1. Introduction
Gestational diabetes, a common complication of pregnancy, is associated with short-term and long-term health implications for the baby [
1,
2]. Infants are commonly large-for-gestational-age at birth (LGA; >90th centile) and have a higher risk of obesity in childhood [
2,
3]. Unfortunately, very few interventions are available with proven efficacy to reduce the likelihood of childhood obesity in these high-risk children. The early development of obesity in children with existing environmental and genetic susceptibilities to type 2 diabetes is a major public health concern [
4].
Events in pregnancy, perinatal and early postnatal periods may be important for future childhood obesity, but are relatively understudied, particularly in specific high-risk populations [
5]. Babies born to mothers with gestational diabetes often have multiple risk factors for childhood obesity, which appear to have an additive effect upon risk. Maternal obesity in pregnancy [
6,
7], maternal excessive gestational weight gain [
6], maternal postnatal weight retention [
6], exposure to hyperglycaemia in utero [
8,
9,
10], perinatal complications such as large-for-gestational age at birth [
9,
11,
12], infant formula feeding [
13] and increased growth trajectory in early life [
14] are all established risk factors for childhood obesity or adiposity and are common features of a pregnancy affected by gestational diabetes.
It is therefore possible that an intervention which addresses maternal weight in pregnancy may reduce obesity rates in offspring. Family interventions (which target at least one parent to improve obesity rates in children) are already well-established in the prevention of childhood obesity [
5]. However, many interventions to reduce the risk of childhood obesity target older children (2–10 years) and may miss the opportunity to intervene in early years [
5,
15]. The DiGest study, a currently ongoing dietary intervention in pregnant diagnosed with gestational diabetes, provides the opportunity to study the influence of a pregnancy weight intervention upon risk factors for childhood obesity in early life [
16].
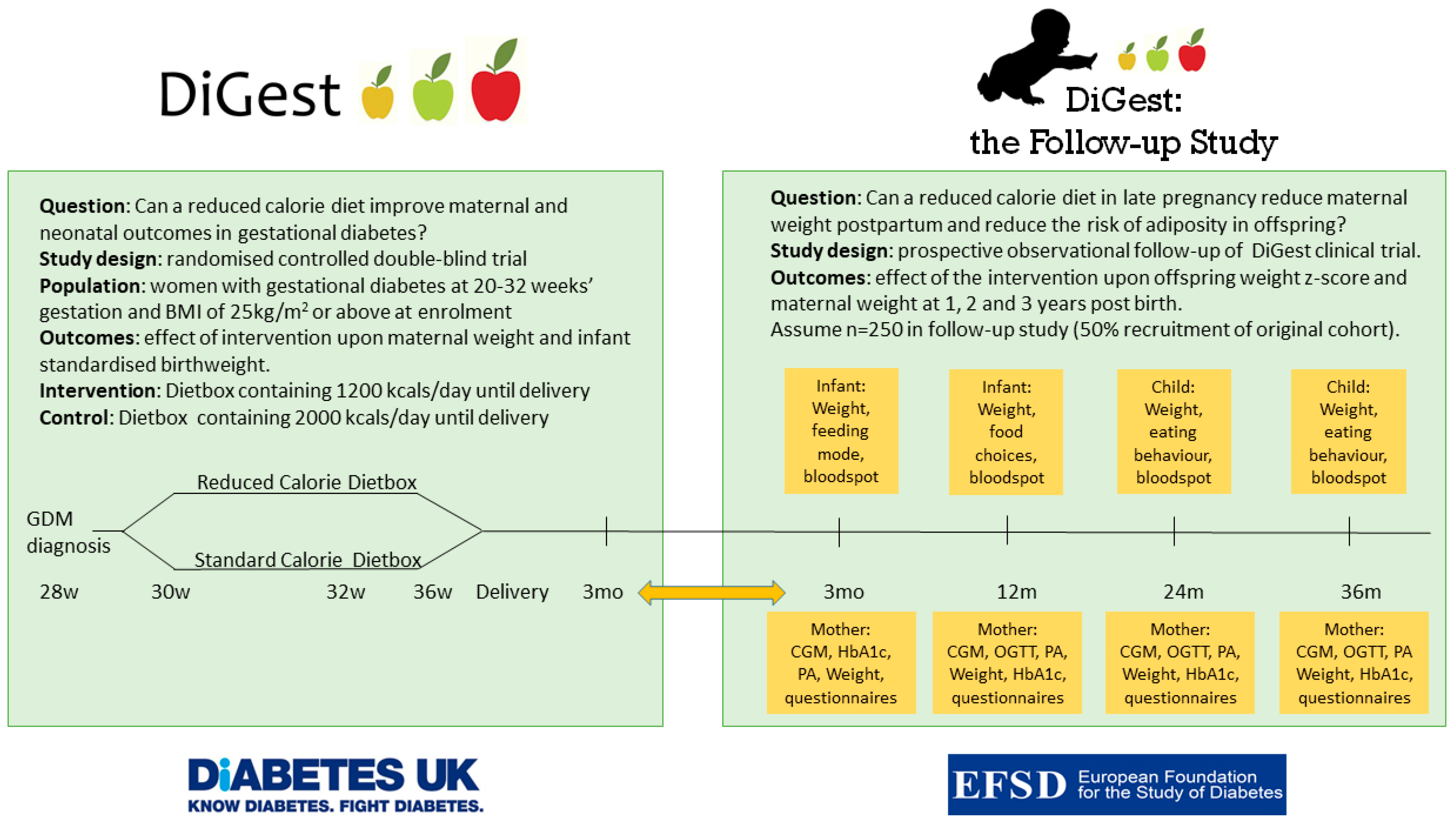
The DiGest Study is a randomised, double-blind controlled trial of a reduced calorie diet using a novel dietary intervention to assess the benefits of controlling maternal weight gain in late pregnancy in gestational diabetes. The trial is described in detail elsewhere [
16]. Briefly, women are randomised to receive a weekly dietbox containing all meals and snacks and are blinded to the overall calorie content (1200 kcal/day for intervention group and 2000 kcal/day for control group; 40% carbohydrate, 25% protein, 35% fat). The dietbox commences at enrolment, typically 28–32 weeks’ gestation, and continues until delivery of the infant. The clinical care team and research team are also blinded to calorie allocation. Dietboxes are nutritionally balanced and low in glycaemic index, low in saturated fat, high in vegetables and protein and suitable for use in pregnancy. Data will be collected to assess the impact upon maternal weight gain, infant birthweight and a range of obstetric and glycaemic outcomes during late pregnancy up to 3 months postnatally [
16]. The design of the DiGest trial provides the opportunity for a controlled and blinded dietary study and reduces potential bias due to differences in maternal educational level, cooking ability, income and kitchen facilities.
