
The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Intervention
2.2. Recording Food and Drink Events with a Smartphone Application
2.3. Categorising Ingestion Events Based on Free-Text Annotations
2.4. Quantifying Compliance to the Study Intervention
2.5. Primary and Secondary Outcomes, Other Measurements
2.6. Statistical Analyses
3. Results
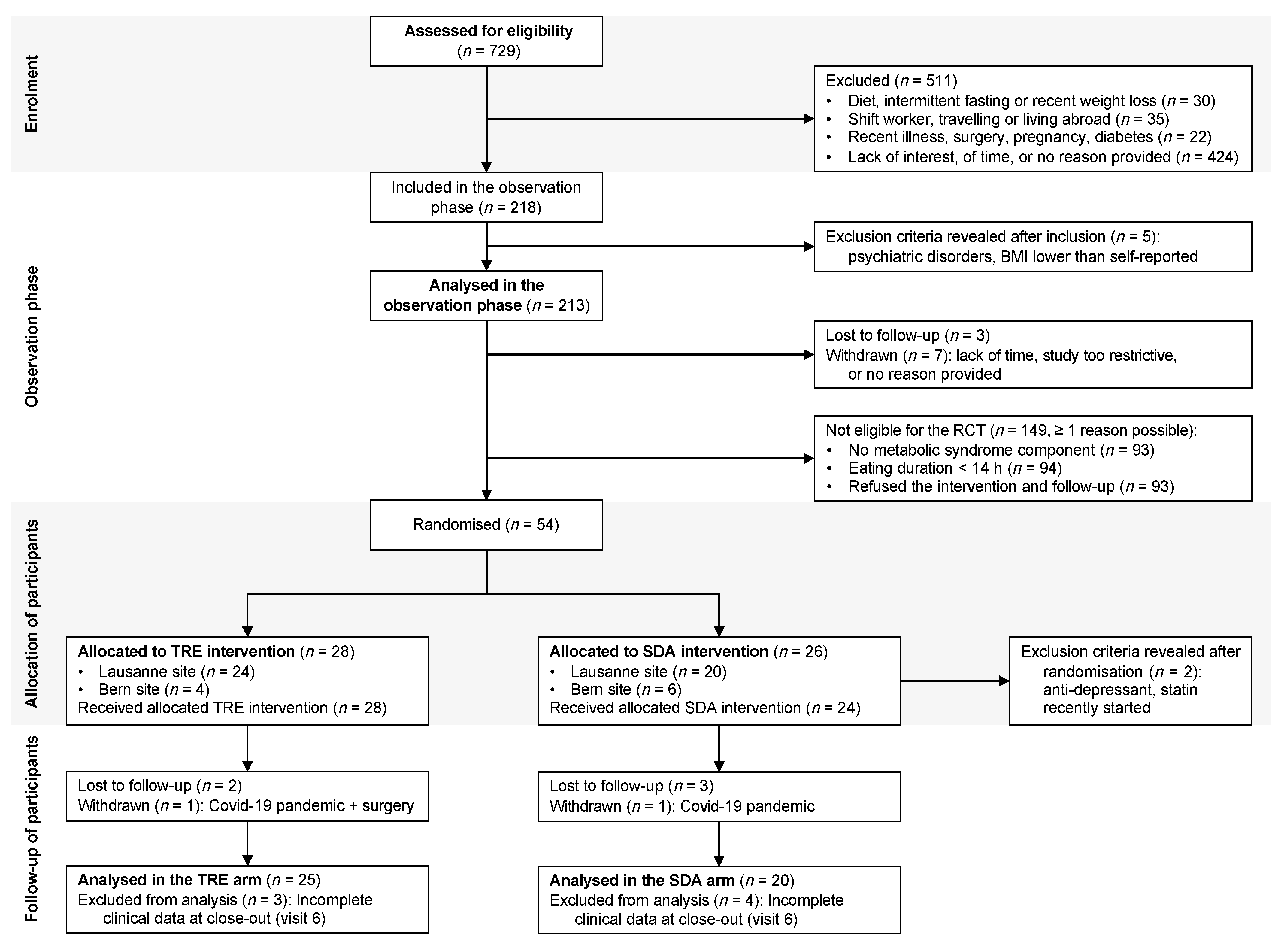
3.1. Recruitment of Participants
3.2. Baseline Characteristics of the Participants
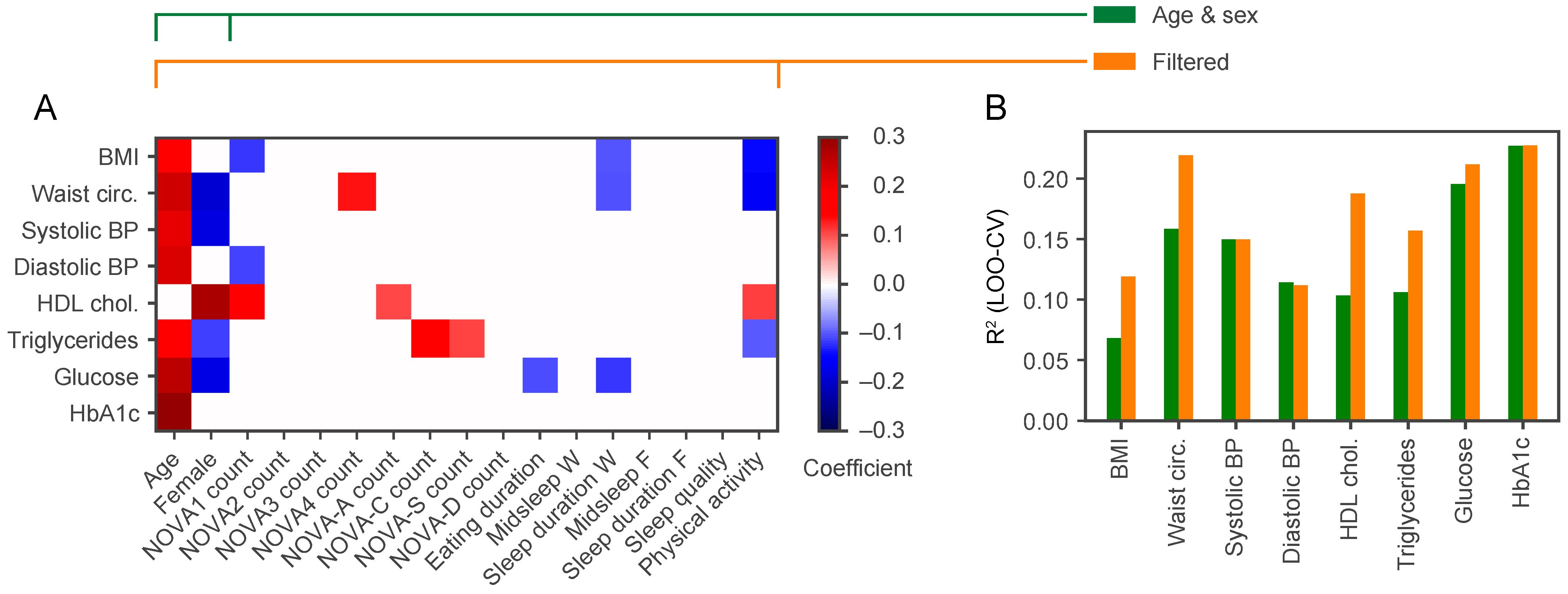
3.3. Relationship between Metabolic Health, Unprocessed and Processed Food Consumption at Baseline
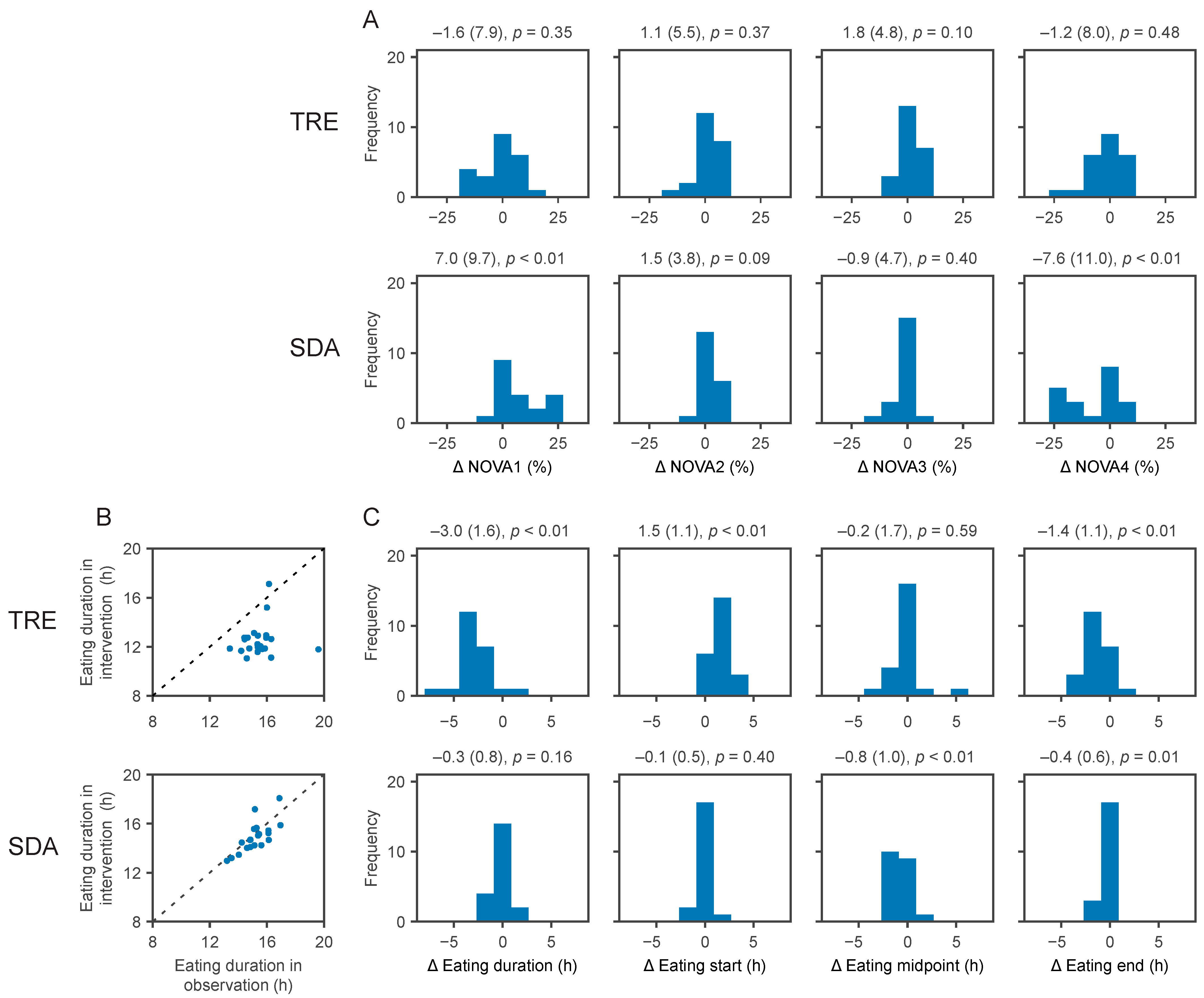
3.4. Compliance with the Randomly Assigned Interventions
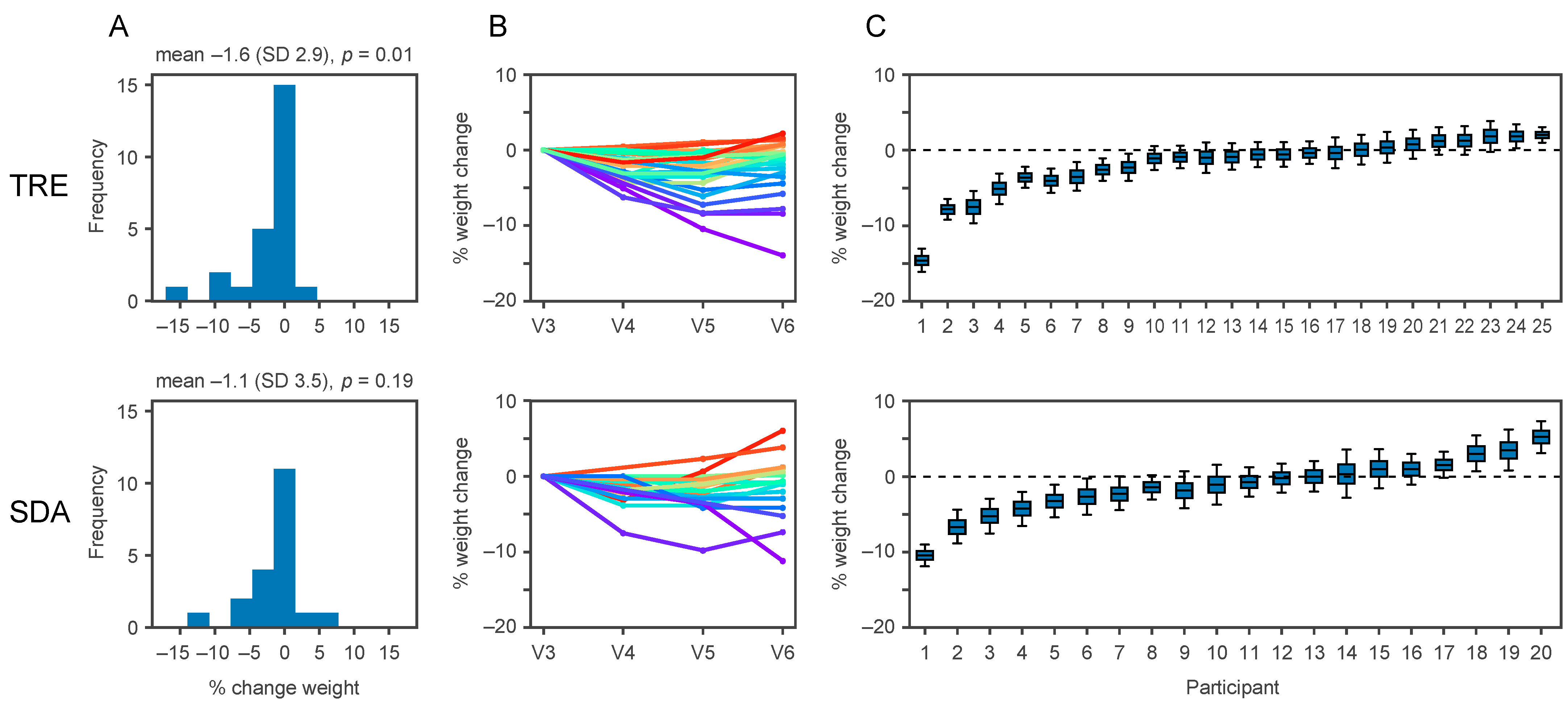
3.5. The Effects of TRE versus SDA on Clinical Outcomes
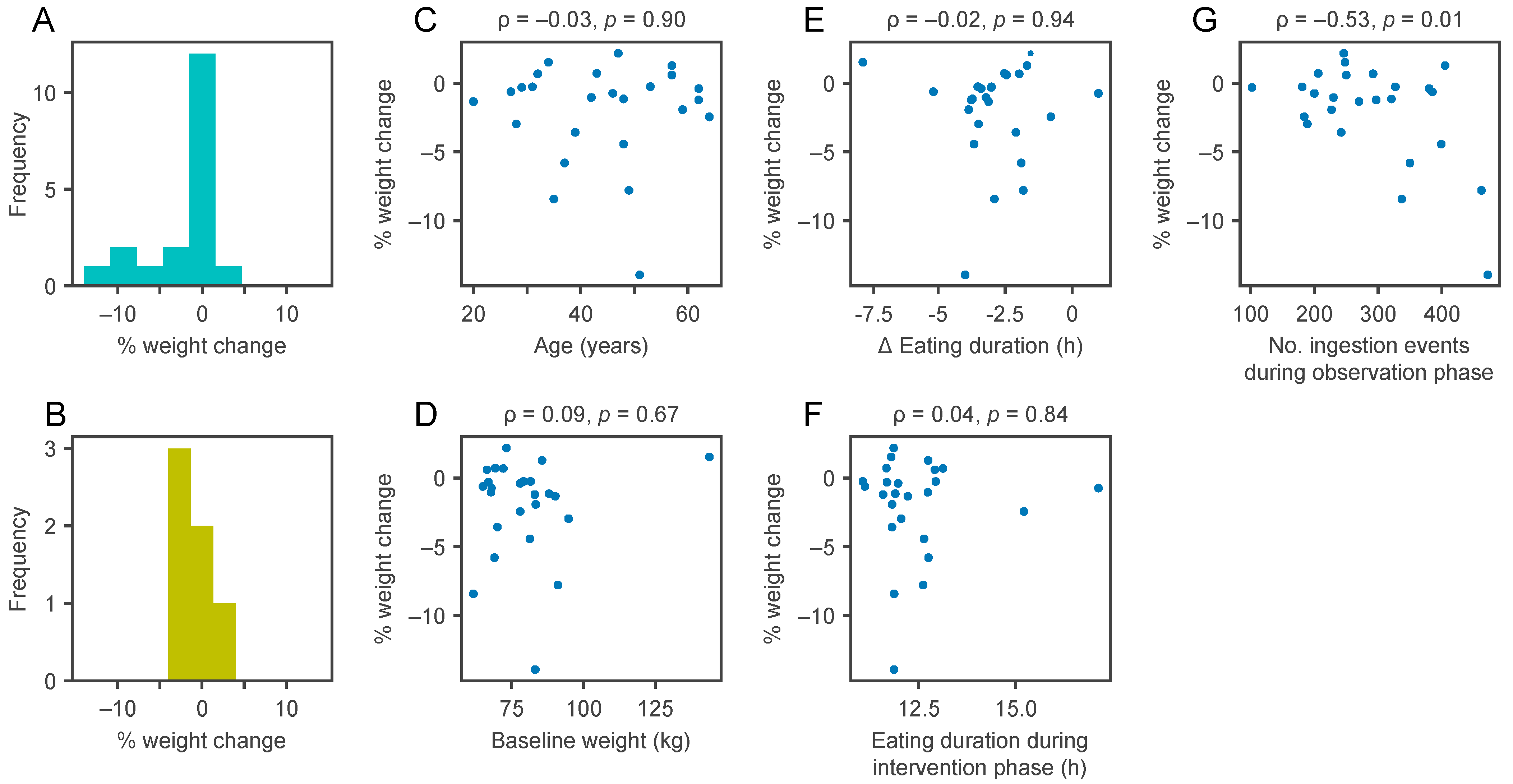
3.6. Weight Loss during the TRE Intervention Is Associated with the Number of Events Recorded in the Observation Phase
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Butler, J.; Rodondi, N.; Zhu, Y.; Figaro, K.; Fazio, S.; Vaughan, D.E.; Satterfield, S.; Newman, A.B.; Goodpaster, B.; Bauer, D.C.; et al. Metabolic Syndrome and the Risk of Cardiovascular Disease in Older Adults. J. Am. Coll. Cardiol. 2006, 47, 1595–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A.; Frühbeck, G.; Ryan, D.H.; Wilding, J.P.H. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef] [Green Version]
- Khera, R.; Murad, M.H.; Chandar, A.K.; Dulai, P.S.; Wang, Z.; Prokop, L.J.; Loomba, R.; Camilleri, M.; Singh, S. Association of Pharmacological Treatments for Obesity With Weight Loss and Adverse Events: A Systematic Review and Meta-Analysis. JAMA 2016, 315, 2424–2434. [Google Scholar] [CrossRef]
