
A Generation Shift in Mediterranean Diet Adherence and Its Association with Biological Markers and Health in Dalmatia, Croatia

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
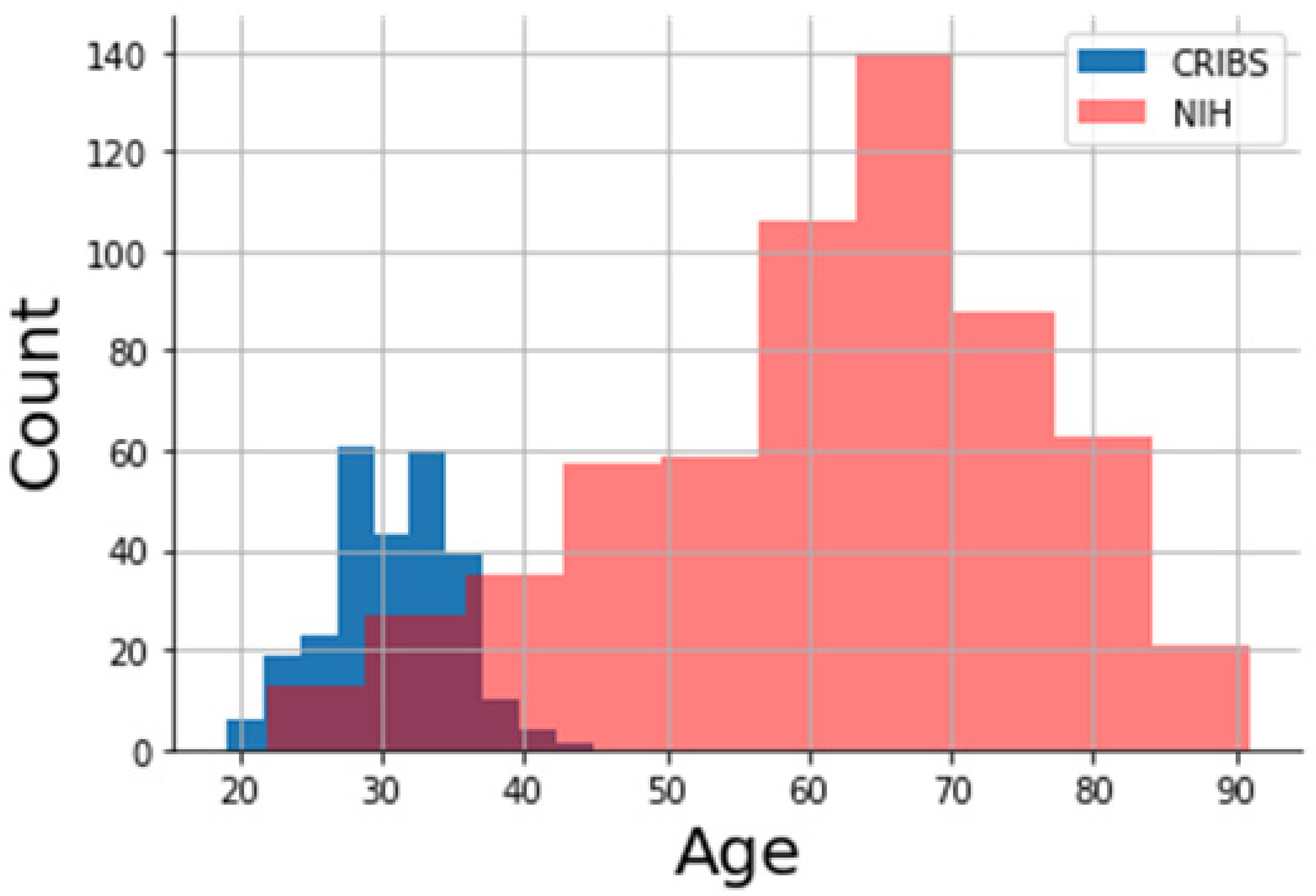
3.1. Differences between the Cohorts
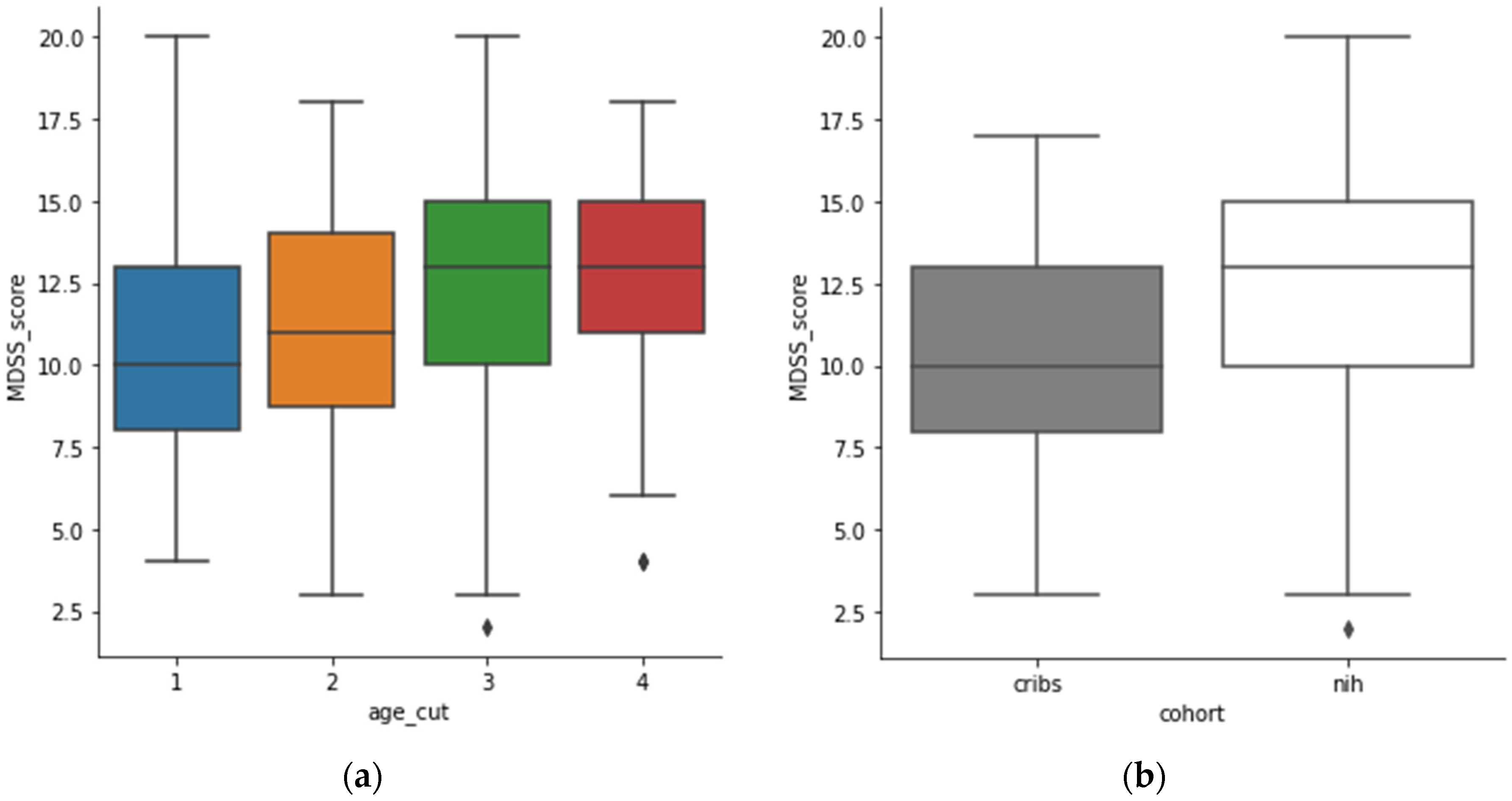
3.2. Adherence to Mediterranean Diet Associates with Increasing Age
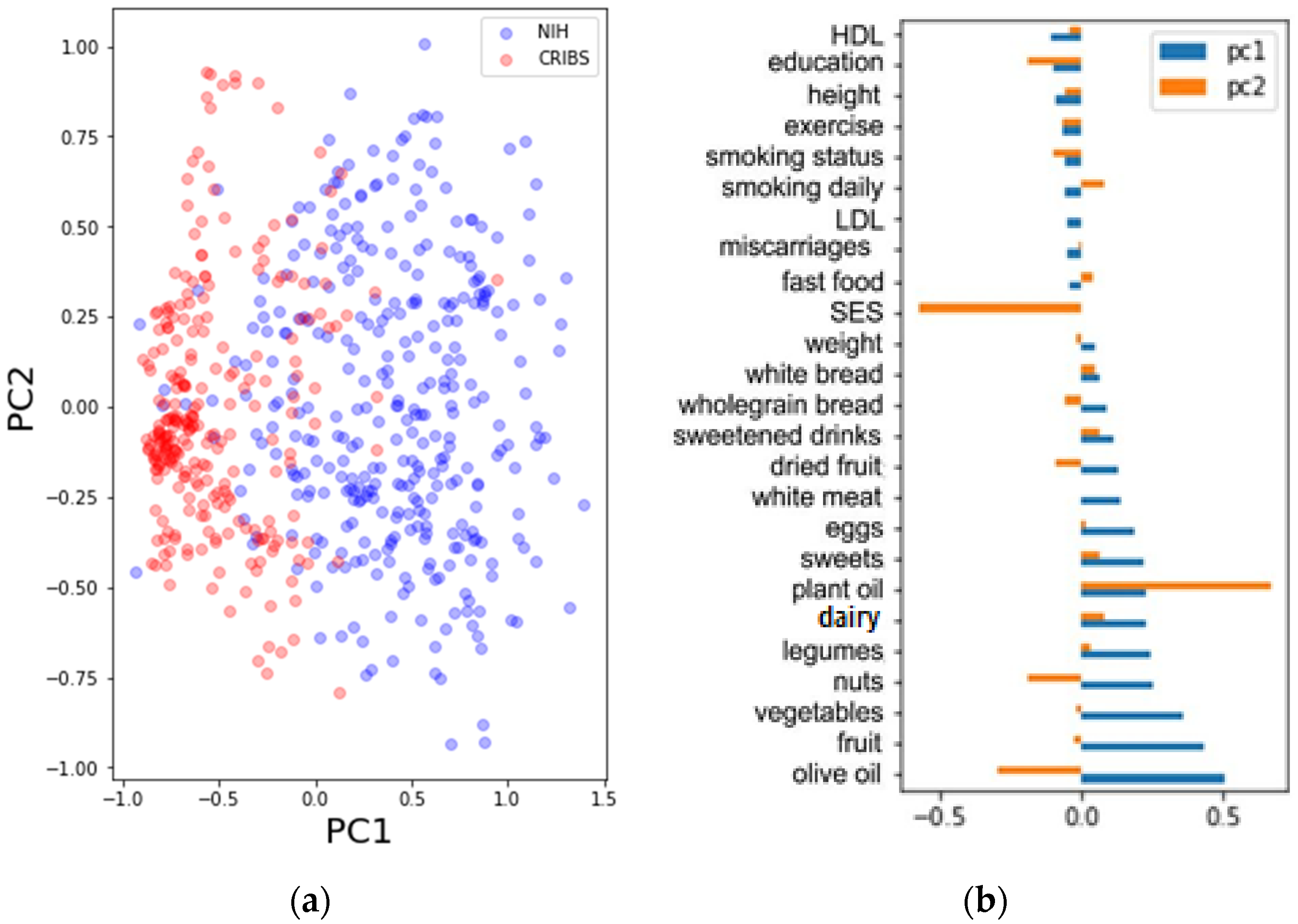
3.3. Lifestyle Is Associated with Mediterranean Dietary Pattern
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variable Short Name | Variable Description | Included in Model | Excluded in Stat | Excluced in PCA | Exlcuded in GLS |
|---|---|---|---|---|---|
| dairy | daily consummation of dairy | ||||
| systolic blood pressure | systolic blood pressure value | x | x | ||
| other fat, oil | daily consummation of oil (excl. olive and plant oil) | x | x | ||
| dried fruit | daily consummation of dried fruit | ||||
| vegetables | daily consummation of vegetables | ||||
| wholegrain bread | daily consummation of wholegrain bread | ||||
| equipment | measure of socieconomic status according to equipment in the household | ||||
| total cholesterol | total cholesterol value | x | x | ||
| fast food | daily consummation of fast food | ||||
| potatoes | daily consummation of potatoes | x | x | ||
| height | height | ||||
| financial status | monthly household income | x | x | ||
| pasta, rice | daily consummation of pasta and rice | x | x | ||
| red meat | daily consummation of red meat | x | x | ||
| eggs | daily consummation of eggs | ||||
| age | age | x | |||
| sweetened drinks | daily consummation of sweetened drinks | ||||
| glucose | fasting glucose value | x | x | ||
| nuts | daily consummation of nuts | ||||
| number pregnancy | number of pregnancies or parity | x | x | ||
| diastolic blood pressure | diastolic blood pressure value | x | x | ||
| fruit | daily consummation of fruit | ||||
