
The Association between Daily Total Dietary Nutrient Intake and Recent Glycemic Control States of Non-Pregnant Adults 20+ Years Old from NHANES 1999–2018 (Except for 2003–2004)


Abstract
:1. Introduction
2. Methods
2.1. Database and Study Population
2.2. Variables
2.3. Statistical Analysis
3. Result
3.1. Baseline Characteristics
3.2. Binary Logistic Regression Analysis
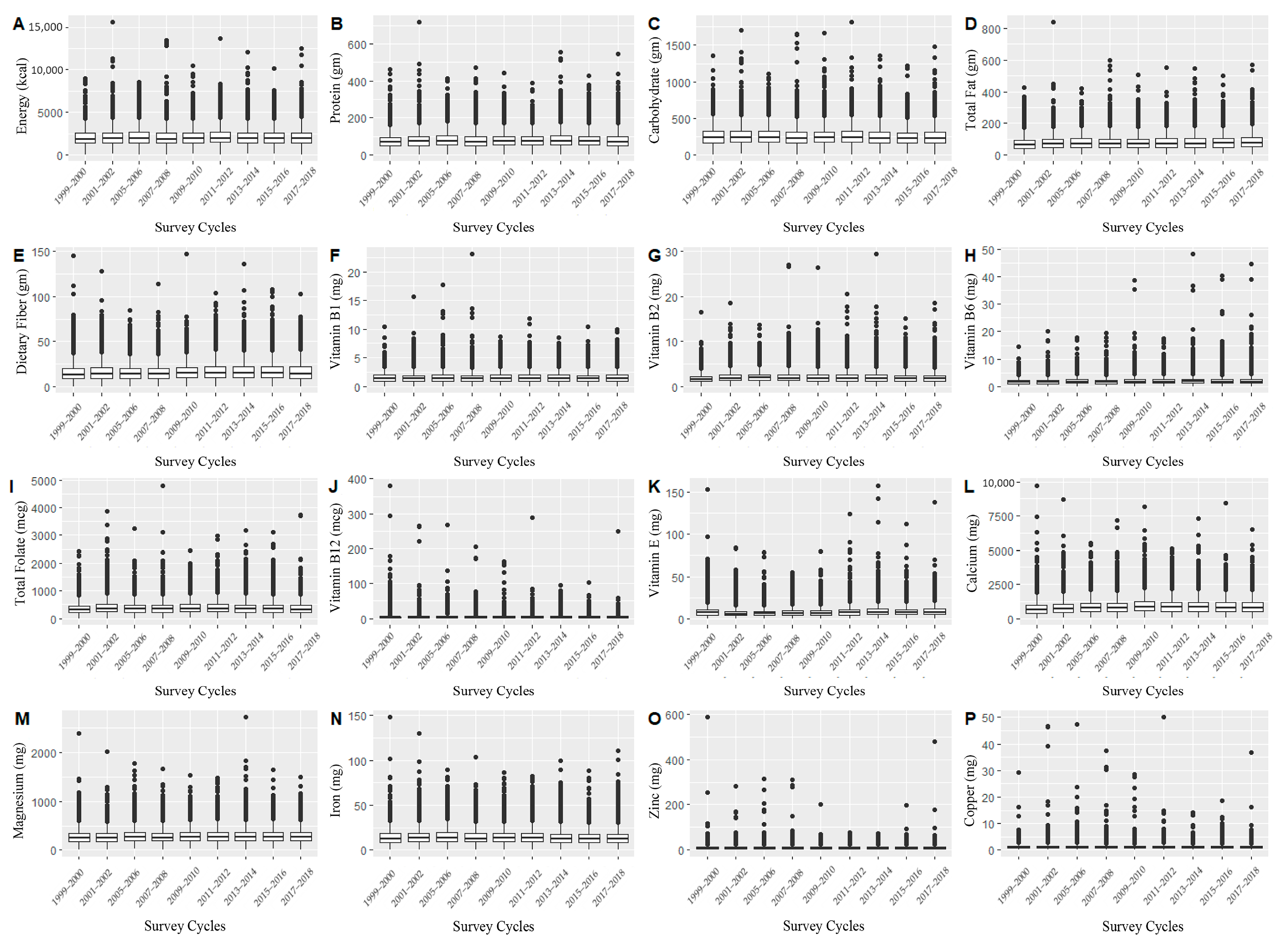
3.2.1. The Association between RGCS and Daily Total Dietary Energy, Macronutrients, Vitamins, and Minerals
3.2.2. The Association between Adjusted Covariates and RGCS
3.3. Model Fitting, Linear Discriminant Analysis, and ROC Analysis
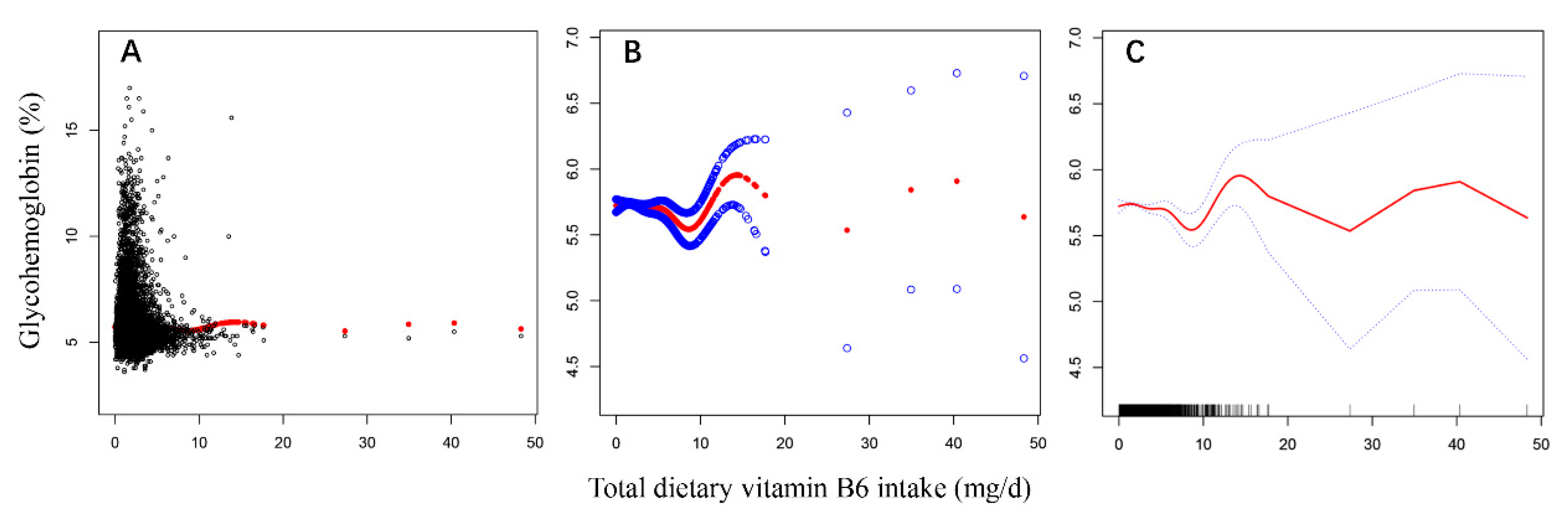
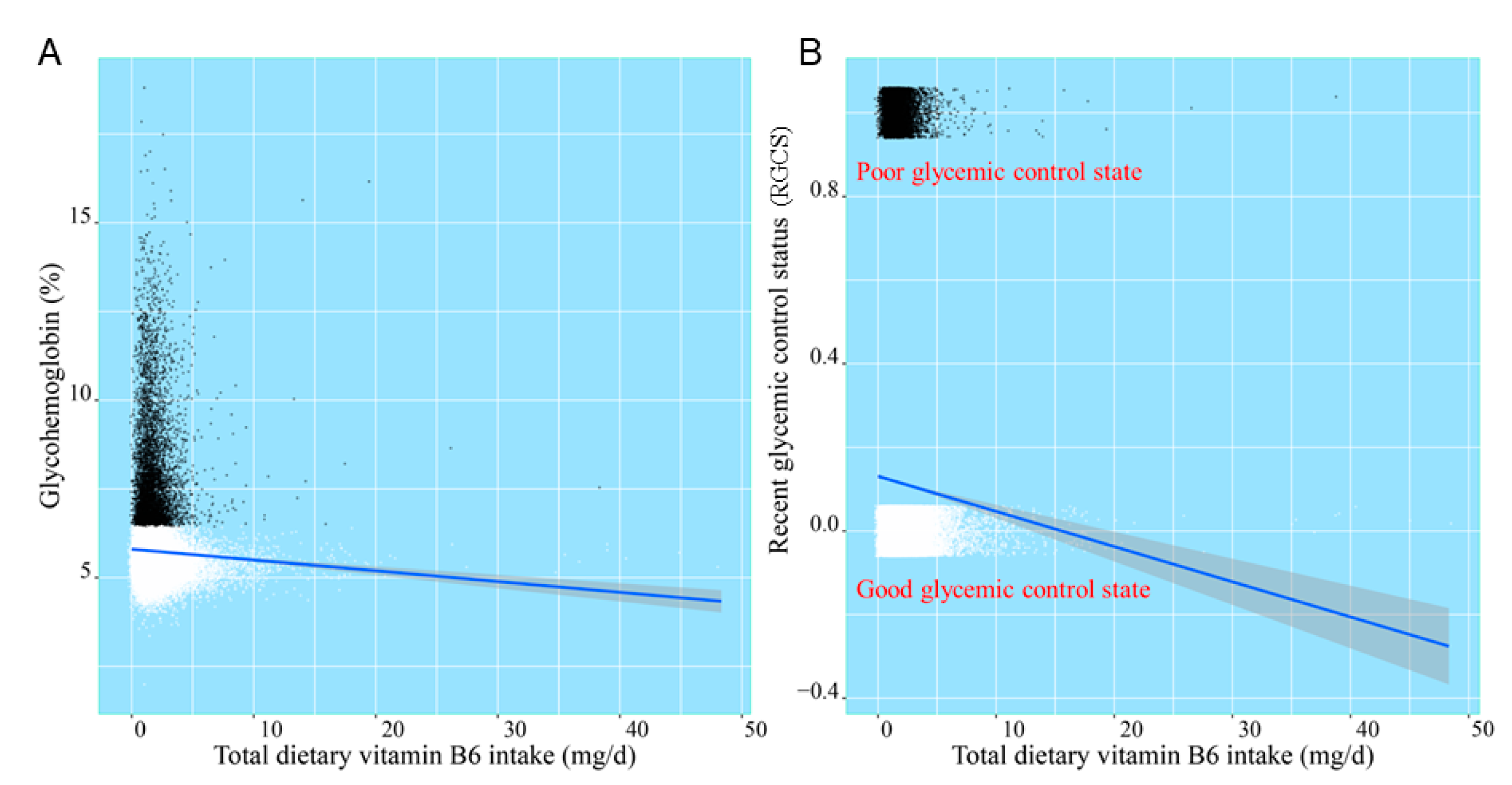
3.3.1. Model Fitting and Linear Discriminant Analysis of Daily Total Dietary Vitamin B6 Intake, Glycohemoglobin, and RGCS
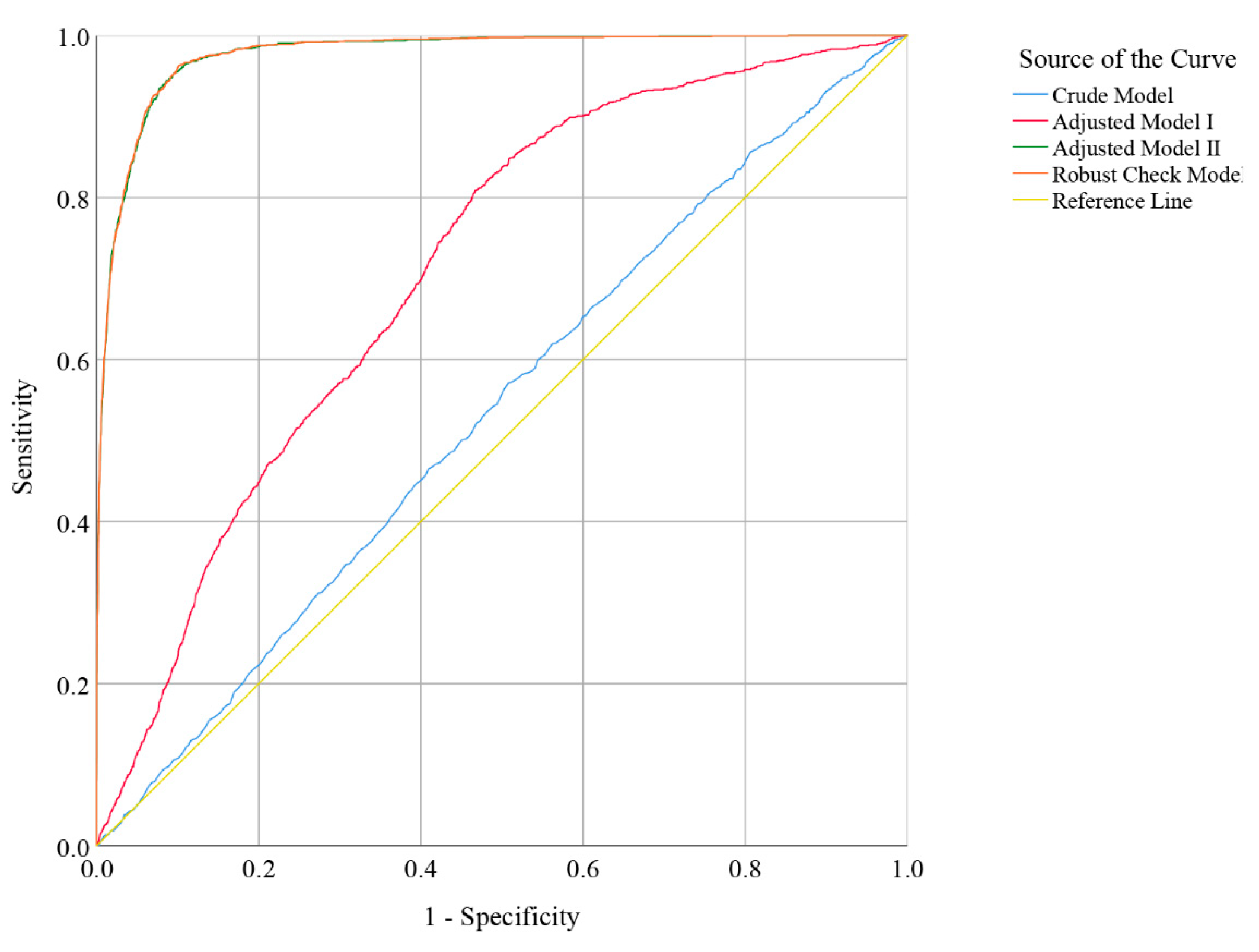
3.3.2. ROC Analysis of Daily Total Dietary Vitamin B6 Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Venn, B.J. Macronutrients and Human Health for the 21st Century. Nutrients 2020, 12, 2363. [Google Scholar] [CrossRef]
- Franz, M.J. Diabetes Nutrition Therapy: Effectiveness, Macronutrients, Eating Patterns and Weight Management. Am. J. Med Sci. 2016, 351, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.; Kempf, P.; Bally, L.; Stettler, C. Carbohydrate Intake in the Context of Exercise in People with Type 1 Diabetes. Nutrients 2019, 11, 3017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, S.; Beck, E.; Salman, H.; Tapsell, L. New Horizons for the Study of Dietary Fiber and Health: A Review. Plant Foods Hum. Nutr. 2016, 71, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R., Jr.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.; Ke, M.Y.; Li, W.H.; Zhang, S.Q.; Fang, X.C. The impact of soluble dietary fibre on gastric emptying, postprandial blood glucose and insulin in patients with type 2 diabetes. Asia Pac. J. Clin. Nutr. 2014, 23, 210–218. [Google Scholar] [CrossRef]