- Horne, B.D.; Muhlestein, J.B.; Anderson, J.L. Health effects of intermittent fasting: Hormesis or harm? A systematic review. Am. J. Clin. Nutr. 2015, 102, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Di Francesco, A.; Di Germanio, C.; Bernier, M.; De Cabo, R. A time to fast. Science 2018, 362, 770–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G.; Leeuwenburgh, C.; Mattson, M.P. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obes. Silver Spring 2018, 26, 254–268. [Google Scholar] [CrossRef]
- Chaix, A.; Manoogian, E.N.C.; Melkani, G.C.; Panda, S. Time-Restricted Eating to Prevent and Manage Chronic Metabolic Diseases. Annu. Rev. Nutr. 2019, 39, 291–315. [Google Scholar] [CrossRef]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef] [PubMed]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-h time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Antoni, R.; Robertson, T.M.; Robertson, M.D.; Johnston, J.D. A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. J. Nutr. Sci. 2018, 7, 107. [Google Scholar] [CrossRef] [Green Version]
- Świątkiewicz, I.; Woźniak, A.; Taub, P.R. Time-Restricted Eating and Metabolic Syndrome: Current Status and Future Perspectives. Nutrients 2021, 13, 221. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.S.; Manoogian, E.N.C.; Alvear, A.; Fleischer, J.G.; Thor, H.; Dietsche, K.; Wang, Q.; Hodges, J.S.; Esch, N.; Malaeb, S.; et al. Time-Restricted Eating Effects on Body Composition and Metabolic Measures in Humans who are Overweight: A Feasibility Study. Obes. Silver Spring 2020, 28, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Kesztyüs, D.; Cermak, P.; Gulich, M.; Kesztyüs, T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre-Post Design. Nutrients 2019, 11, 2854. [Google Scholar] [CrossRef] [Green Version]
