Association of Nutrition Education and Its Interaction with Lifestyle Factors on Kidney Function Parameters and Cardiovascular Risk Factors among Chronic Kidney Disease Patients in Taiwan

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
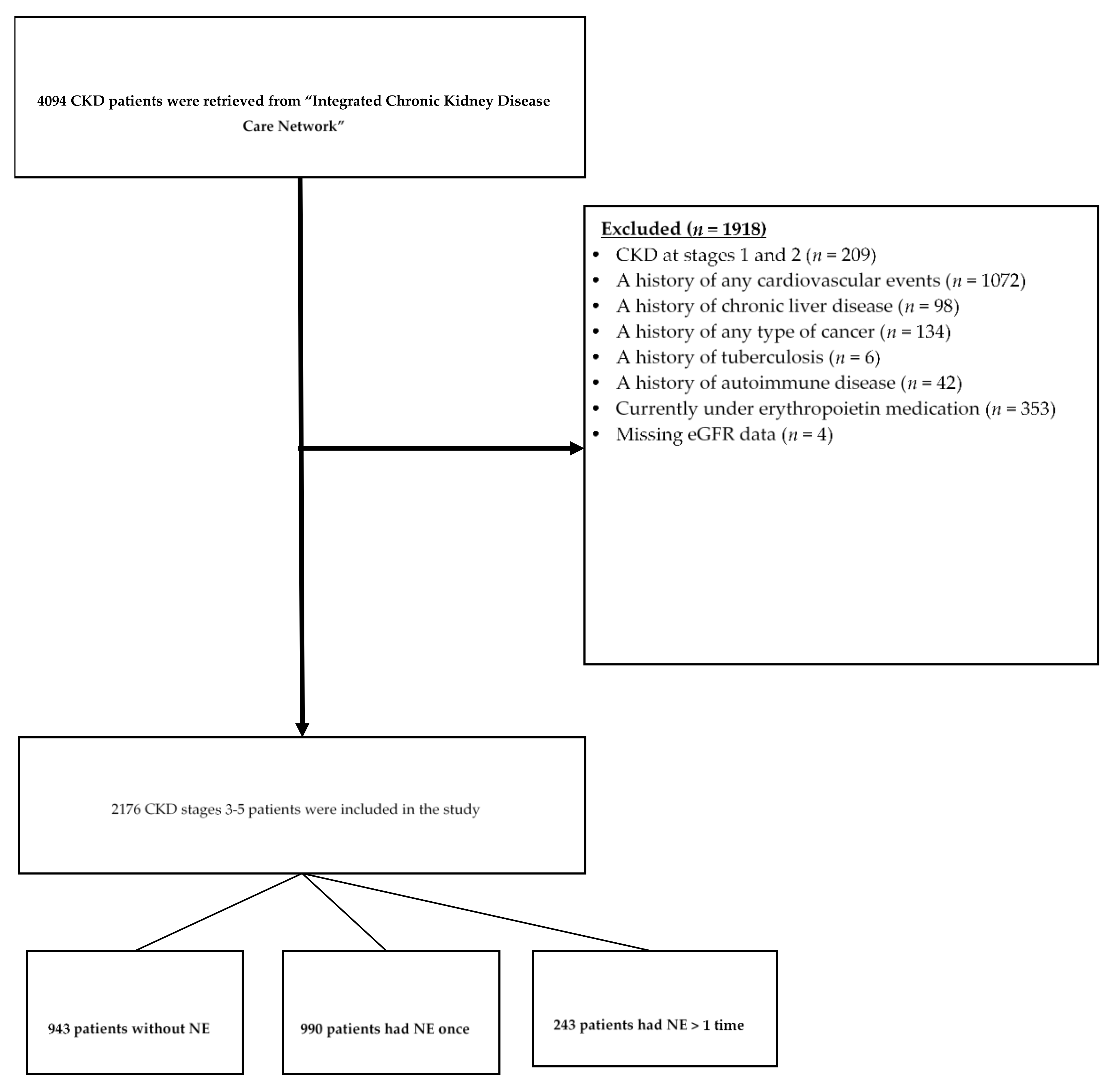
2.1. Study Subjects and Nutrition Education
2.2. Sociodemographic Data, Lifestyle, and Use of Drugs
2.3. Clinical and Biochemical Data
2.4. Statistical Analysis
3. Results
3.1. Characteristics, Clinical Data, and Biochemical Measures of the Study Patients
3.2. Nutrition Education and Kidney Function
3.3. Nutrition Education and Cardiovascular Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Health Promotion Administration, Ministry of Health and Welfare, Taiwan. 2019 Health Promotion Administration Annual Report. Available online: https://www.hpa.gov.tw/EngPages/Detail.aspx?nodeid=1070&pid=12811 (accessed on 12 August 2020).
