
Reproducibility and Validity of a Food Frequency Questionnaire (FFQ) Developed for Middle-Aged and Older Adults in Semarang, Indonesia

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
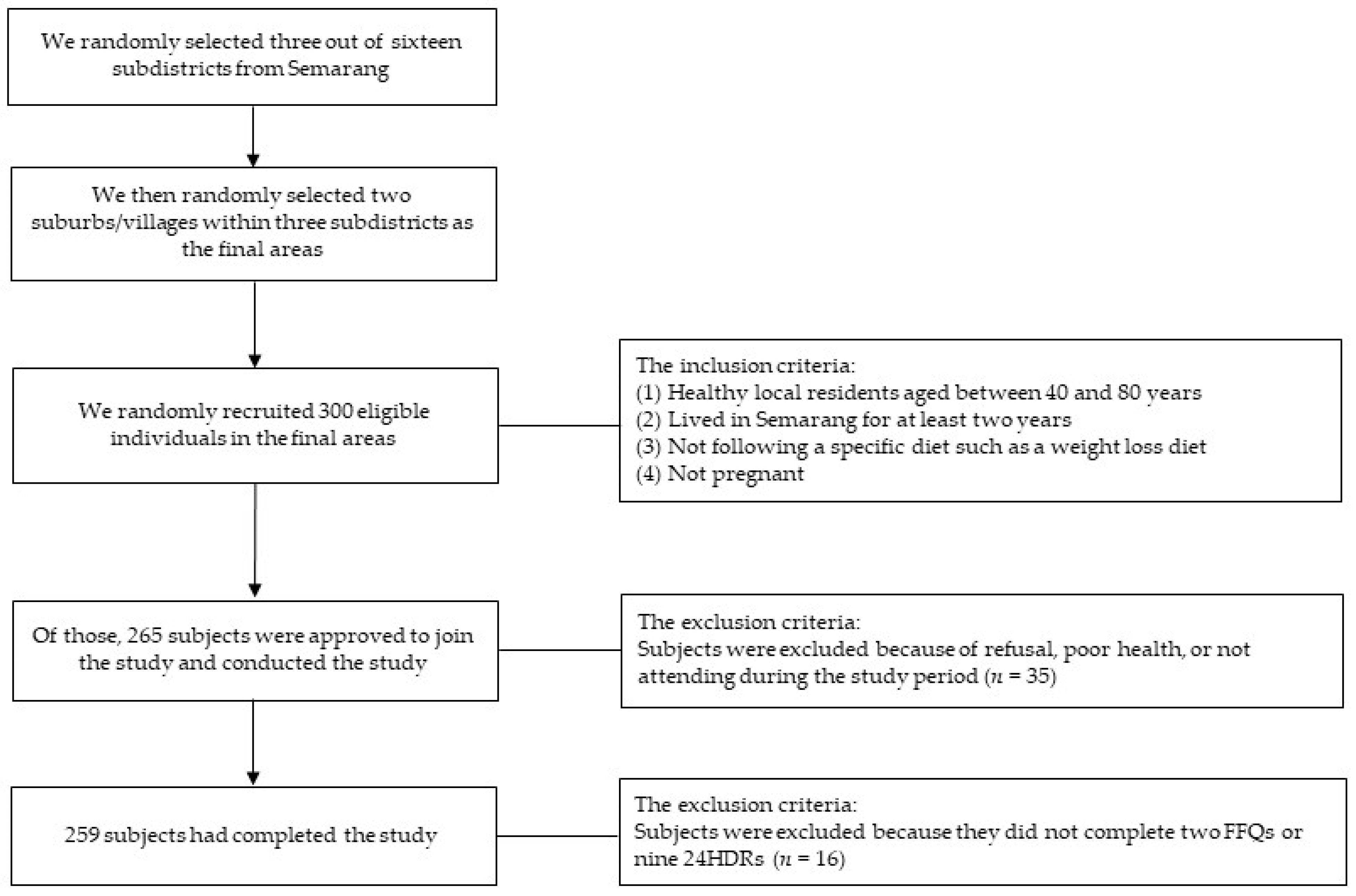
2.1. Study Population
2.2. Assessment of Dietary Intake
2.3. Other Variables
2.4. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yach, D.; Hawkes, C.; Gould, C.L.; Hofman, K.J. The global burden of chronic diseases: Overcoming impediments to prevention and control. JAMA 2004, 291, 2616–2622. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Sutradhar, R.; Yao, Z.; Wodchis, W.P.; Rosella, L.C. Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int. J. Epidemiol. 2020, 49, 113–130. [Google Scholar] [CrossRef] [PubMed]
- Syauqy, A.; Hsu, C.Y.; Lee, H.A.; Rau, H.H.; Chao, J.C.J. Association between dietary patterns and kidney function parameters in adults with metabolic syndrome: A cross-sectional study. Nutrients 2020, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Milagro, F.I.; Allayee, H.; Chmurzynska, A.; Choi, M.S.; Curi, R.; De Caterina, R.; Ferguson, L.R.; Goni, L.; Kang, J.X.; et al. Guide for current nutrigenetic, nutrigenomic, and nutriepigenetic approaches for precision nutrition involving the prevention and management of chronic diseases associated with obesity. J. Nutr. Nutr. 2017, 10, 43–62. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Syauqy, A.; Hsu, C.Y.; Rau, H.H.; Chao, J.C.J. Association of dietary patterns with components of metabolic syndrome and inflammation among middle-aged and older adults with metabolic syndrome in Taiwan. Nutrients 2018, 10, 143. [Google Scholar] [CrossRef] [Green Version]
- Syauqy, A.; Noer, E.R.; Fajrani, A.M.; Kurniawati, D.M.a.; Purwanti, R.; Rahadiyanti, A.; Rahma, D.E. Dietary patterns were associated with obesity parameters among healthy women. J. Nutr. Coll. 2020, 9, 6. [Google Scholar] [CrossRef]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Cui, Q.; Xia, Y.; Wu, Q.; Chang, Q.; Niu, K.; Zhao, Y. A meta-analysis of the reproducibility of food frequency questionnaires in nutritional epidemiological studies. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 12. [Google Scholar] [CrossRef]
