
Orosensory Perception of Fat/Sweet Stimuli and Appetite-Regulating Peptides before and after Sleeve Gastrectomy or Gastric Bypass in Adult Women with Obesity

 , , and
, , and
Abstract
:1. Introduction
2. Subjects and Methods
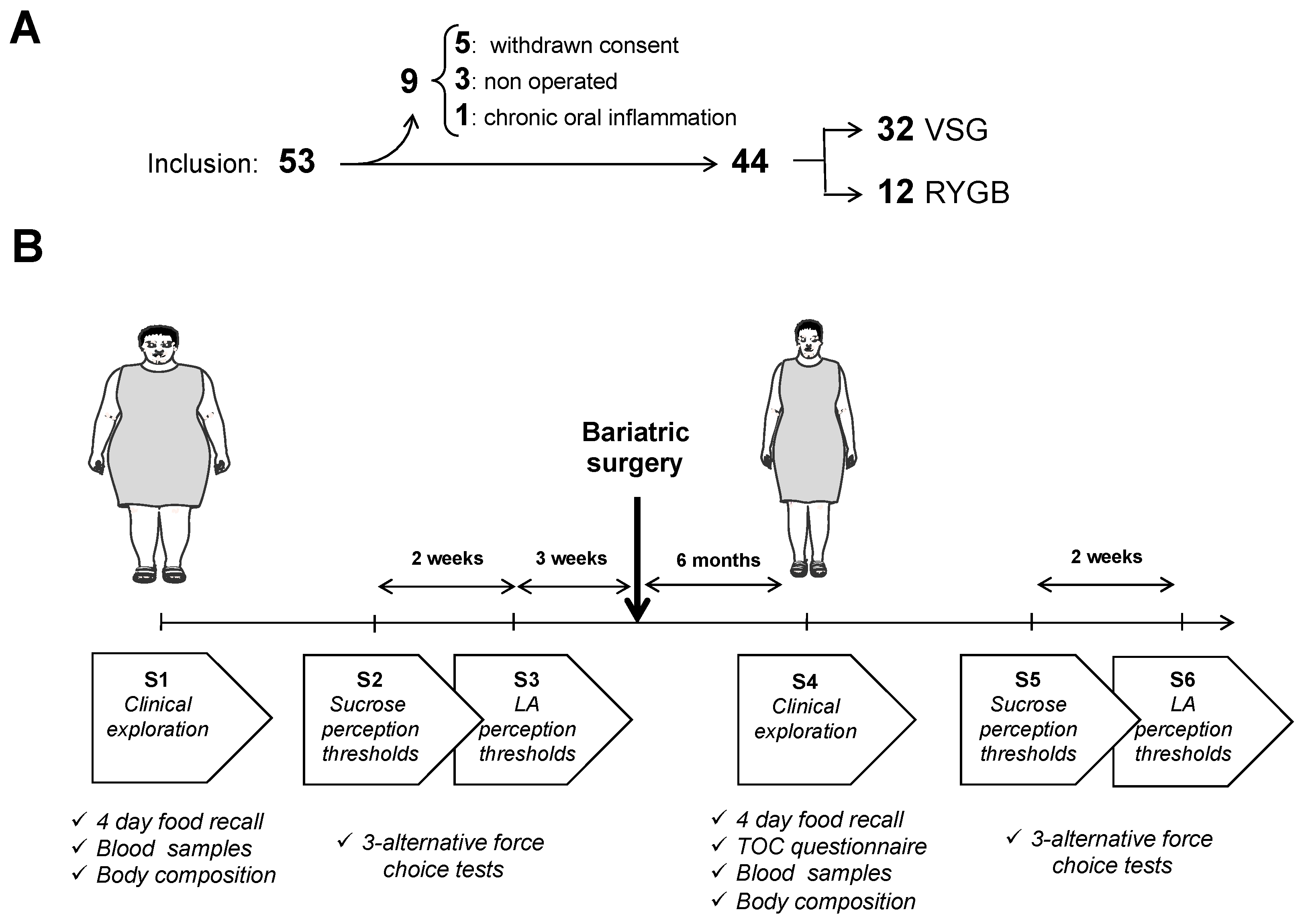
2.1. Subjects
2.2. 3-Alternative Force-Choice Tests
2.3. Preparation of Linoleic Acid Samples for 3-AFC Tests
2.4. Hormonal Assessments
2.5. Statistics
2.6. Power Analysis
3. Results
3.1. Changes of the Body Composition and Food Intake after VSG or RYGB
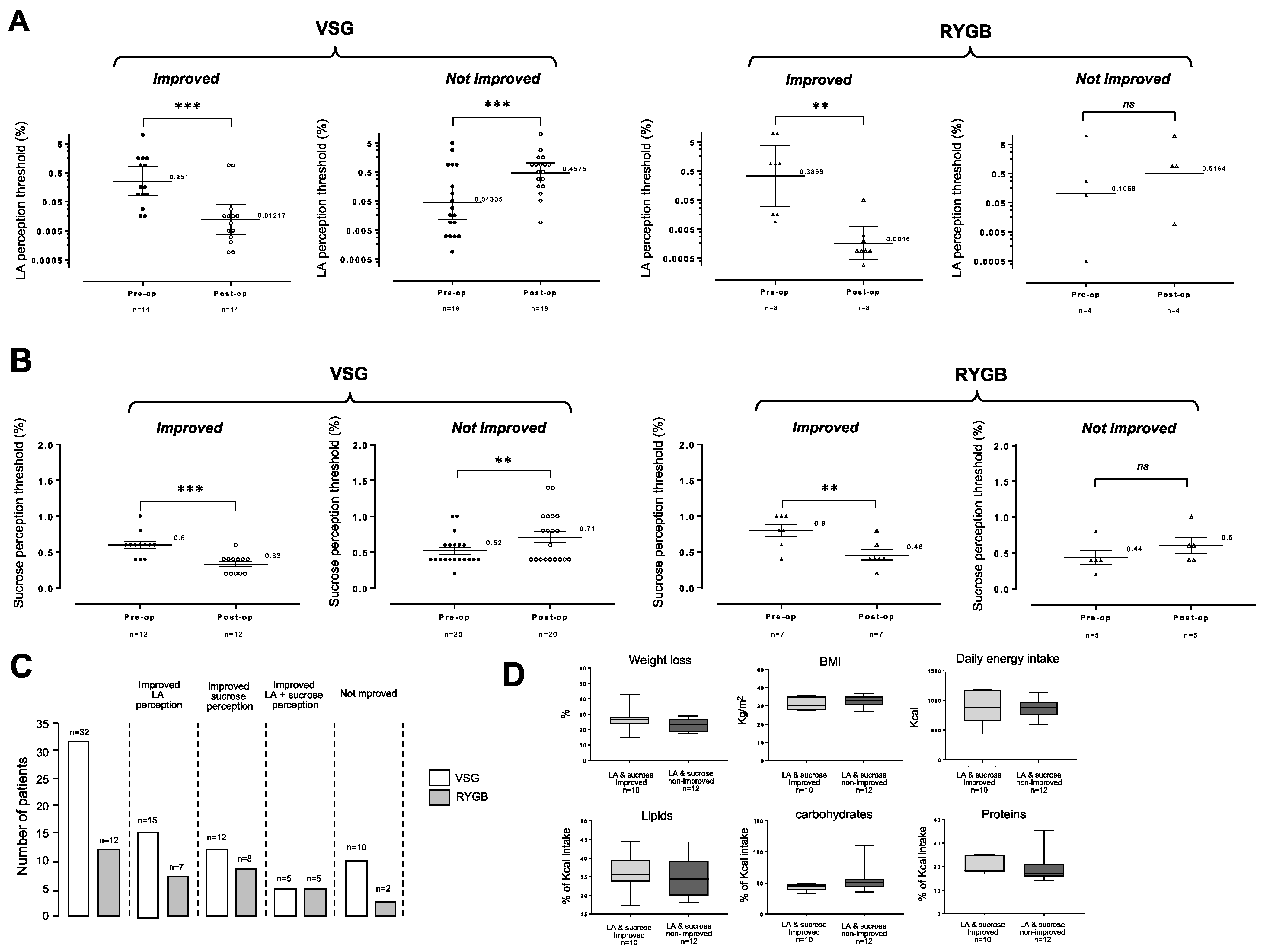
3.2. Impacts of VSG and RYGB on the Orosensory Perception of Lipid and Sweet Stimuli
3.3. Changes in Subjective Food Sensations after VSG or RYGB
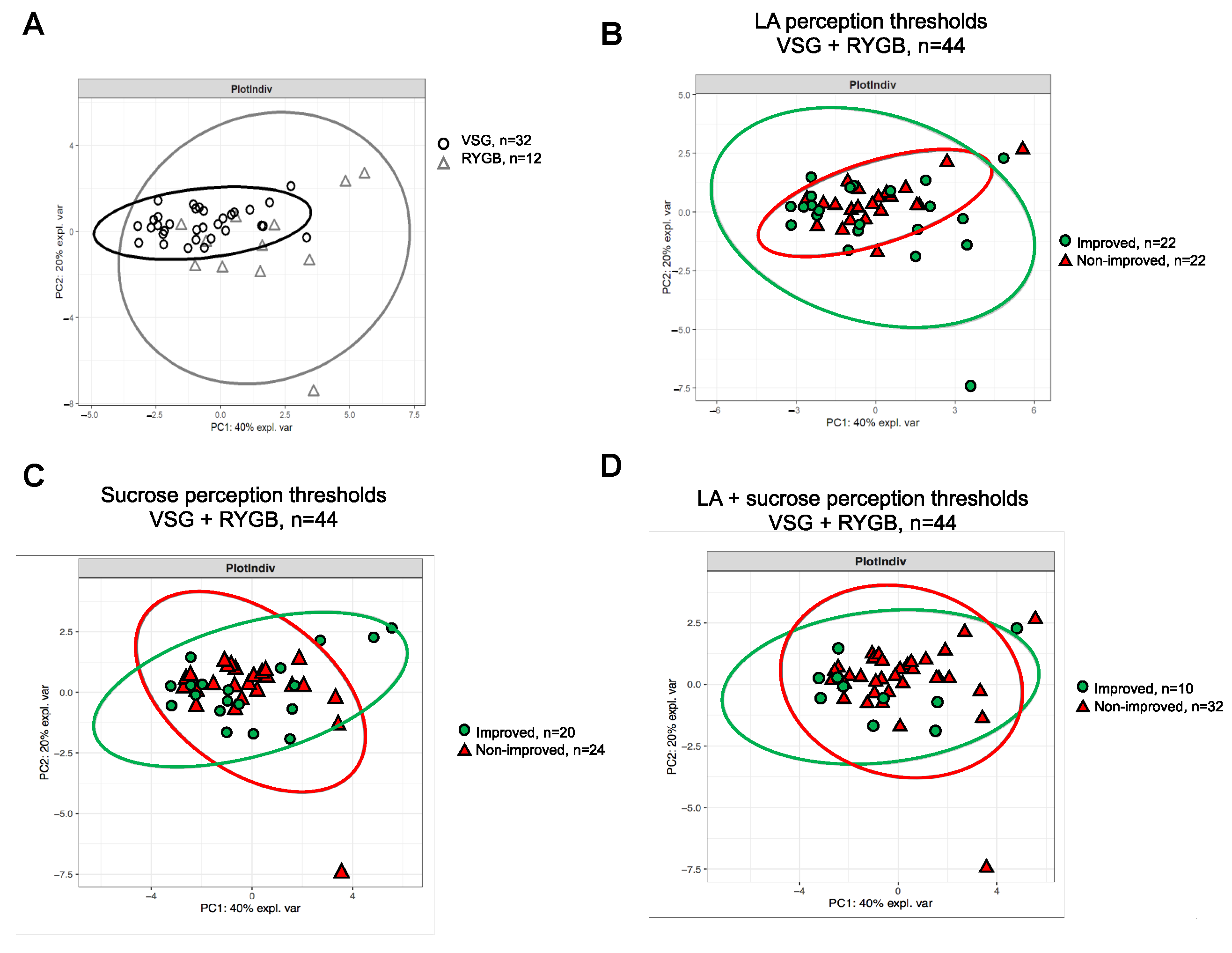
3.4. Impacts of Bariatric Surgery on the Fat and Sweet Tastes Are Not the Same in All Operated Patients
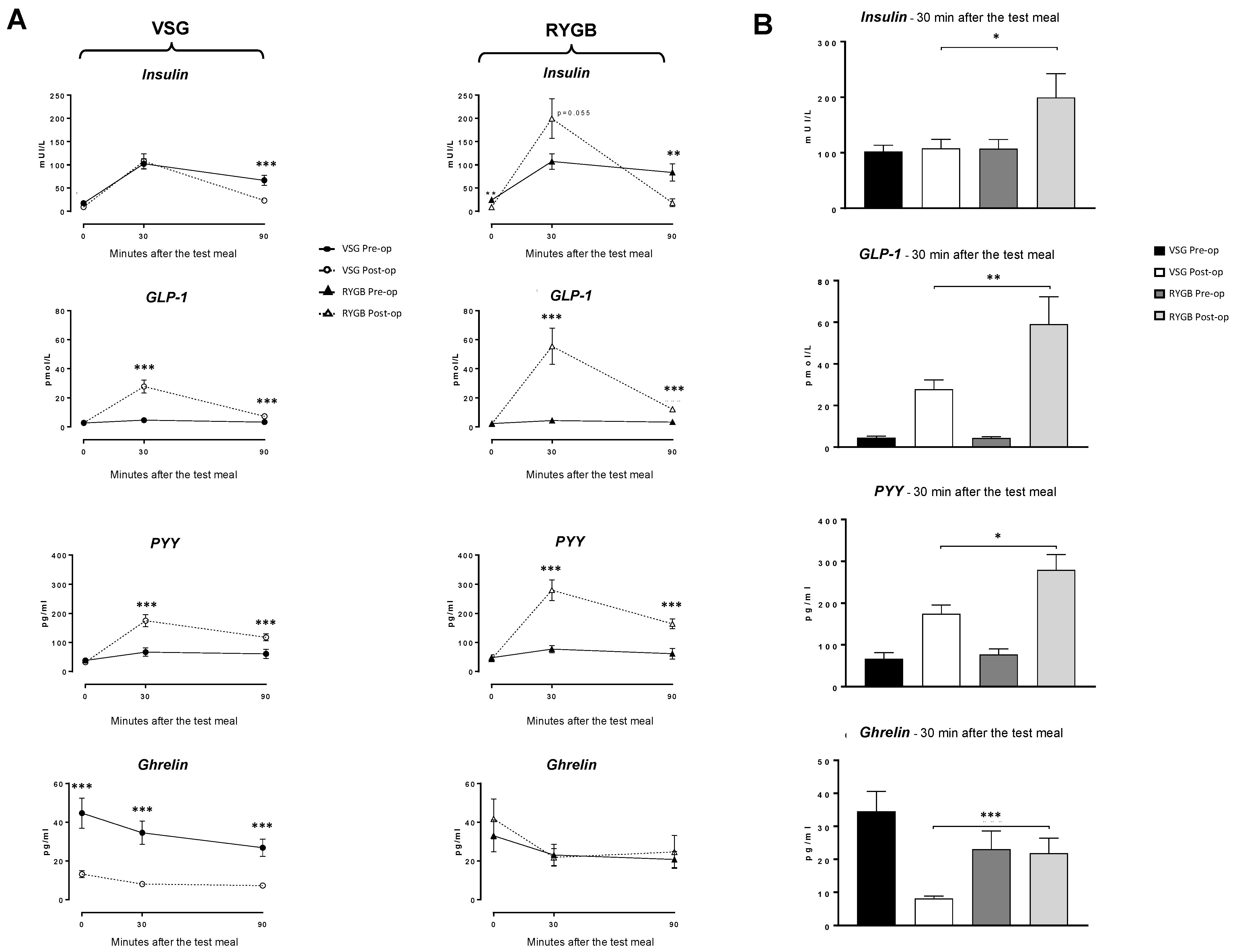
3.5. Relationships between Appetite-Regulating Peptides and Sweet and Fatty Taste Perceptions after VSG or RYGB
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drewnowski, A. Fat and sugar: An economic analysis. J. Nutr. 2003, 133, 838S–840S. [Google Scholar] [CrossRef]
- Stewart, J.E.; Feinle-Bisset, C.; Golding, M.; Delahunty, C.; Clifton, P.M.; Keast, R.S. Oral sensitivity to fatty acids, food consumption and BMI in human subjects. Br. J. Nutr. 2010, 104, 145–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proserpio, C.; Laureati, M.; Bertoli, S.; Battezzati, A.; Pagliarini, E. Determinants of Obesity in Italian Adults: The Role of Taste Sensitivity, Food Liking, and Food Neophobia. Chem. Sens. 2016, 41, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Ettinger, L.; Duizer, L.; Caldwell, T. Body fat, sweetness sensitivity, and preference: Determining the relationship. Can. J. Diet. Pract. Res. 