- Peeke, P.M.; Greenway, F.L.; Billes, S.K.; Zhang, D.; Fujioka, K. Effect of time restricted eating on body weight and fasting glucose in participants with obesity: Results of a randomized, controlled, virtual clinical trial. Nutr. Diabetes 2021, 11, 6. [Google Scholar] [CrossRef]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef] [Green Version]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-restricted feeding improves glucose tolerance in men at risk for type 2 diabetes: A randomized crossover trial. Obesity 2019, 26, 759. [Google Scholar] [CrossRef]
- Dhurandhar, N.V.; Schoeller, D.A.; Brown, A.W.; Heymsfield, S.B.; Thomas, D.M.; Sørensen, T.I.A.; Speakman, J.R.; Jeansonne, M.; Allison, D.B.; Energy Balance Measurement Working Group. Energy balance measurement: When something is not better than nothing. Int. J. Obes. 2015, 39, 1109–1113. [Google Scholar] [CrossRef] [Green Version]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Costa Louzada, M.L.; Pereira Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2017, 21, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fardet, A.; Rock, E.; Bassama, J.; Bohuon, P.; Prabhasankar, P.; Monteiro, C.; Moubarac, J.-C.; Achir, N. Current Food Classifications in Epidemiological Studies Do Not Enable Solid Nutritional Recommendations for Preventing Diet-Related Chronic Diseases: The Impact of Food Processing. Adv. Nutr. 2015, 6, 629–638. [Google Scholar] [CrossRef]
- Swiss Society for Nutrition; Federal Food Safety and Veterinary Office. Pyramide Alimentaire Suisse (Swiss Food Pyramid). Available online: https://www.sge-ssn.ch/fr/toi-et-moi/boire-et-manger/equilibre-alimentaire/pyramide-alimentaire-suisse (accessed on 31 December 2020).