- Dehghan, M.; Ilow, R.; Zatonska, K.; Szuba, A.; Zhang, X.; Mente, A.; Regulska-Ilow, B. Development, reproducibility and validity of the food frequency questionnaire in the Poland arm of the Prospective Urban and Rural Epidemiological (PURE) study. J. Hum. Nutr. Diet. 2012, 25, 225–232. [Google Scholar] [CrossRef]
- Xue, Y.; Yang, K.; Wang, B.; Liu, C.; Mao, Z.; Yu, S.; Li, X.; Wang, Y.; Sun, H.; Wang, C.; et al. Reproducibility and validity of an FFQ in the Henan Rural Cohort Study. Public Health Nutr. 2020, 23, 34–40. [Google Scholar] [CrossRef]
- Visser, M.; Elstgeest, L.E.M.; Winkens, L.H.H.; Brouwer, I.A.; Nicolaou, M. Relative validity of the HELIUS food frequency questionnaire for measuring dietary intake in older adult participants of the longitudinal aging study Amsterdam. Nutrients 2020, 12, 1998. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Hong, X.; Wang, Z.; Yang, H.; Chen, X.; Zhou, H.; Wang, C.; Lai, Y.; Sun, L.; Xu, F. Reproducibility and validity of an FFQ developed for adults in Nanjing, China. Br. J. Nutr. 2016, 115, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Doustmohammadian, A.; Amini, M.; Esmaillzadeh, A.; Omidvar, N.; Abtahi, M.; Dadkhah-Piraghaj, M.; Nikooyeh, B.; Neyestani, T.R. Validity and reliability of a dish-based semi-quantitative food frequency questionnaire for assessment of energy and nutrient intake among Iranian adults. BMC Res. Notes 2020, 13, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurul-Fadhilah, A.; Teo, P.S.; Foo, L.H. Validity and reproducibility of a food frequency questionnaire (FFQ) for dietary assessment in Malay adolescents in Malaysia. Asia Pac. J. Clin. Nutr. 2012, 21, 97–103. [Google Scholar]
- Ramadhani, P.P.; Dieny, F.F.; Kurniawati, D.; Sandi, H.; Fitranti, D.Y.; Rahadiyanti, A.; Tsani, A.F.A. Household food security and diet quality with chronic energy deficiency among preconception women. Indones. J. Nutr. 2021, 9, 111–122. [Google Scholar] [CrossRef]
- Herningtyas, E.H.; Ng, T.S. Prevalence and distribution of metabolic syndrome and its components among provinces and ethnic groups in Indonesia. BMC Public Health 2019, 19, 377. [Google Scholar] [CrossRef] [Green Version]
- Statistics of Semarang Municipality. Available online: https://semarangkota.bps.go.id/ (accessed on 1 August 2021).