2012, 73, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Brolin, R.E. Bariatric surgery and long-term control of morbid obesity. JAMA 2002, 288, 2793–2796. [Google Scholar] [CrossRef]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Formisano, G.; Buchwald, H.; Scopinaro, N. Bariatric Surgery Worldwide 2013. Obes. Surg. 2015, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Rubino, F.; Forgione, A.; Cummings, D.E.; Vix, M.; Gnuli, D.; Mingrone, G.; Castagneto, M.; Marescaux, J. The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes. Ann. Surg. 2006, 244, 741–749. [Google Scholar] [CrossRef]
- Bikman, B.T.; Zheng, D.; Pories, W.J.; Chapman, W.; Pender, J.R.; Bowden, R.C.; Reed, M.A.; Cortright, R.N.; Tapscott, E.B.; Houmard, J.A.; et al. Mechanism for improved insulin sensitivity after gastric bypass surgery. J. Clin. Endocrinol. Metab. 2008, 93, 4656–4663. [Google Scholar] [CrossRef] [Green Version]
- Besnard, P. Lipids and obesity: Also a matter of taste? Rev. Endocr. Metab. Disord. 2016, 17, 159–170. [Google Scholar] [CrossRef]
- Miras, A.D.; le Roux, C.W. Bariatric surgery and taste: Novel mechanisms of weight loss. Curr. Opin. Gastroenterol. 2010, 26, 140–145. [Google Scholar] [CrossRef]
- Ahmed, K.; Penney, N.; Darzi, A.; Purkayastha, S. Taste Changes after Bariatric Surgery: A Systematic Review. Obes. Surg. 2018, 28, 3321–3332. [Google Scholar] [CrossRef] [Green Version]
- Nance, K.; Acevedo, M.B.; Pepino, M.Y. Changes in taste function and ingestive behavior following bariatric surgery. Appetite 2020, 146, 104423. [Google Scholar] [CrossRef] [PubMed]