In this manuscript we describe a follow up study to the DiGest trial which investigates the effect of the reduced calorie dietary intervention in pregnant women upon the development of obesity in a high-risk population of children from birth to 3 years of age. The hypothesis is that a reduced calorie diet in late pregnancy in women with gestational diabetes reduces offspring adiposity and improves maternal weight at 1, 2 and 3 years postpartum.
2. Materials and Methods
Study design and ethical approval: The DiGest Follow up study is an observational study on the effects of a multicentre, prospective, randomised double-blind controlled dietary intervention trial conducted in late pregnancy. In summary, participants of the follow up study will have been exposed to either the intervention diet of 1200 kcal/day, or the control diet of 2000 kcal/day as part of the DiGest study. Macronutrient ratios were identical for each diet; 40% carbohydrate, 25% protein, 35% fat. Meals were prepared from the same recipes, with a factor of 1.667 used to convert portion size to obtain meals of two different sizes. This diet it provided from enrolment (typically 28–32 weeks’ gestation) to delivery of the infant. Participants will have attended 4 study visits in total to provide blood samples, blood pressure, body weight and anthropometry measurements, and to complete a series of questionnaires. Randomisation for the original DiGest study was stratified for centre. Throughout the DiGest intervention and Follow-up study, both mothers and children will receive standard NHS care, as described in the NICE guidelines [
17]. The study is being conducted in accordance with the Declaration of Helsinki, and the protocol has been submitted to the Research Ethics Committee (UK Bloomsbury REC 21/PR/0213) and the NHS Health Research Authority (IRAS 281062).
Recruitment: The DiGest trial recruitment occurs at 5 hospital trusts in East Anglia, UK. The same study sites will be used for the follow-up study. At 3 months postpartum, DiGest trial participants will be given information about the follow-up study and invited to participate by the research midwives, nurses, clinical research staff or by their physician/obstetrician. For training purposes, students in healthcare disciplines (e.g., medicine, biomedical science, nursing, midwifery) may also occasionally recruit patients under appropriate supervision. Informed consent will be obtained at the final visit of the DiGest dietary intervention, with the mothers providing consent on their infant’s behalf. Participants (or mother-infant dyad) can withdraw from the study at any time without reason without affecting their clinical care. There is no financial incentive for this study, but a small token of appreciation is provided for the child at each visit in line with guidelines of the Royal College of Paediatrics and Child Health [
18].
Eligibility criteria: All women from the DiGest cohort (confirmed gestational diabetes and BMI 25 kg/m2 or above at enrolment) are eligible to enrol in the follow-up study, however, they must be recruited within 12 months of the baby’s birth. Mothers would be excluded if they are unwilling or unable to provide informed consent, if they experienced stillbirth, neonatal death or had an infant born with severe congenital anomaly.
Follow-up visit structure: The study timeline is outlined in
Figure 1. Study visits will be carried out in the participants’ home, local hospital or at another place convenient for the participant. The initial follow-up visit will coincide with the final DiGest visit at 3 months after the birth, where the consent form will be signed for both the mother and infant. Maternal and infant anthropometry will be measured at this visit as part of the DiGest study. Further Follow-up visits will take place at 1, 2 and 3 years postnatally and will take approximately 45 min.
