
Is Probiotic Supplementation Useful for the Management of Body Weight and Other Anthropometric Measures in Adults Affected by Overweight and Obesity with Metabolic Related Diseases? A Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Eligibility
2.3. Data analysis and Presentation of Results
3. Results
3.1. Overweight and Obesity
3.2. Type 2 Diabetes Mellitus
3.3. NASH
3.4. Metabolic Syndrome
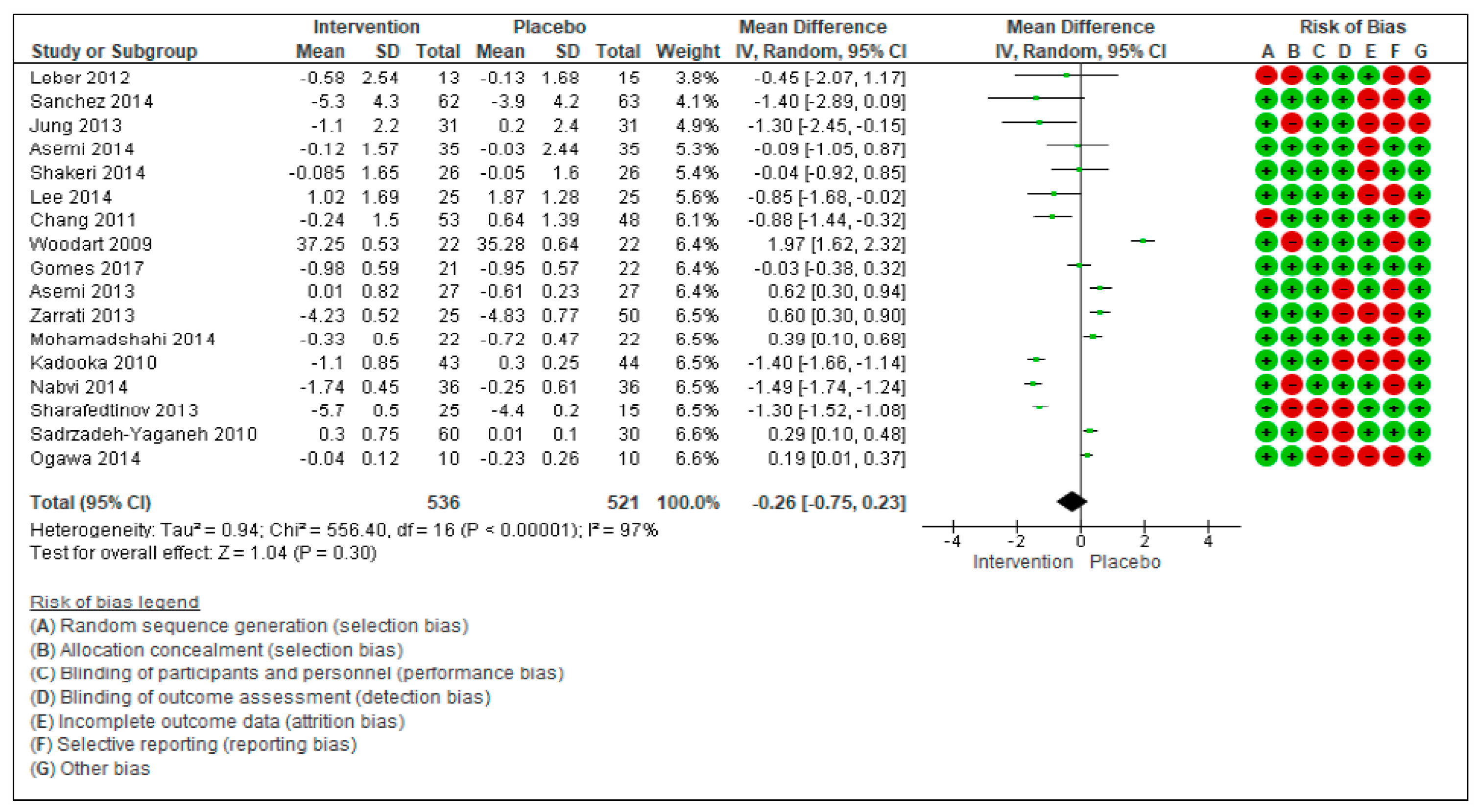
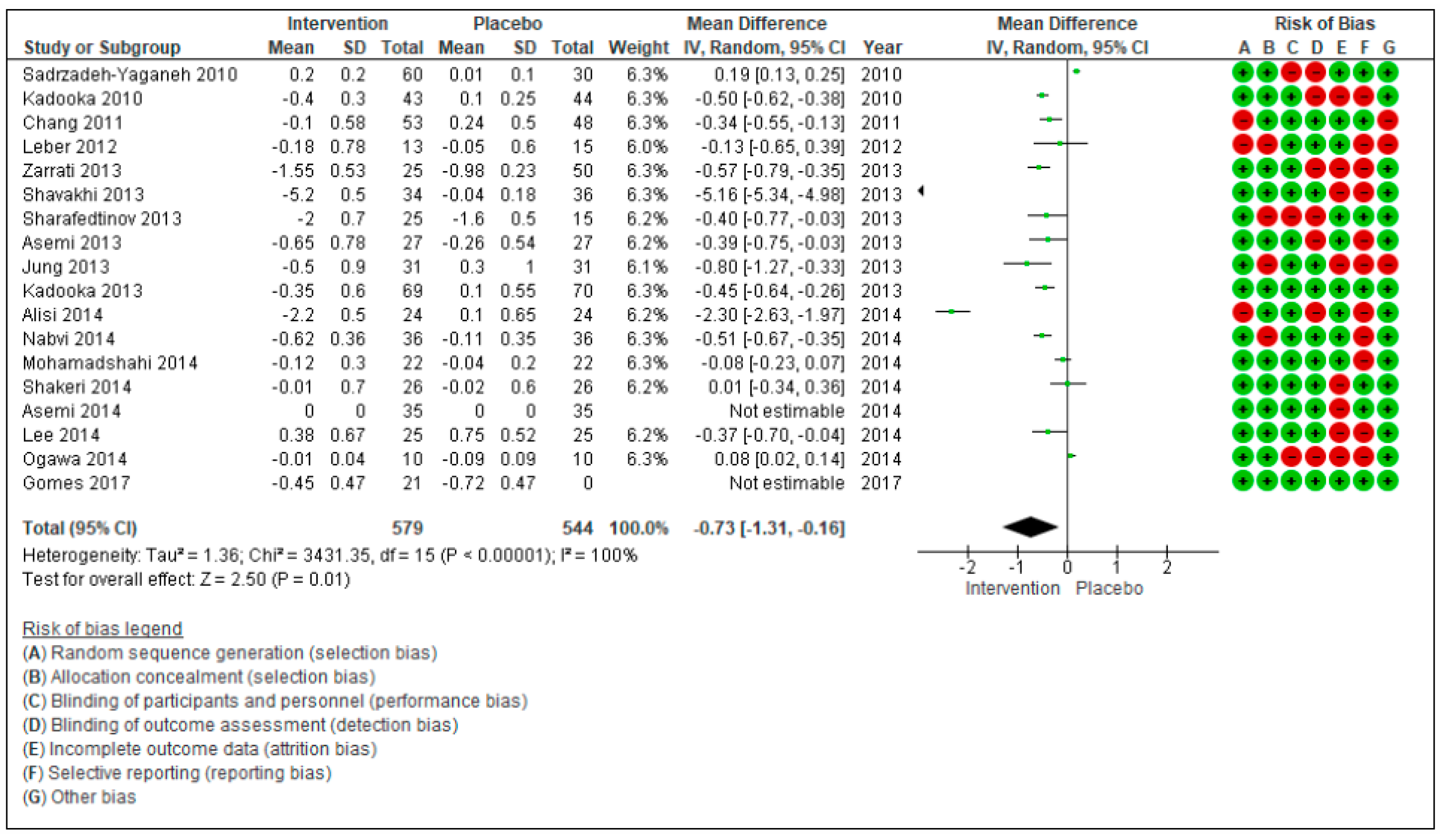
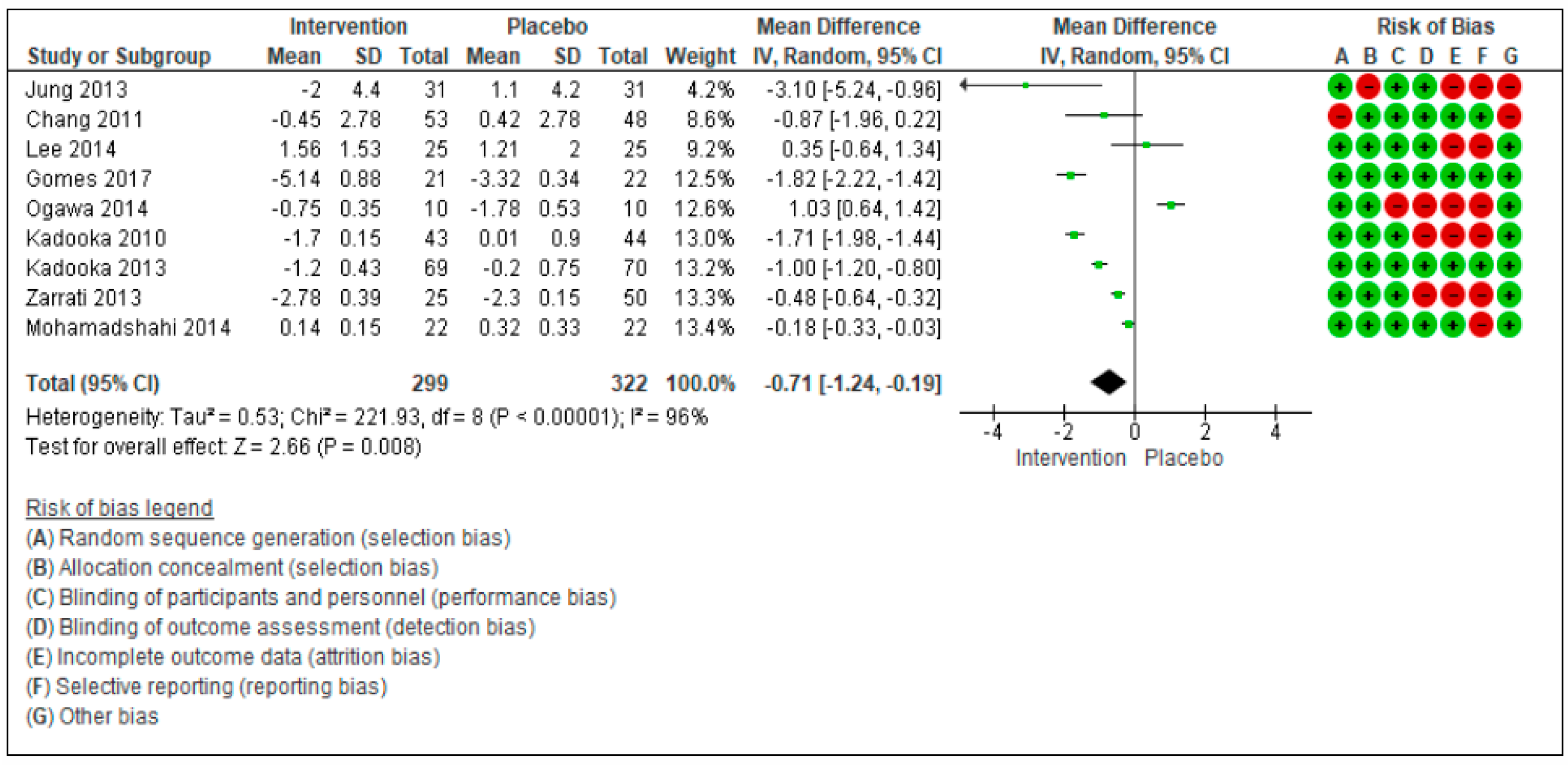
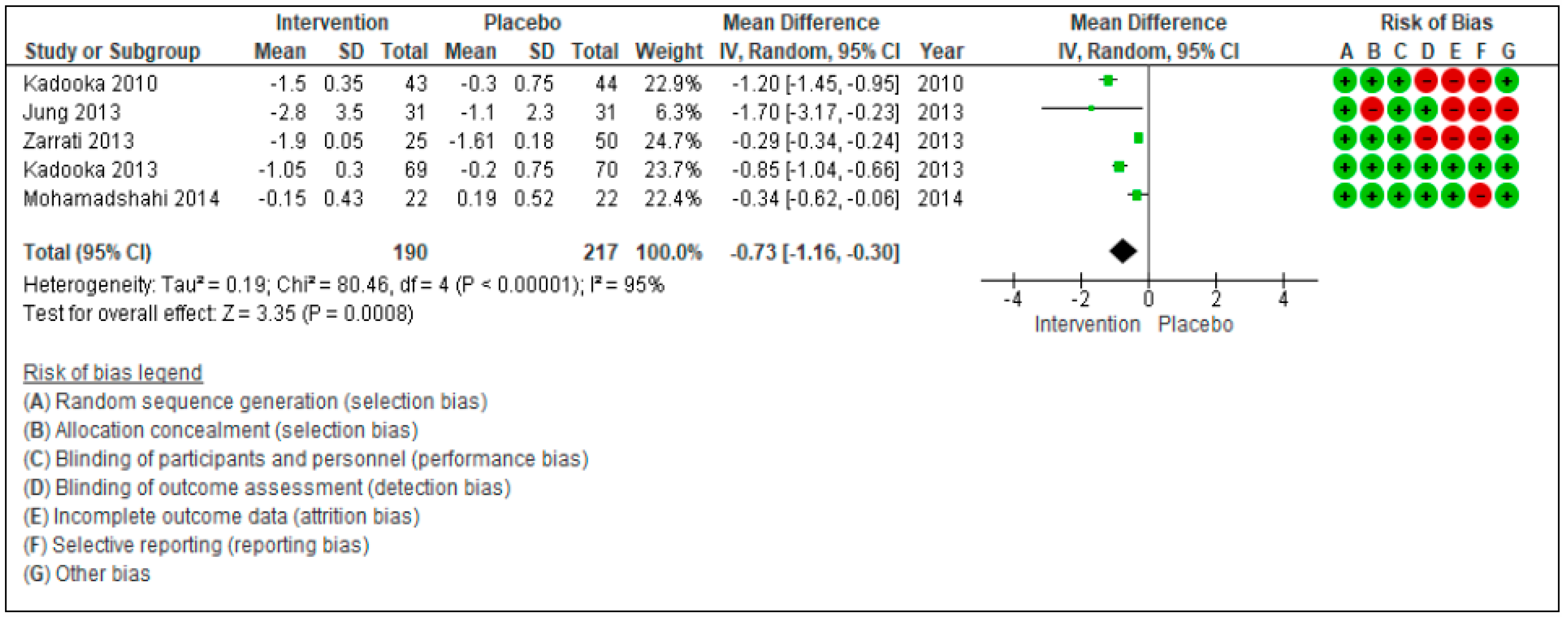
3.5. Meta-Analyzed Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baothman, O.A.; Zamzami, M.A.; Taher, I.; Abubaker, J.; Abu-Farha, M. The Role of Gut Microbiota in the Development of Obesity and Diabetes. Lipids Health Dis. 2016, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.W.; Ince, J.; Duncan, S.H.; Webster, L.M.; Holtrop, G.; Ze, X.; Brown, D.; Stares, M.D.; Scott, P.; Bergerat, A.; et al. Dominant and Diet-Responsive Groups of Bacteria within the Human Colonic Microbiota. ISME J. 2011, 5, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Jumpertz, R.; Le, D.S.; Turnbaugh, P.J.; Trinidad, C.; Bogardus, C.; Gordon, J.I.; Krakoff, J. Energy-Balance Studies Reveal Associations between Gut Microbes, Caloric Load, and Nutrient Absorption in Humans. Am. J. Clin. Nutr. 2011, 94, 58–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, E.F.; Cotter, P.D.; Healy, S.; Marques, T.M.; O’Sullivan, O.; Fouhy, F.; Clarke, S.F.; O’Toole, P.W.; Quigley, E.M.; Stanton, C.; et al. Composition and Energy Harvesting Capacity of the Gut