- Lin, C.C.; Huang, Y.L. Chromium, zinc and magnesium status in type 1 diabetes. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 588–592. [Google Scholar] [CrossRef]
- Skalnaya, M.G.; Skalny, A.V.; Grabeklis, A.R.; Serebryansky, E.P.; Demidov, V.A.; Tinkov, A.A. Hair Trace Elements in Overweight and Obese Adults in Association with Metabolic Parameters. Biol. Trace Elem. Res. 2018, 186, 12–20. [Google Scholar] [CrossRef]
- Soliman, A.T.; De Sanctis, V.; Yassin, M.; Soliman, N. Iron deficiency anemia and glucose metabolism. Acta Bio-Med. Atenei Parm. 2017, 88, 112–118. [Google Scholar] [CrossRef]
- Deshmukh, S.V.; Prabhakar, B.; Kulkarni, Y.A. Water Soluble Vitamins and their Role in Diabetes and its Complications. Curr. Diabetes Rev. 2020, 16, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Kaur, B.; Henry, J. Micronutrient status in type 2 diabetes: A review. Adv. Food Nutr. Res. 2014, 71, 55–100. [Google Scholar] [CrossRef]
- Li, X.; Liu, Y.; Zheng, Y.; Wang, P.; Zhang, Y. The Effect of Vitamin D Supplementation on Glycemic Control in Type 2 Diabetes Patients: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lips, P.; Eekhoff, M.; van Schoor, N.; Oosterwerff, M.; de Jongh, R.; Krul-Poel, Y.; Simsek, S. Vitamin D and type 2 diabetes. J. Steroid Biochem. Mol. Biol. 2017, 173, 280–285. [Google Scholar] [CrossRef]
- Fazelian, S.; Rouhani, M.H.; Bank, S.S.; Amani, R. Chromium supplementation and polycystic ovary syndrome: A systematic review and meta-analysis. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. (GMS) 2017, 42, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Suksomboon, N.; Poolsup, N.; Yuwanakorn, A. Systematic review and meta-analysis of the efficacy and safety of chromium supplementation in diabetes. J. Clin. Pharm. Ther. 2014, 39, 292–306. [Google Scholar] [CrossRef]
- Yin, R.V.; Phung, O.J. Effect of chromium supplementation on glycated hemoglobin and fasting plasma glucose in patients with diabetes mellitus. Nutr. J. 2015, 14, 14. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Xu, Y.; Huang, Z.; Wei, Y.; Hou, J.; Long, T.; Wang, F.; Hu, H.; Duan, Y.; Guo, H.; et al. Association between exposure to arsenic, nickel, cadmium, selenium, and zinc and fasting blood glucose levels. Environ. Pollut. 2019, 255, 113325. [Google Scholar] [CrossRef]