- Scruggs, D.M.; Buffington, C.; Cowan, G.S., Jr. Taste Acuity of the Morbidly Obese before and after Gastric Bypass Surgery. Obes. Surg. 1994, 4, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Pepino, M.Y.; Bradley, D.; Eagon, J.C.; Sullivan, S.; Abumrad, N.A.; Klein, S. Changes in taste perception and eating behavior after bariatric surgery-induced weight loss in women. Obesity 2014, 22, E13–E20. [Google Scholar] [CrossRef]
- El Labban, S.; Safadi, B.; Olabi, A. Effect of Roux-en-Y gastric bypass and sleeve gastrectomy on taste acuity and sweetness acceptability in postsurgical subjects. Nutrition 2016, 32, 1299–1302. [Google Scholar] [CrossRef] [PubMed]
- Nance, K.; Eagon, J.C.; Klein, S.; Pepino, M.Y. Effects of Sleeve Gastrectomy vs. Roux-en-Y Gastric Bypass on Eating Behavior and Sweet Taste Perception in Subjects with Obesity. Nutrients 2017, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Burge, J.C.; Schaumburg, J.Z.; Choban, P.S.; DiSilvestro, R.A.; Flancbaum, L. Changes in patients’ taste acuity after Roux-en-Y gastric bypass for clinically severe obesity. J. Am. Diet. Assoc. 1995, 95, 666–670. [Google Scholar] [CrossRef]
- Bueter, M.; Miras, A.D.; Chichger, H.; Fenske, W.; Ghatei, M.A.; Bloom, S.R.; Unwin, R.J.; Lutz, T.A.; Spector, A.C.; le Roux, C.W. Alterations of sucrose preference after Roux-en-Y gastric bypass. Physiol. Behav. 2011, 104, 709–721. [Google Scholar] [CrossRef] [Green Version]
- Holinski, F.; Menenakos, C.; Haber, G.; Olze, H.; Ordemann, J. Olfactory and Gustatory Function After Bariatric Surgery. Obes. Surg. 2015, 25, 2314–2320. [Google Scholar] [CrossRef]
- Altun, H.; Hanci, D.; Altun, H.; Batman, B.; Serin, R.K.; Karip, A.B.; Akyuz, U. Improved Gustatory Sensitivity in Morbidly Obese Patients After Laparoscopic Sleeve Gastrectomy. Ann. Otol. Rhinol. Laryngol. 2016, 125, 536–540. [Google Scholar] [CrossRef]
