CrossRef] [Green Version]
- Pot, G.K.; Almoosawi, S.; Stephen, A.M. Meal irregularity and cardiometabolic consequences: Results from observational and intervention studies. Proc. Nutr. Soc. 2016, 75, 475–486. [Google Scholar] [CrossRef]
- Sierra-Johnson, J.; Unden, A.L.; Linestrand, M.; Rosell, M.; Sjogren, P.; Kolak, M.; De Faire, U.; Fisher, R.M.; Hellenius, M.L. Eating meals irregularly: A novel environmental risk factor for the metabolic syndrome. Obesity 2008, 16, 1302–1307. [Google Scholar] [CrossRef]
- Shin, A.; Lim, S.-Y.; Sung, J.; Shin, H.-R.; Kim, J. Dietary Intake, Eating Habits, and Metabolic Syndrome in Korean Men. J. Am. Diet. Assoc. 2009, 109, 633–640. [Google Scholar] [CrossRef]
- Pot, G.K.; Hardy, R.; Stephen, A.M. Irregular consumption of energy intake in meals is associated with a higher cardiometabolic risk in adults of a British birth cohort. Int. J. Obes. 2014, 38, 1518–1524. [Google Scholar] [CrossRef] [Green Version]
- Farshchi, H.R.; Taylor, M.A.; Macdonald, I.A. Regular meal frequency creates more appropriate insulin sensitivity and lipid profiles compared with irregular meal frequency in healthy lean women. Eur. J. Clin. Nutr. 2004, 58, 1071–1077. [Google Scholar] [CrossRef]
- Farshchi, H.R.; Taylor, M.A.; Macdonald, I.A. Beneficial metabolic effects of regular meal frequency on dietary thermogenesis, insulin sensitivity, and fasting lipid profiles in healthy obese women. Am. J. Clin. Nutr. 2005, 81, 16–24. [Google Scholar] [CrossRef]
- Garaulet, M.; Madrid, J.A. Chronobiological aspects of nutrition, metabolic syndrome and obesity. Adv. Drug Deliv. Rev. 2010, 62, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Wainstein, J.; Ahren, B.; Bar-Dayan, Y.; Landau, Z.; Rabinovitz, H.R.; Froy, O. High-energy breakfast with low-energy dinner decreases overall daily hyperglycaemia in type 2 diabetic patients: A randomised clinical trial. Diabetologia 2015, 58, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Morgan, L.M.; Shi, J.W.; Hampton, S.M.; Frost, G. Effect of meal timing and glycaemic index on glucose control and insulin secretion in healthy volunteers. Br. J. Nutr. 2012, 108, 1286–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeCheminant, J.D.; Christenson, E.; Bailey, B.W.; Tucker, L.A. Restricting night-time eating reduces daily energy intake in healthy young men: A short-term cross-over study. Br. J. Nutr. 2013, 110, 2108–2113. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. 2018, 27, 1212–1221.e1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Almiron-Roig, E.; Rutters, F.; de Graaf, C.; Forde, C.G.; Tudur Smith, C.; Nolan, S.J.; Jebb, S.A. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. Am. J. Clin. Nutr. 2014, 100, 123–151. [Google Scholar] [CrossRef] [Green Version]
- Hurst, Y.; Fukuda, H. Effects of changes in eating speed on obesity in patients with diabetes: A secondary analysis of longitudinal health check-up data. BMJ Open 2018, 8, e019589. [Google Scholar] [CrossRef]
- Lee, J.S.; Mishra, G.; Hayashi, K.; Watanabe, E.; Mori, K.; Kawakubo, K. Combined eating behaviors and overweight: Eating quickly, late evening meals, and skipping breakfast. Eat. Behav. 2016, 21, 84–88. [Google Scholar] [CrossRef]
- Ohkuma, T.; Hirakawa, Y.; Nakamura, U.; Kiyohara, Y.; Kitazono, T.; Ninomiya, T. Association between eating rate and obesity: A systematic review and meta-analysis. Int. J. Obes. 2015, 39, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Paz-Graniel, I.; Babio, N.; Mendez, I.; Salas-Salvadó, J. Association between Eating Speed and Classical Cardiovascular Risk Factors: A Cross-Sectional Study. Nutrients 2019, 11, 83. [Google Scholar] [CrossRef] [Green Version]
- Tao, L.; Yang, K.; Huang, F.; Liu, X.; Li, X.; Luo, Y.; Wu, L.; Guo, X. Association between self-reported eating speed and metabolic syndrome in a Beijing adult population: A cross-sectional study. BMC Public Health 2018, 18, 855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spetter, M.S.; Mars, M.; Viergever, M.A.; de Graaf, C.; Smeets, P.A.M. Taste matters—Effects of bypassing oral stimulation on hormone and appetite responses. Physiol. Behav. 2014, 137, 9–17. [Google Scholar] [CrossRef]
- Sun, L.; Ranawana, D.V.; Tan, W.J.K.; Quek, Y.C.R.; Henry, C.J. The impact of eating methods on eating rate and glycemic response in healthy adults. Physiol. Behav. 2015, 139, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, N.; Mars, M.; de Wijk, R.A.; Westerterp-Plantenga, M.S.; de Graaf, C. The effect of viscosity on ad libitum food intake. Int. J. Obes. 2008, 32, 676–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Castro, J.M. Family and friends produce greater social facilitation of food intake than other companions. Physiol. Behav. 1994, 56, 445. [Google Scholar] [CrossRef]