| MDSS 2 kat | Mediterranean Diet Serving Score in two categories (low and high) | x | x | x | |
| white meat | daily consummation of white meat | ||||
| smoking years | years of smoking | x | x | ||
| miscarriages | number of miscarriages | ||||
| HDL | HDL cholesterol value | ||||
| smoking daily | daily number of cigarettes | ||||
| cohort | NIH and CRIBS cohort | x | x | x | |
| fish | daily consummation of fish | x | x | ||
| white bread | daily consummation of white bread | ||||
| MDSS score | Mediterranean Diet Serving Score in numbers (12.5 cut-off) | x | x | x | |
| BMI | body mass index | x | x | ||
| sweets | daily consummation of sweets | ||||
| olive oil | daily consummation of olive oil | ||||
| exercise | daily activity level in three categories (low, moderate, high) | ||||
| sex | sex | x | x | x | |
| legumes | daily consummation of legumes | ||||
| triglycerides | triglyceride value | x | x | ||
| LDL | LDL cholesterol value | ||||
| smoking status | smoking status in three categories (smoker, non-smoker, ex-smoker) | ||||
| location | mainland vs. islands | x | x | x | |
| plant oil | daily consummation of plant oil | ||||
| working status | working/employment status | x | x | ||
| education | education level | ||||
| weight | weight |
References
- Keys, A.S.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Karvonen, M.; Kimura, N.; Menotti, A.; et al. Seven Countries: A Multivariate Analysis of Death and Coronary Heart Disease; Harvard University Press: Cambridge, MA, USA; London, UK, 1980; pp. 1–381. [Google Scholar]
- Menotti, A.; Kromhout, D.; Blackburn, H.; Fidanza, F.; Buzina, R.; Nissinen, A. Food intake patterns and 25-year mortality from coronary heart disease: Cross-cultural correlations in the seven countries study. Eur. J. Epidemiol. 1999, 15, 507–515. [Google Scholar] [CrossRef]
