
Consensus and Controversy in the Debate over the Biphasic Impact of Alcohol Consumption on the Cardiovascular System



Abstract
:1. Introduction
2. Background
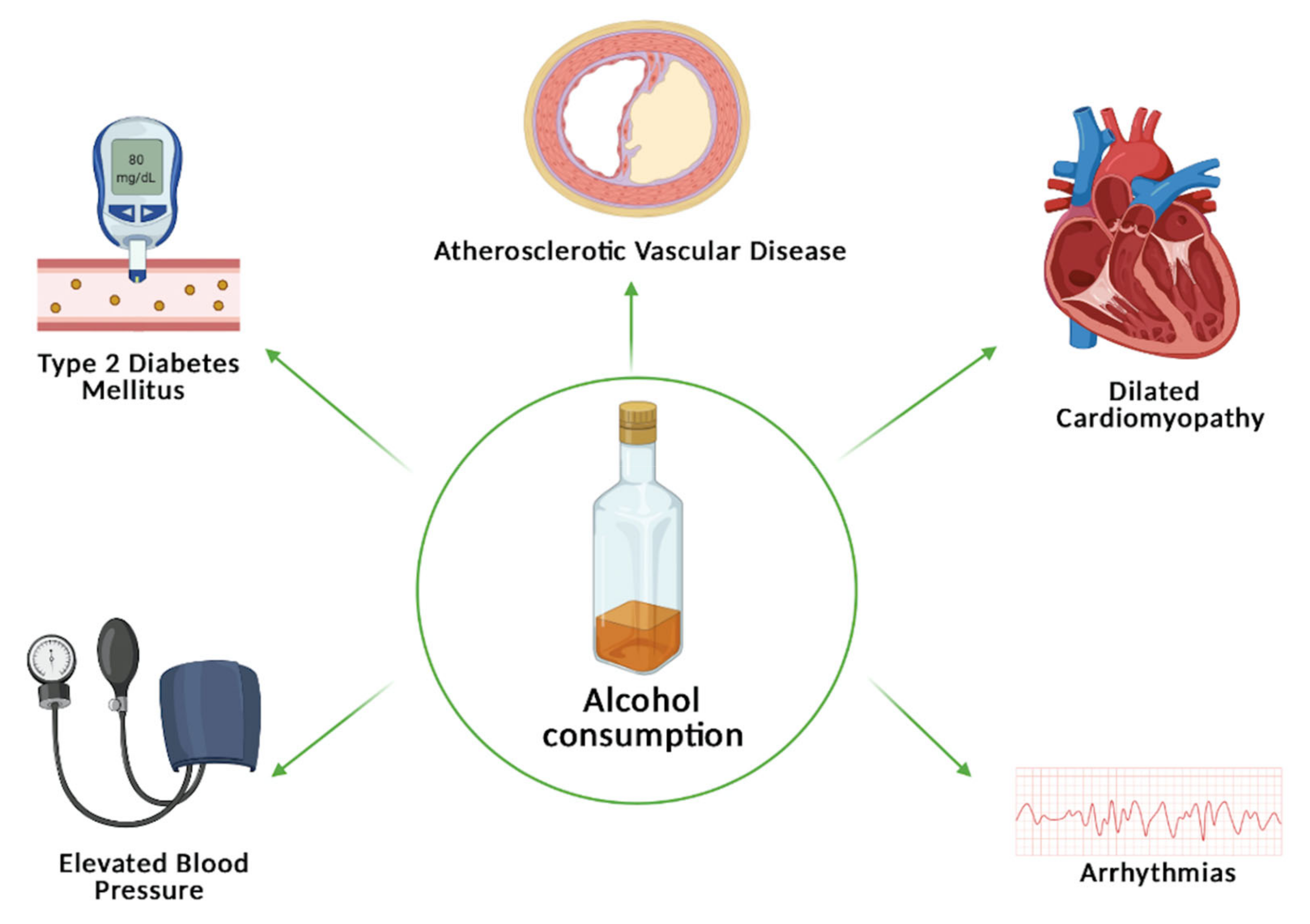
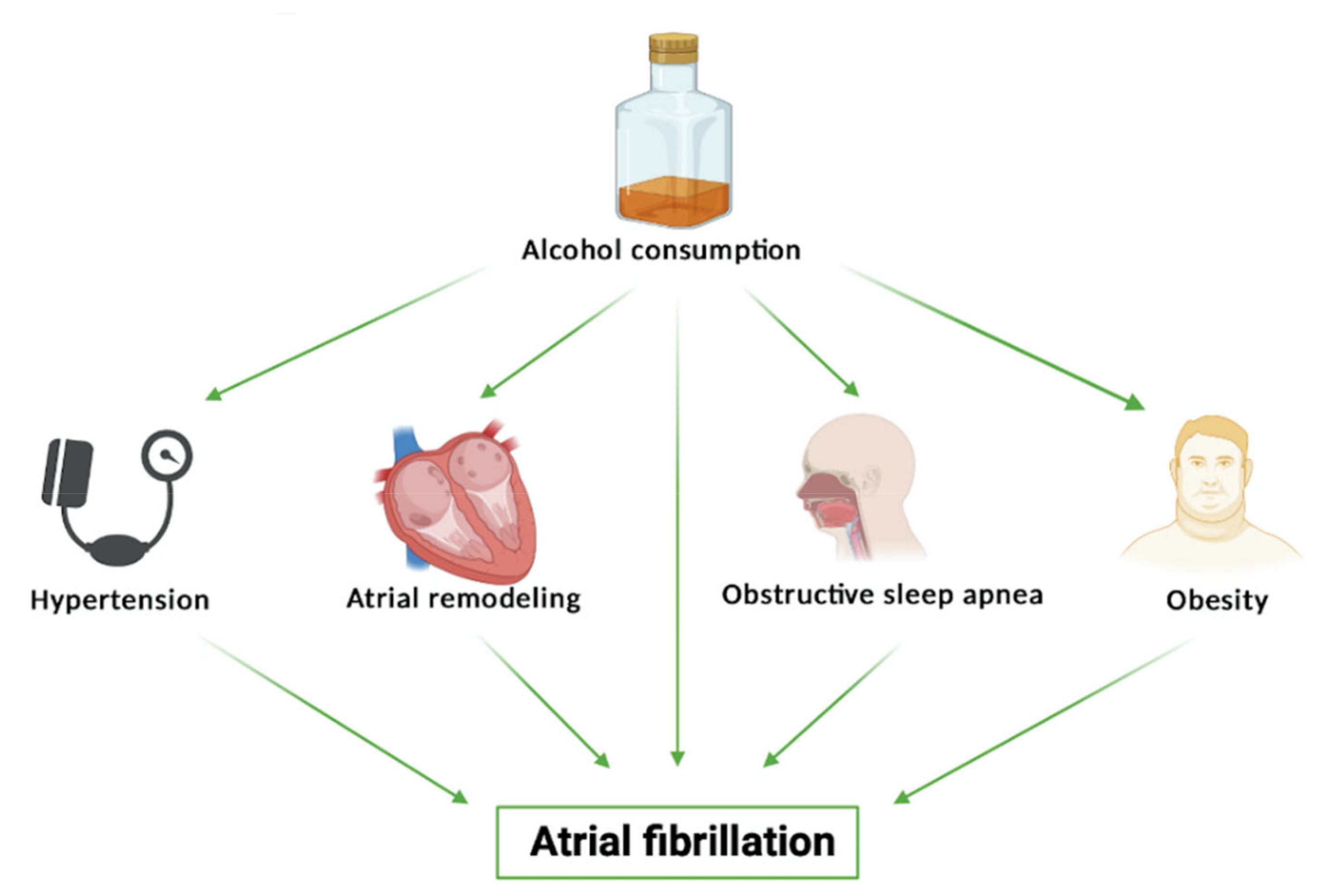
3. Alcohol-Related Arrhythmia
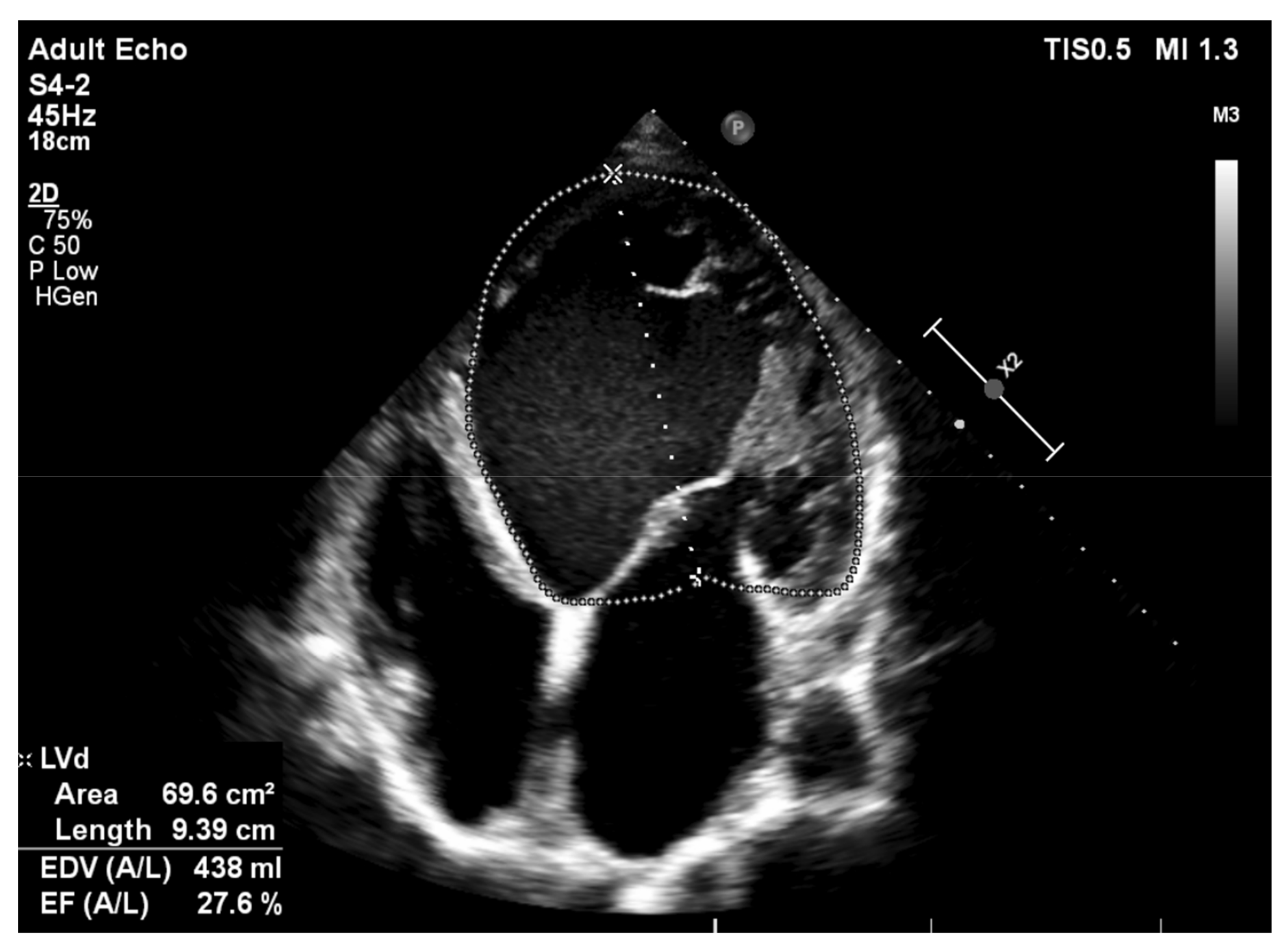
4. Alcoholic Cardiomyopathy
5. Alcohol Intake and Elevated Blood Pressure
6. Alcohol Consumption and Atherosclerotic Vascular Disease
7. Linkage of Alcohol Consumption with Type 2 Diabetes Mellitus—A Notorious Cardiovascular Risk Factor
8. Established Benefits of Dietary Interventions with Alcoholic Beverages
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeed, A.; Kampangkaew, J.; Nambi, V. Prevention of Cardiovascular Disease in Women. Methodist DeBakey Cardiovasc. J. 2017, 13, 185–192. [Google Scholar] [CrossRef]
- O’Keefe, E.L.; DiNicolantonio, J.J.; O’Keefe, J.H.; Lavie, C.J. Alcohol and CV Health: Jekyll and Hyde J-Curves. Prog. Cardiovasc. Dis. 2018, 61, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Chiva-Blanch, G.; Badimon, L. Benefits and Risks of Moderate Alcohol Consumption on Cardiovascular Disease: Current Findings and Controversies. Nutrients 2019, 12, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Castelnuovo, A.; Costanzo, S.; Bagnardi, V.; Donati, M.B.; Iacoviello, L.; de Gaetano, G. Alcohol dosing and total mortality in men and women: An updated meta-analysis of 34 prospective studies. Arch. Intern. Med. 2006, 166, 2437–2445. [Google Scholar] [CrossRef]
- Oppenheimer, G.M.; Bayer, R. Is Moderate Drinking Protective Against Heart Disease? The Science, Politics and History of a Public Health Conundrum. Milbank Q. 2020, 98, 39–56. [Google Scholar] [CrossRef] [PubMed]
- Spiegelman, D.; Lovato, L.C.; Khudyakov, P.; Wilkens, T.L.; Adebamowo, C.A.; Adebamowo, S.N.; Appel, L.J.; Beulens, J.W.; Coughlin, J.W.; Dragsted, L.O.; et al. The Moderate Alcohol and Cardiovascular Health Trial (MACH15): Design and methods for a randomized trial of moderate alcohol consumption and cardiometabolic risk. Eur. J. Prev. Cardiol. 2020, 27, 1967–1982. [Google Scholar] [CrossRef]
- Xi, B.; Veeranki, S.P.; Zhao, M.; Ma, C.; Yan, Y.; Mi, J. Relationship of Alcohol Consumption to All-Cause, Cardiovascular, and Cancer-Related Mortality in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 913–922. [Google Scholar] [CrossRef]
- Fernández-Solà, J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat. Rev. Cardiol. 2015, 12, 576–587. [Google Scholar] [CrossRef]
- Yan, J.; Thomson, J.K.; Zhao, W.; Gao, X.; Huang, F.; Chen, B.; Liang, Q.; Song, L.S.; Fill, M.; Ai, X. Role of Stress Kinase JNK in Binge Alcohol-Evoked Atrial Arrhythmia. J. Am. Coll. Cardiol. 2018, 71, 1459–1470. [Google Scholar] [CrossRef] [PubMed]