- Hermans, R.C.; Lichtwarck-Aschoff, A.; Bevelander, K.E.; Herman, C.P.; Larsen, J.K.; Engels, R.C. Mimicry of food intake: The dynamic interplay between eating companions. PLoS ONE 2012, 7, e31027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumsion, T. The Delphi Technique: An Adaptive Research Tool. Br. J. Occup. Ther. 1998, 61, 153–156. [Google Scholar] [CrossRef]
- Bertéus Forslund, H.; Lindroos, A.K.; Sjöström, L.; Lissner, L. Meal patterns and obesity in Swedish women-a simple instrument describing usual meal types, frequency and temporal distribution. Eur. J. Clin. Nutr. 2002, 56, 740–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiuganji, N.M.; Nehme, P.; Marqueze, E.C.; Isherwood, C.M.; Martins, A.J.; Vasconcelos, S.; Cipolla-Neto, J.; Lowden, A.; Skene, D.J.; Moreno, C.R.C. Eating Behavior (Duration, Content, and Timing) Among Workers Living under Different Levels of Urbanization. Nutrients 2020, 12, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Objective | Does the Delphi study aim to address consensus? | Yes, by presenting results reflecting the level of consensus amongst members of the expert panel. |
| Participants | How will participants be selected or excluded? | Inclusion criteria:
|
| Consensus definition | How will consensus be defined? | Consensus is defined as ≥70% agreement. |
| Delphi process | Were items dropped? What criteria will be used to determine which items to drop? | No items were dropped, they were merged. Items will be dropped if there is ≥70% consensus on the rating “1: Irrelevant”. |
| What criteria will be used to determine to stop the Delphi process or will it be run for a specific number of rounds only? | The Delphi process will run for only three rounds. |
| n | % | ||
|---|---|---|---|
| Gender | Male | 5 | 18 |
| Female | 23 | 82 | |
| Age | 20–29 years | 4 | 14 |
| 30–39 years | 10 | 36 | |
| 40–49 years | 8 | 29 | |
| 50–59 years | 4 | 14 | |
| 60–69 years | 1 | 4 | |
| ≥70 years | 1 | 4 | |
| Current role | Academic | 28 | 100 |
| Clinician | 0 | 0 | |
| Highest education level | Bachelor’s degree | 1 | 4 |
| Master’s degree | 1 | 4 | |
| Doctorate degree | 26 | 93 | |
| Years of experience in the field of expertise | 1–5 years | 7 | 25 |
| 6–10 years | 8 | 29 | |
| 11–15 years | 3 | 11 | |
| 16–20 years | 3 | 11 | |
| >20 years | 7 | 25 | |
| Country of work | Australia | 11 | 39 |
| Brazil | 2 | 7 | |
| Canada | 1 | 4 | |
| Czech Republic | 1 | 4 | |
| Israel | 1 | 4 | |
| Netherlands | 2 | 7 | |
| United Kingdom | 4 | 14 | |
| United States | 6 | 21 | |
| Expert Suggestions and Comments | Changes Made or Clarifications | |
|---|---|---|
| Questionnaire instructions and requirements | Include instructions to participants, with a clear recall period. | New section: “Instructions to participants” as suggested. |
| Improve questionnaire format and layout. | As suggested, particularly:
| |
| Improve choice of wording | As suggested. | |
| Demographic data | Include questions about:
| New section: “Demographics”, to gather data as suggested. |
| Outcomes of interest | Instead of “weekdays” and weekends”, use “work/school” and “work-free/school-free days”. | As suggested. |
| Consider limitations of asking about sleep/wake patterns only on specific shift and free-day scenarios that not all shift workers have as part of their shift schedules. | Shift and free-day scenarios were based on the MCTQShift. It is acknowledged that shift workers whose shifts don’t align with these scenarios cannot be chronotyped. | |
| Determine alarm clock use for waking, as in the MCTQ (waking up without an alarm clock better indicates circadian phase and estimation of chronotype). | Participants asked to state wake up time if able to choose freely (without using an alarm clock and unaffected by children/pets, hobbies) following the ultra-short MCTQ and MCTQ. | |
| What is the time window for “day of a morning/afternoon/night shift” within which temporal patterns of eating are captured? | Updated definitions. | |
| Consider that timing of eating occasions “on a work-free day” for shift workers may be affected by the prior day’s shift type. | Updated to “on a work-free day after a work-free day” to minimise influence of the prior day’s shift type on timing of eating occasions. | |