- Montagnese, C.; Santarpia, L.; Buonifacio, M.; Nardelli, A.; Caldara, A.R.; Silvestri, E.; Contaldo, F.; Pasanisi, F. European food-based dietary guidelines: A comparison and update. Nutr. Burbank Los Angel. Cty. Calif. 2015, 31, 908–915. [Google Scholar] [CrossRef]
- Firmann, M.; Mayor, V.; Vidal, P.M.; Bochud, M.; Pécoud, A.; Hayoz, D.; Paccaud, F.; Preisig, M.; Song, K.S.; Yuan, X.; et al. The CoLaus study: A population-based study to investigate the epidemiology and genetic determinants of cardiovascular risk factors and metabolic syndrome. BMC Cardiovasc. Disord. 2008, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Julia, C.; Martinez, L.; Allès, B.; Touvier, M.; Hercberg, S.; Méjean, C.; Kesse-Guyot, E. Contribution of ultra-processed foods in the diet of adults from the French NutriNet-Santé study. Public Health Nutr. 2018, 21, 27–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, E.M.; Baraldi, L.G.; Louzada, M.L.D.C.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-processed foods and added sugars in the US diet: Evidence from a nationally representative cross-sectional study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [Green Version]
- Petak, S.; Barbu, C.G.; Yu, E.W.; Fielding, R.; Mulligan, K.; Sabowitz, B.; Wu, C.-H.; Shepherd, J.A. The Official Positions of the International Society for Clinical Densitometry: Body Composition Analysis Reporting. J. Clin. Densitom. Off. J. Int. Soc. Clin. Densitom. 2013, 16, 508–519. [Google Scholar] [CrossRef]
- Micklesfield, L.K.; Goedecke, J.H.; Punyanitya, M.; Wilson, K.E.; Kelly, T.L. Dual-Energy X-Ray Performs as Well as Clinical Computed Tomography for the Measurement of Visceral Fat. Obes. Silver Spring 2012, 20, 1109–1114. [Google Scholar] [CrossRef]