- Melis, M.; Pintus, S.; Mastinu, M.; Fantola, G.; Moroni, R.; Pepino, M.Y.; Barbarossa, I.T. Changes of Taste, Smell and Eating Behavior in Patients Undergoing Bariatric Surgery: Associations with PROP Phenotypes and Polymorphisms in the Odorant-Binding Protein OBPIIa and CD36 Receptor Genes. Nutrients 2021, 13, 250. [Google Scholar] [CrossRef]
- Drewnowski, A.; Almiron-Roig, E. Human Perceptions and Preferences for Fat-Rich Foods. In Fat Detection: Taste, Texture, and Post Ingestive Effects; Montmayeur, J.P., Le Coutre, J., Eds.; Taylor and Francis: Boca Raton, FL, USA, 2010. [Google Scholar]
- Dimitriadis, G.K.; Randeva, M.S.; Miras, A.D. Potential Hormone Mechanisms of Bariatric Surgery. Curr. Obes. Rep. 2017, 6, 253–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besnard, P.; Passilly-Degrace, P.; Khan, N.A. Taste of Fat: A Sixth Taste Modality? Physiol. Rev. 2016, 96, 151–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makaronidis, J.M.; Batterham, R.L. Potential Mechanisms Mediating Sustained Weight Loss Following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy. Endocrinol. Metab. Clin. N. Am. 2016, 45, 539–552. [Google Scholar] [CrossRef]
- Coupaye, M.; Riviere, P.; Breuil, M.C.; Castel, B.; Bogard, C.; Dupre, T.; Flamant, M.; Msika, S.; Ledoux, S. Comparison of nutritional status during the first year after sleeve gastrectomy and Roux-en-Y gastric bypass. Obes. Surg. 2014, 24, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Fried, M.; Yumuk, V.; Oppert, J.M.; Scopinaro, N.; Torres, A.; Weiner, R.; Yashkov, Y.; Fruhbeck, G. Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes. Surg. 2014, 24, 42–55. [Google Scholar] [CrossRef] [Green Version]
- Ledoux, S.; Sami, O.; Breuil, M.C.; Delapierre, M.; Calabrese, D.; Msika, S.; Coupaye, M. Relevance of Self-reported Behavioral Changes Before Bariatric Surgery to Predict Success After Surgery. Obes. Surg. 2017, 27, 1453–1459. [Google Scholar] [CrossRef]