- Van de Luitgaarden, I.A.T.; Schrieks, I.C.; Kieneker, L.M.; Touw, D.J.; van Ballegooijen, A.J.; van Oort, S.; Grobbee, D.E.; Mukamal, K.J.; Kootstra-Ros, J.E.; Muller Kobold, A.C.; et al. Urinary Ethyl Glucuronide as Measure of Alcohol Consumption and Risk of Cardiovascular Disease: A Population-Based Cohort Study. J. Am. Heart Assoc. 2020, 9, e014324. [Google Scholar] [CrossRef]
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020, 395, 795–808. [Google Scholar] [CrossRef] [Green Version]
- Rosoff, D.B.; Davey Smith, G.; Mehta, N.; Clarke, T.K.; Lohoff, F.W. Evaluating the relationship between alcohol consumption, tobacco use, and cardiovascular disease: A multivariable Mendelian randomization study. PLoS Med. 2020, 17, e1003410. [Google Scholar] [CrossRef]
- Bell, S.; Daskalopoulou, M.; Rapsomaniki, E.; George, J.; Britton, A.; Bobak, M.; Casas, J.P.; Dale, C.E.; Denaxas, S.; Shah, A.D.; et al. Association between clinically recorded alcohol consumption and initial presentation of 12 cardiovascular diseases: Population based cohort study using linked health records. BMJ 2017, 356, j909. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C.L.; Hu, F.B.; Kawachi, I.; Williams, D.R.; Mukamal, K.J.; Rimm, E.B. Black-White differences in the relationship between alcohol drinking patterns and mortality among US men and women. Am. J. Public Health 2015, 105, S534–S543. [Google Scholar] [CrossRef]
- Schooling, C.M.; Sun, W.; Ho, S.Y.; Chan, W.M.; Tham, M.K.; Ho, K.S.; Leung, G.M.; Lam, T.H. Moderate alcohol use and mortality from ischaemic heart disease: A prospective study in older Chinese people. PLoS ONE 2008, 3, e2370. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Jankhotkaew, J.; Bundhamcharoen, K.; Suphanchaimat, R.; Waleewong, O.; Chaiyasong, S.; Markchang, K.; Wongworachate, C.; Vathesatogkit, P.; Sritara, P. Associations between alcohol consumption trajectory and deaths due to cancer, cardiovascular diseases and all-cause mortality: A 30-year follow-up cohort study in Thailand. BMJ Open 2020, 10, e038198. [Google Scholar] [CrossRef]
- Ettinger, P.O.; Wu, C.F.; De La Cruz, C., Jr.; Weisse, A.B.; Ahmed, S.S.; Regan, T.J. Arrhythmias and the "Holiday Heart": Alcohol-associated cardiac rhythm disorders. Am. Heart J. 1978, 95, 555–562. [Google Scholar] [CrossRef]
- Day, E.; Rudd, J.H.F. Alcohol use disorders and the heart. Addiction 2019, 114, 1670–1678. [Google Scholar] [CrossRef] [Green Version]
- Tonelo, D.; Providência, R.; Gonçalves, L. Holiday heart syndrome revisited after 34 years. Arq. Bras. Cardiol. 2013, 101, 183–189. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Prabhu, S.; Ling, L.H.; Kalman, J.M.; Kistler, P.M. Alcohol and Atrial Fibrillation: A Sobering Review. J. Am. Coll. Cardiol. 2016, 68, 2567–2576. [Google Scholar] [CrossRef] [PubMed]