Microbiota: Relationship to Diet, Obesity and Time in Mouse Models. Gut 2010, 59, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An Obesity-Associated Gut Microbiome with Increased Capacity for Energy Harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Tagliabue, A.; Elli, M. The Role of Gut Microbiota in Human Obesity: Recent Findings and Future Perspectives. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.; Su, W.; Rahat-Rozenbloom, S.; Wolever, T.M.S.; Comelli, E.M. Adiposity, Gut Microbiota and Faecal Short Chain Fatty Acids Are Linked in Adult Humans. Nutr. Diabetes 2014, 4, e121. [Google Scholar] [CrossRef] [PubMed]
- Schwiertz, A.; Taras, D.; Schäfer, K.; Beijer, S.; Bos, N.A.; Donus, C.; Hardt, P.D. Microbiota and SCFA in Lean and Overweight Healthy Subjects. Obesity 2010, 18, 190–195. [Google Scholar] [CrossRef]
- Sanmiguel, C.; Gupta, A.; Mayer, E.A. Gut Microbiome and Obesity: A Plausible Explanation for Obesity. Curr. Obes. Rep. 2015, 4, 250–261. [Google Scholar] [CrossRef] [Green Version]
- Turnbaugh, P.J.; Hamady, M.; Yatsunenko, T.; Cantarel, B.L.; Duncan, A.; Ley, R.E.; Sogin, M.L.; Jones, W.J.; Roe, B.A.; Affourtit, J.P.; et al. A Core Gut Microbiome in Obese and Lean Twins. Nature 2009, 457, 480–484. [Google Scholar] [CrossRef] [Green Version]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.M.; Kennedy, S.; et al. Richness of Human Gut Microbiome Correlates with Metabolic Markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Kasai, C.; Sugimoto, K.; Moritani, I.; Tanaka, J.; Oya, Y.; Inoue, H.; Tameda, M.; Shiraki, K.; Ito, M.; Takei, Y.; et al. Comparison of the Gut Microbiota Composition between Obese and Non-Obese Individuals in a Japanese Population, as Analyzed by Terminal Restriction Fragment Length Polymorphism and next-Generation Sequencing. BMC Gastroenterol. 