- Shen, J.; Wilmot, K.A.; Ghasemzadeh, N.; Molloy, D.L.; Burkman, G.; Mekonnen, G.; Gongora, M.C.; Quyyumi, A.A.; Sperling, L.S. Mediterranean Dietary Patterns and Cardiovascular Health. Annu. Rev. Nutr. 2015, 35, 425–449. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A journey into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analyses. BMJ Open 2015, 5, e008222. [Google Scholar] [CrossRef] [Green Version]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E. The role of the Mediterranean diet on weight loss and obesity-related diseases. Rev. Endocr. Metab. Disord. 2020, 21, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Guyomard, H.; Darcy-Vrillon, B.; Esnouf, C.; Marin, M.; Russel, M.; Guillou, M. Eating patterns and food systems: Critical knowledge requirements for policy design and implementation. Agric. Food Secur. 2012, 1, 13. [Google Scholar] [CrossRef] [Green Version]
- Foscolou, A.; Tyrovolas, S.; Soulis, G.; Mariolis, A.; Piscopo, S.; Valacchi, G.; Anastasiou, F.; Lionis, C.; Zeimbekis, A.; Tur, J.A.; et al. The Impact of the Financial Crisis on Lifestyle Health Determinants Among Older Adults Living in the Mediterranean Region: The Multinational MEDIS Study (2005–2015). J. Prev. Med. Public Health 2017, 50, 19. [Google Scholar] [CrossRef] [PubMed]
- Hachem, F.; Capone, R.; Yannakoulia, M.; Dernini, S.; Hwalla, N.; Kalaitzidis, C. The Mediterranean diet: A sustainable food consumption pattern. In Mediterra 2016. Zero Waste in the Mediterranean; Presses de Sciences Po: Paris, France, 2016; pp. 243–259. [Google Scholar]
- Grosso, G.; Marventano, S.; Giorgianni, G.; Raciti, T.; Galvano, F.; Mistretta, A. Mediterranean Diet Adherence Rates in Sicily, Southern Italy. Multicent. Study Public Health Nutr. 2014, 17, 2001–2009. [Google Scholar] [CrossRef]
- Cuschieri, S.; Libra, M. Adherence to the Mediterranean Diet in Maltese Adults. Int. J. Environ. Res. Public Health 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- García Cabrera, S.; Herrera Fernández, N.; Rodríguez Hernández, C.; Nissensohn, M.L.; Román-Viñas, B.; Serra-Majem, L. Kidmed Test; Prevalence of Low Adherence to the Mediterranean Diet in Children and Young; A Systematic Review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar] [CrossRef]