- Lowenstein, S.R.; Gabow, P.A.; Cramer, J.; Oliva, P.B.; Ratner, K. The role of alcohol in new-onset atrial fibrillation. Arch. Intern. Med. 1983, 143, 1882–1885. [Google Scholar] [CrossRef] [PubMed]
- Hansson, A.; Madsen-Härdig, B.; Olsson, S.B. Arrhythmia-provoking factors and symptoms at the onset of paroxysmal atrial fibrillation: A study based on interviews with 100 patients seeking hospital assistance. BMC Cardiovasc. Disord. 2004, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, S.; Herbel, R.; Drobesch, C.; Peters, A.; Massberg, S.; Kääb, S.; Sinner, M.F. Alcohol consumption, sinus tachycardia, and cardiac arrhythmias at the Munich Octoberfest: Results from the Munich Beer Related Electrocardiogram Workup Study (MunichBREW). Eur. Heart J. 2017, 38, 2100–2106. [Google Scholar] [CrossRef] [Green Version]
- Csengeri, D.; Sprünker, N.A.; Di Castelnuovo, A.; Niiranen, T.; Vishram-Nielsen, J.K.; Costanzo, S.; Söderberg, S.; Jensen, S.M.; Vartiainen, E.; Donati, M.B.; et al. Alcohol consumption, cardiac biomarkers, and risk of atrial fibrillation and adverse outcomes. Eur. Heart J. 2021, 42, 1170–1177. [Google Scholar] [CrossRef]
- Kim, Y.G.; Han, K.D.; Choi, J.I.; Boo, K.Y.; Kim, D.Y.; Lee, K.N.; Shim, J.; Kim, J.S.; Kim, Y.H. Frequent drinking is a more important risk factor for new-onset atrial fibrillation than binge drinking: A nationwide population-based study. Europace 2020, 22, 216–224. [Google Scholar] [CrossRef]
- Kim, Y.G.; Han, K.D.; Choi, J.I.; Choi, Y.Y.; Choi, H.Y.; Boo, K.Y.; Kim, D.Y.; Lee, K.N.; Shim, J.; Kim, J.S.; et al. Non-genetic risk factors for atrial fibrillation are equally important in both young and old age: A nationwide population-based study. Eur. J. Prev. Cardiol. 2020, 10, 2047487320915664. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Kalman, J.M.; De Silva, A.; Nicholls, T.; Costello, B.; Nanayakkara, S.; Prabhu, S.; Stub, D.; Azzopardi, S.; Vizi, D.; et al. Alcohol Abstinence in Drinkers with Atrial Fibrillation. N. Engl. J. Med. 2020, 382, 20–28. [Google Scholar] [CrossRef]
- Hietanen, S.; Herajärvi, J.; Junttila, J.; Pakanen, L.; Huikuri, H.V.; Liisanantti, J. Characteristics of subjects with alcoholic cardiomyopathy and sudden cardiac death. Heart 2020, 106, 686–690. [Google Scholar] [CrossRef]
- Rossinen, J.; Sinisalo, J.; Partanen, J.; Nieminen, M.S.; Viitasalo, M. Effects of acute alcohol infusion on duration and dispersion of QT interval in male patients with coronary artery disease and in healthy controls. Clin. Cardiol. 1999, 22, 591–594. [Google Scholar] [CrossRef]
- Selb Semerl, J.; Selb, K. Coffee and alcohol consumption as triggering factors for sudden cardiac death: Case-crossover study. Croat. Med. J. 2004, 45, 775–780. [Google Scholar] [PubMed]
