
Do Temporal Eating Patterns Differ in Healthy versus Unhealthy Overweight/Obese Individuals?

 ,
, 
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling Method
2.2. Adiposity and Biochemical Parameters
2.3. Determination of Metabolic Health Status
2.4. Dietary Intake and Timing
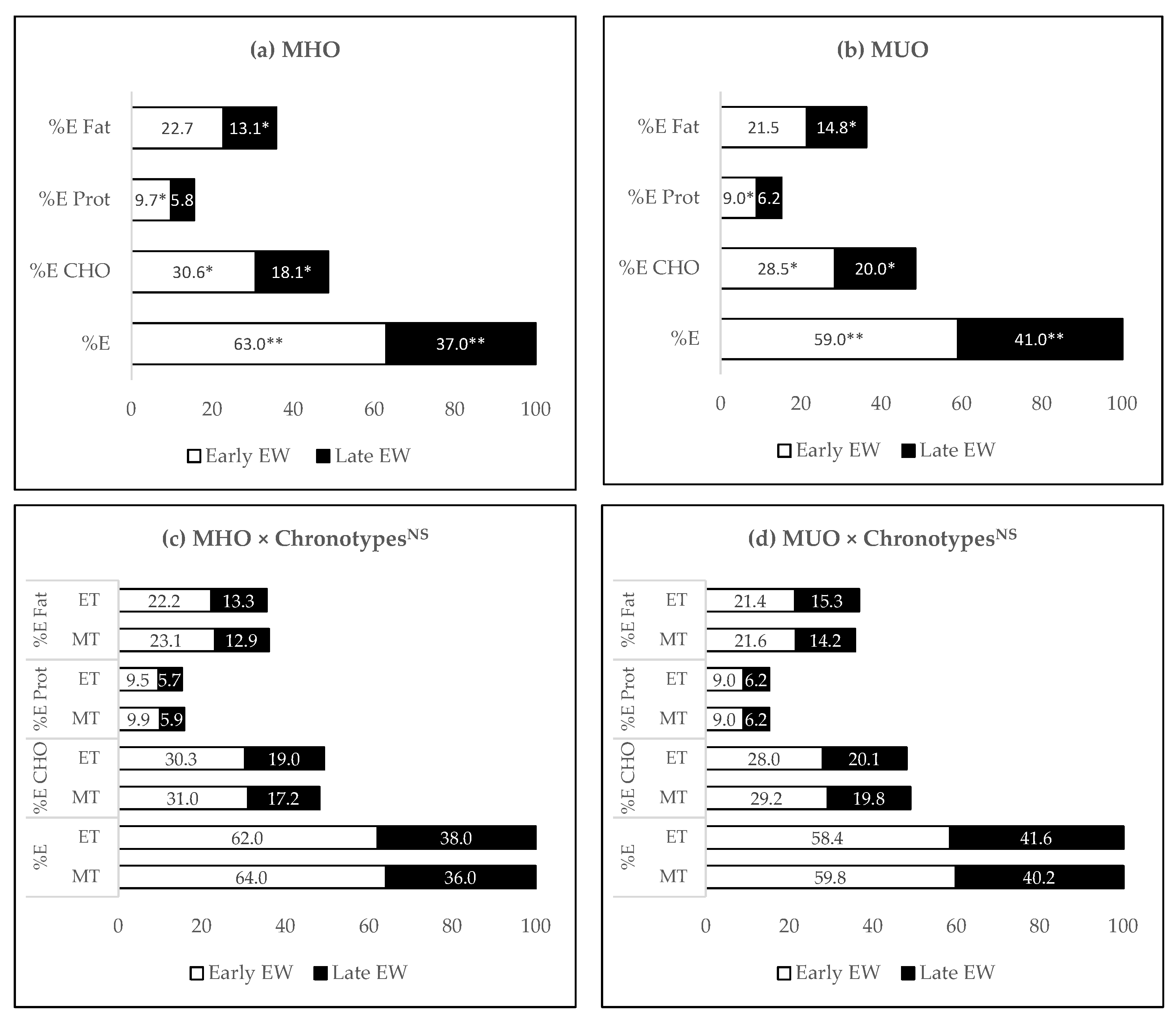
- Energy intake (kcal) during early window = the sum of energy intake before midpoint of eating. Thus, %E intake during early window = [(energy intake (kcal) during early window ÷ total energy intake) × 100]. The same calculation method was applied for intake in the late window.
- For example, carbohydrate intake early window = the sum of carbohydrate intake before the midpoint of eating. Thus, %E from carbohydrate intake during early window = [((carbohydrate intake (g) during early window × 4 kcal) ÷ total energy intake) × 100]. The same calculation method was applied for the intake in the late window and applied to other macronutrient (e.g., protein and fat) intake.