- Tucker, R.M.; Kaiser, K.A.; Parman, M.A.; George, B.J.; Allison, D.B.; Mattes, R.D. Comparisons of Fatty Acid Taste Detection Thresholds in People Who Are Lean vs. Overweight or Obese: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169583. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.S.; Ritz, C.; Wewer Albrechtsen, N.J.; Holst, J.J.; le Roux, C.W.; Sjodin, A. Oxyntomodulin and Glicentin May Predict the Effect of Bariatric Surgery on Food Preferences and Weight Loss. J. Clin. Endocrinol. Metab. 2020, 105. [Google Scholar] [CrossRef]
- Zerrweck, C.; Zurita, L.; Alvarez, G.; Maydon, H.G.; Sepulveda, E.M.; Campos, F.; Caviedes, A.; Guilbert, L. Taste and Olfactory Changes Following Laparoscopic Gastric Bypass and Sleeve Gastrectomy. Obes. Surg. 2016, 26, 1296–1302. [Google Scholar] [CrossRef]
- Chale-Rush, A.; Burgess, J.R.; Mattes, R.D. Evidence for human orosensory (taste?) sensitivity to free fatty acids. Chem. Sens. 2007, 32, 423–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chevrot, M.; Passilly-Degrace, P.; Ancel, D.; Bernard, A.; Enderli, G.; Gomes, M.; Robin, I.; Issanchou, S.; Verges, B.; Nicklaus, S.; et al. Obesity interferes with the orosensory detection of long-chain fatty acids in humans. Am. J. Clin. Nutr. 2014, 99, 975–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Cao, K.A.; Gonzalez, I.; Dejean, S. integrOmics: An R package to unravel relationships between two omics datasets. Bioinformatics 2009, 25, 2855–2856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melissas, J.; Koukouraki, S.; Askoxylakis, J.; Stathaki, M.; Daskalakis, M.; Perisinakis, K.; Karkavitsas, N. Sleeve gastrectomy: A restrictive procedure? Obes. Surg. 2007, 17, 57–62. [Google Scholar] [CrossRef]
