
Accidental Consumption of Aspartame in Phenylketonuria: Patient Experiences

 ,
,  and
and
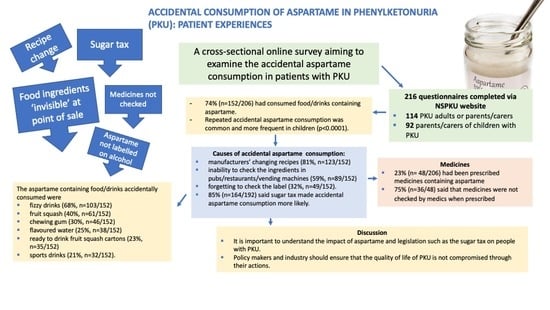
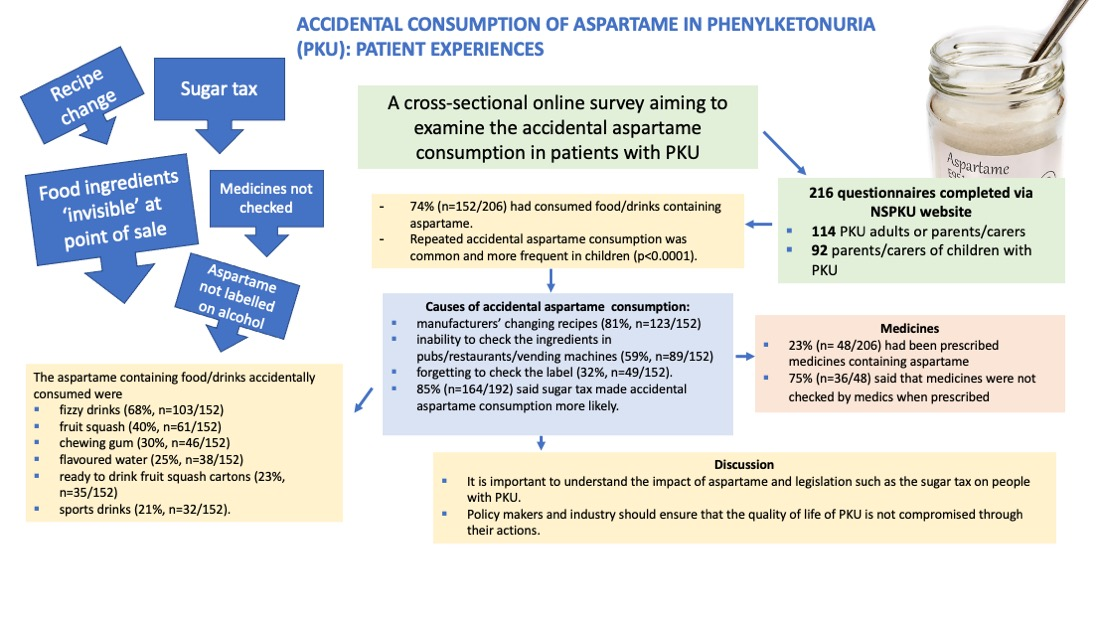
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collected
2.3. Statistics
2.4. Ethics
3. Results
3.1. Accidental Consumption of Aspartame in Food and Drink
- “Drinks that were previously free from aspartame and fine to drink had their recipe changed without seemingly advertising the change. This meant that it was only on consumption and tasting the difference from how it used to be that the ingredients were checked, and aspartame was found.”
- “I don’t know how many times I have consumed aspartame, but I know I have. In a crowded bar it is hard to request a specific brand name and it is not possible to read a label on a multi dispensing tap such as that used by bar staff to add coke or tonic to a drink.’’
- “I have never seen a lolly with aspartame in before, so I didn’t check it from the ice-cream man—I checked it only after she had eaten it.’’
- “Both my girls have autism. They do not understand consequences and are unable to challenge/ask people if the drinks contain aspartame, therefore they will just drink what is given to them. They have also picked up the wrong bottles of coke as the packaging is not much different at all’’.
- “Aspartame isn’t required to be listed on alcoholic drinks, therefore it’s hard to know if it’s present or not.’’
3.2. Foods/Drinks Involved in Accidental Aspartame Consumption
3.3. Aspartame Consumption of Medically Prescribed and over the Counter Medications
- “I checked the ingredients and found the medicine contained aspartame and had a written warning about phenylalanine. I called the doctor who couldn’t think of a different medicine so was told to go to hospital with my child to receive “better care.”