- Rosi, A.; Paolella, G.; Biasini, B.; Scazzina, F.; SINU Working Group on Nutritional Surveillance in Adolescents. Dietary habits of adolescents living in North America, Europe or Oceania: A review on fruit, vegetable and legume consumption, sodium intake, and adherence to the Mediterranean Diet. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 544–560. [Google Scholar] [CrossRef]
- Ruggiero, E.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; Bracone, F.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M.; et al. Socioeconomic and psychosocial determinants of adherence to the Mediterranean diet in a general adult Italian population. Eur. J. Public Health 2018, 29, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Missoni, S.; Šarac, J. Population Dynamics, Dietary Habits and Lifestyle Changes in the Eastern Adriatic: A Review. In Biological Implications of Human Mobility; Koziel, S., Chakraborty, R., Bose, K., Eds.; Nova Science Publishers, Inc.: New York, NY, USA, 2016; pp. 187–200. [Google Scholar]
- Havaš Auguštin, D.; Šarac, J.; Lovrić, M.; Živković, J.; Malev, O.; Fuchs, N.; Novokmet, N.; Turkalj, M.; Missoni, S. Adherence to Mediterranean Diet and Maternal Lifestyle during Pregnancy: Island-Mainland Differentiation in the CRIBS Birth Cohort. Nutrients 2020, 12, 2179. [Google Scholar] [CrossRef] [PubMed]
- Deka, R.; Smolej Narancic, N.; Xi, H.; Turek, S.; Cubrilo Turek, M.; Vrhovski-Hebrang, D.; Janicijevic, B.; Szirovicza, L.; Rudan, I.; Jin, L.; et al. Metabolic syndrome in an island population of the Eastern Adriatic coast of Croatia. Coll. Anthropol. 2008, 32, 85–91. [Google Scholar]