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.; Albertus, P.; Ayanian, J.; Balkrishnan, R.; Bragg-Gresham, J.; Cao, J.; Chen, J.L.; et al. US Renal Data System 2016 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2017, 69, A7–A8. [Google Scholar] [CrossRef]
- Tsai, M.H.; Hsu, C.Y.; Lin, M.Y.; Yen, M.F.; Chen, H.H.; Chiu, Y.H.; Hwang, S.J. Incidence, prevalence, and duration of chronic kidney disease in Taiwan: Results from a community-based screening program of 106,094 individuals. Nephron 2018, 140, 175–184. [Google Scholar] [CrossRef]
- National Health Insurance Administration, Ministry of Health and Welfare, Taiwan. National Health Insurance Annual Statistical Report 2018. Available online: https://www.nhi.gov.tw/english/Content_List.aspx?n=AB41B66610EAC01A&topn=616B97F8DF2C3614 (accessed on 12 August 2020).
- Herzog, C.A.; Asinger, R.W.; Berger, A.K.; Charytan, D.M.; Diez, J.; Hart, R.G.; Eckardt, K.U.; Kasiske, B.L.; McCullough, P.A.; Passman, R.S.; et al. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011, 80, 572–586. [Google Scholar] [CrossRef] [Green Version]
- Coresh, J.; Turin, T.C.; Matsushita, K.; Sang, Y.; Ballew, S.H.; Appel, L.J.; Arima, H.; Chadban, S.J.; Cirillo, M.; Djurdjev, O.; et al. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA 2014, 311, 2518–2531. [Google Scholar] [CrossRef] [Green Version]
- Menon, V.; Gul, A.; Sarnak, M.J. Cardiovascular risk factors in chronic kidney disease. Kidney Int. 2005, 68, 1413–1418. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.P.; Cheng, T.Y.D.; Tsai, M.K.; Chang, Y.C.; Chan, H.T.; Tsai, S.P.; Chiang, P.H.; Hsu, C.C.; Sung, P.K.; Hsu, Y.H.; et al. All-cause mortality attributable to chronic kidney disease: A prospective cohort study based on 462 293 adults in Taiwan. Lancet 2008, 371, 2173–2182. [Google Scholar] [CrossRef]
- Parikh, N.I.; Hwang, S.J.; Larson, M.G.; Meigs, J.B.; Levy, D.; Fox, C.S. Cardiovascular disease risk factors in chronic kidney disease: Overall burden and rates of treatment and control. Arch. Intern. Med. 2006, 166, 1884–1891. [Google Scholar] [CrossRef] [Green Version]
- Dhingra, R.; Sullivan, L.M.; Fox, C.S.; Wang, T.J.; D’Agostino, R.B.; Gaziano, J.M.; Vasan, R.S. Relations of serum phosphorus and calcium levels to the incidence of cardiovascular disease in the community. Arch. Intern. Med. 2007, 167, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Shanahan, C.M.; Crouthamel, M.H.; Kapustin, A.; Giachelli, C.M. Arterial calcification in chronic kidney disease: Key roles for calcium and phosphate. Circ. Res. 2011, 109, 697–711. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P.; Kuchmak, O.; Lu, J.L.; Kalantar-Zadeh, K. Outcomes associated with serum calcium level in men with non-dialysis-dependent chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 468–476. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G. National kidney foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- Hernández Morante, J.J.; Sanchez-Villazala, A.; Cutillas, R.C.; Fuentes, M.C.C. Effectiveness of a nutrition education program for the prevention and treatment of malnutrition in end-stage renal disease. J. Renal Nutr 2014, 24, 42–49. [Google Scholar] [CrossRef]