- Kaul, S.; Rothney, M.P.; Peters, D.M.; Wacker, W.K.; Davis, C.E.; Shapiro, M.D.; Ergun, D.L. Dual-Energy X-Ray Absorptiometry for Quantification of Visceral Fat. Obes. Silver Spring 2012, 20, 1313–1318. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index—A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between Clocks: Daily Temporal Patterns of Human Chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef] [Green Version]
- Gelman, A.; Carlin, J.B.; Stern, H.S.; Dunson, D.B.; Vehtari, A.; Rubin, D.B. Bayesian Data Analysis, 3rd ed.; CRC Press: London, UK, 2013. [Google Scholar]
- Carpenter, B.; Gelman, A.; Hoffman, M.D.; Lee, D.; Goodrich, B.; Betancourt, M.; Brubaker, M.; Guo, J.; Li, P.; Riddell, A. Stan: A Probabilistic Programming Language. J. Stat. Softw. 2017, 76, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Fergusson, D.; Aaron, S.D.; Guyatt, G.; Hébert, P. Post-randomisation exclusions: The intention to treat principle and excluding patients from analysis. BMJ 2002, 325, 652–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juul, F.; Hemmingsson, E. Trends in consumption of ultra-processed foods and obesity in Sweden between 1960 and 2010. Public Health Nutr. 2015, 18, 3096–3107. [Google Scholar] [CrossRef] [Green Version]
- Juul, F.; Simões, B.D.S.; Litvak, J.; Martinez-Steele, E.; Deierlein, A.; Vadiveloo, M.; Parekh, N. Processing level and diet quality of the US grocery cart: Is there an association? Public Health Nutr. 2019, 22, 2357–2366. [Google Scholar] [CrossRef]
- Beslay, M.; Srour, B.; Méjean, C.; Allès, B.; Fiolet, T.; Debras, C.; Chazelas, E.; Deschasaux, M.; Wendeu-Foyet, M.G.; Hercberg, S.; et al. Ultra-processed food intake in association with BMI change and risk of overweight and obesity: A prospective analysis of the French NutriNet-Santé cohort. PLoS Med. 2020, 17, e1003256. [Google Scholar] [CrossRef]
