
Rationale for Timing of Follow-Up Visits to Assess Gluten-Free Diet in Celiac Disease Patients Based on Data Mining



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
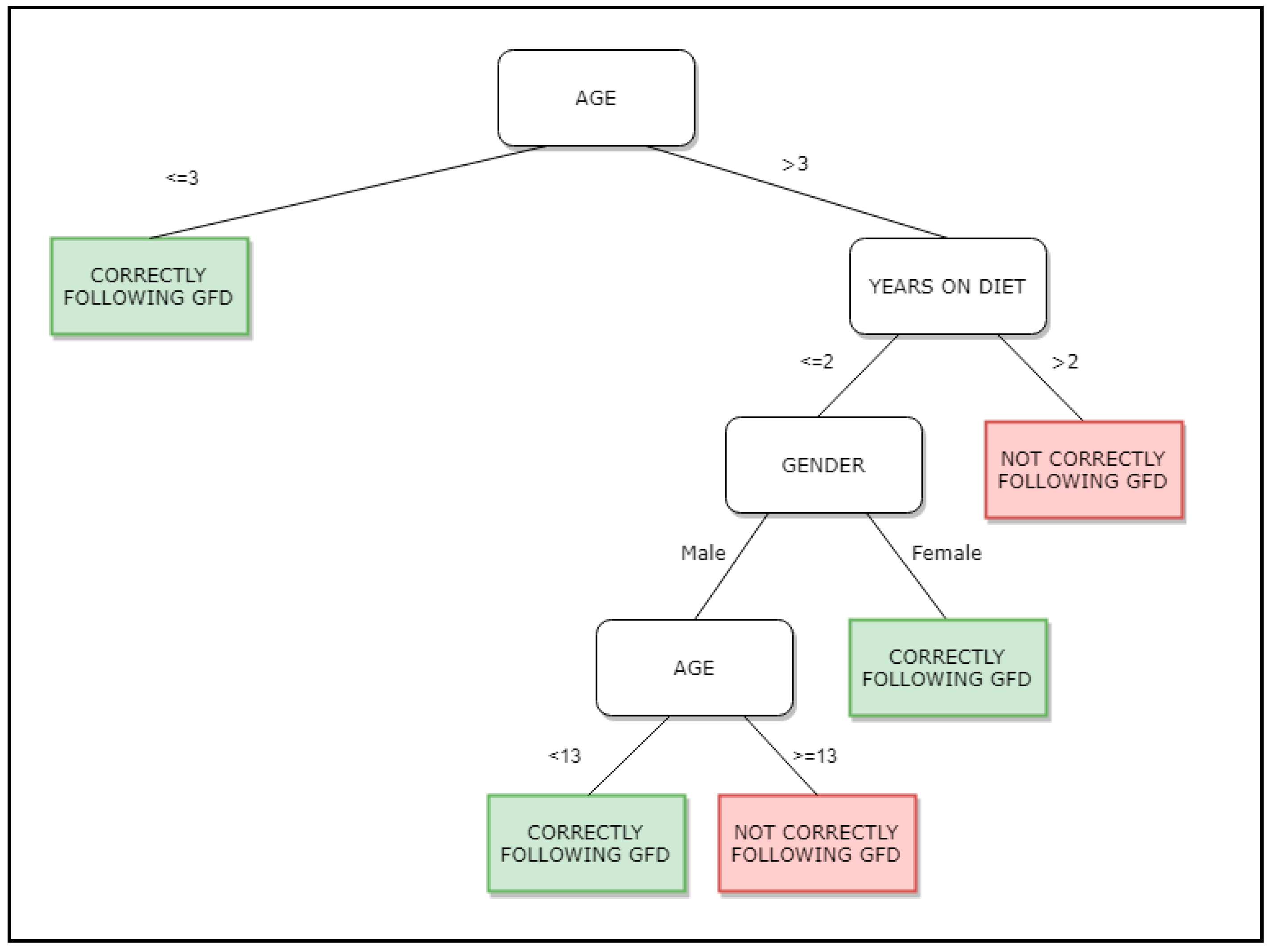
Data Mining Methods
- Case 1. All the registers in S belong to the same target label or S is not big enough. Then the tree is created with only one leaf, with the target label more frequent S.
- Case 2. In other cases, select a test base on a single variable with two or more outcomes. This test becomes the root of the tree, and one branch is created for each outcome. Then, split S into subsets S1, S2… depending to the outcome for each register, and apply the same procedure recursively to each subset.