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Walters, W.A.; Xu, Z.; Knight, R. Meta-Analyses of Human Gut Microbes Associated with Obesity and IBD. FEBS Lett. 2014, 588, 4223–4233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Microbial Ecology: Human Gut Microbes Associated with Obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef]
- Duncan, S.H.; Lobley, G.E.; Holtrop, G.; Ince, J.; Johnstone, A.M.; Louis, P.; Flint, H.J. Human Colonic Microbiota Associated with Diet, Obesity and Weight Loss. Int. J. Obes. 2008, 32, 1720–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furet, J.-P.; Kong, L.-C.; Tap, J.; Poitou, C.; Basdevant, A.; Bouillot, J.-L.; Mariat, D.; Corthier, G.; Doré, J.; Henegar, C.; et al. Differential Adaptation of Human Gut Microbiota to Bariatric Surgery-Induced Weight Loss: Links with Metabolic and Low-Grade Inflammation Markers. Diabetes 2010, 59, 3049–3057. [Google Scholar] [CrossRef] [Green Version]
- Angelakis, E.; Armougom, F.; Carrière, F.; Bachar, D.; Laugier, R.; Lagier, J.C.; Robert, C.; Michelle, C.; Henrissat, B.; Raoult, D. A Metagenomic Investigation of the Duodenal Microbiota Reveals Links with Obesity. PLoS ONE 2015, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Million, M.; Angelakis, E.; Maraninchi, M.; Henry, M.; Giorgi, R.; Valero, R.; Vialettes, B.; Raoult, D. Correlation between Body Mass Index and Gut Concentrations of Lactobacillus Reuteri, Bifidobacterium Animalis, Methanobrevibacter Smithii and Escherichia Coli. Int. J. Obes. 2013, 37, 1460–1466. [Google Scholar] [CrossRef] [Green Version]