- Deka, R.; Durakovic, Z.; Niu, W.; Zhang, G.; Karns, R.; Smolej-Narancic, N.; Missoni, S.; Caric, D.; Caric, T.; Rudan, D.; et al. Prevalence of metabolic syndrome and related metabolic traits in an island population of the Adriatic. Ann. Ann. Hum. Biol. 2012, 39, 46–53. [Google Scholar] [CrossRef]
- Perinić Lewis, A.; Zajc Petranović, M.; Carić, T.; Pribačić Ambrožić, V.; Karelović, D.; Janković, S.; Missoni, S.A. sociodemographic profile of the participants in the Croatian Islands’ Birth Cohort Study (CRIBS). Hrvat. Geogr. Glas. 2019, 81, 83–105. [Google Scholar] [CrossRef] [Green Version]
- Šarac, J.; Ilić, S.; Zajc Petranović, M.; Havaš Auguštin, D.; Novokmet, N.; Cameron, N.; Missoni, S. The association between maternal anthropometry and blood pressure in pregnancy—Results from the Croatian Islands’ Birth Cohort Study (CRIBS). MEBM 2019, 2, 33–39. [Google Scholar]
- Sahay, R.D.; Couch, S.C.; Missoni, S.; Sujoldžić, A.; Novokmet, N.; Duraković, Z.; Rao, M.B.; Musić Milanović, S.; Deka, R.; Vuletić, S.; et al. Dietary Patterns in Adults from an Adriatic Island of Croatia and their Associations with Metabolic Syndrome and its Components. Coll. Antropol. 2013, 37, 335–342. [Google Scholar]
- Sahay, R.D.; Ollberding, N.J.; Missoni, S.; Novokmet, N.; Šarac, J.; Šarić, T.; Rao, M.B.; Rudan, P.; Deka, R. Fish and Shellfish Intake and Diabetes in a Costal Population of the Adriatic. Coll. Antropol. 2015, 39, 401–409. [Google Scholar]
- Monteagudo, C.; Mariscal-Arcas, M.; Rivas, A.; Lorenzo-Tovar, M.L.; Tur, J.A.; Olea-Serrano, F. Proposal of a Mediterranean Diet Serving Score. PLoS ONE 2015, 10, e0128594. [Google Scholar] [CrossRef] [Green Version]
- Seabold, S.; Perktold, J. Statsmodels: Econometric and Statistical Modeling with Python Quantitative histology of aorta View project Statsmodels: Econometric and Statistical Modeling with Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; pp. 92–96. [Google Scholar]