2.5. Night Eating Syndrome
2.6. Chronotypes and Physical Activity
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NCDRF Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Ford, N.D.; Patel, S.A.; Narayan, K.V. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malnick, S.D.H.; Knobler, H. The medical complications of obesity. J. Assoc. Physicians 2006, 99, 565–579. [Google Scholar] [CrossRef] [Green Version]
- Iacobini, C.; Pugliese, G.; Blasetti Fantauzzi, C.; Federici, M.; Menini, S. Metabolically healthy versus metabolically unhealthy obesity. Metabolism 2019, 92, 51–60. [Google Scholar] [CrossRef]
- Rusali, R.; Manaf, Z.A.; Shahar, S.; Mazri, F.H.; Ibrahim, N.; Ludin, A.F.M.; Singh, D.K.A.; Ali, N.M. Comparison of the Effectiveness of Online and Face-to-Face Weight-loss Interventations in the Workplace: Evidence from Malaysia. Sains Malays. 2018, 47, 2437–2445. [Google Scholar] [CrossRef]
- Stanton, M.; Robinson, J.L.; Kirkpatrick, S.M.; Farzinkhou, S.; Avery, E.C.; Rigdon, J.; Offringa, L.C.; Trepanowski, J.F.; Hauser, M.E.; Hartle, J.C.; et al. DIETFITS study (diet intervention examining the factors interacting with treatment success)—Study design and methods. Contemp. Clin. Trials 2017, 53, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Basir, S.A.; Manaf, Z.A.; Ahmad, M.; Kadir, N.A.; Ismail, W.; Ludin, A.M.; Shahar, S. Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults. Int. J. Environ. Res. Public Health 2021, 18, 1021. [Google Scholar] [CrossRef] [PubMed]
- Mazri, F.H.; Malaysia, U.K.; Shahar, S.; Kosai, N.R.; Omar, M.A.; Ramilis, N.; Rajan, R.; Centre, U.K.M.M. A retrospective study of weight-loss predictors following bariatric surgery in Malaysian patients with obesity. Malays. J. Nutr. 2020, 25, 423–433. [Google Scholar] [CrossRef]
- Nordmo, M.; Danielsen, Y.S.; Nordmo, M. The challenge of keeping it off, a descriptive systematic review of high-quality, follow-up studies of obesity treatments. Obes. Rev. 2020, 21, e12949. [Google Scholar] [CrossRef]
- Blüher, M. Metabolically healthy obesity. Endocr. Rev. 2020, 41, 405–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- April-Sanders, A.K.; Rodriguez, C.J. Metabolically Healthy Obesity Redefined. JAMA Netw. Open 2021, 4, e218860. [Google Scholar] [CrossRef]
- Vilela, D.L.; Fonseca, P.G.; Pinto, S.L.; Bressan, J. Influence of dietary patterns on the metabolically healthy obesity phenotype: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2779–2791. [Google Scholar] [CrossRef] [PubMed]
- Stelmach-Mardas, M.; Walkowiak, J. Dietary Interventions and Changes in Cardio-Metabolic Parameters in Metabolically Healthy Obese Subjects: A Systematic Review with Meta-Analysis. Nutrients 2016, 8, 455. [Google Scholar] [CrossRef] [Green Version]
- Crispim, C.A.; Mota, M.C. New perspectives on chrononutrition. Biol. Rhythm. Res. 2019, 50, 63–77. [Google Scholar] [CrossRef]
- Pot, G.K. Chrono-nutrition—An emerging, modifiable risk factor for chronic disease? Nutr. Bull. 2021. [Google Scholar] [CrossRef]
- Hawley, J.A.; Sassone-Corsi, P.; Zierath, J.R. Chrono-nutrition for the prevention and treatment of obesity and type 2 diabetes: From mice to men. Diabetologia 2020, 63, 2253–2259. [Google Scholar] [CrossRef]