- Wang, X.; Wu, W.; Zheng, W.; Fang, X.; Chen, L.; Rink, L.; Min, J.; Wang, F. Zinc supplementation improves glycemic control for diabetes prevention and management: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2019, 110, 76–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simental-Mendía, L.E.; Sahebkar, A.; Rodríguez-Morán, M.; Guerrero-Romero, F. A systematic review and meta-analysis of randomized controlled trials on the effects of magnesium supplementation on insulin sensitivity and glucose control. Pharmacol. Res. 2016, 111, 272–282. [Google Scholar] [CrossRef]
- Volpe, S.L. Magnesium in disease prevention and overall health. Adv. Nutr. 2013, 4, 378s–383s. [Google Scholar] [CrossRef]
- Yazdanpanah, S.; Rabiee, M.; Tahriri, M.; Abdolrahim, M.; Rajab, A.; Jazayeri, H.E.; Tayebi, L. Evaluation of glycated albumin (GA) and GA/HbA1c ratio for diagnosis of diabetes and glycemic control: A comprehensive review. Crit. Rev. Clin. Lab. Sci. 2017, 54, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Weykamp, C. HbA1c: A review of analytical and clinical aspects. Ann. Lab. Med. 2013, 33, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Konishi, K.; Wada, K.; Tamura, T.; Tsuji, M.; Kawachi, T.; Nagata, C. Dietary magnesium intake and the risk of diabetes in the Japanese community: Results from the Takayama study. Eur. J. Nutr. 2017, 56, 767–774. [Google Scholar] [CrossRef]
- Bo, S.; Pisu, E. Role of dietary magnesium in cardiovascular disease prevention, insulin sensitivity and diabetes. Curr. Opin. Lipidol. 2008, 19, 50–56. [Google Scholar] [CrossRef]
- Gannon, M.C.; Nuttall, F.Q. Effect of a high-protein, low-carbohydrate diet on blood glucose control in people with type 2 diabetes. Diabetes 2004, 53, 2375–2382. [Google Scholar] [CrossRef] [Green Version]