3. Results and Discussion
Current Recommendations for Frequency of Follow-Up in CD
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Comino, I.; Fernández-Bañares, F.; Esteve, M.; Ortigosa, L.; Castillejo, G.; Fambuena, B.; Ribes-Koninckx, C.; Sierra, C.; Rodríguez-Herrera, A.; Salazar, J.C.; et al. Fecal gluten peptides reveal limitations of serological tests and food questionnaires for monitoring gluten-free diet in celiac disease patients. Am. J. Gastroenterol. 2016, 111, 1456–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catassi, C.; Gatti, S.; Fasano, A. The New Epidemiology of Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, S7–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundin, K.E.A.; Qiao, S.-W.; Snir, O.; Sollid, L.M. Coeliac disease—From genetic and immunological studies to clinical applications. Scand. J. Gastroenterol. 2015, 50, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Sollid, L.M.; Jabri, B. Triggers and drivers of autoimmunity: Lessons from coeliac disease. Nat. Rev. Immunol. 2013, 13, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Vriezinga, S.L.; Schweizer, J.J.; Koning, F.; Mearin, M.L. Coeliac disease and gluten-related disorders in childhood. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 527–536. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.R.; Hadjivassiliou, M.; Holdoway, A.; Van Heel, D.A.; et al. Diagnosis and management of adult coeliac disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef]
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffler, D.A.; Duerksen, D.R. Tests for serum transglutaminase and endomysial antibodies do not detect most patients with celiac disease and persistent villous atrophy on gluten-free diets: A meta-analysis. Gastroenterology 2017, 1533, 689–701. [Google Scholar] [CrossRef]
- de Lourdes Moreno, M.; Cebolla, Á.; Muñoz-Suano, A.; Carrillo-Carrion, C.; Comino, I.; Pizarro, Á.; Sousa, C. Detection of gluten immunogenic peptides in the urine of patients with coeliac disease reveals transgressions in the gluten-free diet and incomplete mucosal healing. Gut 2017, 662, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Morón, B.; Cebolla, Á.; Manyani, H.; Álvarez-Maqueda, M.; Megías, M.; Thomas, M.D.C.; López, M.C.; Sousa, C. Sensitive detection of cereal fractions that are toxic to celiac disease patients by using monoclonal antibodies to a main immunogenic wheat peptide. Am. J. Clin. Nutr. 2008, 87, 405–414. [Google Scholar] [CrossRef] [Green Version]
- Morón, B.; Bethune, M.T.; Comino, I.; Manyani, H.; Ferragud, M.; López, M.C.; Cebolla, Á.; Khosla, C.; Sousa, C. Toward the Assessment of Food Toxicity for Celiac Patients: Characterization of Monoclonal Antibodies to a Main Immunogenic Gluten Peptide. PLoS ONE 2008, 3, e2294. [Google Scholar] [CrossRef] [Green Version]
- Comino, I.; Real, A.; Vivas, S.; Síglez, M.Á.; Caminero, A.; Nistal, E.; Casqueiro, J.; Rodríguez-Herrera, A.; Cebolla, Á.; Sousa, C. Monitoring of gluten-free diet compliance in celiac patients by assessment of gliadin 33-mer equivalent epitopes in feces. Am. J. Clin. Nutr. 2012, 95, 670–677. [Google Scholar] [CrossRef] [Green Version]
- A Silvester, J.; Rashid, M. Long-term Follow-Up of Individuals with Celiac Disease: An Evaluation of Current Practice Guidelines. Can. J. Gastroenterol. 2007, 21, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Javorsky, E.; Robinson, A.; Kimball, A.B. Evidence-based guidelines to determine follow-up intervals: A call for action. Am. J. Manag. Care 2014, 201, 17. [Google Scholar]
- Han, J.; Pei, J.; Kamber, M. Data Mining: Concepts and Techniques; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Iavindrasana, J.; Cohen, G.; Depeursinge, A.; Müller, H.; Meyer, R.; Geissbuhler, A. Clinical data mining: A review. Yearb. Med. Inform. 2009, 1801, 121–133. [Google Scholar]
- Syage, J.A.; Murray, J.A.; Green, P.H.; Khosla, C.; Adelman, D.C.; Sealey-Voyksner, J.A. Oral Latiglutenase Improves Chronic Symptoms in Seropositive Celiac Disease Patients. Gastroenterology 2017, 152, S163. [Google Scholar] [CrossRef]
- Kaw, C.; Hefle, S.; Taylor, S.L. Sandwich Enzyme-Linked Immunosorbent Assay (ELISA) for the Detection of Lupine Residues in Foods. J. Food Sci. 2008, 73, T135–T140. [Google Scholar] [CrossRef]
- Fayyad, U.; Piatetsky-Shapiro, G.; Smyth, P. From data mining to knowledge discovery in databases. AI Mag. 1996, 173, 37. [Google Scholar]
- Phyu, T.N. Survey of classification techniques in data mining. In Proceedings of the International MultiConference of Engineers and Computer Scientists, Hong Kong, China, 18–20 March 2009; pp. 18–20. [Google Scholar]
- Goebel, M.; Gruenwald, L. A survey of data mining and knowledge discovery software tools. ACM SIGKDD Explor. Newsl. 1999, 11, 20–33. [Google Scholar] [CrossRef]
- Wu, X.; Kumar, V.; Quinlan, J.R.; Ghosh, J.; Yang, Q.; Motoda, H.; Hou, Z.H. Top 10 algorithms in data mining. Knowl. Inf. Syst. 2008, 141, 1–37. [Google Scholar] [CrossRef] [Green Version]
- Quinlan, J.R. Bagging, boosting, and C4. 5. AAAI Conf. Artif. Intell. 1996, 1, 725–730. [Google Scholar]
- Quinlan, J.R. Induction of decision trees. Mach. Learn. 1986, 11, 81–106. [Google Scholar] [CrossRef] [Green Version]
- Friedl, M.; Brodley, C. Decision tree classification of land cover from remotely sensed data. Remote Sens. Environ. 1997, 61, 399–409. [Google Scholar] [CrossRef]
- Play Tennis. Simple Dataset with Decisions about Playing Tennis. Available online: https://www.kaggle.com/fredericobreno/play-tennis (accessed on 16 January 2021).