- Million, M.; Maraninchi, M.; Henry, M.; Armougom, F.; Richet, H.; Carrieri, P.; Valero, R.; Raccah, D.; Vialettes, B.; Raoult, D. Obesity-Associated Gut Microbiota Is Enriched in Lactobacillus Reuteri and Depleted in Bifidobacterium Animalis and Methanobrevibacter Smithii. Int. J. Obes. 2012, 36, 817–825. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria. Fao Who 2001, 1–34. [Google Scholar] [CrossRef]
- Gérard, P. Gut Microbiota and Obesity. Cell. Mol. Life Sci. 2016, 73, 147–162. [Google Scholar] [CrossRef]
- Million, M.; Angelakis, E.; Paul, M.; Armougom, F.; Leibovici, L.; Raoult, D. Comparative Meta-Analysis of the Effect of Lactobacillus Species on Weight Gain in Humans and Animals. Microb. Pathog. 2012, 53, 100–108. [Google Scholar] [CrossRef]
- Aoun, A.; Darwish, F.; Hamod, N. The Influence of the Gut Microbiome on Obesity in Adults and the Role of Probiotics, Prebiotics, and Synbiotics for Weight Loss. Preventive Nutrition Food Sci. 2020, 25, 113–123. [Google Scholar] [CrossRef]
- Ballini, A.; Scacco, S.; Boccellino, M.; Santacroce, L.; Arrigoni, R. Microbiota and Obesity: Where Are We Now? Biology 2020, 9, 415. [Google Scholar] [CrossRef]
- Home-PubMed-NCBI. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed (accessed on 27 September 2018).
- Scopus Preview-Scopus-Welcome to Scopus. Available online: https://0-www-scopus-com.brum.beds.ac.uk/home.uri (accessed on 27 September 2018).