- “Happens a lot. There have been times when I’ve had to visit several chemists to finally get a variation without aspartame. I’ve also asked the GP to issue a script for an alternative medicine. It’s always down to the patient to check and Drs and pharmacists are unaware.’’
- “Always been told it’s best to take the medication and get better then worry about levels afterwards.’’
- “We checked, and it only had a small amount of aspartame and he was very poorly and he needed to have it.”
3.4. “Sugar Tax”
- “Drinks are something we can share and enjoy. Drinks that we could enjoy, experiment with, taste and talk about are now becoming less accessible and it has a really big impact on us. Sugar is actually one of the few things that we can ingest without fear of brain damage, and mental and physical damage.”
- “My daughter is aware of the higher cost of the non-aspartame products so will often choose to go without; thinking about the extra expense to us as parents.”
- “It has made an already difficult diet even harder to follow and people just think you are unhealthy choosing sugar versions and a faddy diet.”
- “Soul destroying for a person to check every food label/every morsel they put into their mouths”.
3.5. Choice of Drinks in Different Venues
3.6. Label Checking
3.7. Ease of Identifying Aspartame on the Ingredient Label
3.8. Challenges in Identifying Products which Contain Aspartame
- “Writing is often too small on supermarket products. Ingredients section often very full of text so hard to spot aspartame especially if you are rushing.”
- “Sometimes I find it tricky to identify aspartame in products due to weird E numbers that I have no idea about. Clear labelling of aspartame needs to be on all consumable products.’’
- “If eating out often, the restaurant staff are reluctant to check labels or are unsure about ingredients. Catering size products are not easy for staff to find info. Details of ingredients might only be listed on the outer packaging which may have been discarded.”
- “You are checking the label for aspartame, but the warning is not always in the same place”.
- “The warning text is very small. It inhibits my son’s independence as it’s unrealistic to expect a child to check for labelling that is so hard to see. After the sugar tax, packaging changed and removed the easy visual clues that you could rely on to indicate that the product had aspartame. As an example, there is now a Coca Cola in a red can which has aspartame in it. There are frequently types with aspartame in and some without with virtually the same packaging, you have to check everything, and this is stressful”.Many people commented about the time it takes to check labels.
- “We are really careful when we check labels, but it takes time, and it is difficult sometimes”.
- “I can easily identify aspartame in products with labels, but it is time consuming and annoying. I worry that other caregivers, e.g., grandparents, would not be able to. There is no labelling in restaurants, so we err on the side of caution and only order what we know does not contain aspartame.”
- “Should be written in bold/special box like allergens.”
- “Aspartame should be highlighted in a different colour or bold writing as they do for peanut allergies.”
3.9. Effect of Aspartame on People with PKU and Parents/Carers
- “It’s very isolating for our son. He feels people see him as fussy until we have to explain and even then, they don’t seem to understand.”
- “Feel bad when I can’t find suitable drinks for my children with PKU, whereas my children without PKU can drink whatever they want.”
- “The PKU diet is heavily restricted and time consuming. Aspartame adds another level of restriction and extra time is necessary to check everything before you can buy or eat it.”