- Abdi, H.; Williams, L.J. Principal component analysis. Wiley Interdiscip. Rev. Comput. Stat. 2010, 2, 433–459. [Google Scholar]
- Bibiloni, M.D.M.; González, M.; Julibert, A.; Llompart, I.; Pons, A.; Tur, J.A. Ten-Year Trends (1999–2010) of Adherence to the Mediterranean Diet among the Balearic Islands’ Adult Population. Nutrients 2017, 9, 749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnaba, L.; Intorre, F.; Azzini, E.; Ciarapica, D.; Venneria, E.; Foddai, M.S.; Maiani, F.; Raguzzini, A.; Polito, A. Evaluation of adherence to Mediterranean diet and association with clinical and biological markers in an Italian population. Nutrition 2020, 77, 110813. [Google Scholar] [CrossRef] [PubMed]
- de Wolff, M.G.; Backhausen, M.G.; Iversen, M.L.; Bendix, J.M.; Rom, A.L.; Hegaard, H.K. Prevalence and predictors of maternal smoking prior to and during pregnancy in a regional Danish population: A cross-sectional study. Reprod. Health 2019, 16, 82. [Google Scholar] [CrossRef] [Green Version]
- Neuenschwander, M.; Hoffmann, G.; Schwingshackl, L.; Schlesinger, S. Impact of different dietary approaches on blood lipid control in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Eur. J. Epidemiol. 2019, 34, 837–852. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [Green Version]



| Variable | Category | CRIBS N (%) | NIH N (%) | p Value |
|---|---|---|---|---|
| age | 19–31 | 151 (56.8%) | 14 (4%) | <0.001 |
| 32–46 | 115 (43.2%) | 49 (14.2%) | ||
| 47–64 | 0 (0%) | 128 (37.2%) | ||
| 65–91 | 0 (0%) | 153 (44.5%) | ||
| smoking status | smokers | 62 (23.3%) | 84 (24.4%) | >0.05 |
| non-smokers | 204 (76.7%) | 260 (75.6%) | ||
| education | high | 125 (47%) | 65 (18.9%) | <0.001 |
| low | 141 (53%) | 279 (81.1%) | ||
| employment status | employed | 209 (78.6%) | 112 (32.%) | <0.001 |
| unemployed | 57 (21.4%) | 232 (67.4%) | ||
| financial status | high | 78 (29.3%) | 69 (20.1%) | <0.01 |
| medium | 169 (63.5%) | 241 (70%) | ||
| low | 19 (7.1%) | 34 (9.9%) | ||