- Kadooka, Y.; Sato, M.; Imaizumi, K.; Ogawa, A.; Ikuyama, K.; Akai, Y.; Okano, M.; Kagoshima, M.; Tsuchida, T. Regulation of Abdominal Adiposity by Probiotics (Lactobacillus Gasseri SBT2055) in Adults with Obese Tendencies in a Randomized Controlled Trial. Eur. J. Clin. Nutr. 2010, 64, 636–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadooka, Y.; Sato, M.; Ogawa, A.; Miyoshi, M.; Uenishi, H.; Ogawa, H.; Ikuyama, K.; Kagoshima, M.; Tsuchida, T. Effect of Lactobacillus Gasseri SBT2055 in Fermented Milk on Abdominal Adiposity in Adults in a Randomised Controlled Trial. Br. J. Nutr. 2013, 110, 1696–1703. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, A.; Kadooka, Y.; Kato, K.; Shirouchi, B.; Sato, M. Lactobacillus Gasseri SBT2055 Reduces Postprandial and Fasting Serum Non-Esterified Fatty Acid Levels in Japanese Hypertriacylglycerolemic Subjects. Lipids Health Dis. 2014, 13, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.-P.; Lee, K.-M.; Kang, J.-H.; Yun, S.-I.; Park, H.-O.; Moon, Y.; Kim, J.-Y. Effect of Lactobacillus Gasseri BNR17 on Overweight and Obese Adults: A Randomized, Double-Blind Clinical Trial. Korean J. Fam. Med. 2013, 34, 80–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.J.; Bose, S.; Seo, J.G.; Chung, W.S.; Lim, C.Y.; Kim, H. The Effects of Co-Administration of Probiotics with Herbal Medicine on Obesity, Metabolic Endotoxemia and Dysbiosis: A Randomized Double-Blind Controlled Clinical Trial. Clin. Nutr. 2014, 33, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.; Darimont, C.; Drapeau, V.; Emady-Azar, S.; Lepage, M.; Rezzonico, E.; Ngom-Bru, C.; Berger, B.; Philippe, L.; Ammon-Zuffrey, C.; et al. Effect of Lactobacillus Rhamnosus CGMCC1.3724 Supplementation on Weight Loss and Maintenance in Obese Men and Women. Br. J. Nutr. 2014, 111, 1507–1519. [Google Scholar] [CrossRef] [Green Version]
- Zarrati, M.; Shidfar, F.; Nourijelyani, K.; Mofid, V.; Hossein zadeh-Attar, M.J.; Bidad, K.; Najafi, F.; Gheflati, Z.; Chamari, M.; Salehi, E. Lactobacillus Acidophilus La5, Bifidobacterium BB12, and Lactobacillus Casei DN001 Modulate Gene Expression of Subset Specific Transcription Factors and Cytokines in Peripheral Blood Mononuclear Cells of Obese and Overweight People. BioFactors 2013, 39, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.C.; de Sousa, R.G.M.; Botelho, P.B.; Gomes, T.L.N.; Prada, P.O.; Mota, J.F. The Additional Effects of a Probiotic Mix on Abdominal Adiposity and Antioxidant Status: A Double-Blind, Randomized Trial. Obesity 2017, 25, 30–38. [Google Scholar] [CrossRef]
- Woodard, G.A.; Encarnacion, B.; Downey, J.R.; Peraza, J.; Chong, K.; Hernandez-Boussard, T.; Morton, J.M. Probiotics Improve Outcomes after Roux-En-Y Gastric Bypass Surgery: A Prospective Randomized Trial. J. Gastrointest. Surg. 2009, 13, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Khorrami-Rad, A.; Alizadeh, S.A.; Shakeri, H.; Esmaillzadeh, A. Effects of Synbiotic Food Consumption on Metabolic Status of Diabetic Patients: A Double-Blind Randomized Cross-over Controlled Clinical Trial. Clin. Nutr. 2014, 33, 198–203. [Google Scholar] [CrossRef]
- Shakeri, H.; Hadaegh, H.; Abedi, F.; Tajabadi-Ebrahimi, M.; Mazroii, N.; Ghandi, Y.; Asemi, Z. Consumption of Synbiotic Bread Decreases Triacylglycerol and VLDL Levels While Increasing HDL Levels in Serum from Patients with Type-2 Diabetes. Lipids 2014, 49, 695–701. [Google Scholar] [CrossRef]
- Mohammadi-Sartang, M.; Bellissimo, N.; Totosy de Zepetnek, J.O.; Brett, N.R.; Mazloomi, S.M.; Fararouie, M.; Bedeltavana, A.; Famouri, M.; Mazloom, Z. The Effect of Daily Fortified Yogurt Consumption on Weight Loss in Adults with Metabolic Syndrome: A 10-Week Randomized Controlled Trial. Nutr. Metab. Cardiovasc. Dis. NMCD 2018, 28, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Zohreh, Z.; Shakeri, H.; Sabihi, S.; Esmaillzadeh, A. Effect of Multispecies Probiotic Supplements on Metabolic Profile, Hs-CRP, and Oxidative Stress in Patients with Type 2 Diabetes. Ann. Nutr. Metab. 2013, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kassaian, N.; Aminorroaya, A.; Feizi, A.; Jafari, P.; Amini, M. The Effects of Probiotic and Synbiotic Supplementation on Metabolic Syndrome Indices in Adults at Risk of Type 2 Diabetes: Study Protocol for a Randomized Controlled Trial. Trials 2017, 18, 148. [Google Scholar] [CrossRef] [Green Version]
- Palacios, T.; Vitetta, L.; Coulson, S.; Madigan, C.D.; Denyer, G.S.; Caterson, I.D. The Effect of a Novel Probiotic on Metabolic Biomarkers in Adults with Prediabetes and Recently Diagnosed Type 2 Diabetes Mellitus: Study Protocol for a Randomized Controlled Trial. Trials 2017, 18, 7. [Google Scholar] [CrossRef] [Green Version]