- Intra, J.; Limonta, G.; Cappellini, F.; Bertona, M.; Brambilla, P. Glycosylated Hemoglobin in Subjects Affected by Iron-Deficiency Anemia. Diabetes Metab. J. 2019, 43, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Lee, J.E. Dietary Patterns Related to Triglyceride and High-Density Lipoprotein Cholesterol and the Incidence of Type 2 Diabetes in Korean Men and Women. Nutrients 2018, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandão-Lima, P.N.; Carvalho, G.B.; Santos, R.K.F.; Santos, B.D.C.; Dias-Vasconcelos, N.L.; Rocha, V.S.; Barbosa, K.B.F.; Pires, L.V. Intakes of Zinc, Potassium, Calcium, and Magnesium of Individuals with Type 2 Diabetes Mellitus and the Relationship with Glycemic Control. Nutrients 2018, 10, 1948. [Google Scholar] [CrossRef] [Green Version]
- Mascolo, E.; Vernì, F. Vitamin B6 and Diabetes: Relationship and Molecular Mechanisms. Int. J. Mol. Sci. 2020, 21, 3669. [Google Scholar] [CrossRef] [PubMed]
- Bender, D.A. Vitamin B6 requirements and recommendations. Eur. J. Clin. Nutr. 1989, 43, 289–309. [Google Scholar]
- Ueland, P.M.; Ulvik, A.; Rios-Avila, L.; Midttun, Ø.; Gregory, J.F. Direct and Functional Biomarkers of Vitamin B6 Status. Annu. Rev. Nutr. 2015, 35, 33–70. [Google Scholar] [CrossRef] [PubMed]
- Ueland, P.M.; McCann, A.; Midttun, Ø.; Ulvik, A. Inflammation, vitamin B6 and related pathways. Mol. Asp. Med. 2017, 53, 10–27. [Google Scholar] [CrossRef]
- Hellmann, H.; Mooney, S. Vitamin B6: A molecule for human health? Molecules 2010, 15, 442–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horikawa, C.; Aida, R.; Kamada, C.; Fujihara, K.; Tanaka, S.; Tanaka, S.; Araki, A.; Yoshimura, Y.; Moriya, T.; Akanuma, Y.; et al. Vitamin B6 intake and incidence of diabetic retinopathy in Japanese patients with type 2 diabetes: Analysis of data from the Japan Diabetes Complications Study (JDCS). Eur. J. Nutr. 2020, 59, 1585–1594. [Google Scholar] [CrossRef]