| Will variation in timing of food intake within the same day type be captured? | Slight variations captured by asking about “typical” times. Otherwise, identified by question on regularity. | |
Better capture concept of regularity
|
| |
| Consider if one has two meals that are equally large. | Updated to ask about time of largest meal(s). | |
| Is defining largest meal by portion size too subjective? | No change (refer to Discussion). | |
| Instead of time of largest meal, consider time when most calories are consumed (drinks and snacks may contain more than a meal). | ||
| Refine definitions of terms. | As suggested. | |
| Additional outcomes to include |
| Not included. |
| Expert Suggestions and Comments | Changes Made or Clarifications | |
|---|---|---|
| Questionnaire instructions and requirements | Improve choice of wording. | As suggested. |
| Improve questionnaire format and layout. | As suggested, particularly:
| |
| Demographic data | Improve definition of “general population” as shift workers are technically within general population. | Removed, as redundant after addition of pathway questions. |
| Allow participants to state if they go to both work and school, and the start and end times of each. | As suggested. | |
| What does the term “school” refer to? | Adults who are studying. | |
| Include option for non-standard shifts beyond morning/evening/night shifts. | Added option for split shift workers (refer to Discussion). | |
| Outcomes of interest | Better capture concept of regularity:
|
|
| What if shift workers have more than one sleep episode in between shifts? | They will be asked to choose times of main sleep, not naps. If they have ≥2 sleeps that are of equal duration, they may choose one, to be validated against data from sleep diaries/actigraphy in a later study. | |
| One may not be able to freely choose wake up time unaffected by other factors (e.g., children/pets, hobbies). | Participants asked to specify wake up time without alarm clock use only. | |
| Preference of time window for “day of a morning/afternoon/night shift” within which temporal patterns of eating are captured to be limited by sleep/wake time before and after the shift instead of 12 a.m.–12 a.m. limits for morning shifts and 12 p.m.–12 p.m. limits for afternoon and night shifts. | As suggested. | |
| Aid identification of eating occasion (≥210 kJ) with a calorie counter. | ||
| Refine definitions of terms. | ||
| Additional outcomes to include | Food composition, as carbohydrate and fat-rich foods may be relevant in terms of timing of food intake. | Not included. |
| Expert Suggestions and Comments | Changes Made or Clarifications | |
|---|---|---|
| Questionnaire instructions and requirements | Improve choice of wording. | As suggested. |
| Demographic data | Provide definition for “work” to include both paid and unpaid work. | As suggested. |
| Provide definition for “school”. | ||
| “General population”: provide an option of “Other” for individuals do not go to work/school and are free to structure their day. | As suggested. | |
| “Shift work population”: provide more shift options to categorise participants. | ||
| Outcomes of interest | Better capture concept of regularity:
| No change (refer to Discussion). |
| Consider if an eating occasion lasts a long duration (e.g., a drink sipped over 3 h). | ||
| Refine definitions of terms within the questionnaire. | As suggested. | |
| Additional outcomes to include | Are meal breaks at work scheduled or dependent on workload? | Not included (refer to Discussion). |
| Other | Obtain mixed population feedback about language and burden of the questionnaire. | Considered. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phoi, Y.Y.; Bonham, M.P.; Rogers, M.; Dorrian, J.; Coates, A.M. Content Validation of a Chrononutrition Questionnaire for the General and Shift Work Populations: A Delphi Study. Nutrients 2021, 13, 4087. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114087
Phoi YY, Bonham MP, Rogers M, Dorrian J, Coates AM. Content Validation of a Chrononutrition Questionnaire for the General and Shift Work Populations: A Delphi Study. Nutrients. 2021; 13(11):4087. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114087
Chicago/Turabian StylePhoi, Yan Yin, Maxine P. Bonham, Michelle Rogers, Jillian Dorrian, and Alison M. Coates. 2021. "Content Validation of a Chrononutrition Questionnaire for the General and Shift Work Populations: A Delphi Study" Nutrients 13, no. 11: 4087. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114087