- Ellison, R.C.; Zhang, Y.; Qureshi, M.M.; Knox, S.; Arnett, D.K.; Province, M.A. Lifestyle determinants of high-density lipoprotein cholesterol: The National Heart, Lung, and Blood Institute Family Heart Study. Am. Heart J. 2004, 147, 529–535. [Google Scholar] [CrossRef]
- Cai, L.; Ma, D.; Zhang, Y.; Liu, Z.; Wang, P. The effect of coffee consumption on serum lipids: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2012, 66, 872–877. [Google Scholar] [CrossRef]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P. For the CONSORT NPT Group CONSORT Statement for Randomized Trials of Nonpharmacologic Treatments: A 2017 Update and a CONSORT Extension for Nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women (n = 152) | Men (n = 61) | Overall (n = 213) | p for Comparison a | |
|---|---|---|---|---|
| Demographics | ||||
| Age, mean (SD) | 40.2 (13.3) | 40.1 (13.4) | 40.1 (13.3) | 0.96 |
| Marital status b, n (%) | 0.92 | |||
| Married, partnership | 96 (72%) | 39 (71%) | 135 (71%) | |
| Single, separated, widow(er) | 38 (28%) | 16 (29%) | 54 (29%) | |
| Education b, n (%) | 0.23 | |||
| Primary, secondary | 16 (10%) | 6 (10%) | 22 (10%) | |
| Apprenticeship, vocational | 27 (18%) | 7 (12%) | 34 (16%) | |
| Professional school | 27 (18%) | 6 (10%) | 33 (16%) | |
| University, or higher degree | 81 (54%) | 41 (68%) | 122 (58%) | |
| Born in Switzerland, n (%) | 94 (62%) | 37 (61%) | 131 (62%) | 0.87 |
| Clinical characteristics | ||||
| Weight, kg, median (IQR) | 69.0 (62.7–80.1) | 83.6 (74.2–95.5) | 73.3 (65.0–84.2) | <0.0001 |
| BMI, kg/m2, median (IQR) | 24.6 (22.2–29.0) | 25.3 (23.4–29.5) | 24.9 (22.6–29.1) | 0.16 |
| BMI < 25.0 kg/m2, n (%) | 81 (53%) | 29 (48%) | 110 (52%) | |
| BMI 25.0–29.9 kg/m2, n (%) | 40 (26%) | 18 (30%) | 58 (27%) | |
| BMI ≥ 30.0 kg/m2, n (%) | 31 (20%) | 14 (23%) | 45 (21%) | |