- Indonesian Food Composition Data. Available online: https://www.panganku.org/en-EN/beranda (accessed on 1 August 2021).
- United States Department of Agriculture. Available online: https://ndb.nal.usda.gov/ndb/search/list (accessed on 1 August 2021).
- Rosner, B.; Willett, W.C. Interval estimates for correlation coefficients corrected for within-person variation: Implications for study design and hypothesis testing. Am. J. Epidemiol. 1988, 127, 377–386. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012; Volume 40. [Google Scholar]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Zhuang, M.; Yuan, Z.; Lin, L.; Hu, B.; Wang, X.; Yang, Y.; Chen, X.; Jin, L.; Lu, M.; Ye, W. Reproducibility and relative validity of a food frequency questionnaire developed for adults in Taizhou, China. PLoS ONE 2012, 7, e48341. [Google Scholar] [CrossRef] [Green Version]
- Xia, W.; Sun, C.; Zhang, L.; Zhang, X.; Wang, J.; Wang, H.; Wu, L. Reproducibility and relative validity of a food frequency questionnaire developed for female adolescents in Suihua, North China. PLoS ONE 2011, 6, e19656. [Google Scholar] [CrossRef] [Green Version]
- Marques-Vidal, P.; Ross, A.; Wynn, E.; Rezzi, S.; Paccaud, F.; Decarli, B. Reproducibility and relative validity of a food-frequency questionnaire for French-speaking Swiss adults. Food Nutr. Res. 2011, 55, 5905. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Maes, L. A Belgian study on the reliability and relative validity of the health behaviour in school-aged children food-frequency questionnaire. Public Health Nutr. 2003, 6, 581–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. (In Zagreb) [Google Scholar] [CrossRef]
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Grubb, D.A.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, V.; de Lauzon-Guillain, B.; Lafay, L.; Borys, J.M.; Charles, M.A.; Romon, M. Reproducibility and relative validity of a food-frequency questionnaire among French adults and adolescents. Eur. J. Clin. Nutr. 2009, 63, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.X.; Ho, S.C. Validity and reproducibility of a food frequency questionnaire among Chinese women in Guangdong province. Asia Pac. J. Clin. Nutr. 2009, 18, 240–250. [Google Scholar]
- Villegas, R.; Yang, G.; Liu, D.; Xiang, Y.B.; Cai, H.; Zheng, W.; Shu, X.O. Validity and reproducibility of the food-frequency questionnaire used in the Shanghai men’s health study. Br. J. Nutr. 2007, 97, 993–1000. [Google Scholar] [CrossRef] [Green Version]