Anthropometry Measurements: At all visits, maternal height and weight will be measured using a routinely calibrated stadiometer and weight scale (Seca Hammer Steindamm, Birmingham, U.K.). Waist and hip circumference will be measured to the nearest 0.1 cm with a fibreglass tape, in accordance with the World Health Organisation criteria [
19]. Waist circumference is located at the midpoint between the lowest palpable rib and the iliac crest. Hip circumference is measured at the greater trochanters, or at the widest extension of the buttocks. Other maternal anthropometry that will be measured include mid upper arm circumference and skinfold thickness, using Harpenden calipers recorded to the nearest 0.2 mm. Infant length and weight will be taken in a supine position, measured to the nearest 0.1 cm using fibreglass tape, and 0.01 kg using scales (SECA 757 Infant digital scale, Seca, Birmingham, UK). Infant abdominal circumference, head circumference, skinfold thickness (Holtain calipers, Crosswell, Wales, U.K.), mid upper arm circumference will also be measured by trained research staff according to methods described elsewhere [
16]. All equipment used to measure anthropometry are routinely calibrated.
Maternal Glucose Assessment: Due to the COVID-19 pandemic, a home-based OGTT using continuous glucose monitoring (CGM) will replace the gold standard OGTT for assessment of maternal glucose tolerance postnatally. An HbA1c will also be performed to replace mothers’ annual diabetes check in primary care. We have previously assessed the feasibility and efficacy of the home-based OGTT with good results (Kusinski et al., submitted to press). In brief, a Dexcom G6 CGM sensor is sited during the study visit with a masked receiver so participants do not see their glucose results in real time. On day 3, participants are asked to eat normally, and fast overnight for at least 10 h. On the morning of day 4, at 09.00, participants are asked to drink a sachet of Rapilose (Galen, Craigavon, UK) containing 75 g of anhydrous glucose. Participants can have sips of water but are asked to consume no other foods or drinks for 3 h after the test. The timing of the home OGTT is chosen to coincide with peak sensor accuracy. Glucose readings are taken automatically every 5 min and transmit to the CGM receiver. Results from the OGTT at 0, 1 and 2 h are included in the analysis. Other CGM metrics will also be used to assess glycaemia as described in a recent CGM consensus statement. CGM metrics will be reported using both adult non-pregnant and pregnant ranges to allow comparison with pregnancy data gathered in the DiGest trial (also using a Dexcom G6 system).
Physical Activity Assessment
Participants will be asked to wear a wrist-worn accelerometer continuously for 7 days concurrently with the CGM. The triaxial accelerometer is waterproof and does not have a visual display, nor any auditory or vibrational cues, which means that participants will not be able to influence their activity level based on what is recorded by the device and nor will they be prompted to move about during periods of inactivity. These accelerometers have been used in in women during and after pregnancy to assess their daily physical activity with high compliance and produce reliable estimates of energy expenditure, overall physical activity and moderate-vigorous intensity activity [
20,
21,
22]. Accelerometry data at 100 Hz will be collected and downloaded from the monitors for analysis. At the end of the recording period, mothers will be asked to complete the Recent Physical Activity Questionnaire (RPAQ), a self-completion questionnaire designed to assess an individual’s physical activity over the previous four weeks. The questionnaire contains questions about physical activity in four domains: at home, at work, commuting and during leisure time. RPAQ has been validated against doubly labelled water and individually calibrated heart rate and movement sensing to assess physical activity energy expenditure (PAEE) in adults [
23,
24]. It has been used in diabetes prevention trials [
25] and in longitudinal studies of pregnant women [
26].
Other Biochemistry samples: A blood spot sample will be taken from mothers and frozen at −80 °C for future batch analysis of C-peptide and metabolomics. An optional heelprick blood spot will also be taken from infants, for future batch analysis of C-peptide and metabolomics. If a genetic sample has not been taken already as part of the DiGest trial, a cheek swab will be taken from both mothers and infants. Mothers will be asked to provide a sample of milk (formula or breast) which will be collected onto filter paper for assessment of infant nutrition including lipidomic profiling. To protect participant’s privacy, this can be performed after the visit.
Questionnaires: Mothers will be asked to complete validated questionnaires about quality of life (EuroQuol EQ5D), eating behaviour (three factor eating questionnaire—TFEQ-18) [
27], physical activity (RPAQ) [
24] and web-based multiple pass 24 h dietary recalls to assess habitual dietary intake (Intake24; [
28,
29]). These questionnaires have been used during the DiGest trial and participants will be familiar with them. In addition, mothers will be asked to complete questionnaires about parental feeding style (PFSQ) and their baby or child’s eating behaviour (CEBQ) [
30,
31,
32,
33]. Information will be collected about infant feeding choice and if relevant, duration of breastfeeding.