- Shavakhi, A.; Minakari, M.; Firouzian, H.; Assali, R.; Hekmatdoost, A.; Ferns, G. Effect of a Probiotic and Metformin on Liver Aminotransferases in Non-Alcoholic Steatohepatitis: A Double Blind Randomized Clinical Trial. Int. J. Prev. Med. 2013, 4, 531–537. [Google Scholar]
- Alisi, A.; Bedogni, G.; Baviera, G.; Giorgio, V.; Porro, E.; Paris, C.; Giammaria, P.; Reali, L.; Anania, F.; Nobili, V. Randomised Clinical Trial: The Beneficial Effects of VSL#3 in Obese Children with Non-Alcoholic Steatohepatitis. Aliment. Pharmacol. Ther. 2014, 39, 1276–1285. [Google Scholar] [CrossRef] [PubMed]
- Nabavi, S.; Rafraf, M.; Somi, M.H.; Homayouni-Rad, A.; Asghari-Jafarabadi, M. Effects of Probiotic Yogurt Consumption on Metabolic Factors in Individuals with Nonalcoholic Fatty Liver Disease. J. Dairy Sci. 2014, 97, 7386–7393. [Google Scholar] [CrossRef] [PubMed]
- Sadrzadeh-Yeganeh, H.; Elmadfa, I.; Djazayery, A.; Jalali, M.; Heshmat, R.; Chamary, M. The Effects of Probiotic and Conventional Yoghurt on Lipid Profile in Women. Br. J. Nutr. 2010, 103, 1778–1783. [Google Scholar] [CrossRef]
- Chang, B.J.; Park, S.U.; Jang, Y.S.; Ko, S.H.; Joo, N.M.; Kim, S.I.; Kim, C.H.; Chang, D.K. Effect of Functional Yogurt NY-YP901 in Improving the Trait of Metabolic Syndrome. Eur. J. Clin. Nutr. 2011, 65, 1250–1255. [Google Scholar] [CrossRef] [Green Version]
- Leber, B.; Tripolt, N.J.; Blattl, D.; Eder, M.; Wascher, T.C.; Pieber, T.R.; Stauber, R.; Sourij, H.; Oettl, K.; Stadlbauer, V. The Influence of Probiotic Supplementation on Gut Permeability in Patients with Metabolic Syndrome: An Open Label, Randomized Pilot Study. Eur. J. Clin. Nutr. 2012, 66, 1110–1115. [Google Scholar] [CrossRef] [Green Version]
- Sharafedtinov, K.K.; Plotnikova, O.A.; Alexeeva, R.I.; Sentsova, T.B.; Songisepp, E.; Stsepetova, J.; Smidt, I.; Mikelsaar, M. Hypocaloric Diet Supplemented with Probiotic Cheese Improves Body Mass Index and Blood Pressure Indices of Obese Hypertensive Patients—A Randomized Double-Blind Placebo-Controlled Pilot Study. Nutr. J. 2013, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Abenavoli, L.; Scarpellini, E.; Colica, C.; Boccuto, L.; Salehi, B.; Sharifi-Rad, J.; Aiello, V.; Romano, B.; De Lorenzo, A.; Izzo, A.A.; et al. Gut Microbiota and Obesity: A Role for Probiotics. Nutrients 2019, 11, 2690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef]
- Wiciński, M.; Gębalski, J.; Gołębiewski, J.; Malinowski, B. Probiotics for the Treatment of Overweight and Obesity in Humans—A Review of Clinical Trials. Microorganisms 2020, 8, 1148. [Google Scholar] [CrossRef]
- Mazloom, K.; Siddiqi, I.; Covasa, M. Probiotics: How Effective Are They in the Fight against Obesity? Nutrients 2019, 11, 258. [Google Scholar] [CrossRef] [Green Version]
- Daniali, M.; Nikfar, S.; Abdollahi, M. A Brief Overview on the Use of Probiotics to Treat Overweight and Obese Patients. Expert Rev. Endocrinol. Metab. 2020, 15, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronsson, L.; Huang, Y.; Parini, P.; Korach-André, M.; Håkansson, J.; Gustafsson, J.-Å.; Pettersson, S.; Arulampalam, V.; Rafter, J. Decreased Fat Storage by Lactobacillus Paracasei Is Associated with Increased Levels of Angiopoietin-Like 4 Protein (ANGPTL4). PLoS ONE 2010, 5, e13087. [Google Scholar] [CrossRef]
- Ogawa, A.; Kobayashi, T.; Sakai, F.; Kadooka, Y.; Kawasaki, Y. Lactobacillus Gasseri SBT2055 Suppresses Fatty Acid Release through Enlargement of Fat Emulsion Size in Vitro and Promotes Fecal Fat Excretion in Healthy Japanese Subjects. Lipids Health Dis. 2015, 14, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarmozzino, F.; Poli, A.; Visioli, F. Microbiota and cardiovascular disease risk: A scoping review. Pharmacol. Res. 2020, 159. [Google Scholar] [CrossRef] [PubMed]
- Lescheid, D.W. Probiotics as Regulators of Inflammation: A Review. Funct. Foods Health Dis. 2014, 4, 299. [Google Scholar] [CrossRef]
- Peng, L.; Li, Z.R.; Green, R.S.; Holzman, I.R.; Lin, J. Butyrate enhances the intestinal barrier by facilitating tight junction assembly via activation of AMP-activated protein kinase in Caco-2 cell monolayers. J. Nutr. 2009, 139, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wu, Y.; Fei, X. Effect of Probiotics on Body Weight and Body-Mass Index: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. Int. J. Food Sci. Nutr. 2016, 67, 571–580. [Google Scholar] [CrossRef]
- Abbasi, J. Are Probiotics Money Down the Toilet? or Worse? JAMA J. Am. Med. Assoc. 2019, 321, 633–635. [Google Scholar] [CrossRef]
- Daniel, H. Diet and the gut microbiome: From hype to hypothesis. Br. J. Nutr. 2020, 124, 521–530. [Google Scholar] [CrossRef] [Green Version]
- Hiergeist, A.; Reischl, U.; Gessner, A.; Garzetti, D.; Stecher, B.; Gálvez, E.J.C.; Strowig, T.; Yang, I.; Suerbaum, S.; Fischer, N.; et al. Multicenter quality assessment of 16S ribosomal DNA-sequencing for microbiome analyses reveals high inter-center variability. Int. J. Med. Microbiol. 2016, 306, 334–342. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Study Design | Participants (Age) | Intervention Group(s) | Placebo Group(s) | Duration | Changes in Intervention Group(s) a | Changes in Control Group(s) a |