- Praagman, J.; Adolphs, A.P.; van Rossum, C.T.; Sluijs, I.; van der Schouw, Y.T.; Beulens, J.W. Reproducibility and relative validity of a FFQ to estimate the intake of fatty acids. Br. J. Nutr. 2016, 115, 2154–2161. [Google Scholar] [CrossRef] [Green Version]
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noor Hafizah, Y.; Ang, L.C.; Yap, F.; Nurul Najwa, W.; Cheah, W.L.; Ruzita, A.T.; Jumuddin, F.A.; Koh, D.; Lee, J.A.C.; Essau, C.A.; et al. Validity and reliability of a food frequency questionnaire (FFQ) to assess dietary intake of preschool children. Int. J. Environ. Res. Public Health 2019, 16, 4722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haftenberger, M.; Heuer, T.; Heidemann, C.; Kube, F.; Krems, C.; Mensink, G.B. Relative validation of a food frequency questionnaire for national health and nutrition monitoring. Nutr. J. 2010, 9, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Food Groups | Food Items |
|---|---|
| Rice/flour products | Rice, noodles, vermicelli, plain bread |
| Root crops | Boiled/steamed potato, taro, cassava |
| Whole grains | Whole grains, whole wheat, mixed grains, brown rice, oatmeal |
| Staples cook with oil | Fried rice, fried noodle, kwetiau, uduk rice, kebuli rice, yellow rice |
| Legumes and nuts | Peas, nuts, beans, peanuts coated with flour |
| Soybeans | Steamed tempe, tahu, tofu |
| Milk and dairy products | Milk, cheese, yoghurt |
| Light-colored vegetables | Cabbage, Chinese cabbage, cucumber, pechay, chayote, squash, radish, bean sprouts, pumpkin, mushroom |
| Dark-colored vegetables | Spinach, carrots, kale, buncis, caisin, lotus root leaves, papaya leaves, long beans, mustard greens, glossy nightshade |
| Eggs | Chicken eggs, duck eggs, quail eggs |
| Fish and seafood | Fish, squid, shrimp, octopus, crab |
| Meat | Beef, veal, lamb, goat, pork |
| Poultry | Chicken, duck, goose, pigeon |
| Fast food | Instant noodles, chicken nugget, pizza, hamburger, doughnut, martabak, bakso |
| Processed food | Sausage, canned food, instant food |
| Fried food | Fried chicken, dried fish-tofu (batagor), bakwan, risol, cakwe, pastel, cireng, gorengan, fried fish (pempek), fried banana, chips, cassava chips |
| Organs of animals | Liver, kidney, heart, intestines |
| Fruits | Banana, orange, pear, mango, papaya, avocado, watermelon, apple, grape, starfruit, dragon fruit, duku, rambutan, rose apple, lemon, coconut, mangosteen, giant granadilla, jack fruit, snack fruit, soursop, breadfruit |
| Processed fruit | Canned fruit, rujak, asinan |
| Traditional snacks | Gethuk, serabi cake, putu cake, gemblong, pukis |
| Jam/honey | Jam, honey |
| Sugary drinks | Soft drinks, soda, energy drinks, flavored fruit drinks |