| MDSS score | high | 74 (27.8%) | 184 (53.5%) | <0.001 |
| low | 192 (72.2%) | 160 (46.5%) |
| Variable | Coefficient | p-Value |
|---|---|---|
| vegetables | 0.736 | 0.000 |
| smoking status | −0.359 | 0.000 |
| HDL | −0.39 | 0.000 |
| smoking daily | −0.482 | 0.000 |
| sweets | 0.251 | 0.000 |
| white meat | 0.297 | 0.001 |
| education | −0.164 | 0.001 |
| fruit | 0.157 | 0.001 |
| dairy | 0.125 | 0.006 |
| height | −0.183 | 0.006 |
| miscarriages | −0.186 | 0.006 |
| dried fruit | −0.18 | 0.008 |
| Variable | Low MDSS | High MDSS | p-Value |
|---|---|---|---|
| smoking | 6.81 | 3.644 | <0.001 |
| diastolic blood pressure | 71.026 | 75.081 | <0.001 |
| glucose | 5.091 | 5.521 | <0.001 |
| systolic blood pressure | 121.971 | 126.586 | <0.01 |
| HDL | 1.756 | 1.668 | <0.01 |
| BMI | 24.084 | 25.26 | <0.01 |
| triglycerides | 1.705 | 1.566 | <0.01 |
| total cholesterol | 6.433 | 6.121 | <0.01 |
| LDL | 3.93 | 3.783 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šarac, J.; Havaš Auguštin, D.; Lovrić, M.; Stryeck, S.; Šunić, I.; Novokmet, N.; Missoni, S. A Generation Shift in Mediterranean Diet Adherence and Its Association with Biological Markers and Health in Dalmatia, Croatia. Nutrients 2021, 13, 4564. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124564
Šarac J, Havaš Auguštin D, Lovrić M, Stryeck S, Šunić I, Novokmet N, Missoni S. A Generation Shift in Mediterranean Diet Adherence and Its Association with Biological Markers and Health in Dalmatia, Croatia. Nutrients. 2021; 13(12):4564. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124564
Chicago/Turabian StyleŠarac, Jelena, Dubravka Havaš Auguštin, Mario Lovrić, Sarah Stryeck, Iva Šunić, Natalija Novokmet, and Saša Missoni. 2021. "A Generation Shift in Mediterranean Diet Adherence and Its Association with Biological Markers and Health in Dalmatia, Croatia" Nutrients 13, no. 12: 4564. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124564