- “Checking for aspartame increases stress and anxiety especially when eating out which is supposed to be a nice/happy experience.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fry, J. The world market for intense sweeteners. World Rev. Nutr. Diet 1999, 85, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Mazur, R.H. Aspartic Acid-Based Sweeteners; AVI Publishing: Westport, CT, USA, 1974. [Google Scholar]
- Mazur, R.H. Discovery of Aspartame; Marcel Dekker: New York, NY, USA, 1984. [Google Scholar]
- Mourad, I.M.; Noor, N.A. Aspartame (a widely used artificial sweetener) and oxidative stress in the rat cerebral cortex. Int. J. Pharm. Biomed. Sci. 2011, 2, 4–10. [Google Scholar]
- Yang, Q. Gain weight by “going diet?” Artificial sweeteners and the neurobiology of sugar cravings: Neuroscience 2010. Yale J. Biol. Med. 2010, 83, 101–108. [Google Scholar] [PubMed]
- Grembecka, M.; Szefer, P. Differentiation of Confectionery Products Based on Mineral Composition. Food Anal. Methods 2012, 5, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Mallikarjun, S.; Sieburth, R.M. Aspartame and Risk of Cancer: A Meta-analytic Review. Arch. Environ. Occup. Health 2015, 70, 133–141. [Google Scholar] [CrossRef] [PubMed]
- JECFA (Joint FAO/WHO Expert Committee on Food Additives). Toxicological Evaluation of Certain Food Additives: Aspartame; JECFA: Geneva, Switzerland, 1981. [Google Scholar]
- FDA (US Food and Drug Administration). Food Additives Permitted for Direct Addition to Food for Human Consumption: Aspartame; Register, F., Ed.; FDA: Silver Spring, MD, USA, 1996; pp. 33654–33656. [Google Scholar]
- EFSA Panel on Food Additives Nutrient Sources added to Food. Scientific Opinion on the re-evaluation of aspartame (E 951) as a food additive. EFSA J. 2013, 11, 3496. [Google Scholar] [CrossRef]
- MacDonald, A.; van Wegberg, A.M.J.; Ahring, K.; Beblo, S.; Bélanger-Quintana, A.; Burlina, A.; Campistol, J.; Coşkun, T.; Feillet, F.; Giżewska, M.; et al. PKU dietary handbook to accompany PKU guidelines. Orphanet J. Rare Dis. 2020, 15, 171. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.C.; Carvalho, T.S.; da Silva, F.B.; Pires, R.F.; Giugliani, R.; Pereira, M.L. Aspartame loading test in PKU heterozygous individuals bearing severe and moderate mutations. Clin. Genet. 2000, 58, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Stegink, L.D.; Filer, L.J., Jr.; Baker, G.L.; McDonnell, J.E. Effect of an abuse dose of aspartame upon plasma and erythrocyte levels of amino acids in phenylketonuric heterozygous and normal adults. J. Nutr. 1980, 110, 2216–2224. [Google Scholar] [CrossRef]
- Stegink, L.D.; Koch, R.; Blaskovics, M.E.; Filer, L.J., Jr.; Baker, G.L.; McDonnell, J.E. Plasma phenylalanine levels in phenylketonuric heterozygous and normal adults administered aspartame at 34 mg/kg body weight. Toxicology 1981, 20, 81–90. [Google Scholar] [CrossRef]
- Hillert, A.; Anikster, Y.; Belanger-Quintana, A.; Burlina, A.; Burton, B.K.; Carducci, C.; Chiesa, A.E.; Christodoulou, J.; Đorđević, M.; Desviat, L.R.; et al. The Genetic Landscape and Epidemiology of Phenylketonuria. Am. J. Hum. Genet. 2020, 107, 234–250. [Google Scholar] [CrossRef]
- Scala, I.; Concolino, D.; Della Casa, R.; Nastasi, A.; Ungaro, C.; Paladino, S.; Capaldo, B.; Ruoppolo, M.; Daniele, A.; Bonapace, G.; et al. Long-term follow-up of patients with phenylketonuria treated with tetrahydrobiopterin: A seven years experience. Orphanet J. Rare Dis. 2015, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [Green Version]
- EMA—Palynziq Product Information. Available online: https://www.ema.europa.eu/en/documents/product-information/palynziq-epar-product-information_en.pdf (accessed on 16 February 2021).
- Ford, S.; O’Driscoll, M.; MacDonald, A. Living with Phenylketonuria: Lessons from the PKU community. Mol. Genet. Metab. Rep. 2018, 17, 57–63. [Google Scholar] [CrossRef]
- European Parliament. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004 Text with EEA relevance. Official Journal of the European Union. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2011:304:0018:0063:en:PDF (accessed on 15 January 2021).
- The Soft Drinks Industry Levy (Enforcement) Regulations 2018; UK Statutory Instruments No 264; Legislation UK: London, UK, 2018.
- Rimmer, A. Don’t scrap the sugar tax, doctors tell Johnson. BMJ 2019, 367, l7051. [Google Scholar] [CrossRef] [PubMed]
- HMRC. Available online: https://www.gov.uk/government/publications/soft-drinks-industry-levy--2/soft-drinks-industry-levy-initial-equality-impact-assessment (accessed on 28 December 2020).