| Sweet dessert | Butter bread, sweet bread, cake, cookies, biscuit, crackers |
| Tea and coffee | Green tea, black tea, black coffee, traditional coffee |
| Characteristics | All Subjects |
|---|---|
| Age, years | 54.8 ± 9.6 |
| Gender, % | |
| Male | 57.9 |
| Female | 42.1 |
| Marital status, % | |
| Married | 81.5 |
| Not married/divorce | 18.5 |
| Smoking status, % | |
| Current smoker | 55.2 |
| Ex-smoker | 17.0 |
| Never smoke | 27.8 |
| Body mass index, kg/m2 | 24.0 ± 3.2 |
| Variables | FFQ1 | FFQ2 | 24HDRs | p-Value 1 | Percentage of Mean Difference | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | FFQ1 vs. FFQ2 | FFQ1 vs. 24HDRs | FFQ1 vs. FFQ2 | FFQ1 vs. 24HDRs | |
| Energy (kcal) 2 | 1921 | 423 | 1877 | 386 | 1751 | 413 | 0.008 | <0.001 | 2.4 | 9.7 |
| Carbohydrate (g) 2 | 288 | 67 | 282 | 64 | 264 | 66 | <0.001 | <0.001 | 2.0 | 8.8 |
| Fiber (g) 2 | 18 | 4 | 16 | 3 | 15 | 3 | <0.001 | <0.001 | 8.9 | 19.5 |
| Fat (g) 2 | 61 | 14 | 59 | 12 | 55 | 13 | 0.015 | <0.001 | 2.5 | 11.0 |
| MUFA (g) 3 | 22 | 6 | 21 | 5 | 21 | 6 | 0.055 | <0.001 | 2.9 | 6.5 |
| PUFA (g) 3 | 11 | 2 | 10 | 2 | 8 | 2 | <0.001 | <0.001 | 8.1 | 31.3 |
| Cholesterol (mg) 3 | 129 | 33 | 123 | 32 | 109 | 29 | 0.002 | <0.001 | 5.4 | 19.0 |
| Protein (g) 2 | 55 | 13 | 52 | 11 | 50 | 12 | 0.005 | <0.001 | 2.7 | 8.6 |
| Retinol (µg) 2 | 438 | 121 | 405 | 142 | 331 | 131 | <0.001 | <0.001 | 7.9 | 32.1 |
| β-Carotene (µg) 2 | 1884 | 531 | 1834 | 530 | 1716 | 502 | 0.08 | <0.001 | 2.7 | 9.8 |
| Vitamin C (mg) 2 | 116 | 41 | 112 | 33 | 90 | 34 | 0.038 | <0.001 | 3.7 | 29.0 |
| Vitamin D (µg) 3 | 2.81 | 0.56 | 2.59 | 0.66 | 2.49 | 0.73 | <0.001 | <0.001 | 8.5 | 12.9 |
| Vitamin E (mg) 3 | 2.29 | 0.63 | 2.11 | 0.64 | 2.03 | 0.58 | <0.001 | <0.001 | 8.5 | 12.8 |
| Thiamin (mg) 2 | 1.15 | 0.58 | 0.90 | 0.54 | 0.75 | 0.50 | <0.001 | <0.001 | 27.8 | 53.3 |
| Riboflavin (mg) 2 | 1.87 | 0.60 | 1.76 | 0.40 | 1.64 | 0.41 | <0.001 | <0.001 | 6.3 | 14.0 |
| Niacin (mg) 2 | 13.5 | 3.3 | 13.3 | 3.7 | 12.7 | 3.6 | 0.203 | <0.001 | 1.7 | 6.6 |
| Sodium (mg) 2 | 1705 | 466 | 1674 | 443 | 1580 | 453 | 0.09 | <0.001 | 1.9 | 7.9 |
| Potassium (mg) 2 | 3795 | 948 | 3538 | 945 | 3328 | 968 | <0.001 | <0.001 | 7.3 | 14.0 |
| Calcium (mg) 2 | 579 | 122 | 540 | 124 | 477 | 127 | <0.001 | <0.001 | 7.2 | 21.4 |
| Phosphorus (mg) 2 | 623 | 141 | 590 | 124 | 536 | 137 | <0.001 | <0.001 | 5.6 | 16.3 |
| Magnesium (mg) 3 | 377 | 91 | 370 | 100 | 364 | 101 | <0.001 | <0.001 | 1.9 | 3.5 |
| Iron (mg) 2 | 11.8 | 3.3 | 10.7 | 3.4 | 10.2 | 3.3 | <0.001 | <0.001 | 10.1 | 16.2 |