- Thomas, E.A.; Zaman, A.; Cornier, M.-A.; Catenacci, V.A.; Tussey, E.J.; Grau, L.; Arbet, J.; Broussard, J.L.; Rynders, C.A. Later Meal and Sleep Timing Predicts Higher Percent Body Fat. Nutrients 2020, 13, 73. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.S.; Gómez-Abellán, P.; Qian, J.; Esteban, A.; Morales, E.; Scheer, F.A.J.L.; Garaulet, M. Late eating is associated with cardiometabolic risk traits, obesogenic behaviors, and impaired weight loss. Am. J. Clin. Nutr. 2021, 113, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Torres-Castillo, N.; Martinez-Lopez, E.; Vizmanos-Lamotte, B.; Garaulet, M. Healthy Obese Subjects Differ in Chronotype, Sleep Habits, and Adipose Tissue Fatty Acid Composition from Their Non-Healthy Counterparts. Nutrients 2020, 13, 119. [Google Scholar] [CrossRef]
- Goday, A.; Calvo, E.; Vázquez, L.A.; Caveda, E.; Margallo, T.; Catalina-Romero, C.; Reviriego, J. Prevalence and clinical characteristics of metabolically healthy obese individuals and other obese/non-obese metabolic phenotypes in a working population: Results from the Icaria study. BMC Public Health 2016, 16, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Ludin, A.F.M. The Association between Chronotype and Dietary Pattern among Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Maukonen, M.; Kanerva, N.; Partonen, T.; Kronholm, E.; Tapanainen, H.; Kontto, J.; Männistö, S. Chronotype differences in timing of energy and macronutrient intakes: A population-based study in adults. Obesity 2017, 25, 608–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseinpanah, F.; Tasdighi, E.; Barzin, M.; Mahdavi, M.; Ghanbarian, A.; Valizadeh, M.; Azizi, F. The association between transition from metabolically healthy obesity to metabolic syndrome, and incidence of cardiovascular disease: Tehran lipid and glucose study. PLoS ONE 2020, 15, e0239164. [Google Scholar] [CrossRef]
- Pan, W.-H.; Yeh, W.-T. How to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: An extension of Asian-Pacific recommendations. Asia Pac. J. Clin. Nutr. 2008, 17, 370. [Google Scholar] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Shahar, S.; Earland, J.; Abdulrahman, S. Validation of a Dietary History Questionnaire against a 7-D Weighed Record for Estimating Nutrient Intake among Rural Elderly Malays. Malays. J. Nutr. 2000, 6, 33–44. [Google Scholar]
- Shahar, S.; Safii, N.S.; Abdul Manaf, Z.; Haron, H. Atlas of Food Exchanges and Portion Sizes, 3rd ed.; MDC Publishers Sdn Bhd: Kuala Lumpur, Malaysia, 2015. [Google Scholar]
- Allison, K.C.; Lundgren, J.D.; O’Reardon, J.P.; Martino, N.S.; Sarwer, D.B.; Wadden, T.A.; Crosby, R.; Engel, S.G.; Stunkard, A.J. The Night Eating Questionnaire (NEQ): Psychometric properties of a measure of severity of the Night Eating Syndrome. Eat. Behav. 2008, 9, 62–72. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Mazri, M.F.H.; Manaf, Z.A.; Shahar, S.; Ludin, A.F.M.; Karim, N.A.; Ban, A.Y.-L.; Osman, R.A. Modified Munich chronotype questionnaire for application to short-interval split sleep of non-shift workers. Chronobiol. Int. 2021, 38, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between Clocks: Daily Temporal Patterns of Human Chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Q.; Garaulet, M.; Scheer, F.A.J.L. Meal timing and obesity: Interactions with macronutrient intake and chronotype. Int. J. Obes. 2019, 43, 1701–1711. [Google Scholar] [CrossRef]