- Cho, Y.O.; Kim, B.Y. Vitamin B6 intake by Koreans should be based on sufficient amount and a variety of food sources. Nutrition 2005, 21, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Bolzetta, F.; Veronese, N.; De Rui, M.; Berton, L.; Toffanello, E.D.; Carraro, S.; Miotto, F.; Inelmen, E.M.; Donini, L.M.; Manzato, E.; et al. Are the Recommended Dietary Allowances for Vitamins Appropriate for Elderly People? J. Acad. Nutr. Diet. 2015, 115, 1789–1797. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Good RGCS (HbA1 < 6.5%) # n = 36,594 | Poor RGCS (HbA1 ≥ 6.5%) # n = 4708 | -Value | |
|---|---|---|---|---|
| Gender (%) | 21.006 | <0.001 | ||
| Male | 17,978 (87.9) | 2480 (12.1) | ||
| Female | 18,616 (89.3) | 2228 (10.7) | ||
| Age (%) | 2119.291 | <0.001 | ||
| ≥60 years old | 11,414 (80.1) | 2843 (19.9) | ||
| 40–59 years old | 12,125 (88.6) | 1554 (11.4) | ||
| <40 years old | 13,055 (97.7) | 311 (2.3) | ||
| Race (%) | 322.688 | <0.001 | ||
| Non-Hispanic White | 16,857 (91.6) | 1547 (8.4) | ||
| Non-Hispanic Black | 7201 (85.1) | 1257 (14.9) | ||
| Mexican American | 6140 (85.8) | 1013 (14.2) | ||
| Other Races | 6396 (87.8) | 891 (12.2) | ||
| Education level (%) † | 255.723 | <0.001 | ||
| ≤High School | 17,597 (86.1) | 2845 (13.9) | ||
| College or above | 18,955 (91.1) | 1855 (8.9) | ||
| BMI (Kg/m2) *† | 219.213 | <0.001 | ||
| ≥30.0 | 102 (87.9) | 14 (12.1) | ||
| 25.0–29.9 | 12,455 (90.5) | 1304 (9.5) | ||
| <25.0 | 11,298 (95.3) | 557 (4.7) | ||
| Moderate/severe physical activity (%) † | 162.861 | <0.001 | ||
| Yes | 14,859 (91.1) | 1457 (8.9) | ||
| No | 21,719 (87.0) | 3249 (13.0) | ||
| Hypertension (%) † | 537.915 | <0.001 | ||
| Yes | 14,672 (84.7) | 2648 (15.3) | ||
| No | 19,138 (92.2) | 1611 (7.8) | ||
| The doctor told you that you had diabetes (%) | 18,424.978 | <0.001 | ||
| Yes | 1711 (33.1) | 3462 (66.9) | ||
| Borderline | 676 (76.2) | 211 (23.8) | ||
| No | 34,207 (97.1) | 1035 (2.9) | ||
| Had at least 12 cups of alcoholic drink per year (%) ‡† | 157.612 | <0.001 | ||
| Yes | 25,714 (89.8) | 2932 (10.2) | ||
| No | 8981 (85.2) | 1559 (14.8) | ||
| Consumed over 100 cigarettes in lifetime (%) † | 26.543 | <0.001 | ||
| Yes | 16,589 (87.7) | 2321 (12.3) | ||