- Maisch, B. Alcoholic cardiomyopathy: The result of dosage and individual predisposition. Herz 2016, 41, 484–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Solà, J. The Effects of Ethanol on the Heart: Alcoholic Cardiomyopathy. Nutrients 2020, 12, 572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Nicolás, J.M.; Villegas, E.; Junqué, A.; Urbano-Márquez, A. Relationship between ethanol-related diseases and nutritional status in chronically alcoholic men. Alcohol Alcohol. 1993, 28, 543–550. [Google Scholar]
- Mirijello, A.; Tarli, C.; Vassallo, G.A.; Sestito, L.; Antonelli, M.; d’Angelo, C.; Ferrulli, A.; De Cosmo, S.; Gasbarrini, A.; Addolorato, G. Alcoholic cardiomyopathy: What is known and what is not known. Eur. J. Intern. Med. 2017, 43, 1–5. [Google Scholar] [CrossRef]
- Rehm, J.; Hasan, O.S.M.; Imtiaz, S.; Neufeld, M. Quantifying the contribution of alcohol to cardiomyopathy: A systematic review. Alcohol 2017, 61, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.S.; Amor-Salamanca, A.; Tayal, U.; Govind, R.; Serrano, I.; Salazar-Mendiguchía, J.; García-Pinilla, J.M.; Pascual-Figal, D.A.; Nuñez, J.; Guzzo-Merello, G.; et al. Genetic Etiology for Alcohol-Induced Cardiac Toxicity. J. Am. Coll. Cardiol. 2018, 71, 2293–2302. [Google Scholar] [CrossRef]
- Li, X.; Nie, Y.; Lian, H.; Hu, S. Histopathologic features of alcoholic cardiomyopathy compared with idiopathic dilated cardiomyopathy. Medicine 2018, 97, e12259. [Google Scholar] [CrossRef]
- Sulaiman, S.; Yousef, N.; Benjamin, M.M.; Sundararajan, S.; Wingert, R.; Wingert, M.; Mohammed, A.; Jahangir, A. Burden of arrhythmia and electrophysiologic procedures in alcoholic cardiomyopathy hospitalizations. Int. J. Cardiol. 2020, 304, 61–68. [Google Scholar] [CrossRef]
- Ram, P.; Lo, K.B.; Shah, M.; Patel, B.; Rangaswami, J.; Figueredo, V.M. National trends in hospitalizations and outcomes in patients with alcoholic cardiomyopathy. Clin. Cardiol. 2018, 41, 1423–1429. [Google Scholar] [CrossRef]
- Fang, W.; Luo, R.; Tang, Y.; Hua, W.; Fu, M.; Chen, W.; Lai, L.; Li, X. The Prognostic Factors of Alcoholic Cardiomyopathy: A single-center cohort study. Medicine 2018, 97, e11744. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.A.; Schiffrin, E.L.; White, W.B.; Mann, S.; Lindholm, L.H.; Kenerson, J.G.; Flack, J.M.; Carter, B.L.; Materson, B.J.; Ram, C.V.; et al. Clinical practice guidelines for the management of hypertension in the community: A statement by the American Society of Hypertension and the International Society of Hypertension. J. Clin. Hypertens 2014, 16, 14–26. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Zhao, F.; Liu, Q.; Li, Y.; Feng, X.; Chang, H.; Lyu, J. Association between alcohol consumption and hypertension in Chinese adults: Findings from the CHNS. Alcohol 2020, 83, 83–88. [Google Scholar] [CrossRef]