- Soo, K.L.; Wan Abdul Manan, W.M.; Wan Suriati, W.N. The bahasa melayu version of the global physical activity questionnaire: Reliability and validity study in Malaysia. Asia-Pac. J. Public Health 2015, 27, NP184–NP193. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Makarem, N.; Sears, D.D.; St-Onge, M.-P.; Zuraikat, F.M.; Gallo, L.C.; Talavera, G.A.; Castaneda, S.F.; Lai, Y.; Mi, J.; Aggarwal, B. Habitual Nightly Fasting Duration, Eating Timing, and Eating Frequency are Associated with Cardiometabolic Risk in Women. Nutrients 2020, 12, 3043. [Google Scholar] [CrossRef] [PubMed]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High Caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Madjd, A.; Taylor, M.; Delavari, A.; Malekzadeh, R.; Macdonald, I.; Farshchi, H.R. Beneficial effect of high energy intake at lunch rather than dinner on weight loss in healthy obese women in a weight-loss program: A randomized clinical trial. Am. J. Clin. Nutr. 2016, 104, 982–989. [Google Scholar] [CrossRef] [Green Version]
- Maukonen, M.; Kanerva, N.; Partonen, T.; Männistö, S. Chronotype and energy intake timing in relation to changes in anthropometrics: A 7-year follow-up study in adults. Chronobiol. Int. 2018, 36, 27–41. [Google Scholar] [CrossRef]
- Lucassen, E.A.; Zhao, X.; Rother, K.I.; Mattingly, M.S.; Courville, A.B.; de Jonge, L.; Csako, G.; Cizza, G.; Sleep Extension Study Group. Evening Chronotype Is Associated with Changes in Eating Behavior, More Sleep Apnea, and Increased Stress Hormones in Short Sleeping Obese Individuals. PLoS ONE 2013, 8, e56519. [Google Scholar] [CrossRef] [Green Version]
- Taetzsch, A.; Roberts, S.B.; Bukhari, A.; Lichtenstein, A.H.; Gilhooly, C.H.; Martin, E.; Krauss, A.J.; Hatch-McChesney, A.; Das, S.K. Eating Timing: Associations with Dietary Intake and Metabolic Health. J. Acad. Nutr. Diet. 2021, 121, 738–748. [Google Scholar] [CrossRef]
- McHill, A.W.; Phillips, A.J.; A Czeisler, C.; Keating, L.; Yee, K.; Barger, L.K.; Garaulet, M.; Scheer, F.; Klerman, E.B. Later circadian timing of food intake is associated with increased body fat. Am. J. Clin. Nutr. 2017, 106, 1213–1219. [Google Scholar] [CrossRef]
- McHill, A.W.; Czeisler, C.A.; Phillips, A.J.K.; Keating, L.; Barger, L.K.; Garaulet, M.; Scheer, F.A.J.L.; Klerman, E.B. Caloric and Macronutrient Intake Differ with Circadian Phase and between Lean and Overweight Young Adults. Nutrients 2019, 11, 587. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Minguez, J.; Dashti, H.S.; Madrid-Valero, J.J.; Madrid, J.A.; Saxena, R.; Scheer, F.A.; Ordoñana, J.R.; Garaulet, M. Heritability of the timing of food intake. Clin. Nutr. 2019, 38, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Reid, K.J.; Baron, K.G.; Zee, P.C. Meal timing influences daily caloric intake in healthy adults. Nutr. Res. 2014, 34, 930–935. [Google Scholar] [CrossRef] [Green Version]
- Garaulet, M.; Gómez-Abellán, P.; Béjar, J.J.A.; Lee, Y.-C.; Ordovas, J.; Scheer, F. Timing of food intake predicts weight loss effectiveness. Int. J. Obes. 2013, 37, 604–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, A.; Bechtold, D.A.; Pot, G.K.; Johnston, J.D. Chrono-nutrition: From molecular and neuronal mechanisms to human epidemiology and timed feeding patterns. J. Neurochem. 2021, 157, 53–72. [Google Scholar] [CrossRef]