|---|---|---|---|---|---|---|---|
| Gomes, 2017 | Randomized controlled trial (RCT) | 43 (20–59 years) | n = 21 Diet and 4 sachets/day: 1 × 109 CFU of Lactobacillus acidophilus LA-14, L. casei LC-11, L. lactis LL-23, Bifidobacterium bifidum BB-06, and B. lactis BL-4 | n = 22 diet | 8 weeks | BW (kg): −0.98 BMI (kg/m2): −0.45 WC (cm): −5.14 | BW (kg): −0.95 BMI (kg/m2): −0.72 WC: (cm) −3.32 |
| Lee, 2014 | RCT | 50 (19–65 years) | n = 25 Twice/day Bofutsushosan, containing 18 components, 3 g per admnistration and priobiotic capsules (Duolac 7 included 5 billion viable of Streptococcus thermophiles, L. Plantarum, L. acidophilus, L. rhamnosus, B. Lactis, B. longum, and B. breve | n = 25 Twice/dayBTS (3 g per admnistration) and placebo capsules | 8 weeks | BW (kg): 1.02 ± 1.69 BMI (kg/m2): 0.38 ± 0.67 WC (cm): 1.56 ± 1.53 | BW (kg): 1.87 ± 1.28 BMI: 0.75 ± 0.52 WC (cm): 1.21 ± 2.00 |
| Sanchez, 2014 | RCT | 125 (18–55 years) | n = 62 two capsules daily (6 × 108cfu of L. rhamnosus CGMCC1.3724 (LPR)) | n = 63 Two capsules daily | 24 weeks | BW (kg): −5.3 ± 4.3 | BW (kg): −3.9 ± 4.2 |
| Zarrati, 2013 | RCT | 75 (20–50 years) | Group 1, -, n = 25: diet and 200 g/day of probiotic yogurt (PLCD), containing S. thermophiles and L. bulgaricus - enriched with the L. acidophilus LA5, L. casei DN001 and, B. lactis Bb12 (1 × 108 cfu/g each strain) | Group 2, n = 25: diet and 200 g/die of regular yogurt (RLCD)- Group 3, n = 25: 200 g/day of probiotic yogurt without any diet (PWLCD) | 8 weeks | PLCD: BW (kg): −4.23 BMI (kg/m2): −1.3 WC (cm): −2.78 HC (cm): −2 | RLCD: BW (kg): −4.87 BMI (kg/m2): −1.9 WC (cm): −2.3 HC (cm): −3.18 PWLCD: BW (kg): −0.04 HC (cm): −0.03 |
| Jung, 2013 | RCT | 62 (19–60 years) | n = 31 6 capsules/day composed of 1010 cfu of L. gasseri BNR17 | n = 31 6 placebo capsules/day | 12 weeks | BW (kg): (−1.1 ± 2.2) BMI (kg/m2): (−0.5 ± 0.9) WC (cm): (−2 ± 4.4) HC (cm): (−2.8 ± 3.5) | BW (cm): (0.2 ± 2.4) BMI (kg/m2): (0.3 ± 1.0) WC (cm): (1.1 ± 4.2) HC (cm): (−1.1 ± 2.3) |
| Sharafedtinov, 2013 | RCT | 40 (30–69 years) | n = 25 50 g/day of probiotic product (semi-hard cheese) containing L. plantarum TENSIA, added in amounts of 1.5 × 1011 | n = 15 50 g/day of cheese without probiotics | 3 weeks | BW (kg): −5.7 BMI (kg/m2): −2 | BW (kg): −4.4 BMI (kg/m2): −2.3 |
| Kadooka, 2013 | RCT | 210 (35–60 years) | n = 69 Fermented milk (FM) containing 107 cfu LG2055/g n = 71 FM containing 106 cfu LG2055/g | n = 70 Control FM containing 0 cfu LG2055/g | 12 weeks | 107 dose BMI (kg/m2): (−0.3) WC (cm): (−1.3) HC (cm): (−1.2) 106 dose BMI (kg/m2): (−0.4) WC (cm): (−1.1) HC (cm): (−0.9) | BMI (kg/m2): (0.1) WC (cm): (−0.1) HC (cm): (−0.2) |
| Kadooka, 2010 | RCT | 87 (33–63 years) | n = 43 200 g daily of FM with L. gasseri SBT2055 (LG2055), 5 × 1010 cfu/100 g of FM | n = 44 200 g (2 portions of 100 g each) daily of FM without LG2055 | 12 weeks | BW (kg): −1.1 BMI (kg/m2): −0.4 WC (cm): −1.7 HC (cm): −1.5 | BW (kg): 0.3 BMI (kg/m2): 0.1 HC (kg): −0.3 |
| Woodard, 2009 | RCT | 44 (median age of treated group was 48.6 years, of placebo group was 41.2) | n = 22 1 pill/day of Puritan’s Pride®, probiotic supplement containing 2.4 billion live cells of Lactobacillus species. | n = 22 placebo | 24 weeks | Weight loss % (6 weeks postoperative): 29.90 | Weight loss % (6 weeks postoperative):25.50 |
| Asemi, 2014 | RCT | 70 (35–70 years) | n = 35 3 times/day of synbiotic food with L sporogenes (1 × 107 cfu) and 0.04 inulin as prebiotic. Then they received 27 × 107 cfu L. sporogenes and 1.08 g of inulin each day | n = 35 Control food: the same substance without probiotic bacteria and prebiotic inulin | 6 weeks | BW (kg): (−0.12 ± 1.57) BMI (kg/m2): (−0.05 ± 0.62) | BW (kg): (−0.03 ± 2.44) BMI (kg/m2): (−0.02 ± 1) |
| Asemi, 2013 | RCT | 54 (35–70 years) | n = 27 The probiotic supplement has L. acidophilus (2 × 109 cfu), L. casei (7 × 109 cfu), L.rhamnosus (1.5 × 109 cfu), L.bulgaricus (2 × 108 cfu), B. breve (2 × 1010 cfu), B.longum (7 × 109 cfu), S. thermophilus (1.5 × 109 cfu) and 100 mg fructo-oligosaccharides | n = 27 Placebo: the same substance without bacteria | 8 weeks | BMI (kg/m2): −0.65 | BW (kg): −0.61 BMI (kg/m2): −0.26 |
| Shakeri, 2014 | RCT | 78 (35–70 years) | n = 26 The synbiotic bread contained probiotic L. sporogenes (1 × 108 cfu) and 0.07 g inulin as prebiotic per 1 g. n = 26 The probiotic bread contained L. sporogenes (1 × 108 cfu) per 1 g. | n = 26 Control bread: the same substance without probiotic bacteria and prebiotic inulin | 8 weeks | Synbiotic bread: BW (kg): (0.03 ± 1.9) BMI (kg/m2): (0.02 ± 0.8) Probiotic bread: BW (kg): (-0.2 ± 1.4) BMI (kg/m2): (−0.04 ± 0.6) | Control bread: BW (kg): (−0.05 ± 1.6) BMI (kg/m2): (−0.02 ± 0.6) |