- Sterling, S.A.; Palzes, V.A.; Lu, Y.; Kline-Simon, A.H.; Parthasarathy, S.; Ross, T.; Elson, J.; Weisner, C.; Maxim, C.; Chi, F.W. Associations Between Medical Conditions and Alcohol Consumption Levels in an Adult Primary Care Population. JAMA Netw. Open 2020, 3, e204687. [Google Scholar] [CrossRef] [PubMed]
- Tasnim, S.; Tang, C.; Musini, V.M.; Wright, J.M. Effect of alcohol on blood pressure. Cochrane Database Syst. Rev. 2020, 7, Cd012787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roerecke, M.; Tobe, S.W.; Kaczorowski, J.; Bacon, S.L.; Vafaei, A.; Hasan, O.S.M.; Krishnan, R.J.; Raifu, A.O.; Rehm, J. Sex-Specific Associations Between Alcohol Consumption and Incidence of Hypertension: A Systematic Review and Meta-Analysis of Cohort Studies. J. Am. Heart Assoc. 2018, 7, e008202. [Google Scholar] [CrossRef] [Green Version]
- Jung, M.H.; Shin, E.S.; Ihm, S.H.; Jung, J.G.; Lee, H.Y.; Kim, C.H. The effect of alcohol dose on the development of hypertension in Asian and Western men: Systematic review and meta-analysis. Korean J. Intern. Med. 2020, 35, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Mayl, J.J.; German, C.A.; Bertoni, A.G.; Upadhya, B.; Bhave, P.D.; Yeboah, J.; Singleton, M.J. Association of Alcohol Intake With Hypertension in Type 2 Diabetes Mellitus: The ACCORD Trial. J. Am. Heart Assoc. 2020, 9, e017334. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Anderson, P.; Prieto, J.A.A.; Armstrong, I.; Aubin, H.J.; Bachmann, M.; Bastus, N.B.; Brotons, C.; Burton, R.; Cardoso, M.; et al. Towards new recommendations to reduce the burden of alcohol-induced hypertension in the European Union. BMC Med. 2017, 15, 173. [Google Scholar] [CrossRef] [Green Version]
- Hanschmidt, F.; Manthey, J.; Kraus, L.; Scafato, E.; Gual, A.; Grimm, C.; Rehm, J. Barriers to Alcohol Screening Among Hypertensive Patients and the Role of Stigma: Lessons for the Implementation of Screening and Brief Interventions in European Primary Care Settings. Alcohol Alcohol. 2017, 52, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Zaidi Touis, L.; Bolbrinker, J.; Riemer, T.G.; Kreutz, R. Moderation of alcohol consumption as a recommendation in European hypertension management guidelines: A survey on awareness, screening and implementation among European physicians. BMJ Open 2018, 8, e022026. [Google Scholar] [CrossRef] [Green Version]
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality From Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef]