- Mason, J.; Khunti, K.; Stone, M.; Farooqi, A.; Carr, S. Educational interventions in kidney disease care: A systematic review of randomized trials. Am. J. Kidney Dis. 2008, 51, 933–951. [Google Scholar] [CrossRef]
- Paes-Barreto, J.G.; Silva, M.I.B.; Qureshi, A.R.; Bregman, R.; Cervante, V.F.; Carrero, J.J.; Avesani, C.M. Can renal nutrition education improve adherence to a low-protein diet in patients with stages 3 to 5 chronic kidney disease? J. Ren. Nutr. 2013, 23, 164–171. [Google Scholar] [CrossRef]
- Campbell, K.L.; Ash, S.; Bauer, J.D. The impact of nutrition intervention on quality of life in pre-dialysis chronic kidney disease patients. Clin. Nutr. 2008, 27, 537–544. [Google Scholar] [CrossRef]
- Michishita, R.; Matsuda, T.; Kawakami, S.; Kiyonaga, A.; Tanaka, H.; Morito, N.; Higaki, Y. The association between unhealthy lifestyle behaviors and the prevalence of chronic kidney gisease (CKD) in middle-aged and older men. J. Epidemiol. 2016, 26, 378–385. [Google Scholar] [CrossRef] [Green Version]
- Muga, M.A.; Owili, P.O.; Hsu, C.Y.; Chao, J.C. Association of lifestyle factors with blood lipids and inflammation in adults aged 40 years and above: A population-based cross-sectional study in Taiwan. BMC Public Health 2019, 19, 1346. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.J.; Lin, K.R.; Lin, M.T.; Chang, J.L. Association between lifestyle factors and decreased kidney function in older adults: A community-based cross-sectional analysis of the Taipei City elderly health examination database. BMC Nephrol. 2020, 21, 1–10. [Google Scholar] [CrossRef]
- Evans, M.; Bower, H.; Cockburn, E.; Jacobson, S.H.; Barany, P.; Carrero, J.J. Contemporary management of anaemia, erythropoietin resistance and cardiovascular risk in patients with advanced chronic kidney disease: A nationwide analysis. Clin. Kidney, J. 2020, 13, 821–827. [Google Scholar] [CrossRef]
- Payne, R.B.; Little, A.J.; Williams, R.B.; Milner, J.R. Interpretation of serum calcium in patients with abnormal serum proteins. Br. Med. J. 1973, 4, 643–646. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [Green Version]
- Bailie, G.R.; Massry, S.G.; National Kidney, F. Clinical practice guidelines for bone metabolism and disease in chronic kidney disease: An overview. Pharmacotherapy 2005, 25, 1687–1707. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J. Chronic kidney disease. Lancet 2012, 379, 165–180. [Google Scholar] [CrossRef]
- Richardson, D.B.; Kaufman, J.S. Estimation of the relative excess risk due to interaction and associated confidence bounds. Am. J. Epidemiol. 2009, 169, 756–760. [Google Scholar] [CrossRef] [Green Version]