| Copper (mg) 2 | 634 | 183 | 619 | 135 | 578 | 163 | 0.06 | <0.001 | 2.5 | 9.6 |
| Zinc (mg) 2 | 10.1 | 2.3 | 8.4 | 1.8 | 6.9 | 1.8 | <0.001 | <0.001 | 20.1 | 46.2 |
| Variables | FFQ1 vs. FFQ2 | FFQ1 vs. 24HDRs | |||||
|---|---|---|---|---|---|---|---|
| PCC | ICC | PCC | |||||
| Crude | Energy Adjust | Crude | Energy Adjust | Crude | Energy Adjust | De-Attenuated | |
| Energy (kcal) | 0.78 | - | 0.77 | - | 0.63 | - | 0.70 |
| Carbohydrate (g) | 0.76 | 0.47 | 0.76 | 0.48 | 0.56 | 0.49 | 0.67 |
| Fiber (g) | 0.50 | 0.30 | 0.44 | 0.31 | 0.51 | 0.33 | 0.69 |
| Fat (g) | 0.71 | 0.43 | 0.70 | 0.45 | 0.53 | 0.76 | 0.65 |
| MUFA (g) | 0.60 | 0.41 | 0.59 | 0.44 | 0.58 | 0.68 | 0.67 |
| PUFA (g) | 0.67 | 0.50 | 0.62 | 0.34 | 0.46 | 0.35 | 0.58 |
| Cholesterol (mg) | 0.58 | 0.56 | 0.55 | 0.52 | 0.52 | 0.46 | 0.71 |
| Protein (g) | 0.74 | 0.42 | 0.71 | 0.43 | 0.54 | 0.39 | 0.66 |
| Retinol (µg) | 0.72 | 0.70 | 0.70 | 0.66 | 0.57 | 0.58 | 0.74 |
| β-Carotene (µg) | 0.64 | 0.44 | 0.63 | 0.38 | 0.70 | 0.66 | 0.78 |
| Vitamin C (mg) | 0.70 | 0.72 | 0.68 | 0.65 | 0.60 | 0.59 | 0.73 |
| Vitamin D (µg) | 0.65 | 0.44 | 0.58 | 0.44 | 0.46 | 0.46 | 0.60 |
| Vitamin E (mg) | 0.69 | 0.67 | 0.66 | 0.64 | 0.56 | 0.56 | 0.68 |
| Thiamin (mg) | 0.60 | 0.72 | 0.75 | 0.56 | 0.41 | 0.50 | 0.54 |
| Riboflavin (mg) | 0.66 | 0.62 | 0.60 | 0.54 | 0.55 | 0.70 | 0.68 |
| Niacin (mg) | 0.62 | 0.62 | 0.61 | 0.63 | 0.56 | 0.73 | 0.67 |
| Sodium (mg) | 0.61 | 0.44 | 0.78 | 0.53 | 0.65 | 0.59 | 0.74 |
| Potassium (mg) | 0.81 | 0.53 | 0.69 | 0.42 | 0.67 | 0.52 | 0.77 |
| Calcium (mg) | 0.78 | 0.78 | 0.74 | 0.66 | 0.60 | 0.83 | 0.76 |
| Phosphorus (mg) | 0.79 | 0.48 | 0.78 | 0.45 | 0.61 | 0.31 | 0.74 |
| Magnesium (mg) | 0.60 | 0.58 | 0.58 | 0.38 | 0.43 | 0.40 | 0.55 |
| Iron (mg) | 0.62 | 0.63 | 0.59 | 0.60 | 0.48 | 0.48 | 0.59 |
| Copper (mg) | 0.71 | 0.70 | 0.67 | 0.62 | 0.69 | 0.89 | 0.78 |
| Zinc (mg) | 0.55 | 0.53 | 0.57 | 0.55 | 0.48 | 0.48 | 0.82 |
| Variables | FFQ1 vs. FFQ2 | FFQ1 vs. 24HDRs | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Same Quartile | Adjacent Quartile | One Quartile Apart | Opposite Quartile | Weighted Kappa | Same Quartile | Adjacent Quartile | One Quartile Apart | Opposite Quartile | Weighted Kappa | |
| Energy (kcal) | 50.6 | 42.1 | 7.0 | 0.4 | 0.34 | 42.1 | 44.0 | 10.4 | 3.5 | 0.23 |
| Carbohydrate (g) | 51.4 | 43.2 | 4.6 | 0.8 | 0.35 | 39.3 | 45.2 | 11.2 | 4.3 | 0.20 |
| Fiber (g) | 41.6 | 48.8 | 7.7 | 1.9 | 0.21 | 43.3 | 42.9 | 10.4 | 3.5 | 0.24 |
| Fat (g) | 52.1 | 39.4 | 7.0 | 1.5 | 0.37 | 44.4 | 40.5 | 10.8 | 4.3 | 0.26 |
| MUFA (g) | 50.6 | 36.3 | 9.3 | 3.9 | 0.34 | 49.4 | 37.1 | 10.8 | 2.7 | 0.32 |