- Queiroz, J.D.N.; Macedo, R.C.O.; Tinsley, G.M.; Reischak-Oliveira, A. Time-restricted eating and circadian rhythms: The biological clock is ticking. Crit. Rev. Food Sci. Nutr. 2021, 61, 2863–2875. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.; Herzog, N.; Janka, S.; Baumann, T.; Kistenmacher, A.; Oltmanns, K.M. Twice as High Diet-Induced Thermogenesis After Breakfast vs Dinner On High-Calorie as Well as Low-Calorie Meals. J. Clin. Endocrinol. Metab. 2020, 105, e211–e221. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Fadda, M.; Castiglione, A.; Ciccone, G.; De Francesco, A.; Fedele, D.; Guggino, A.; Parasiliti-Caprino, M.; Ferrara, S.; Boggio, M.V.; et al. Is the timing of caloric intake associated with variation in diet-induced thermogenesis and in the metabolic pattern? A randomized cross-over study. Int. J. Obes. 2015, 39, 1689–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, C.J.; Garcia, J.I.; Myers, S.; Yang, J.N.; Trienekens, N.; Scheer, F.A. The Human Circadian System Has a Dominating Role in Causing the Morning/Evening Difference in Diet-Induced Thermogenesis. Obesity 2015, 23, 2053–2058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerterp, K.R. Diet induced thermogenesis. Nutr. Metab. 2004, 14, 1–5. [Google Scholar]
- Rynders, C.A.; Morton, S.J.; Bessesen, D.H.; Wright, K.P., Jr.; Broussard, J.L. Circadian Rhythm of Substrate Oxidation and Hormonal Regulators of Energy Balance. Obesity 2020, 28, S104–S113. [Google Scholar] [CrossRef]
- Zitting, K.-M.; Vujovic, N.; Yuan, R.K.; Isherwood, C.M.; Medina, J.E.; Wang, W.; Buxton, O.M.; Williams, J.S.; Czeisler, C.A.; Duffy, J.F. Human Resting Energy Expenditure Varies with Circadian Phase. Curr. Biol. 2018, 28, 3685–3690.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, C.J.; Yang, J.N.; Garcia, J.I.; Myers, S.; Bozzi, I.; Wang, W.; Buxton, O.; Shea, S.; Scheer, F.A.J.L. Endogenous circadian system and circadian misalignment impact glucose tolerance via separate mechanisms in humans. Proc. Natl. Acad. Sci. USA 2015, 112, E2225–E2234. [Google Scholar] [CrossRef] [Green Version]
- Qian, J.; Scheer, F.A. Circadian System and Glucose Metabolism: Implications for Physiology and Disease. Trends Endocrinol. Metab. 2016, 27, 282–293. [Google Scholar] [CrossRef] [Green Version]
- Qian, J.; Man, C.D.; Morris, C.J.; Cobelli, C.; Scheer, F. Differential effects of the circadian system and circadian misalignment on insulin sensitivity and insulin secretion in humans. Diabetes Obes. Metab. 2018, 20, 2481–2485. [Google Scholar] [CrossRef]
- Bandín, C.; Scheer, F.A.J.L.; Luque, A.J.; Ávila-Gandía, V.; Zamora, S.; Madrid, J.A.; Gómez-Abellán, P.; Garaulet, M. Meal timing affects glucose tolerance, substrate oxidation and circadian-related variables: A randomized, crossover trial. Int. J. Obes. 2015, 39, 828–833. [Google Scholar] [CrossRef]
- Hall, K.D. Did the Food Environment Cause the Obesity Epidemic? Obesity 2018, 26, 11–13. [Google Scholar] [CrossRef]
- Ali, N.; Ali, H.; Abdullah, M.A. Food security among the Urban Population in Malaysia. Issues of changing life style and risk. In Proceedings of the SEAGA International Conference on Transformations and Embodiments in Southeasth Asian (and Other) Geographies: Changing Environment, People and Cultural Groups, Institutions and Landscapes, Quezoncity, Philippines, 3–6 June 2008. [Google Scholar]
- Ali, N.; Abdullah, M.A. The food consumption and eating behaviour of Malaysian urbanites: Issues and concerns. Malays. J. Soc. Space 2012, 8, 157–165. [Google Scholar]