- Knol, M.J.; VanderWeele, T.J.; Groenwold, R.H.H.; Klungel, O.H.; Rovers, M.M.; Grobbee, D.E. Estimating measures of interaction on an additive scale for preventive exposures. Eur. J. Epidemiol. 2011, 26, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Bergstrom, J.; Lindholm, B. Malnutrition, cardiac disease, and mortality: An integrated point of view. Am. J. Kidney Dis. 1998, 32, 834–841. [Google Scholar] [CrossRef]
- Anderson, C.A.M.; Nguyen, H.A. Nutrition education in the care of patients with chronic kidney disease and end-stage renal disease. Semin. Dial. 2018, 31, 115–121. [Google Scholar] [CrossRef]
- Mitch, W.E.; Remuzzi, G. Diets for patients with chronic kidney disease, still worth prescribing. J. Am. Soc. Nephrol. 2004, 15, 234–237. [Google Scholar] [CrossRef] [Green Version]
- Fouque, D.; Aparicio, M. Eleven reasons to control the protein intake of patients with chronic kidney disease. Nat. Clin. Pract Nephrol 2007, 3, 383–392. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Fumagalli, G.; Vigo, V.; Meola, M.; Cianchi, C.; Egidi, M.F. Nutrition and physical activity in CKD patients. Kidney Blood Press. Res. 2014, 39, 107–113. [Google Scholar] [CrossRef]
- Lopez-Vargas, P.A.; Tong, A.; Howell, M.; Craig, J.C. Educational interventions for patients with CKD: A systematic review. Am. J. Kidney Dis. 2016, 68, 353–370. [Google Scholar] [CrossRef]
- Jahanpeyma, P.; Makhdoomi, K.; Sajadi, S.A. The effect of nutrition education program on biochemical parameters among patients with chronic kidney disease undergoing hemodialysis. Crit. Care Nurs. J. 2017, 10, e12453. [Google Scholar] [CrossRef] [Green Version]
- Jafari, F.; Hashemi, N.; Reisi, M. The effect of diet training on variations in blood pressure, weight, and some biochemical factors in hemodialysis patients: A clinical trial. J. Clin. Nurs. Midwifery 2015, 3, 13–19. [Google Scholar]
- Ebrahimi, H.; Sadeghi, M. The effect of dietary regimen education on the laboratory variables in hemodialysis patients. J. Nurs. Educ. 2014, 2, 12–22. [Google Scholar]
- Naseri-Salahshour, V.; Sajadi, M.; Nikbakht-Nasrabadi, A.; Davodabady, F.; Fournier, A. The effect of nutritional education program on quality of life and serum electrolytes levels in hemodialysis patients: A single-blind randomized controlled trial. Patient Educ. Couns. 2020, 103, 1774–1779. [Google Scholar] [CrossRef]
- Miller, C.K.; Edwards, L.; Kissling, G.; Sanville, L. Nutrition education improves metabolic outcomes among older adults with diabetes mellitus: Results from a randomized controlled trial. Prev. Med. 2002, 34, 252–259. [Google Scholar] [CrossRef]
- Franz, M.J.; Monk, A.; Barry, B.; Mcclain, K.; Weaver, T.; Cooper, N.; Upham, P.; Bergenstal, R.; Mazze, R.S. Effectiveness of medical nutrition therapy provided by dietitians in the management of non-insulin-dependent diabetes-mellitus—A randomized, controlled clinical-trial. J. Am. Diet. Assoc. 1995, 95, 1009–1017. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional management of chronic kidney disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef]