| WC, cm, median (IQR) | 81.8 (73.5–92.3) | 90.0 (81.0–101.5) | 84.5 (75.5–97.0) | 0.0001 |
| Current smokers, n (%) | 21 (14%) | 13 (21%) | 34 (16%) | 0.18 |
| Cardiovascular disease c, n (%) | 3 (2%) | 5 (8%) | 8 (4%) | 0.045 |
| Endocrine disorder d, n (%) | 14 (9%) | 0 | 14 (7%) | 0.01 |
| Respiratory disorder, n (%) | 20 (13%) | 10 (16%) | 30 (14%) | 0.54 |
| Metabolic syndrome (MS) e | ||||
| MS components, n (%) | ||||
| 1. Central obesity | 84 (55%) | 24 (39%) | 108 (51%) | 0.04 |
| 2. Hypertension | 30 (20%) | 26 (43%) | 56 (26%) | <0.001 |
| 3. Impaired fasting glucose | 13 (9%) | 17 (29%) | 30 (14%) | <0.001 |
| 4. High triglycerides | 12 (8%) | 14 (24%) | 26 (12%) | 0.002 |
| 5. Low HDL-cholesterol | 21 (14%) | 6 (10%) | 27 (13%) | 0.46 |
| MS by the IDF definition, n (%) | 17 (11%) | 13 (21%) | 30 (14%) | 0.055 |
| Lifestyle | ||||
| Sleep duration f, hours, mean (SD) | 7.47 (0.94) | 6.99 (0.80) | 7.33 (0.93) | <0.001 |
| Sleep quality g, mean (SD) | 5.3 (2.8) | 5.0 (2.8) | 5.2 (2.8) | 0.31 |
| Physical activity h, median (IQR) | 1289 (687–2232) | 1884 (930–2849) | 1386 (693–2598) | 0.06 |
| Time-Restricted Eating (TRE) | Standard Dietary Advice (SDA) | Between- Group Difference (95% Confidence Interval) b | p for Comparison of Pre–Post Changes between TRE and SDA a | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Pre-Intervention | Post-Intervention | p for Comparison (Pre–Post) a | Pre-Intervention | Post-Intervention | p For Comparison (Pre-Post) a | ||
| Weight, kg | 79.6 (15.9) | 78.0 (16.4) | 0.01 | 77.5 (13.8) | 76.4 (12.7) | 0.19 | −0.5 (−2.4; 1.4) | 0.61 |
| Body mass index, kg/m2 | 28.0 (4.1) | 27.5 (4.3) | 0.01 | 27.0 (4.0) | 26.7 (4.0) | 0.20 | −0.2 (−0.9; 0.4) | 0.52 |
| Waist circumference, cm | 92.4 (11.6) | 90.9 (12.4) | 0.04 | 90.1 (11.0) | 88.0 (10.5) | 0.09 | 0.6 (−2.0; 3.2) | 0.64 |