- Van Vliet, K.; Melis, E.S.; de Blaauw, P.; van Dam, E.; Maatman, R.; Abeln, D.; van Spronsen, F.J.; Heiner-Fokkema, M.R. Aspartame and Phe-Containing Degradation Products in Soft Drinks across Europe. Nutrients 2020, 12, 1887. [Google Scholar] [CrossRef]
- NSPKU Statement on Aspartame. Available online: https://www.nspku.org/download/statement-on-aspartame/ (accessed on 15 January 2021).
- CMPH (Committee for Medicinal Products for Human Use). Information for the Package Leaflet Regarding Aspartame and Phenylalanine Used as Excipients in Medicinal Products for Human Use; EMA/CHMP/134648/2015 corr. 1; European Medicine’s Agency: Amsterdam, The Netherlands, 2017.
- NHS Staff Health & Wellbeing: CQUIN 2017-19 Indicator 1 Implementation Support; NHS: London, UK, 2021.
- Food Labelling Food Standards Agency. Available online: https://labellingtraining.food.gov.uk/module10/overview_1.html (accessed on 15 January 2021).
- European Commission Labelling of Alcoholic Beverages in the EU: Some Facts. Available online: https://ec.europa.eu/food/safety/labelling_nutrition/labelling_legislation/alcohol_en (accessed on 12 January 2021).

{kind=link}
| Venue | Extremely Dissatisfied | Fairly Dissatisfied | Neither Dissatisfied nor Satisfied | Fairly Satisfied | Extremely Satisfied |
|---|---|---|---|---|---|
| Leisure Centre/Sports Centre (n = 165) | n = 42 (25%) | n = 68 (41%) | n = 20 (12%) | n = 30 (18%) | n = 5 (3%) |
| Hospital Clinics (n = 167) | n = 41 (25%) | n = 40 (24%) | n = 32 (19%) | n = 47 (28%) | n = 7 (4%) |
| Fast Food Chains (n = 193) | n = 47 (24%) | n = 73 (38%) | n = 23 (12%) | n = 41 (21%) | n = 9 (5%) |
| Pubs/Bars (n = 188) | n = 42 (22%) | n = 69 (37%) | n = 13 (7%) | n = 59 (31%) | n = 5 (3%) |
| Restaurants (n = 195) | n = 41 (21%) | n = 76 (39%) | n = 26 (13%) | n = 46 (24%) | n = 6 (3%) |
| Schools (n = 123) | n = 24 (20%) | n = 42 (34%) | n = 24 (20%) | n = 26 (21%) | n = 7 (6%) |
| Tourist Attraction e.g., Alton Towers (n = 170) | n = 32 (19%) | n = 65 (38%) | n = 26 (15%) | n = 40 (24%) | n = 7 (4%) |
| Motorway Cafes (n = 170) | n = 31 (18%) | n = 58 (34%) | n = 28 (16%) | n = 42 (25%) | n = 11 (6%) |
| Cafes (n = 197) | n = 34 (17%) | n = 63 (32%) | n = 32 (16%) | n = 63 (32%) | n = 5 (3%) |
| Hotels (n = 170) | n = 29 (17%) | n = 55 (32%) | n = 36 (21%) | n = 43 (25%) | n = 7 (4%) |
| Workplace (n = 113) | n = 19 (17%) | n = 30 (27%) | n = 25 (22%) | n = 29 (26%) | n = 10 (9%) |
| College (n = 64) | n = 10 (16%) | n = 23 (36%) | n = 17 (27%) | n = 13 (20%) | n = 1 (2%) |
| Airports (n = 165) | n = 24 (15%) | n = 45 (27%) | n = 38 (23%) | n = 43 (26%) | n = 15 (9%) |
| Nurseries (n = 73) | n = 10 (14%) | n = 21 (29%) | n = 22 (30%) | n = 17 (23%) | n = 3 (4%) |
| Petrol Stations (n = 180) | n = 23 (13%) | n = 49 (27%) | n = 25 (14%) | n = 64 (36%) | n = 19 (11%) |
| University (n = 65) | n = 7 (11%) | n = 24 (37%) | n = 18 (28%) | n = 13 (20%) | n = 3 (5%) |
| Other People’s Homes e.g., Friends/Family (n = 198) | n = 12 (6%) | n = 61 (31%) | n = 42 (21%) | n = 65 (33%) | n = 18 (9%) |
| Not at All | Rarely | Sometimes | Most of the Time | Always | |
|---|---|---|---|---|---|
| Food (n = 203) | n = 1 (<1%) | n = 13 (6%) | n = 24 (12%) | n = 51 (25%) | n = 114 (56%) |