| No | 19,979 (89.3) | 2383 (10.7) | ||
| Food security (%) | 38.584 | <0.001 | ||
| Yes | 26,893 (89.4) | 3174 (10.6) | ||
| No | 5300 (86.7) | 812 (13.3) | ||
| PIR *† | 2.2 (1.2–4.2) | 1.8 (1.0–3.3) | 6.236 | <0.001 |
| Energy (kcal) | 1948.0 (1441.1–2612.0) | 1725.0 (1257.0–2329.0) | 7.599 | <0.001 |
| Protein (gm) | 72.3 (51.8–100.7) | 69.0 (49.3–94.0) | 3.809 | <0.001 |
| Carbohydrate (gm) | 236.6 (170.6–319.7) | 204.5 (147.4–278.1) | 8.295 | <0.001 |
| Total fat (gm) | 71.3 (47.6–102.3) | 64.6 (42.7–96.2) | 4.666 | <0.001 |
| Dietary fiber (gm) | 14.3 (9.3–21.2) | 14.1 (9.3–20.8) | 1.140 | 0.148 |
| Thiamin (Vitamin B1) (mg) | 1.4 (1.0–2.0) | 1.4 (0.9–1.9) | 2.685 | <0.001 |
| Riboflavin (Vitamin B2) (mg) | 1.8 (1.3–2.6) | 1.7 (1.2–2.3) | 4.151 | <0.001 |
| Vitamin B6 (mg) | 1.7 (1.1–2.5) | 1.6 (1.1–2.3) | 4.416 | <0.001 |
| Total folate (mcg) | 341.0 (230.0–496.0) | 320.0 (215.0–459.0) | 3.558 | <0.001 |
| Vitamin B12 (mcg) | 3.7 (2.1–6.2) | 3.4 (1.9–5.6) | 3.452 | <0.001 |
| Vitamin E (mg) | 6.5 (4.2–10.0) | 6.1 (3.8–9.3) | 3.294 | <0.001 |
| Calcium (mg) | 779.0 (496.0–1151.0) | 713.0 (468.0–1040.8) | 4.185 | <0.001 |
| Magnesium (mg) | 265.0 (190.0–363.0) | 249.0 (180.0–336.0) | 4.041 | <0.001 |
| Iron (mg) | 12.8 (8.9–18.4) | 12.3 (8.5–17.5) | 2.466 | <0.001 |
| Zinc (mg) | 9.7 (6.6–14.1) | 8.9 (6.1–13.0) | 3.824 | <0.001 |
| Copper (mg) | 1.1 (0.8–1.5) | 1.0 (0.7–1.4) | 4.124 | <0.001 |
| Insulin (uU/mL) † | 9.5 (6.2–15.2) | 14.7 (8.8–25.0) | 10.705 | <0.001 |
| Glucose (mg/dL) † | 91.0 (85.0–99.0) | 149.0 (118.0–149.0) | 45.353 | <0.001 |
| Hemoglobin (g/dL) † | 14.2 (13.2–15.2) | 13.9 (12.8–15.0) | 5.840 | <0.001 |
| Variables | Crude Model a | Model I b | Model II c | Robust Check Model d |
|---|---|---|---|---|
| β (SE) | β (SE) | β (SE) | β (SE) | |
| Energy (kcal) | −0.001 (0.0002) *** | −0.001 (0.0002) ** | −0.00003 (0.0003) | −0.00006 (0.0003) |
| Protein (gm) | 0.007 (0.002) *** | 0.006 (0.002) ** | 0.001 (0.003) | 0.001 (0.003) |
| Carbohydrate (gm) | −0.001 (0.001) | −0.0005 (0.001) | 0.0001 (0.001) | 0.0003 (0.001) |