3. Results
The aim of the study is to investigate the effects of a reduced calorie diet in late pregnancy in women diagnosed with gestational diabetes upon longer-term maternal and offspring metabolic outcomes. The primary outcome for child health is standardised weight at 1, 2 and 3 years of age. The primary outcome for the maternal population is maternal weight at 1, 2 and 3 years postpartum.
Offspring secondary outcomes at 1, 2 and 3 years of age: There are multiple secondary outcomes for children including weight, BMI, growth trajectory, and blood spot biomarkers such as C-peptide or metabolomics at 1, 2 and 3 years. Questionnaire data will be assessed to identify effects of the intervention in pregnancy upon child eating behaviour, with assessment for confounding factors including maternal BMI, maternal eating behaviour and parental feeding style.
Maternal secondary outcomes at 1, 2 and 3 years postpartum: Maternal outcomes to be studied include maternal weight and weight change, BMI, anthropometry measures of adiposity, glycaemia (CGM metrics, HbA1c, OGTT results, indices of insulin production and sensitivity, including HOMA-IR and HOMA-B, Matsuda score and Stumvoll index [
34,
35], cardiometabolic health (blood pressure, heart rate, lipids, fasting insulin, fasting glucose), maternal food intake, food nutritional content and quality, eating behaviour, quality of life, and incidence of type 2 diabetes or gestational diabetes in a future pregnancy.
Analysis Plan: An intention to treat analysis of the primary outcome for child health (standardised weight at 1, 2 and 3 years of age) will be based on linear regression with adjustment for the stratification variable of study centre through a fixed effects model. The potential role of other explanatory variables such as pre-pregnancy BMI, infant nutrition, infant postnatal growth trajectory or information from the questionnaires will be investigated. A per protocol analysis will also be performed in participants with >80% compliance and at least 4 weeks’ exposure to the intervention. Secondary outcomes will also be examined through regression analyses (linear or logistic) appropriate for the type of outcome being considered.
Power calculation: All eligible women and their infants will be invited to join the follow-up study. However, calculations are based on assuming a 50% recruitment rate (
n = 250 women and their infants) and a 20% withdrawal rate. For the maternal primary endpoint, data from earlier work suggest that typical values for maternal BMI outside of pregnancy in women with a history of gestational diabetes is mean 28.7 kg/m
2 (SD 7.1;
n = 416) and maternal postpartum HbA1c 37.5 mmol/mol (SD 7.5;
n = 157) [
36]. Using these figures, recruitment of 250 women, will give 90% power to identify a 3 kg/m
2 difference in BMI (e.g., 29 vs. 32 kg/m
2) and a 3 mmol/mol difference in HbA1c postnatally while allowing for a 10–20% withdrawal rate. At 80% power, this sample size is sufficient to identify a 2 kg/m
2 difference in BMI (e.g., 30 vs. 32 kg/m
2) and a 2 mmol/mol difference in HbA1c postnatally.
For the offspring primary endpoint, assessment of infant weight will be based upon z-(SD) scores. At the sample size of 250 infants, there will be 90% power to identify a 0.45 SD increase in weight with 80% power to identify 0.4 SD increase in weight. At the age of 2 years old, a z-score of 0.4 is equivalent to 0.5 kg.
4. Discussion
This follow-up study of the DiGest randomised controlled trial provides a unique opportunity to assess the potential benefits of a dietary intervention in late pregnancy upon the development of obesity in children with multiple risk factors. The availability of data from mid pregnancy until the age of 3 years also allows detailed characterisation of the relative importance of pregnancy and postnatal risk factors in the development of adiposity in early childhood.
Rates of maternal obesity are increasing in the antenatal population throughout the world, and pre-pregnancy BMI is a strong predictor of both birthweight and future childhood obesity. A recent metanalysis identified that maternal obesity was significantly associated with overweight/obesity in early, mid and late childhood with odds ratios 2.43, 3.12 and 4.47, respectively [
6]. Weight gain in pregnancy is also important and has repercussions for women’s BMI for 15 years or more after the pregnancy [
37]. Landon and colleagues found that gestational weight gain was strongly related to obesity in children aged 5–10 years old [
10].
In addition to the effects of maternal obesity, exposure to intrauterine hyperglycaemia appears to further increase the risk of childhood obesity. There is evidence that maternal glycaemia in gestational diabetes is associated with childhood obesity at 10–14 years [
2] and altered anthropometry at 5–10 years, favouring obesity [
10]. Maternal hyperglycaemia can also indirectly increase childhood obesity rates, by increasing the risk of LGA in offspring. Data from the UK and Canada suggest that childhood obesity rates in LGA infants are at least twice that of children born appropriate for gestational age [
11,
38]. The exact mechanisms behind these intrauterine exposures and later life obesity are unclear. It is possible that altered placental secretary function, offspring hyperinsulinism and genetic susceptibilities all play a role.