- Salleh, R.; Ganapathy, S.S.; Wong, N.I.; Cheong, S.M.; Ahmad, M.H.; Palaniveloo, L.; Othman, F.; Baharudin, A.; Radzi, M.R.M.; Selamat, R.; et al. Is socio-demographic status, body mass index, and consumption of food away from home associated with high sodium intake among adults in Malaysia?: Findings from the Malaysian Community Salt Survey (MyCoSS). J. Health Popul. Nutr. 2021, 40, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wellard-Cole, L.; Davies, A.; Allman-Farinelli, M. Contribution of foods prepared away from home to intakes of energy and nutrients of public health concern in adults: A systematic review. Crit. Rev. Food Sci. Nutr. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (N = 299) | MHO (n = 173) | MUO (n = 126) | p Value |
|---|---|---|---|---|
| Age a | 40.3 ± 6.9 | 39.8 ± 6.8 | 41.2 ± 6.9 | 0.078 |
| Gender b | ||||
| Women, n (%) | 220 (73.6) | 136 (61.8) | 84 (38.2) | 0.021 * |
| Men, n (%) | 79 (26.4) | 37 (46.8) | 42 (53.2) | |
| Marital status | ||||
| Married, n (%) | 256 (85.6) | 146 (57.0) | 110 (43.0) | 0.479 |
| Unmarried, n (%) | 43 (14.4) | 27 (62.8) | 16 (37.2) | |
| Ethnicity b | ||||
| Malay | 296 (99.0) | 172 (58.1) | 124 (41.9) | 0.387 |
| Chinese | 3 (1.0) | 1 (33.3) | 2 (66.7) | |
| Chronotypes b | ||||
| M-type, n (%) | 149 (49.8) | 88 (59.1) | 61 (40.9) | 0.675 |
| E-type, n (%) | 150 (50.2) | 85 (57.9) | 65 (43.3) | |
| Smoking status b | ||||
| Non-smoker/Ex-smoker, n (%) | 280 (96.6) | 163 (58.2) | 117 (41.8) | 0.252 |
| Smoker, n (%) | 10 (3.4) | 4 (40.0) | 6 (60.0) | |
| Hypertension, n (%) b | 39 (14.6) | 10 (25.6) | 29 (74.4) | <0.001 *** |
| Diabetes mellitus, n (%) b | 15 (5.6) | 1 (6.7) | 14 (93.3) | <0.001 *** |
| Dyslipidaemia, n (%) b | 30 (11.2) | 8 (26.7) | 22 (73.3) | <0.001 *** |
| Adiposity parameters c | ||||
| Weight (kg) | 80.89 ± 15.87 | 77.62 ± 1.01 | 86.28 ± 1.19 | <0.001 *** |
| BMI (kg/m2) | 31.59 ± 4.92 | 30.62 ± 0.36 | 33.24 ± 0.42 | <0.001 *** |
| Body fat (%) | 40.83 ± 7.58 | 39.81 ± 0.39 | 42.13 ± 0.46 | <0.001 *** |
| WC (cm) | 96.62 ± 12.17 | 94.62 ± 0.81 | 101.19 ± 0.96 | <0.001 *** |
| Biochemical parameters c | ||||
| FBG ᶧ (mmol/L) | 5.04 ± 1.15 | 4.75 ± 0.11 | 5.96 ± 0.13 | <0.001 *** |
| Insulin ᶤ (μIU/mL) | 11.55 ± 7.16 | 9.76 ± 0.56 | 15.52 ± 0.66 | <0.001 *** |
| HbA1c (%) ᶧ | 5.72 ± 0.91 | 5.52 ± 0.08 | 6.38 ± 0.09 | <0.001 *** |
| HOMA-IR ᶤ | 2.70 ± 2.41 | 2.06 ± 0.19 | 4.24 ± 0.22 | <0.001 *** |
| Total cholesterol (mmol/L) | 5.05 ± 0.92 | 5.08 ± 0.07 | 5.08 ± 0.08 | 0.999 |
| Triglyceride ᶧ (mmol/L) | 1.27 ± 0.78 | 1.03 ± 0.05 | 1.72 ± 0.06 | <0.001 *** |
| LDL-C (mmol/L) | 3.18 ± 0.80 | 3.19 ± 0.06 | 3.17 ± 0.08 | 0.828 |
| Non-HDL-C (mmol/L) | 3.75 ± 0.88 | 3.66 ± 0.07 | 3.92 ± 0.08 | 0.012 * |
| HDL-C (mmol/L) | 1.30 ± 0.30 | 1.41 ± 0.02 | 1.15 ± 0.02 | <0.001 *** |
| Uric acid (mmol/L) | 0.36 ± 0.09 | 0.36 ± 0.01 | 0.37 ± 0.01 | 0.085 |
| Blood pressure c | ||||
| Systolic (mmHg) | 123.67 ± 15.64 | 122.95 ± 1.12 | 129.93 ± 1.41 | <0.001 *** |
| Diastolic (mmHg) | 79.45 ± 12.99 | 76.58 ± 0.94 | 85.24 ± 1.1 | <0.001 *** |
| Characteristics | Total (N = 299) Mean ± SD | MHO (n = 173) Mean ± SE | MUO (n = 126) Mean ± SE | p Value |
|---|---|---|---|---|
| Sleep traits | ||||
| Sleep duration workdays (hour) | 6.2 ± 1.0 | 6.1 ± 0.1 | 6.2 ± 0.1 | 0.530 |
| Sleep duration free days (hour) | 6.7 ± 1.3 | 6.7 ± 0.1 | 6.6 ± 0.1 | 0.567 |
| MSW (local time) | 02:30 ± 0:44 | 02:28 ± 0:46 | 02:33 ± 0:41 | 0.227 |
| MSF (local time) | 02:55 ± 0:59 | 02:53 ± 1:01 | 02:57 ± 0:56 | 0.531 |
| Social jetlag (minute) | 30.9 ± 35.5 | 33.3 ± 2.7 | 27.6 ± 3.2 | 0.183 |
| Physical activity | ||||