| Total fat (gm) | 0.011 (0.002) *** | 0.010 (0.002) *** | −0.0005 (0.003) | −0.0001 (0.003) |
| Dietary fiber (gm) | 0.025 (0.005) *** | 0.011 (0.005) * | 0.004 (0.009) | 0.003 (0.009) |
| Thiamin (Vitamin B1) (mg) | 0.120 (0.049) * | 0.162 (0.053) ** | −0.011 (0.107) | −0.011 (0.108) |
| Riboflavin (Vitamin B2) (mg) | 0.034 (0.045) | −0.012 (0.050) | 0.017 (0.085) | 0.026 (0.085) |
| Vitamin B6 (mg) | −0.091 (0.037) * | −0.058 (0.039) | −0.157 (0.070) * | −0.165 (0.070) * |
| Total folate (mcg) | −0.0004 (0.0002) | −0.0003 (0.0002) | 0.001 (0.0004) | 0.001 (0.0004) |
| Vitamin B12 (mcg) | −0.001 (0.005) | −0.005 (0.006) | 0.006 (0.008) | 0.005 (0.008) |
| Vitamin E (mg) | −0.017 (0.007) * | −0.012 (0.007) | −0.013 (0.013) | −0.014 (0.013) |
| Calcium (mg) | −0.00008 (0.00008) | 0.0001 (0.00008) | 0.00002 (0.0001) | −0.00002 (0.0001) |
| Magnesium (mg) | −0.001 (0.0005) | −0.001 (0.0005) | 0.001 (0.001) | 0.001 (0.001) |
| Iron (mg) | 0.022 (0.006) ** | 0.015 (0.007) * | −0.002 (0.012) | 0.0004 (0.012) |
| Zinc (mg) | −0.020 (0.007) ** | −0.015 (0.007) * | −0.007 (0.013) | −0.005 (0.013) |
| Copper (mg) | −0.027 (0.058) | −0.002 (0.057) | −0.077 (0.086) ** | −0.061 (0.090) |
| Age (<40 years old) | - | Reference | Reference | Reference |
| Age (40−59 years old) | - | 2.211 (0.103) *** | 0.985 (0.190) *** | 0.978 (0.191) *** |
| Age (≥ 60 years old) | - | 1.561 (0.104) *** | 0.792 (0.189) *** | 0.782 (0.189) *** |
| Gender (male) | - | 0.230 (0.058) *** | 0.322 (0.117) ** | 0.311 (0.118) ** |
| Race (other races) | - | Reference | Reference | Reference |
| Race (Mexican American) | - | −0.551 (0.083) *** | −0.269 (0.150) | −0.229 (0.151) |
| Race (non-Hispanic Black) | - | 0.298 (0.089) ** | 0.342 (0.163) * | 0.396 (0.164) * |
| Race (non-Hispanic White) | - | 0.209 (0.091) * | −0.024 (0.170) | 0.043 (0.172) |
| Education level (≤ high school) | - | - | 0.179 (0.107) | 0.187 (0.108) |
| BMI † (<25.0) | - | - | Reference | Reference |
| BMI (25.0–29.9) | - | - | 0.726 (0.146) *** | 0.714 (0.146) *** |