- Van de Luitgaarden, I.A.T.; Schrieks, I.C.; De Bacquer, D.; van Oort, S.; Mirrakhimov, E.M.; Pogosova, N.; Davletov, K.; Dolzhenko, M.; van Ballegooijen, A.J.; Kotseva, K.; et al. Alcohol consumption patterns across Europe and adherence to the European guidelines in coronary patients: Findings from the ESC-EORP EUROASPIRE V survey. Atherosclerosis 2020, 313, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Bortnick, A.E.; Shahid, M.; Shitole, S.G.; Park, M.; Broder, A.; Rodriguez, C.J.; Scheuer, J.; Faillace, R.; Kizer, J.R. Outcomes of ST-elevation myocardial infarction by age and sex in a low-income urban community: The Montefiore STEMI Registry. Clin. Cardiol. 2020, 43, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Gaudel, P.; Kaunonen, M.; Neupane, S.; Joronen, K.; Koivisto, A.M.; Rantanen, A. Lifestyle-related risk factors among patients with coronary artery disease in Nepal. Scand. J. Caring Sci. 2020, 34, 782–791. [Google Scholar] [CrossRef]
- Ikehara, S.; Iso, H. Alcohol consumption and risks of hypertension and cardiovascular disease in Japanese men and women. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2020, 43, 477–481. [Google Scholar] [CrossRef]
- Ricci, C.; Wood, A.; Muller, D.; Gunter, M.J.; Agudo, A.; Boeing, H.; van der Schouw, Y.T.; Warnakula, S.; Saieva, C.; Spijkerman, A.; et al. Alcohol intake in relation to non-fatal and fatal coronary heart disease and stroke: EPIC-CVD case-cohort study. BMJ 2018, 361, k934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinkohl, F.; Barbieri, F.; Senoner, T.; Strobl, S.; Finkenstedt, A.; Plank, F.; Langer, C.; Beyer, C.; Birkl, K.; Widmann, G.; et al. Coronary atherosclerosis profile in patients with end-stage liver disease prior to liver transplantation due to alcoholic fatty liver: A coronary CTA study. Eur. Radiol. 2021, 31, 494–503. [Google Scholar] [CrossRef]
- Yang, X.; Gao, L.Y.; Qin, S.; Ma, K.H.; Luo, S.X.; Qin, C.C. Alcohol consumption may not affect the diameter of the coronary arteries in men with chest pain. J. Int. Med Res. 2020, 48, 300060520913781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noflatscher, M.; Schreinlechner, M.; Sommer, P.; Deutinger, P.; Theurl, M.; Kirchmair, R.; Bauer, A.; Marschang, P. Association of Food and Alcohol Consumption with Peripheral Atherosclerotic Plaque Volume as Measured by 3D-Ultrasound. Nutrients 2020, 12, 3711. [Google Scholar] [CrossRef]
- Yang, S.; Wang, S.; Yang, B.; Zheng, J.; Cai, Y.; Yang, Z. Alcohol Consumption Is a Risk Factor for Lower Extremity Arterial Disease in Chinese Patients with T2DM. J. Diabetes Res. 2017, 2017, 8756978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charakida, M.; Georgiopoulos, G.; Dangardt, F.; Chiesa, S.T.; Hughes, A.D.; Rapala, A.; Davey Smith, G.; Lawlor, D.; Finer, N.; Deanfield, J.E. Early vascular damage from smoking and alcohol in teenage years: The ALSPAC study. Eur. Heart J. 2019, 40, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Ying, Y.Y.; Li, S.X.; Wang, S.J.; Gong, Q.H.; Li, H. Association