| PUFA (g) | 43.6 | 50.2 | 4.6 | 1.5 | 0.25 | 46.7 | 37.8 | 11.2 | 4.3 | 0.29 |
| Cholesterol (mg) | 40.5 | 49.8 | 7.7 | 1.9 | 0.21 | 43.3 | 42.9 | 10.4 | 3.5 | 0.24 |
| Protein (g) | 48.7 | 42.1 | 8.9 | 0.4 | 0.30 | 44.8 | 38.2 | 15.8 | 1.2 | 0.25 |
| Retinol (µg) | 56.8 | 35.1 | 7.7 | 0.4 | 0.42 | 43.3 | 37.8 | 18.5 | 0.4 | 0.24 |
| β-Carotene (µg) | 50.6 | 36.3 | 9.3 | 3.9 | 0.34 | 49.8 | 39.8 | 6.9 | 3.5 | 0.33 |
| Vitamin C (mg) | 55.2 | 35.5 | 8.5 | 0.8 | 0.40 | 50.6 | 36.3 | 10.4 | 2.7 | 0.34 |
| Vitamin D (µg) | 54.1 | 34.4 | 8.8 | 2.7 | 0.39 | 45.6 | 35.1 | 13.5 | 5.8 | 0.27 |
| Vitamin E (mg) | 55.2 | 34.4 | 9.7 | 0.8 | 0.41 | 49.1 | 37.1 | 9.7 | 4.2 | 0.32 |
| Thiamin (mg) | 44.8 | 36.3 | 17.8 | 1.2 | 0.26 | 44.0 | 41.3 | 11.2 | 3.5 | 0.25 |
| Riboflavin (mg) | 40.5 | 49.8 | 7.7 | 1.9 | 0.21 | 43.3 | 42.9 | 10.4 | 3.5 | 0.24 |
| Niacin (mg) | 42.1 | 40.5 | 16.6 | 0.8 | 0.22 | 44.0 | 41.3 | 11.2 | 3.5 | 0.25 |
| Sodium (mg) | 55.2 | 37.1 | 7.0 | 0.8 | 0.40 | 47.9 | 41.7 | 7.7 | 2.7 | 0.32 |
| Potassium (mg) | 49.0 | 44.0 | 6.6 | 0.4 | 0.33 | 44.8 | 44.4 | 8.5 | 2.3 | 0.27 |
| Calcium (mg) | 46.8 | 42.9 | 7.0 | 3.4 | 0.39 | 44.8 | 44.0 | 10.4 | 0.8 | 0.24 |
| Phosphorus (mg) | 50.6 | 42.5 | 6.6 | 0.4 | 0.32 | 43.3 | 43.2 | 11.2 | 2.3 | 0.20 |
| Magnesium (mg) | 55.2 | 32.4 | 8.1 | 4.3 | 0.39 | 43.6 | 44.0 | 6. 6 | 5.8 | 0.24 |
| Iron (mg) | 56.8 | 31.3 | 9.3 | 2.7 | 0.42 | 47.9 | 33.2 | 14.3 | 4.6 | 0.30 |
| Copper (mg) | 52.9 | 31.3 | 14.7 | 1.2 | 0.37 | 44.0 | 43.6 | 8.9 | 3.5 | 0.25 |
| Zinc (mg) | 42.9 | 42.1 | 13.9 | 1.2 | 0.22 | 42.5 | 39.4 | 13.1 | 5.0 | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syauqy, A.; Afifah, D.N.; Purwanti, R.; Nissa, C.; Fitranti, D.Y.; Chao, J.C.-J. Reproducibility and Validity of a Food Frequency Questionnaire (FFQ) Developed for Middle-Aged and Older Adults in Semarang, Indonesia. Nutrients 2021, 13, 4163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114163
Syauqy A, Afifah DN, Purwanti R, Nissa C, Fitranti DY, Chao JC-J. Reproducibility and Validity of a Food Frequency Questionnaire (FFQ) Developed for Middle-Aged and Older Adults in Semarang, Indonesia. Nutrients. 2021; 13(11):4163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114163
Chicago/Turabian StyleSyauqy, Ahmad, Diana Nur Afifah, Rachma Purwanti, Choirun Nissa, Deny Yudi Fitranti, and Jane C.-J. Chao. 2021. "Reproducibility and Validity of a Food Frequency Questionnaire (FFQ) Developed for Middle-Aged and Older Adults in Semarang, Indonesia" Nutrients 13, no. 11: 4163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114163