The design of the DiGest and DiGest follow-up studies also allows longitudinal assessment of the effects of other pregnancy exposures upon longer-term offspring growth and health. For example, metformin use in pregnancy has been associated with lower birth weight but increased postnatal catch-up growth, but the consequences of this upon longer-term offspring cardiometabolic outcomes remain less clear [
39,
40]. The collection of anthropometric measures in offspring exposed to metformin in utero with paired blood samples, and a comparable unexposed control group, provides opportunity to explore this issue in greater depth.
Serum and cord blood stored for biomarkers such as leptin, adiponectin and placental hormones provides opportunities to identify infants at an earlier stage who are at risk of obesity in childhood. Previous work has demonstrated that cord blood leptin levels are associated with pregnancy diet, physical activity and neonatal body composition in a comparable population [
41,
42]. Cord blood adiponectin has also been associated with body composition effects which may be distinct in male and female neonates [
43] and may additionally provide information about neonatal beta cell function [
44]. Placental growth factors and metabolic function have also shown relevance for pregnancy outcomes [
45,
46]. Taken together, it is feasible that biomarkers in cord blood or maternal serum may facilitate early identification of offspring at risk of obesity and diabetes in later life, who could be prioritized for health interventions.
Although maternal physical activity levels in pregnancy and postpartum are likely to be vital for determining offspring habitual exercise levels, relatively few modifiable factors have been identified in children’s physical activity levels in the very young [
47,
48]. Findings to date suggest that parents’ physical activity levels are associated with children’s activity levels in pre-school aged children and role-modelling by mothers appears to be one of the strongest associations [
48]. However, relatively few studies have examined exercise after gestational diabetes in mothers and children. The DiGest Follow-Up study uses both questionnaires and accelerometers to assess physical activity, information which could inform future interventional studies.
Infant feeding and growth trajectory in the first year of life are also important. Although randomised studies of feeding modality in early life are not possible, observational analyses in unselected populations suggest consistent benefits of breastfeeding upon rates of childhood obesity [
49,
50]. There is also evidence that breastfeeding reduces childhood obesity risk in offspring of mothers with gestational diabetes and obesity [
13,
51]. Stettler and colleagues reported that similar benefits may persist until adulthood in a study of offspring to age 20 years [
52]. The study also includes questionnaires about child eating behaviour, child food preferences and parental feeding style to examine behavioural associations with obesity and feeding behaviour in children aged up to 3 years.
The aetiology of childhood obesity is therefore complex and multifactorial. In infants of mothers with gestational diabetes, multiple risk factors are often evident at birth. Successful interventions are urgently needed to reduce the risk of obesity and future metabolic disease in these high-risk children.
5. Conclusions
The DiGest follow-up study provides the opportunity to assess pregnancy and postnatal risk factors for the development of childhood obesity, and to describe the potential impact of a dietary intervention in pregnancy. Early intervention in offspring with existing environmental and genetic susceptibilities to type 2 diabetes will be vital to break the intergenerational cycle of obesity.
6. Patents
No patents are relevant to the study described in this manuscript.
Author Contributions
C.L.M. designed the study, developed the methodology and wrote and revised the manuscript. C.L.M. acquired funding for the study and has overall responsibility for study conduct. D.J. contributed to writing the manuscript and read and revised the final manuscript. E.D.L.R., K.L.R., L.M.O.G., L.C.K., S.B., D.J.H., K.K.O. and K.B. contributed to aspects of study design, and read and revised the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This paper presents a study protocol for a follow-up study which was funded by the European Foundation for the Study of Diabetes and Novo Nordisk Foundation through the Future Leaders’ Award (NNF19SA058974). The DiGest trial is funded by Diabetes UK (17/0005712).
Institutional Review Board Statement
The study will be conducted according to the guidelines of the Declaration of Helsinki, and is under review by the Bloomsbury Research Ethics Committee (protocol v.1; REC 21/PR/0213 and date 3/3/2021).
Informed Consent Statement
Informed consent will be obtained from all subjects involved in the study. Consent for infants was given by parents.
Data Availability Statement
No applicable.