- Muniyandi, A.P.; Rajeswari, R.; Rajaram, R.K. Network Anomaly Detection by Cascading K-Means Clustering and C4.5 Decision Tree algorithm. Procedia Eng. 2012, 30, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Asencio–Cortés, G.; Morales–Esteban, A.; Shang, X.; Martínez–Álvarez, F. Earthquake prediction in California using regression algorithms and cloud-based big data infrastructure. Comput. Geosci. 2018, 115, 198–210. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef]
- Hill, I.D.; Dirks, M.H.; Liptak, G.S.; Colletti, R.B.; Fasano, A.; Guandalini, S.; Seidman, E.G. Guideline for the diagnosis and treatment of celiac disease in children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatric Gastroenterol. Nutr. 2005, 40, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; E A Lundin, K. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence. Coeliac Disease: Recognition, Assessment and Management. Available online: https://www.guidelines.co.uk/gastrointestinal/nice-coeliac-disease-guideline/252667.article 2015 (accessed on 16 January 2021).
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. American College of Gastroenterology clinical guideline: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 1085, 656. [Google Scholar] [CrossRef] [Green Version]
- SPAIN Ministry of Health. Working Group of the Protocol for the Early Diagnosis of Celiac Disease. Protocol for the Early Diagnosis of Celiac Disease. Ministry of Health, Social Services and Equality. Canary Islands Health Service Evaluation Service SESCS. Available online: https://www.mscbs.gob.es/profesionales/prestacionesSanitarias/publicaciones/Celiaquia/enfermedadCeliaca.pdf (accessed on 20 August 2019).
- Cervino, G.; Fiorillo, L.; Laino, L.; Herford, A.S.; Lauritano, F.; Giudice, G.L.; Famà, F.; Santoro, R.; Troiano, G.; Iannello, G.; et al. Oral health impact profile in celiac patients: Analysis of recent findings in a literature review. Gastroenterol. Res. Pract. 2018, 7848735. [Google Scholar] [CrossRef]
- Norris, S.L.; Lau, J.; Smith, S.J.; Schmid, C.H.; Engelgau, M.M. Self-management education for adults with type 2 diabetes: A meta-analysis of the effect on glycemic control. Diabetes Care 2002, 257, 1159–1171. [Google Scholar] [CrossRef] [Green Version]
- Hall, A.M.; Ferreira, P.H.; Maher, C.G.; Latimer, J.; Ferreira, M.L. The influence of the therapist-patient relationship on treatment outcome in physical rehabilitation: A systematic review. J. Phys. Ther. 2010, 908, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.; Newman, J.M. Celiac diet: Its impact on quality of life. J. Am. Diet. Assoc. 2003, 103, 1533–1535. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Herrera, A.; Reyes-Andrade, J.; Rubio-Escudero, C. Rationale for Timing of Follow-Up Visits to Assess Gluten-Free Diet in Celiac Disease Patients Based on Data Mining. Nutrients 2021, 13, 357. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020357
Rodríguez-Herrera A, Reyes-Andrade J, Rubio-Escudero C. Rationale for Timing of Follow-Up Visits to Assess Gluten-Free Diet in Celiac Disease Patients Based on Data Mining. Nutrients. 2021; 13(2):357. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020357
Chicago/Turabian StyleRodríguez-Herrera, Alfonso, Joaquín Reyes-Andrade, and Cristina Rubio-Escudero. 2021. "Rationale for Timing of Follow-Up Visits to Assess Gluten-Free Diet in Celiac Disease Patients Based on Data Mining" Nutrients 13, no. 2: 357. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020357