| BMI (≥30.0) | - | - | 0.081 (0.156) | 0.076 (0.156) |
| Moderate/severe physical activity (no) | - | - | 0.114 (0.103) | 0.076 (0.104) |
| Hypertension (yes) | - | - | 0.296 (0.100) ** | 0.323 (0.100) |
| The doctor told you that you had diabetes (no) | - | - | Reference | Reference |
| The doctor told you that you had diabetes (borderline) | - | - | 2.501 (0.106) *** | 2.491 (0.106) *** |
| The doctor told you that you had diabetes (yes) | - | - | 1.167 (0.196) *** | 1.141 (0.196) *** |
| Had at least 12 cups alcoholic drink per year (yes) | - | - | −0.057 (0.112) | −0.077 (0.113) |
| Consumed over 100 cigarettes in their lifetime (yes) | - | - | −0.085 (0.103) | −0.073 (0.104) |
| Food security (no) | - | - | 0.076 (0.135) | 0.047 (0.137) |
| PIR † | - | - | −0.049 (0.036) | −0.048 (0.036) |
| Insulin (uU/mL) | - | - | 0.003 (0.002) | 0.003 (0.002) |
| Glucose (mg/dL) | - | - | 0.061 (0.002) *** | 0.061 (0.002) *** |
| Hemoglobin (g/dL) | - | - | −0.095 (0.036) ** | −0.086 (0.036) * |
| Years fixed effect | - | - | - | Included |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, Y.; Zhang, H.; Yang, J.; Peng, L. The Association between Daily Total Dietary Nutrient Intake and Recent Glycemic Control States of Non-Pregnant Adults 20+ Years Old from NHANES 1999–2018 (Except for 2003–2004). Nutrients 2021, 13, 4168. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114168
Bai Y, Zhang H, Yang J, Peng L. The Association between Daily Total Dietary Nutrient Intake and Recent Glycemic Control States of Non-Pregnant Adults 20+ Years Old from NHANES 1999–2018 (Except for 2003–2004). Nutrients. 2021; 13(11):4168. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114168
Chicago/Turabian StyleBai, Yin, Hao Zhang, Jie Yang, and Lei Peng. 2021. "The Association between Daily Total Dietary Nutrient Intake and Recent Glycemic Control States of Non-Pregnant Adults 20+ Years Old from NHANES 1999–2018 (Except for 2003–2004)" Nutrients 13, no. 11: 4168. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114168