Acknowledgments
We thank the National Institute of Health Research (NIHR) Clinical Research Network (CRN Eastern) for supporting research personnel at study sites who are involved in performing this research study. We are grateful to funding to E.D.L.R., K.R. and L.O.G., who are supported by the NIHR Cambridge Biomedical Research Centre (IS-BRC-1215-20014). Thank you also to Søren Brage for constructive comments and input to the physical activity aspects to the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Metzger, B.E.; Coustan, D.R. Summary and recommendations of the Fourth International Workshop-Conference on Gestational Diabetes Mellitus. The Organizing Committee. Diabetes Care 1998, 21 (Suppl. 2), B161–167. [Google Scholar]
- Lowe, W.L., Jr.; Lowe, L.P.; Kuang, A.; Catalano, P.M.; Nodzenski, M.; Talbot, O.; Tam, W.H.; Sacks, D.A.; McCance, D.; Linder, B.; et al. Maternal glucose levels during pregnancy and childhood adiposity in the Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study. Diabetologia 2019, 62, 598–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; McIntyre, H.D.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake-Lamb, T.L.; Locks, L.M.; Perkins, M.E.; Woo Baidal, J.A.; Cheng, E.R.; Taveras, E.M. Interventions for Childhood Obesity in the First 1000 Days A Systematic Review. Am. J. Prev. Med. 2016, 50, 780–789. [Google Scholar] [CrossRef] [Green Version]
- Ash, T.; Agaronov, A.; Young, T.; Aftosmes-Tobio, A.; Davison, K.K. Family-based childhood obesity prevention interventions: A systematic review and quantitative content analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 113. [Google Scholar] [CrossRef]
- Voerman, E.; Santos, S.; Patro Golab, B.; Amiano, P.; Ballester, F.; Barros, H.; Bergstrom, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: An individual participant data meta-analysis. PLoS Med. 2019, 16, e1002744. [Google Scholar] [CrossRef]
- Litwin, L.; Sundholm, J.K.M.; Rönö, K.; Koivusalo, S.B.; Eriksson, J.G.; Sarkola, T. Transgenerational effects of maternal obesity and gestational diabetes on offspring body composition and left ventricle mass: The Finnish Gestational Diabetes Prevention Study (RADIEL) 6-year follow-up. Diabet Med. 2020, 37, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Lu, J.; Li, W.; Liu, H.; Wang, L.; Leng, J.; Zhang, S.; Wang, S.; Tuomilehto, J.; Yu, Z.; et al. Joint Associations of Maternal Gestational Diabetes and Hypertensive Disorders of Pregnancy With Overweight in Offspring. Front. Endocrinol. 2019, 10, 645. [Google Scholar] [CrossRef]
- Hammoud, N.M.; Visser, G.H.A.; van Rossem, L.; Biesma, D.H.; Wit, J.M.; de Valk, H.W. Long-term BMI and growth profiles in offspring of women with gestational diabetes. Diabetologia 2018, 61, 1037–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landon, M.B.; Mele, L.; Varner, M.W.; Casey, B.M.; Reddy, U.M.; Wapner, R.J.; Rouse, D.J.; Tita, A.T.N.; Thorp, J.M.; Chien, E.K.; et al. The relationship of maternal glycemia to childhood obesity and metabolic dysfunction(double dagger). J. Matern. Fetal Neonatal Med. 2018. [Google Scholar] [CrossRef]
- Kaul, P.; Bowker, S.L.; Savu, A.; Yeung, R.O.; Donovan, L.E.; Ryan, E.A. Association between maternal diabetes, being large for gestational age and breast-feeding on being overweight or obese in childhood. Diabetologia 2019, 62, 249–258. [Google Scholar] [CrossRef] [Green Version]
- Boney, C.M.; Verma, A.; Tucker, R.; Vohr, B.R. Metabolic syndrome in childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005, 115, e290–e296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.; Dalrymple, K.V.; Briley, A.L.; Pasupathy, D.; Seed, P.T.; Flynn, A.C.; Poston, L. Mode of infant feeding, eating behaviour and anthropometry in infants at 6-months of age born to obese women—A secondary analysis of the UPBEAT trial. BMC Pregnancy Childbirth 2018, 18, 355. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Haroun, D.; Levene, D.; Darch, T.; Williams, J.E.; Fewtrell, M.S. Prenatal and postnatal programming of body composition in obese children and adolescents: Evidence from anthropometry, DXA and the 4-component model. Int. J. Obes. 2011, 35, 534–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowe, W.L., Jr.; Scholtens, D.M.; Lowe, L.P.; Kuang, A.; Nodzenski, M.; Talbot, O.; Catalano, P.M.; Linder, B.; Brickman, W.J.; Clayton, P.; et al. Association of Gestational Diabetes With Maternal Disorders of Glucose Metabolism and Childhood Adiposity. JAMA 2018, 320, 1005–1016. [Google Scholar] [CrossRef]
- Kusinski, L.C.; Murphy, H.R.; De Lucia Rolfe, E.; Rennie, K.L.; Oude Griep, L.M.; Hughes, D.; Taylor, R.; Meek, C.L. Dietary Intervention in Pregnant Women with Gestational Diabetes; Protocol for the DiGest Randomised Controlled Trial. Nutrients 2020, 12, 1165. [Google Scholar] [CrossRef]
- Diabetes in pregnancy: Management of Diabetes and Its Complications from Preconception to the Postnatal Period. In National Institute of Clinical Excellence (NICE) Guideline NG3; 2015; Available online: https://www.nice.org.uk/guidance/ng3 (accessed on 30 March 2021).
- Royal College of Paediatrics and Child Health Guidelines for the Ethical Conduct of Medical Research Involving Children. Available online: https://www.nihr.ac.uk/documents/children-payment-for-participation-report/12085 (accessed on 21 January 2021).