between alcohol consumption and metabolic syndrome among Chinese adults. Public Health Nutr. 2020, 10, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.; Neuenschwander, M.; Ballon, A.; Nöthlings, U.; Barbaresko, J. Adherence to healthy lifestyles and incidence of diabetes and mortality among individuals with diabetes: A systematic review and meta-analysis of prospective studies. J. Epidemiol. Community Health 2020, 74, 481–487. [Google Scholar] [CrossRef]
- Nyberg, S.T.; Singh-Manoux, A.; Pentti, J.; Madsen, I.E.H.; Sabia, S.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Goldberg, M.; et al. Association of Healthy Lifestyle With Years Lived Without Major Chronic Diseases. JAMA Intern. Med. 2020, 180, 760–768. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, A.M.; Jia, P.; Kim, H.Y.; Cuadros, D.F. Geographic Variation and Associated Covariates of Diabetes Prevalence in India. JAMA Netw. Open 2020, 3, e203865. [Google Scholar] [CrossRef]
- Baik, I.; Park, S.I. Associations of alcohol consumption and physical activity with lean type 2 diabetes mellitus among Korean adults: A prospective cohort study. PLoS ONE 2020, 15, e0238641. [Google Scholar] [CrossRef]
- Okamura, T.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. Effect of alcohol consumption and the presence of fatty liver on the risk for incident type 2 diabetes: A population-based longitudinal study. BMJ Open Diabetes Res. Care 2020, 8, e001629. [Google Scholar] [CrossRef] [PubMed]
- Blomdahl, J.; Nasr, P.; Ekstedt, M.; Kechagias, S. Moderate alcohol consumption is associated with advanced fibrosis in non-alcoholic fatty liver disease and shows a synergistic effect with type 2 diabetes mellitus. Metab. Clin. Exp. 2021, 115, 154439. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.C.; Wu, S.Y.; Leung, P.S. Alcohol ingestion induces pancreatic islet dysfunction and apoptosis via mediation of FGF21 resistance. Ann. Transl. Med. 2020, 8, 310. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lv, J.; Yu, C.; Guo, Y.; Bian, Z.; Fan, J.; Yang, L.; Chen, Y.; Du, H.; Long, H.; et al. The Association Between Age at Initiation of Alcohol Consumption and Type 2 Diabetes Mellitus: A Cohort Study of 0.5 Million Persons in China. Am. J. Epidemiol. 2020, 189, 1478–1491. [Google Scholar] [CrossRef] [PubMed]
- Keys, A.; Menotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Renaud, S.; de Lorgeril, M. Wine, alcohol, platelets, and the French paradox for coronary heart disease. Lancet 1992, 339, 1523–1526. [Google Scholar] [CrossRef]