- Ravelli, M.N.; Ramirez, Y.P.G.; Quesada, K.; Rasera, I.; de Oliveira, M.R.M. Chapter 46—Underreporting of Energy Intake and Bariatric Surgery. In Metabolism and Pathophysiology of Bariatric Surgery; Rajendram, R., Martin, C.R., Preedy, V.R., Eds.; Academic Press: Boston, FL, USA, 2017; pp. 429–437. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Christensen, B.J.; Ritz, C.; Rasmussen, S.; Hansen, T.T.; Bredie, W.L.P.; Le Roux, C.W.; Sjodin, A.; Schmidt, J.B. Roux-En-Y Gastric Bypass and Sleeve Gastrectomy Does Not Affect Food Preferences When Assessed by an Ad libitum Buffet Meal. Obes. Surg. 2017, 27, 2599–2605. [Google Scholar] [CrossRef]
- Ochner, C.N.; Gibson, C.; Shanik, M.; Goel, V.; Geliebter, A. Changes in neurohormonal gut peptides following bariatric surgery. Int. J. Obes. 2011, 35, 153–166. [Google Scholar] [CrossRef] [Green Version]
- Thaler, J.P.; Cummings, D.E. Minireview: Hormonal and metabolic mechanisms of diabetes remission after gastrointestinal surgery. Endocrinology 2009, 150, 2518–2525. [Google Scholar] [CrossRef] [Green Version]
- le Roux, C.W.; Aylwin, S.J.; Batterham, R.L.; Borg, C.M.; Coyle, F.; Prasad, V.; Shurey, S.; Ghatei, M.A.; Patel, A.G.; Bloom, S.R. Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Ann. Surg. 2006, 243, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Maudsley, S.; Martin, B. What is the role of metabolic hormones in taste buds of the tongue. Front. Horm. Res. 2014, 42, 134–146. [Google Scholar] [CrossRef] [Green Version]
- Lager, C.J.; Esfandiari, N.H.; Subauste, A.R.; Kraftson, A.T.; Brown, M.B.; Cassidy, R.B.; Nay, C.K.; Lockwood, A.L.; Varban, O.A.; Oral, E.A. Roux-En-Y Gastric Bypass Vs. Sleeve Gastrectomy: Balancing the Risks of Surgery with the Benefits of Weight Loss. Obes. Surg. 2017, 27, 154–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | VSG (n = 32) | p-Value Pre-op vs. Post-op | RYGB (n=12) | p-Value Pre-op vs. Post-op | p-Value Post-op (VSG vs. RYGB) |