- Wakasugi, M.; Kazama, J.J.; Yamamoto, S.; Kawamura, K.; Narita, I. A combination of healthy lifestyle factors is associated with a decreased incidence of chronic kidney disease: A population-based cohort study. Hypertens. Res. 2013, 36, 328–333. [Google Scholar] [CrossRef]
- Shankar, A.; Klein, R.; Klein, B.E.K. The association among smoking, heavy drinking, and chronic kidney disease. Am. J. Epidemiol. 2006, 164, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Parikh, N.I.; Hwang, S.J.; Larson, M.G.; Levy, D.; Fox, C.S. Chronic kidney disease as a predictor of cardiovascular disease (from the Framingham Heart Study). Am. J. Cardiol. 2008, 102, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Ellison, R.C.; Zhang, Y.Q.; Qureshi, M.M.; Knox, S.; Arnett, D.K.; Province, M.A. Lifestyle determinants of high-density lipoprotein cholesterol: The National Heart, Lung, and Blood Institute Family Heart Study. Am. Heart J. 2004, 147, 529–535. [Google Scholar] [CrossRef]
- Mukamal, K.J. The effects of smoking and drinking on cardiovascular disease and risk factors. Alcohol Res. Health 2006, 29, 199–202. [Google Scholar]
- Parsons, T.J.; Sartini, C.; Ash, S.; Lennon, L.T.; Wannamethee, S.G.; Lee, I.M.; Whincup, P.H.; Jefferis, B.J. Objectively measured physical activity and kidney function in older men; a cross-sectional population-based study. Age Ageing 2017, 46, 1010–1014. [Google Scholar] [CrossRef] [Green Version]
- Martens, R.J.H.; van der Berg, J.D.; Stehouwer, C.D.A.; Henry, R.M.A.; Bosma, H.; Dagnelie, P.C.; van Dongen, M.C.J.M.; Eussen, S.J.P.M.; Schram, M.T.; Sep, S.J.S.; et al. Amount and pattern of physical activity and sedentary behavior are associated with kidney function and kidney damage: The Maastricht Study. PLoS ONE 2018, 13, e0195306. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All (n = 2176) | Without Nutrition Education (n = 943) | With Nutrition Education (n = 1233) | pb |
|---|---|---|---|---|
| Age (years) | 72.0 (19.0) | 75.0 (18.0) | 70.0 (19.0) | <0.001 |
| Gender | 0.72 | |||
| Male | 1284 (59.0) | 552 (58.5) | 732 (59.4) | |
| Female | 892 (41.0) | 391 (41.5) | 501 (40.6) | |
| Education | <0.001 | |||
| <high school | 1453 (66.8) | 693 (73.5) | 760 (61.6) | |
| ≥high school | 723 (33.2) | 250 (26.5) | 473 (38.4) | |
| Marital status | 0.01 | |||
| Unmarried | 652 (30.0) | 310 (32.9) | 342 (27.7) | |
| Married | 1524 (70.0) | 633 (67.1) | 891 (72.3) | |
| Smoking | 0.24 | |||
| No | 1620 (74.4) | 714 (75.7) | 906 (73.5) | |
| Yes | 556 (25.5) | 229 (24.3) | 327 (26.5) | |
| Drinking | 0.51 | |||
| No | 1885 (86.6) | 822 (87.2) | 1063 (86.2) | |
| Yes | 291 (13.4) | 121 (12.8) | 170 (13.8) | |
| Chewing betel nut | 0.007 | |||
| No | 2097 (96.4) | 922 (97.8) | 1175 (95.3) | |
| Yes | 79 (3.6) | 21 (2.2) | 58 (4.7) | |
| Physical activity c | 0.002 | |||