- Ditano-Vázquez, P.; Torres-Peña, J.D.; Galeano-Valle, F.; Pérez-Caballero, A.I.; Demelo-Rodríguez, P.; Lopez-Miranda, J.; Katsiki, N.; Delgado-Lista, J.; Alvarez-Sala-Walther, L.A. The Fluid Aspect of the Mediterranean Diet in the Prevention and Management of Cardiovascular Disease and Diabetes: The Role of Polyphenol Content in Moderate Consumption of Wine and Olive Oil. Nutrients 2019, 11, 2833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagetta, D.; Maruca, A.; Lupia, A.; Mesiti, F.; Catalano, R.; Romeo, I.; Moraca, F.; Ambrosio, F.A.; Costa, G.; Artese, A.; et al. Mediterranean products as promising source of multi-target agents in the treatment of metabolic syndrome. Eur. J. Med. Chem. 2020, 186, 111903. [Google Scholar] [CrossRef]
- Stephan, L.S.; Almeida, E.D.; Markoski, M.M.; Garavaglia, J.; Marcadenti, A. Red Wine, Resveratrol and Atrial Fibrillation. Nutrients 2017, 9, 1190. [Google Scholar] [CrossRef] [Green Version]
- Gepner, Y.; Golan, R.; Harman-Boehm, I.; Henkin, Y.; Schwarzfuchs, D.; Shelef, I.; Durst, R.; Kovsan, J.; Bolotin, A.; Leitersdorf, E.; et al. Effects of Initiating Moderate Alcohol Intake on Cardiometabolic Risk in Adults With Type 2 Diabetes: A 2-Year Randomized, Controlled Trial. Ann. Intern. Med. 2015, 163, 569–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osorio-Paz, I.; Brunauer, R.; Alavez, S. Beer and its non-alcoholic compounds in health and disease. Crit. Rev. Food Sci. Nutr. 2020, 60, 3492–3505. [Google Scholar] [CrossRef] [PubMed]
- Wotherspoon, A.; Elshahat, S.; McAlinden, N.; Dean, K.; Young, I.S.; Sharpe, P.C.; Blankenburg, S.; Patterson, C.C.; McKinley, M.C.; Evans, A.; et al. Effect of Moderate Red Wine versus Vodka Consumption on Inflammatory Markers Related to Cardiovascular Disease Risk: A Randomized Crossover Study. J. Am. Coll. Nutr. 2020, 39, 495–500. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cardiovascular Disease or Risk Factor | High Alcohol Consumption | Low to Moderate Doses of Ethanol |
|---|---|---|
| Arrhythmias |
|
|
| ||
| Dilated Cardiomyopathy |
|
|
| Hypertension |
|
|
| Atherosclerotic Vascular Disease |
|
|
| Diabetes mellitus |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stătescu, C.; Clement, A.; Șerban, I.-L.; Sascău, R. Consensus and Controversy in the Debate over the Biphasic Impact of Alcohol Consumption on the Cardiovascular System. Nutrients 2021, 13, 1076. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041076
Stătescu C, Clement A, Șerban I-L, Sascău R. Consensus and Controversy in the Debate over the Biphasic Impact of Alcohol Consumption on the Cardiovascular System. Nutrients. 2021; 13(4):1076. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041076
Chicago/Turabian StyleStătescu, Cristian, Alexandra Clement, Ionela-Lăcrămioara Șerban, and Radu Sascău. 2021. "Consensus and Controversy in the Debate over the Biphasic Impact of Alcohol Consumption on the Cardiovascular System" Nutrients 13, no. 4: 1076. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041076