| Mohamadshahi, 2014 | RCT | 44 (18–70 years) | n = 22 300 g/day of probiotic yogurt (L. delbrueckii subsp. bulgaricus and S. thermophilus + 3.7×106 cfu/g of both B. animalis subsp. lactis Bb12 and L. acidophilus strain La5 | n = 22 300 g/day of conventional yogurt | 8 weeks | BW (kg): −0.33 BMI (kg/m2): −0.12 WC (cm): 0.5 HC (cm): −0.15 | BW (kg): −0.72 BMI (kg/m2): −0.04 WC (cm): 0.34 HC (cm): 0.19 |
| Nabavi, 2014 | RCT | 72 (23–63 years) | n = 36 300 g/day of probiotic yogurt containing L. acidophilus La5 (4.42 × 106 cfu/g) and B. lactis Bb12 (3.85 × 106 cfu/g) | n = 36 300 g/day of conventional yogurt | 8 weeks | BW (kg): −1.74 BMI (kg/m2): −0.68 | BW (kg): −0.25 BMI (kg/m2): −0.11 |
| Alisi, 2014 | RCT | 48 (median age of treated group was 11 years, of placebo group was 10 years) | n = 24 Probiotic VLS#3, 1 sachet/day <10 years old or 2 sachet/day >10 years old | n = 24 Placebo, 1 sachet/day <10 years old or 2 sachet/day >10 years old | 16 weeks | BMI (kg/m2): −2.2 | BMI (kg/m2): 0.1 |
| Shavakhi, 2013 | RCT | 70 (18–75 years) | n = 34 Two tablets/day of metformin 500 mg + two tablets/day of Protexin (L. acidophilus 1 × 108 CFU, L. casei 5 × 108 CFU, L. rhamnosus 7.5 × 107 CFU, L. bulgaricus 1.5 × 108 CFU, B. breve 5 × 107 CFU, B. longum 2.5 × 107 CFU, S. thermophilus 5 × 107 CFU, fructooligosaccharides 350 mg) | n = 36 Two tablets/die of metformin 500 mg + two placebo tablets (120 mg of starch)/day | 24 weeks | BMI (kg/m2): −5.2 | BMI (kg/m2): −0.44 |
| Leber, 2012 | RT | 28 (24–66 years) | n = 13 3 bottles/day (65 ml) containing L. casei Shirota at a concentration of 108/ml (3 × 6.5 × 109 cfu L. casei Shirota) | n = 15 not received the product and served as a control group (standard). | 12 weeks | BW (kg): (−0.58 ± 2.54) BMI (kg/m2): (−0.18 ± 0.78) | BW (kg): (−0.13 ± 1.68) BMI (kg/m2): (−0.05 ± 0.60) |
| Chang, 2011 | RCT | 101 (20–65 years) | n = 53 Functional yogurt containing S. thermophilus ≥3 × 109c.f.u./g, L. acidophilus ≥3 × 109c.f.u./g, B. infantis ≥1 × 1010c.f.u./g and functional ingredients | n = 48 The control yogurts contained the same ingredients of S. thermophilus, L. acidophilus, B. infantis except functional ingredients | 8 weeks | BW (kg): (−0.24 ± 1.50) BMI (kg/m2): (−0.10 ± 0.58) WC (cm): (−0.45 ± 2.78) | BW (kg): ( + 0.64 ± 1.39) BMI (kg/m2): ( + 0.24 ± 0.50) WC (cm): ( + 0.42 ± 2.78) |
| Ogawa, 2014 | Single-blind, CT | 30 (27–69 years) | n = 15 200 g (2 portions of 100 g each) daily of FM with L. gasseri SBT2055 (LG2055) The viable cell count of LG2055 waproximately 5 × 1010 cfu/100g of FM on the initial day | n = 15 200 g (2 portions of 100 g each) daily of control FM without LG2055 L. gasseri SBT2055 (LG2055) | Control FM for 4 weeks; 4 weeks of washout period, active FM for 4 weeks | BW (kg): (−0.04 ± 0.12) BMI (kg/m2): (−0.01 ± 0.04) WC (cm): (−0.75 ± 0.35) | BW (kg): (−0.23 ± 0.26) BMI (kg/m2): (−0.09 ± 0.09) WC (cm): (−1.78 ± 0.53) |
| Sadrzadeh-Yaganeh, 2010 | RCT | 90 (19–49 years) | Group 1: n = 30 consumed daily 300 g probiotic yogurt containing L acidophilus La5 and B. lactis Bb12 (3.9 × 107 of both Bb12 and La5) Group 2: n = 30 consumed daily 300 g conventional yogurt | Group 3: n = 30 did not consume any fermented and probiotic products | 6 weeks | Group 1 BW (kg): 0.2 Group 2 BW (kg): 0.4 BMI (kg/m2): 0.2 | Group 3 No changes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perna, S.; Ilyas, Z.; Giacosa, A.; Gasparri, C.; Peroni, G.; Faliva, M.A.; Rigon, C.; Naso, M.; Riva, A.; Petrangolini, G.; et al. Is Probiotic Supplementation Useful for the Management of Body Weight and Other Anthropometric Measures in Adults Affected by Overweight and Obesity with Metabolic Related Diseases? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 666. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020666
Perna S, Ilyas Z, Giacosa A, Gasparri C, Peroni G, Faliva MA, Rigon C, Naso M, Riva A, Petrangolini G, et al. Is Probiotic Supplementation Useful for the Management of Body Weight and Other Anthropometric Measures in Adults Affected by Overweight and Obesity with Metabolic Related Diseases? A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(2):666. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020666
Chicago/Turabian StylePerna, Simone, Zahra Ilyas, Attilio Giacosa, Clara Gasparri, Gabriella Peroni, Milena Anna Faliva, Chiara Rigon, Maurizio Naso, Antonella Riva, Giovanna Petrangolini, and et al. 2021. "Is Probiotic Supplementation Useful for the Management of Body Weight and Other Anthropometric Measures in Adults Affected by Overweight and Obesity with Metabolic Related Diseases? A Systematic Review and Meta-Analysis" Nutrients 13, no. 2: 666. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020666