| Inactive | 1527 (70.2) | 694 (73.6) | 833 (67.6) | |
| Active | 649 (29.8) | 249 (26.4) | 400 (32.4) | |
| Diuretic drugs user d | 541 (32.0) | 248 (36.0) | 293 (29.3) | 0.004 |
| Other drugs user e | 1871 (88.0) | 764 (84.9) | 1107 (90.3) | <0.001 |
| Characteristics | All (n = 2176) | Without Nutrition Education (n = 943) | With Nutrition Education (n = 1233) | pb |
|---|---|---|---|---|
| BMI (kg/m2) | 25.1 (5.3) | 25.0 (5.1) | 25.2 (5.5) | 0.012 |
| Systolic BP (mmHg) | 133.0 (24.0) | 132.0 (26.0) | 134.0 (23.0) | 0.28 |
| Diastolic BP (mmHg) | 72.0 (16.0) | 71.0 (16.0) | 72.0 (16.0) | 0.5 |
| FBG (mmol/L) | 6.0 (2.3) | 6.0 (2.5) | 5.9 (2.1) | 0.1 |
| HbA1c (%) | 6.3 (1.6) | 6.5 (1.8) | 6.2 (1.5) | <0.001 |
| Albumin (g/L) | 42.0 (7.0) | 41.0 (7.5) | 42.0 (7.0) | 0.002 |
| Blood lipids | ||||
| TG (mmol/L) | 1.4 (1.2) | 1.5 (1.2) | 1.4 (1.1) | 0.075 |
| TC (mmol/L) | 4.8 (1.6) | 4.8 (1.5) | 4.8 (1.6) | 0.89 |
| HDL-C (mmol/L) | 1.1 (0.5) | 1.1 (0.5) | 1.2 (0.5) | 0.07 |
| LDL-C (mmol/L) | 2.5 (1.1) | 2.6 (1.1) | 2.4 (1.1) | 0.005 |
| Minerals | ||||
| C-Ca (mmol/L) | 2.2 (0.1) | 2.2 (0.2) | 2.2 (0.1) | 0.09 |
| Phosphorus (mmol/L) | 1.3 (0.4) | 1.3 (0.4) | 1.3 (0.3) | 0.51 |
| Kidney function | ||||
| BUN (mmol/L) | 11.8 (9.3) | 12.1 (12.9) | 11.4 (7.9) | 0.001 |
| Serum creatinine (μmol/L) | 202.9 (166.2) | 207.6 (253.3) | 200.0 (133.8) | 0.04 |
| eGFR (mL/min/1.73 m2) | 29.2 (23.2) | 27.8 (27.9) | 30.2 (19.8) | 0.003 |
| Urinary protein | ||||
| Urine protein (g/L) | 0.7 (1.7) | 0.5 (1.4) | 0.8 (1.8) | <0.001 |
| Urine creatinine (mmol/L) | 7.0 (5.7) | 7.6 (6.2) | 6.7 (5.7) | < 0.001 |
| Urine protein to creatinine ratio (mg/mmol) c | 77.9 (219.3) | 82.6 (222.2) | 71.0 (199.8) | 0.019 |
| Chronic kidney disease stage, n (%) | <0.001 | |||
| Stage 3a | 272 (12.5) | 163 (17.3) | 109 (8.8) | |
| Stage 3b | 779 (35.8) | 264 (28.0) | 515 (41.8) | |
| Stage 4 | 665 (30.6) | 249 (26.4) | 416 (33.7) | |
| Stage 5 | 460 (21.1) | 267 (28.3) | 193 (15.7) |
| BUN (mmol/L) | Serum Creatinine (μmol/L) | eGFR (mL/min/1.73 m2) | Urine Protein (g/L) | Urine Creatinine (mmol/L) | Urine PCR (mg/mmol) | |
|---|---|---|---|---|---|---|
| With education | −4.16 (−5.14 to −3.19) ** | −122.78 (−145.76 to −99.81) ** | 2.92 (1.55 to 4.30) ** | −0.25 (−0.67 to 0.16) | −1.51 (−2.00 to −1.02) ** | −40.21 (−74.2 to −6.22) * |
| Nutrition education by smoking | ||||||
| Ref: without education, smoking | ||||||
| Non-smoking | −0.01 (−1.84 to 1.84) | −55.66 (−98.99 to −12.33) * | 2.32 (−0.28 to 4.92) | −0.16 (−0.95 to 0.63) | −0.83 (−1.76 to 0.11) | −70.68 (−131.72, −9.64) * |
| With education | ||||||
| Non-smoking | −4.04 (−5.81 to −2.28) ** | −162.07 (−203.56 to −120.59) ** | 4.92 (2.42 to 7.41) ** | −0.42 (−1.17 to 0.33) | −2.04 (−2.94 to −1.15) ** | −97.34 (−157.36 to −37.32) ** |
| Smoking | −4.52 (−6.40 to −2.63) ** | −168.79 (−213.13 to −124.44) ** | 3.83 (1.17 to 6.49) ** | −0.24 (−1.04 to 0.56) | −2.33 (−3.27 to −1.38) ** | −78.21 (−143.46 to −12.95) * |