- World Health Organisation. Noncommunicable Diseases and Their Risk Factors. The STEPS Manual. Available online: https://www.who.int/ncds/surveillance/steps/panammanual/en/ (accessed on 30 January 2017).
- van Hees, V.T.; Renström, F.; Wright, A.; Gradmark, A.; Catt, M.; Chen, K.Y.; Löf, M.; Bluck, L.; Pomeroy, J.; Wareham, N.J.; et al. Estimation of daily energy expenditure in pregnant and non-pregnant women using a wrist-worn tri-axial accelerometer. PLoS ONE 2011, 6, e22922. [Google Scholar] [CrossRef] [Green Version]
- Hesketh, K.R.; Evenson, K.R.; Stroo, M.; Clancy, S.M.; Østbye, T.; Benjamin-Neelon, S.E. Physical activity and sedentary behavior during pregnancy and postpartum, measured using hip and wrist-worn accelerometers. Prev. Med. Rep. 2018, 10, 337–345. [Google Scholar] [CrossRef]
- da Silva, S.G.; Evenson, K.R.; Ekelund, U.; da Silva, I.C.M.; Domingues, M.R.; da Silva, B.G.C.; Mendes, M.A.; Cruz, G.I.N.; Hallal, P.C. How many days are needed to estimate wrist-worn accelerometry-assessed physical activity during the second trimester in pregnancy? PLoS ONE 2019, 14, e0211442. [Google Scholar] [CrossRef]
- Besson, H.; Brage, S.; Jakes, R.W.; Ekelund, U.; Wareham, N.J. Estimating physical activity energy expenditure, sedentary time, and physical activity intensity by self-report in adults. Am. J. Clin. Nutr. 2010, 91, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Golubic, R.; May, A.M.; Benjaminsen Borch, K.; Overvad, K.; Charles, M.A.; Diaz, M.J.; Amiano, P.; Palli, D.; Valanou, E.; Vigl, M.; et al. Validity of electronically administered Recent Physical Activity Questionnaire (RPAQ) in ten European countries. PLoS ONE 2014, 9, e92829. [Google Scholar] [CrossRef] [Green Version]
- Yates, T.; Griffin, S.; Bodicoat, D.H.; Brierly, G.; Dallosso, H.; Davies, M.J.; Eborall, H.; Edwardson, C.; Gillett, M.; Gray, L.; et al. PRomotion Of Physical activity through structured Education with differing Levels of ongoing Support for people at high risk of type 2 diabetes (PROPELS): Study protocol for a randomized controlled trial. Trials 2015, 16, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McParlin, C.; Robson, S.C.; Tennant, P.W.G.; Besson, H.; Rankin, J.; Adamson, A.J.; Pearce, M.S.; Bell, R. Objectively measured physical activity during pregnancy: A study in obese and overweight women. BMC Pregnancy Childbirth 2010, 10, 76. [Google Scholar] [CrossRef]
- Bond, M.J.; McDowell, A.J.; Wilkinson, J.Y. The measurement of dietary restraint, disinhibition and hunger: An examination of the factor structure of the Three Factor Eating Questionnaire (TFEQ). Int. J. Obes. Relat. Metab. Disord. 2001, 25, 900–906. [Google Scholar] [CrossRef] [Green Version]
- Bradley, J.; Simpson, E.; Poliakov, I.; Matthews, J.N.; Olivier, P.; Adamson, A.J.; Foster, E. Comparison of INTAKE24 (an Online 24-h Dietary Recall Tool) with Interviewer-Led 24-h Recall in 11-24 Year-Old. Nutrients 2016, 8, 358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, E.; Lee, C.; Imamura, F.; Hollidge, S.E.; Westgate, K.L.; Venables, M.C.; Poliakov, I.; Rowland, M.K.; Osadchiy, T.; Bradley, J.C.; et al. Validity and reliability of an online self-report 24-h dietary recall method (Intake24): A doubly labelled water study and repeated-measures analysis. J. Nutr. Sci. 2019, 8, e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnell, S.; Wardle, J. Measuring behavioural susceptibility to obesity: Validation of the child eating behaviour questionnaire. Appetite 2007, 48, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, C.H.; van Jaarsveld, C.H.; Johnson, L.; Carnell, S.; Wardle, J. Development and factor structure of the Baby Eating Behaviour Questionnaire in the Gemini birth cohort. Appetite 2011, 57, 388–396. [Google Scholar] [CrossRef]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry 2001, 42, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wardle, J.; Sanderson, S.; Guthrie, C.A.; Rapoport, L.; Plomin, R. Parental feeding style and the inter-generational transmission of obesity risk. Obes. Res. 2002, 10, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Stumvoll, M.; Mitrakou, A.; Pimenta, W.; Jenssen, T.; Yki-Jarvinen, H.; Van Haeften, T.; Renn, W.; Gerich, J. Use of the oral glucose tolerance test to assess insulin release and insulin sensitivity. Diabetes Care 2000, 23, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef]