| MET | 2203 ± 3190 | 1969 ± 250 | 2521 ± 293 | 0.162 |
| Night eating syndrome | ||||
| Score | 10.3 ± 4.8 | 10.2 ± 0.4 | 10.5 ± 0.5 | 0.635 |
| Total dietary intakes | ||||
| Energy intake (kcal/day) | 1850 ± 473 | 1819 ± 34 | 1893 ± 40 | 0.166 |
| Energy intake (kcal/kg BW) | 23.2 ± 6.2 | 23.0 ± 0.5 | 23.5 ± 0.5 | 0.453 |
| CHO (g/day) | 226.3 ± 66.7 | 222.3 ± 4.8 | 231.7 ± 5.6 | 0.212 |
| % E from CHO | 48.7 ± 6.5 | 48.9 ± 0.5 | 48.4 ± 0.6 | 0.457 |
| Protein (g/day) | 69.8 ± 17.2 | 69.2 ± 1.3 | 70.6 ± 1.5 | 0.480 |
| % E from protein | 15.3 ± 2.7 | 15.4 ± 0.2 | 15.2 ± 0.2 | 0.479 |
| Fat (g/day) | 74.0 ± 22.0 | 72.6 ± 1.6 | 76.0 ± 1.9 | 0.188 |
| % E from fat | 35.8 ± 5.4 | 35.6 ± 0.4 | 36.1 ± 0.5 | 0.511 |
| Meal timing | ||||
| First mealtime (local time) | 08:26 ± 0:51 | 08:31 ± 0:52 | 08:19 ± 0:48 | 0.099 |
| Last mealtime (local time) | 20:34 ± 1:30 | 20:41 ± 1:31 | 20:23 ± 1:28 | 0.110 |
| Midpoint of eating (local time) | 14:30 ± 0:55 | 14:36 ± 0:56 | 14:21 ± 0:53 | 0.037 * |
| Elapsed time between last meal and sleep onset (hour) | 3.0 ± 1.5 | 2.8 ± 0.1 | 3.2 ± 0.1 | 0.070 |
| Total eating window (hour) | 12.1 ± 1.6 | 12.2 ± 0.1 | 12.1 ± 0.1 | 0.571 |
| Characteristics | MHO (n = 173) | MUO (n = 126) | p Value | ||
|---|---|---|---|---|---|
| M-Type (n = 88) | E-Type (n = 85) | M-Type (n = 61) | E-Type (n = 65) | ||
| Sleep traits | |||||
| Sleep duration workdays (hour) | 6.3 ± 0.1 | 6.0 ± 0.1 | 6.4 ± 0.1 | 6.1 ± 0.1 | 0.810 |
| Sleep duration free days (hour) | 6.9 ± 0.1 | 6.5 ± 0.1 | 7.1 ± 0.2 | 6.2 ± 0.2 | 0.095 |
| MSW (local time) | 02:03 ± 0:38 | 02:53 ± 0:39 | 02:07 ± 0:29 | 02:57 ± 0:35 | 0.965 |
| MSF (local time) | 02:07 ± 0:39 | 03:41 ± 0:40 | 02:12 ± 0:31 | 03:40 ± 0:37 | 0.492 |
| Social jetlag (minute) | 20.1 ± 3.4 | 47.2 ± 3.5 | 12.7 ± 4.2 | 41.2 ± 4.0 | 0.850 |
| Physical activity | |||||
| MET | 2035 ± 349 | 1901 ± 356 | 2367 ± 420 | 2664 ± 404 | 0.567 |
| Night eating syndrome | |||||
| Score | 9.9 ± 0.5 | 10.6 ± 0.6 | 10.3 ± 0.6 | 10.7 ± 0.6 | 0.801 |
| Total dietary intakes | |||||
| Energy intake (kcal/day) | 1760 ± 47 | 1882 ± 47 | 1864 ± 56 | 1919 ± 54 | 0.505 |
| Energy intake (kcal/kg BW) | 22.2 ± 0.6 | 23.8 ± 0.6 | 22.8 ± 0.8 | 24.2 ± 0.7 | 0.828 |
| CHO (g/day) | 213.5 ± 6.6 | 231.5 ± 6.8 | 228.5 ± 8.0 | 234.6 ± 7.7 | 0.403 |
| % E from CHO | 48.7 ± 0.7 | 49.2 ± 0.7 | 49.0 ± 0.8 | 47.7 ± 0.8 | 0.210 |
| Protein (g/day) | 67.6 ± 1.7 | 70.9 ± 1.8 | 70.6 ± 2.1 | 70.6 ± 2.0 | 0.408 |
| % E from protein | 15.7 ± 0.3 | 15.2 ± 0.3 | 15.3 ± 0.4 | 15.1 ± 0.3 | 0.655 |
| Fat (g/day) | 70.5 ± 2.2 | 74.8 ± 2.3 | 74.4 ± 2.7 | 77.4 ± 2.6 | 0.798 |
| % E from fat | 35.7 ± 0.6 | 35.6 ± 0.6 | 35.8 ± 0.7 | 36.3 ± 0.7 | 0.585 |
| Meal timing | |||||
| First mealtime (local time) | 08:19 ± 0:51 | 08:44 ± 0:51 | 08:14 ± 0:50 | 08:24 ± 0:47 | 0.151 |
| Last mealtime (local time) | 20:20 ± 1:22 | 21:03 ± 1:36 | 20:10 ± 1:14 | 20:36 ± 1:38 | 0.433 |
| Midpoint of eating (local time) | 14:19 ± 0:47 | 14:54 ± 0:59 | 14:11 ± 0:45 | 14:30 ± 1:00 | 0.184 |
| Elapsed time between last meal and sleep onset (hour) | 2.6 ± 0.2 | 3.1 ± 0.2 | 2.8 ± 0.2 | 3.5 ± 0.2 | 0.523 |
| Total eating window (hour) | 12.0 ± 0.2 | 12.4 ± 0.2 | 11.9 ± 0.2 | 12.2 ± 0.2 | 0.832 |
| Percentile (Intake) | Range | Risk of MUO [OR (95% CI)] | ||||
|---|---|---|---|---|---|---|
| Overall (n = 299) | M-Type (n = 149) | E-Type (n = 150) | ||||
| Model 1 | Model 2 | Model 2 | Model 2 | |||