|---|---|---|---|---|---|
| Body mass (kg) | |||||
| Pre-op | 115.8 ± 2.3 | 111.7 ± 3.8 | ns | ||
| Post-op | 85.2 ± 2.1 | *** | 85.4 ± 3.0 | *** | ns |
| Weight loss (kg) | 30.5 ± 1.2 | 26.2 ± 1.7 | 0.06 | ||
| Weight loss (%) | 26.4 ± 1.0 | 23.3 ± 1.2 | ns | ||
| BMI (kg/m2) | |||||
| Pre-op | 43.1 ± 0.7 | 42.3 ± 1.0 | ns | ||
| Post-op | 31.6 ± 0.6 | *** | 32.1 ± 0.9 | *** | ns |
| Fat mass (% BM) | |||||
| Pre-op | 51.6 ± 0.5 | 51.2 ± 0.9 | ns | ||
| Post-op | 43.3 ± 1.0 | *** | 43.9 ± 1.2 | *** | ns |
| Variables | VSG (n = 32) | p-Value Pre-op vs. Post-op | RYGB (n = 12) | p-Value Pre-op vs. Post-op | p-Value Post-op (vsg vs. rygb) |
|---|---|---|---|---|---|
| Food intake (g/d) | |||||
| Pre-op | 1173.0 ± 39.9 | 1083.0 ± 90.8 | * | ||
| Post-op | 568.7 ± 35.5 | *** | 707.3 ± 64.4 | ** | |
| Energy intake (Kcal/d) | |||||
| Pre-op | 1564.5 ± 48.8 | 1557.3 ± 90.1 | ns | ||
| Post-op | 835.5 ± 44.3 | *** | 908.2 ± 61.0 | *** | |
| Carbohydrates (% energy intake) | |||||
| Pre-op | 46.1 ± 1.0 | 48.0 ± 1.2 | ns | ||
| Post-op | 44.0 ± 1.5 | ns | 47.7 ± 2.4 | ns | |
| Lipids (% energy intake) | |||||
| Pre-op | 34.0 ± 0.9 | 31.8 ± 1.3 | * | ||
| Post-op | 37.4 ± 3.1 | * | 32.6 ± 1.9 | ns | |
| Proteins (% energy intake) | |||||
| Pre-op | 20.0 ± 0.6 | 20.1 ± 0.7 | ns | ||
| Post-op | 18.8 + 0.6 | ns | 19.6 ± 1.0 | ns |
| VSG (n = 32) | RYGB (n = 12) | p | |
|---|---|---|---|
| Taste changes | |||
| Increased taste (% of patients) | 56 | 75 | ns |
| Intensity of change (1–10) | 6.4 ± 2.0 | 6.0 ± 1.1 | ns |
| Increased sweet taste (% of patients) | 78 | 75 | ns |
| Intensity of change (1–10) | 4.9 ± 3,1 | 6.9 ± 1.6 | 0.071 |