| Drinks (n = 205) | n = 0 (0%) | n = 0 (0%) | n = 9 (4%) | n = 61 (30%) | n = 135 (66%) |
| Medicines (n = 203) | n = 8 (4%) | n = 18 (9%) | n = 18 (9%) | n = 30 (15%) | n = 129 (64%) |
| Adult (18 or Over) with PKU or Parent/Carer of Adult with PKU (Mean), n = 114 | Parent or Carer of Child with PKU (Mean), n = 92 | Total (Mean), n = 206 | Mann Whitney Test p Value | |
|---|---|---|---|---|
| Food | 4.07 | 4.58 | 4.30 | p < 0.001 |
| Drinks | 4.50 | 4.75 | 4.61 | p < 0.001 |
| Medicines | 3.86 | 4.74 | 4.25 | p < 0.001 |
| Very Difficult | Fairly Difficult | Neither Difficult nor Easy | Fairly Easy | Very Easy | |
|---|---|---|---|---|---|
| Food (n = 205) | n = 11 (5%) | n= 34 (17%) | n = 30 (15%) | n = 89 (43%) | n = 41 (20%) |
| Drinks (n = 205) | n = 8 (4%) | n = 40 (20%) | n = 24 (12%) | n = 80 (39%) | n = 53 (26%) |
| Medicines (n = 189) | n = 19 (10%) | n = 57 (30%) | n = 27 (14%) | n = 57 (30%) | n = 29 (15%) |
| Challenges Faced in Identifying If a Food, Drink or Medicine Contains Aspartame | Percentage Responses (%) | Number of Respondents Per Total Sample (n = 206) |
|---|---|---|
| Difficulties in Identifying Aspartame in Food or Drinks Consumed in Restaurants, Pubs, Cafes, Vending Machines | 77 | 158 |
| Similarities in Appearance of Non-Aspartame and Aspartame Containing Products | 62 | 127 |
| Time Taken to Identify if a Product Contains Aspartame | 56 | 115 |
| Unclear Labelling | 55 | 114 |
| Easy to Make Mistakes | 44 | 91 |
| Unable to Read the Writing on Food Labels (Writing too Small, too Shiny) | 42 | 87 |
| Lack of Knowledge about which Products Contain Aspartame | 20 | 42 |
| Have no Challenges | 4 | 8 |
| Other | 3 | 7 |
| Don’t Know | <1 | 1 |
| Effects of Aspartame | Percentage Responses (%) | Number of Respondents Per Total Sample (n = 206) |
|---|---|---|
| Limits Suitable Drinks in Restaurants/Pubs/Cafes | 86 | 178 |
| Increases Time taken to do Food Shopping | 80 | 164 |
| Causes Anxiety for Person with PKU | 52 | 106 |
| Causes Anxiety for Parent/Carer | 46 | 95 |
| Causes Guilt for Parent/Carer | 42 | 87 |
| Causes Social Isolation | 42 | 87 |
| Person with PKU unable to buy Food or Drinks from Shops, Causing Loss of Independence | 40 | 83 |
| Have to Keep Food Products Separate in the House between PKU and Non-PKU Products | 36 | 75 |
| Causes Person with PKU to Feel Unwell | 33 | 68 |
| Causes Guilt for Person with PKU | 33 | 67 |
| Has no Effect | 5 | 11 |
| Other | 4 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Newbould, E.; Pinto, A.; Evans, S.; Ford, S.; O’Driscoll, M.; Ashmore, C.; Daly, A.; MacDonald, A. Accidental Consumption of Aspartame in Phenylketonuria: Patient Experiences. Nutrients 2021, 13, 707. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020707
Newbould E, Pinto A, Evans S, Ford S, O’Driscoll M, Ashmore C, Daly A, MacDonald A. Accidental Consumption of Aspartame in Phenylketonuria: Patient Experiences. Nutrients. 2021; 13(2):707. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020707
Chicago/Turabian StyleNewbould, Ella, Alex Pinto, Sharon Evans, Suzanne Ford, Mike O’Driscoll, Catherine Ashmore, Anne Daly, and Anita MacDonald. 2021. "Accidental Consumption of Aspartame in Phenylketonuria: Patient Experiences" Nutrients 13, no. 2: 707. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020707