| Systolic BP, mmHg | 123.8 (11.2) | 125.1 (13.4) | 0.57 | 126.4 (10.5) | 122.3 (13.5) | 0.12 | 5.5 (−1.2; 12.2) | 0.12 |
| Diastolic BP, mmHg | 79.3 (11.0) | 81.2 (10.7) | 0.36 | 81.0 (9.6) | 79.5 (11.0) | 0.36 | 3.5 (−1.7; 8.6) | 0.21 |
| HDL cholesterol, mmol/L | 1.47 (0.37) | 1.46 (0.38) | 0.76 | 1.44 (0.29) | 1.41 (0.29) | 0.19 | 0.02 (−0.08; 0.12) | 0.70 |
| Triglycerides, mmol/L | 1.35 (0.66) | 1.24 (0.57) | 0.24 | 1.19 (0.50) | 1.03 (0.36) | 0.09 | 0.05 (−0.20; 0.30) | 0.69 |
| Fasting plasma glucose, mmol/L | 5.21 (0.56) | 5.04 (0.53) | 0.15 | 5.17 (0.67) | 5.29 (0.55) | 0.40 | −0.29 (−0.64; 0.07) | 0.12 |
| HbA1c, % | 5.30 (0.44) | 5.33 (0.39) | 0.55 | 5.23 (0.35) | 5.14 (0.29) | 0.02 | 0.12 (0.01; 0.23) | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phillips, N.E.; Mareschal, J.; Schwab, N.; Manoogian, E.N.C.; Borloz, S.; Ostinelli, G.; Gauthier-Jaques, A.; Umwali, S.; Gonzalez Rodriguez, E.; Aeberli, D.; et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients 2021, 13, 1042. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13031042
Phillips NE, Mareschal J, Schwab N, Manoogian ENC, Borloz S, Ostinelli G, Gauthier-Jaques A, Umwali S, Gonzalez Rodriguez E, Aeberli D, et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients. 2021; 13(3):1042. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13031042
Chicago/Turabian StylePhillips, Nicholas Edward, Julie Mareschal, Nathalie Schwab, Emily N. C. Manoogian, Sylvie Borloz, Giada Ostinelli, Aude Gauthier-Jaques, Sylvie Umwali, Elena Gonzalez Rodriguez, Daniel Aeberli, and et al. 2021. "The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults" Nutrients 13, no. 3: 1042. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13031042