| Increased fat taste (% of patients) | 69 | 67 | ns |
| Intensity of change (1–10) | 6.4 ± 2.7 | 7.8 ± 1.8 | ns |
| Increased salt taste (% of patients) | 50 | 58 | ns |
| Intensity of change (1–10) | 5.6 ± 2.4 | 5.0 ± 2.4 | ns |
| Increased bitter taste (% of patients) | 3 | 25 | 0.056 |
| Intensity of change (1–10) | 6.0 ± 1.6 | 6.3 ± 1.2 | ns |
| Olfactory change (% of patients) | 50 | 33 | ns |
| Increased olfaction (% of patients) | 41 | 25 | ns |
| Intensity of change (1–10) | 5.7 ± 1.8 | 4.3 ± 1.2 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernard, A.; Le Beyec-Le Bihan, J.; Radoi, L.; Coupaye, M.; Sami, O.; Casanova, N.; Le May, C.; Collet, X.; Delaby, P.; Le Bourgot, C.; et al. Orosensory Perception of Fat/Sweet Stimuli and Appetite-Regulating Peptides before and after Sleeve Gastrectomy or Gastric Bypass in Adult Women with Obesity. Nutrients 2021, 13, 878. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030878
Bernard A, Le Beyec-Le Bihan J, Radoi L, Coupaye M, Sami O, Casanova N, Le May C, Collet X, Delaby P, Le Bourgot C, et al. Orosensory Perception of Fat/Sweet Stimuli and Appetite-Regulating Peptides before and after Sleeve Gastrectomy or Gastric Bypass in Adult Women with Obesity. Nutrients. 2021; 13(3):878. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030878
Chicago/Turabian StyleBernard, Arnaud, Johanne Le Beyec-Le Bihan, Loredana Radoi, Muriel Coupaye, Ouidad Sami, Nathalie Casanova, Cédric Le May, Xavier Collet, Pascaline Delaby, Cindy Le Bourgot, and et al. 2021. "Orosensory Perception of Fat/Sweet Stimuli and Appetite-Regulating Peptides before and after Sleeve Gastrectomy or Gastric Bypass in Adult Women with Obesity" Nutrients 13, no. 3: 878. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030878