| EI Early EW | 25th | <893 kcal | 1.05 (0.52, 2.11) | 4.30 (1.41, 13.11) * | 8.40 (1.57, 44.86) * | 2.68 (0.55, 12.98) |
| 50th | 893–1165 kcal | 0.85 (0.43, 1.70) | 2.24 (0.88, 5.69) | 3.24 (0.79, 13.30) | 1.81 (0.51, 6.42) | |
| 75th | 1166–1384 kcal | 0.75 (0.38, 1.51) | 1.28 (0.58, 2.85) | 1.31 (0.40, 4.29) | 1.23 (0.40, 3.76) | |
| 100th | >1384 kcal | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |
| CHO Early EW | 25th | <107.0 g | 0.74 (0.37, 1.46) | 1.79 (0.68, 4.75) | 1.95 (0.48, 7.97) | 1.85 (0.46, 7.48) |
| 50th | 107.0–139.0 g | 0.90 (0.45, 1.79) | 1.82 (0.77, 4.30) | 1.82 (0.52, 6.42) | 1.87 (0.57, 6.16) | |
| 75th | 139.1–171.3 g | 0.51 (0.26, 1.02) | 0.66 (0.31, 1.42) | 0.42 (0.14, 1.28) | 0.96 (0.32, 2.82) | |
| 100th | >171.3 g | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |
| Protein Early EW | 25th | <35.4 g | 1.29 (0.64, 2.58) | 2.45 (0.99, 6.04) | 1.92 (0.55, 6.68) | 3.33 (0.84, 13.30) |
| 50th | 35.4–43.0 g | 0.93 (0.47, 1.85) | 1.62 (0.73, 3.61) | 1.43 (0.49, 4.20) | 1.80 (0.53, 6.16) | |
| 75th | 43.1–51.2 g | 0.99 (0.50, 1.97) | 1.19 (0.58, 2.55) | 0.54 (0.18, 1.64) | 2.33 (0.77, 7.04) | |
| 100th | >51.2 g | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |
| EI Late EW | 25th | <512 kcal | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| 50th | 512–728 kcal | 2.20 (1.08, 4.51) * | 2.38 (1.11, 5.13) * | 1.86 (0.65, 5.31) | 2.79 (0.81, 9.69) | |
| 75th | 729–892 kcal | 2.04 (0.99, 4.19) | 2.33 (1.03, 5.32) * | 3.69 (1.18, 11.58) * | 1.59 (0.43, 5.90) | |
| 100th | >892 kcal | 3.75 (1.82, 7.77) *** | 4.45 (1.71, 11.56) ** | 4.85 (1.44, 16.39) * | 4.53 (0.87, 23.58) | |
| CHO Late EW | 25th | <62.1 g | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| 50th | 62.1–85.0 g | 1.99 (0.98, 4.06) | 2.05 (0.96, 4.39) | 2.00 (0.69, 5.80) | 1.85 (0.58, 5.85) | |
| 75th | 85.1–109.5 g | 1.85 (0.90, 3.77) | 1.98 (0.89, 4.37) | 2.35 (0.82, 6.74) | 1.47 (0.42, 5.15) | |
| 100th | >109.5 g | 3.49 (1.69, 7.22) ** | 3.28 (1.31, 8.19) * | 5.56 (1.47, 21.02) * | 1.95 (0.50, 7.60) | |
| Fat Late EW | 25th | <21.3 g | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| 50th | 21.3–28.0 g | 1.32 (0.66, 2.65) | 1.19 (0.56, 2.53) | 0.98 (0.33, 2.93) | 1.31 (0.43, 4.02) | |
| 75th | 28.1–36.4 g | 1.79 (0.89, 3.57) | 1.63 (0.74, 3.59) | 2.29 (0.76, 6.84) | 1.06 (0.32, 3.57) | |
| 100th | >36.4 g | 2.28 (1.14, 4.56) * | 2.31 (0.99, 5.40) | 2.09 (0.65, 6.68) | 2.46 (0.67, 9.00) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Mat Ludin, A.F.; Karim, N.A.; Hazwari, N.D.D.; Kek, Q.W.; Abdul Basir, S.M.; Arifin, A. Do Temporal Eating Patterns Differ in Healthy versus Unhealthy Overweight/Obese Individuals? Nutrients 2021, 13, 4121. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114121
Mazri FH, Manaf ZA, Shahar S, Mat Ludin AF, Karim NA, Hazwari NDD, Kek QW, Abdul Basir SM, Arifin A. Do Temporal Eating Patterns Differ in Healthy versus Unhealthy Overweight/Obese Individuals? Nutrients. 2021; 13(11):4121. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114121
Chicago/Turabian StyleMazri, Fatin Hanani, Zahara Abdul Manaf, Suzana Shahar, Arimi Fitri Mat Ludin, Norwahidah Abdul Karim, Nur Diyana Dalila Hazwari, Qi Wen Kek, Siti Munirah Abdul Basir, and Asnida Arifin. 2021. "Do Temporal Eating Patterns Differ in Healthy versus Unhealthy Overweight/Obese Individuals?" Nutrients 13, no. 11: 4121. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114121