- Aiken, C.E.M.; Hone, L.; Murphy, H.R.; Meek, C.L. Improving outcomes in gestational diabetes: Does gestational weight gain matter? Diabet Med. 2019, 36, 167–176. [Google Scholar] [CrossRef]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Asher, P. Fat babies and fat children. The prognosis of obesity in the very young. Arch. Dis. Child. 1966, 41, 672–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarry-Adkins, J.L.; Aiken, C.E.; Ozanne, S.E. Neonatal, infant, and childhood growth following metformin versus insulin treatment for gestational diabetes: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002848. [Google Scholar] [CrossRef] [Green Version]
- Tarry-Adkins, J.L.; Aiken, C.E.; Ozanne, S.E. Comparative impact of pharmacological treatments for gestational diabetes on neonatal anthropometry independent of maternal glycaemic control: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003126. [Google Scholar] [CrossRef] [PubMed]
- van Poppel, M.N.M.; Simmons, D.; Devlieger, R.; van Assche, F.A.; Jans, G.; Galjaard, S.; Corcoy, R.; Adelantado, J.M.; Dunne, F.; Harreiter, J.; et al. A reduction in sedentary behaviour in obese women during pregnancy reduces neonatal adiposity: The DALI randomised controlled trial. Diabetologia 2019. [Google Scholar] [CrossRef] [Green Version]
- Okereke, N.C.; Uvena-Celebrezze, J.; Hutson-Presley, L.; Amini, S.B.; Catalano, P.M. The effect of gender and gestational diabetes mellitus on cord leptin concentration. Am. J. Obs. Gynecol. 2002, 187, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Laffineuse, L.; Presley, L.; Minium, J.; Catalano, P.M.; Hauguel-de Mouzon, S. In utero gender dimorphism of adiponectin reflects insulin sensitivity and adiposity of the fetus. Obesity 2009, 17, 1144–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.L.; Du, Q.; Djemli, A.; Julien, P.; Fraser, W.D.; Luo, Z.C. Cord blood insulin, IGF-I, IGF-II, leptin, adiponectin and ghrelin, and their associations with insulin sensitivity, β-cell function and adiposity in infancy. Diabet Med. 2018, 35, 1412–1419. [Google Scholar] [CrossRef] [PubMed]
- Musial, B.; Vaughan, O.R.; Fernandez-Twinn, D.S.; Voshol, P.; Ozanne, S.E.; Fowden, A.L.; Sferruzzi-Perri, A.N. A Western-style obesogenic diet alters maternal metabolic physiology with consequences for fetal nutrient acquisition in mice. J. Physiol. 2017, 595, 4875–4892. [Google Scholar] [CrossRef]
- Sferruzzi-Perri, A.N.; Owens, J.A.; Pringle, K.G.; Robinson, J.S.; Roberts, C.T. Maternal insulin-like growth factors-I and -II act via different pathways to promote fetal growth. Endocrinology 2006, 147, 3344–3355. [Google Scholar] [CrossRef] [PubMed]
- Hnatiuk, J.A.; Hesketh, K.R.; van Sluijs, E.M. Correlates of home and neighbourhood-based physical activity in UK 3-4-year-old children. Eur. J. Public Health 2016, 26, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesketh, K.R.; O’Malley, C.; Paes, V.M.; Moore, H.; Summerbell, C.; Ong, K.K.; Lakshman, R.; van Sluijs, E.M.F. Determinants of Change in Physical Activity in Children 0-6 years of Age: A Systematic Review of Quantitative Literature. Sports Med. 2017, 47, 1349–1374. [Google Scholar] [CrossRef] [Green Version]
- Rito, A.I.; Buoncristiano, M.; Spinelli, A.; Salanave, B.; Kunešová, M.; Hejgaard, T.; García Solano, M.; Fijałkowska, A.; Sturua, L.; Hyska, J.; et al. Association between Characteristics at Birth, Breastfeeding and Obesity in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative—COSI 2015/2017. Obes. Facts 2019, 12, 226–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Collins, C.; Ratliff, M.; Xie, B.; Wang, Y. Breastfeeding Reduces Childhood Obesity Risks. Child. Obes. 2017, 13, 197–204. [Google Scholar] [CrossRef]
- Bider-Canfield, Z.; Martinez, M.P.; Wang, X.; Yu, W.; Bautista, M.P.; Brookey, J.; Page, K.A.; Buchanan, T.A.; Xiang, A.H. Maternal obesity, gestational diabetes, breastfeeding and childhood overweight at age 2 years. Pediatr. Obes. 2017, 12, 171–178. [Google Scholar] [CrossRef]
- Stettler, N.; Kumanyika, S.K.; Katz, S.H.; Zemel, B.S.; Stallings, V.A. Rapid weight gain during infancy and obesity in young adulthood in a cohort of African Americans. Am. J. Clin. Nutr. 2003, 77, 1374–1378. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, {kind=link}