| Nutrition education by drinking | ||||||
| Ref: without education, drinking | ||||||
| Non-drinking | 1.79 (−0.50 to 4.07) | 42.26 (−11.26 to 95.78) | −4.40 (−7.60 to −1.20) ** | −0.42 (−1.38 to 0.55) | −2.02 (−3.17 to −0.88) ** | 1.92 (−72.35 to 76.18) |
| With education | ||||||
| Non-drinking | −2.64 (−4.87 to −0.41) * | −83.92 (−136.15 to −31.69) ** | 4.31 (0.38 to 8.24) * | −0.69 (−1.63 to 0.25) | −3.24 (−4.36 to −2.13) ** | −42.03 (−115.61 to, 31.55) |
| Drinking | −2.50 (−5.10 to 0.11) | −101.65 (−162.66 to −40.64) ** | −0.79 (−4.44 to 2.86) | −0.13 (−1.22 to 0.97) | −3.27 (−4.57 to −1.98) ** | −17.18 (−106.36 to 72.01) |
| Nutrition education by physical activity | ||||||
| Ref: without education, inactive | ||||||
| Active | −2.14 (−3.84 to −0.45) * | −64.77 (−104.52 to −25.02) ** | 3.63 (1.24 to 6.01) ** | 0.03 (−0.69 to 0.76) | 1.39 (0.54 to 2.24) ** | −45.14 (−100,04 to 9.76) |
| With education | ||||||
| Inactive | −4.59 (−5.74 to −3.44) ** | −140.25 (−167.33 to −113.18) ** | 3.67 (2.04 to 5.29) ** | −0.20 (−0.69 to 0.29) | −0.95 (−1.52 to −0.37) ** | −45.09 (−85.56 to −4.62) * |
| Active | −5.25 (−6.67 to −3.82) ** | −144.47 (−177.98 to −110.96) ** | 4.73 (2.71 to 6.74) ** | −0.36 (−0.97 to 0.24) | −1.47 (−2.18 to −0.76) ** | −74.09 (−124.31 to −23.88) ** |
| High FBG (≥5.6 mmol/L) | High HbA1c (≥5.7%) | High TG (≥1.7 mmol/L) | High TC (≥5.2 mmol/L) | Low HDL-C (<1.04 mmol/L) | High LDL-C (≥2.6 mmol/L) | High C-Ca (≥2.4 mmol/L) | High P (≥1.5 mmol/L) | |
|---|---|---|---|---|---|---|---|---|
| n | 1400 | 1229 | 804 | 538 | 308 | 805 | 246 | 506 |
| With education | 0.88 (0.70–1.10) | 0.61 (0.45–0.82) ** | 0.72 (0.57–0.89) ** | 0.97 (0.75–1.25) | 0.68 (0.48–0.98) * | 0.76 (0.60–0.96) * | 0.81 (0.60–1.11) | 0.76 (0.59–0.98) * |
| Nutrition education by smoking | ||||||||
| Ref: without education, smoking | ||||||||
| Non-smoking | 1.23 (0.80–1.89) | 0.93 (0.51–1.69) | 0.97 (0.64–1.47) | 0.91 (0.57–1.48) | 0.73 (0.37–1.42) | 1.00 (0.64–1.55) | 0.58 (0.32–1.02) | 0.70 (0.44–1.11) |
| With education | ||||||||
| Non-smoking | 1.07 (0.72–1.61) | 0.59 (0.33–1.04) | 0.70 (0.47–1.03) | 0.92 (0.59–1.46) | 0.49 (0.26–0.92) * | 0.81 (0.53–1.24) | 0.55 (0.32–0.95) * | 0.54 (0.35–0.84) ** |
| Smoking | 0.90 (0.58–1.39) | 0.53 (0.30–0.96) * | 0.72 (0.47–1.09) | 0.89 (0.55–1.43) | 0.71 (0.37–1.35) | 0.62 (0.40–0.97) * | 0.50 (0.27–0.94) * | 0.72 (0.45–1.14) |
| RERI | −0.06 (−0.59–0.48) | 0.13 (−0.41–0.67) | 0.01 (−0.43–0.44) | 0.12 (−0.38–0.62) | 0.05 (−0.57–0.68) | 0.19 (−0.22–0.61) | 0.47 (0.09–0.85) * | 0.12 (−0.30–0.54) |
| AP | −0.05 (−0.54–0.43) | 0.22 (−0.78–1.22) | 0.01 (−0.62–0.64) | 0.13 (−0.44–0.70) | 0.11 (−1.22–1.43) | 0.24 (−0.32–0.80) | 0.86 (−0.11–1.83) | 0.23 (−0.61–1.06) |
| Nutrition education by drinking | ||||||||
| Ref: without education, drinking | ||||||||
| Non-drinking | 0.87 (0.51–1.49) | 0.80 (0.36–1.79) | 1.21 (0.73–2.03) | 0.95 (0.52–1.70) | 1.27 (0.55–2.94) | 0.67 (0.39–1.14) | 1.67 (0.71–3.91) | 1.31 (0.73–2.37) |
| With education | ||||||||
| Non-drinking | 0.75 (0.44–1.26) | 0.52 (0.24–1.13) | 0.83 (0.50–1.37) | 0.94 (0.53–1.67) | 0.84 (0.37–1.89) | 0.58 (0.32–1.05) | 1.36 (0.59–3.14) | 0.98 (0.55–1.75) |
| Drinking | 1.00 (0.54–1.87) | 0.40 (0.17–0.94) * | 0.96 (0.53–1.73) | 0.84 (0.43–1.65) | 0.81 (0.55–2.94) | 0.53 (0.32–0.90) * | 0.85 (0.31–2.35) | 0.85 (0.44–1.67) |
| RERI | −0.13 (−0.82–0.57) | 0.31 (−0.27–0.89) | −0.34 (−1.10–0.41) | 0.16 (−0.46–0.78) | −0.24 (−1.35–0.87) | 0.28 (−0.14–0.71) | −0.16 (−1.34–1.01) | −0.19 (−0.97–0.60) |
| AP | −0.17 (−1.04–0.70) | 0.60 (−0.91–2.11) | −0.41 (−1.19–0.36) | 0.17 (−0.55–0.88) | −0.28 (−1.44–0.87) | 0.53 (−0.47–1.54) | −0.12 (−0.92–0.68) | −0.19 (−0.92–0.54) |
| Nutrition education by physical activity | ||||||||
| Ref: without education, inactive | ||||||||
| Active | 1.01 (0.68–1.50) | 0.94 (0.55–1.61) | 0.77 (0.52–1.12) | 1.58 (1.00–2.49) * | 0.95 (0.51–1.78) | 0.74 (0.50–1.10) | 0.66 (0.37–1.18) | 0.59 (0.37–0.93) * |
| With education | ||||||||
| Inactive | 0.87 (0.66–1.14) | 0.58 (0.40–0.83) ** | 0.69 (0.53–0.90) ** | 1.05 (0.78–1.42) | 0.74 (0.49–1.12) | 0.72 (0.55–0.94) * | 0.69 (0.48–0.99) * | 0.70 (0.52–0.93) * |
| Active | 0.90 (0.65–1.26) | 0.64 (0.41–0.99) * | 0.60 (0.43–0.83) ** | 1.27 (0.87–1.83) | 0.54 (0.32–0.90) * | 0.64 (0.46–0.90) ** | 0.86 (0.55–1.34) | 0.58 (0.40–0.84) ** |
| RERI | 0.03 (−0.45–0.50) | 0.12 (−0.42–0.66) | 0.14 (−0.22–0.49) | −0.36 (−1.16–0.43) | −0.15 (−0.85–0.54) | 0.19 (−0.18–0.55) | 0.46 (0.01–0.90) * | 0.30 (−0.06–0.65) |
| AP | 0.03 (−0.50–0.56) | 0.19 (−0.67–1.05) | 0.23 (−0.37–0.82) | −0.29 (−0.93–0.36) | −0.29 (−1.57–0.99) | 0.29 (−0.28–0.86) | 0.51 (0.03–0.99) * | 0.51 (−0.11–1.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurniawan, A.-L.; Yang, Y.-L.; Chin, M.-Y.; Hsu, C.-Y.; Paramastri, R.; Lee, H.-A.; Ni, P.-Y.; Chao, J. Association of Nutrition Education and Its Interaction with Lifestyle Factors on Kidney Function Parameters and Cardiovascular Risk Factors among Chronic Kidney Disease Patients in Taiwan. Nutrients 2021, 13, 298. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020298
Kurniawan A-L, Yang Y-L, Chin M-Y, Hsu C-Y, Paramastri R, Lee H-A, Ni P-Y, Chao J. Association of Nutrition Education and Its Interaction with Lifestyle Factors on Kidney Function Parameters and Cardiovascular Risk Factors among Chronic Kidney Disease Patients in Taiwan. Nutrients. 2021; 13(2):298. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020298
Chicago/Turabian StyleKurniawan, Adi-Lukas, Ya-Lan Yang, Mei-Yun Chin, Chien-Yeh Hsu, Rathi Paramastri, Hsiu-An Lee, Po-Yuan Ni, and Jane Chao. 2021. "Association of Nutrition Education and Its Interaction with Lifestyle Factors on Kidney Function Parameters and Cardiovascular Risk Factors among Chronic Kidney Disease Patients in Taiwan" Nutrients 13, no. 2: 298. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020298