
Hypomagnesemia Is a Risk Factor for Infections after Kidney Transplantation: A Retrospective Cohort Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
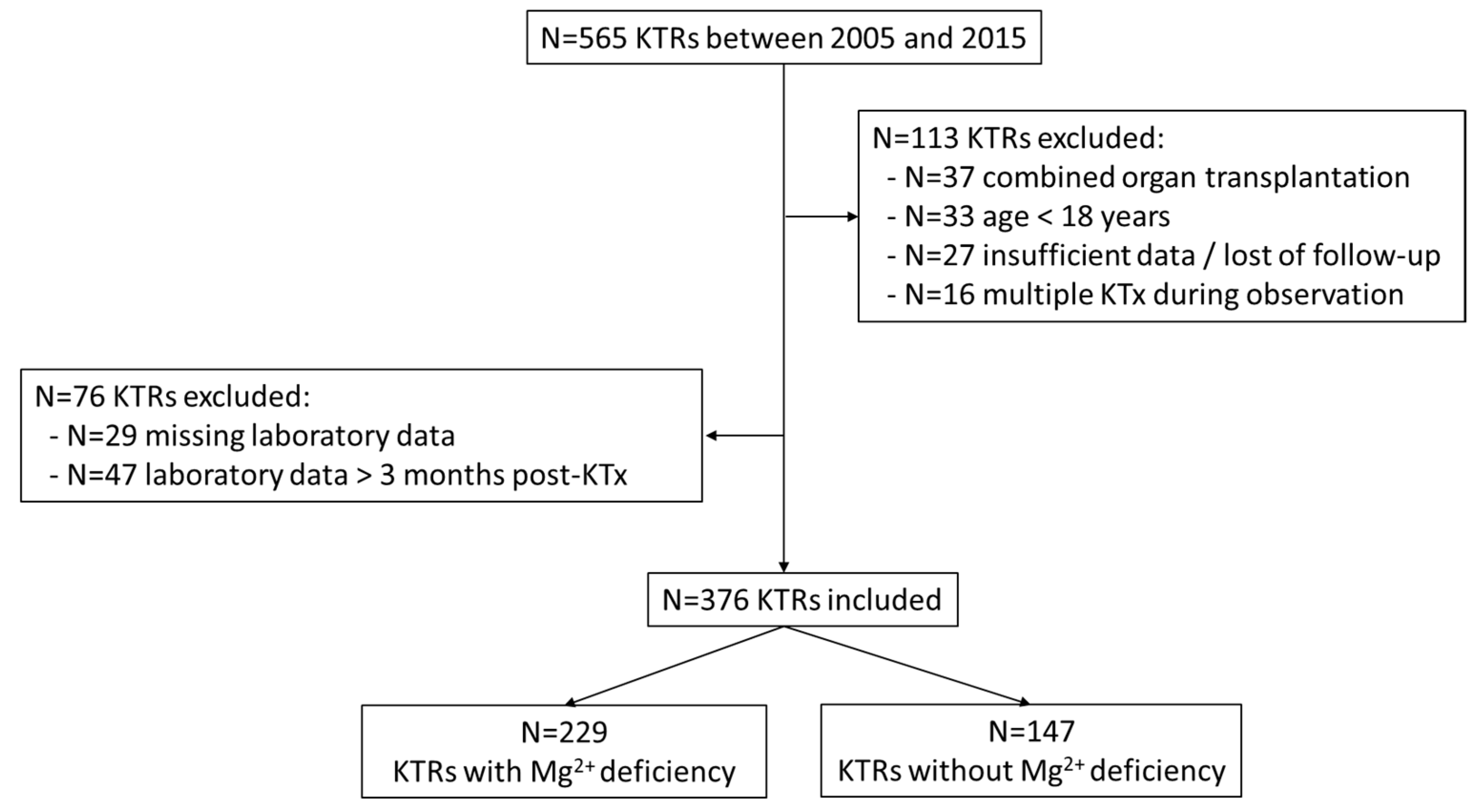
2.1. Study Design and Patients’ Characteristics
2.2. Type of Infections, Laboratory, and Clinical Definitions
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Laboratory Findings
3.2. Percentage and Incidence of Infections
3.3. Risk Factors for Infections
3.4. Risk Factors for Magnesium Deficiency
3.5. Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J.M. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Maguire, M.E. Magnesium and cell proliferation. Ann. N. Y. Acad. Sci. 1988, 551, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Mooren, F.C.; Krüger, K.; Völker, K.; Golf, S.W.; Wadepuhl, M.; Kraus, A. Oral magnesium supplementation reduces insulin resistance in non-diabetic subjects—A double-blind, placebo-controlled, randomized trial. Diabetes Obes. Metab. 2011, 13, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Pilchova, I.; Klacanova, K.; Tatarkova, Z.; Kaplan, P.; Racay, P. The involvement of Mg2+ in regulation of cellular and mitochondrial functions. Oxid. Med. Cell. Longev. 2017, 2017, 6797460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galland, L. Magnesium and immune function: An overview. Magnesium 1988, 7, 290–299. [Google Scholar]
- Liang, R.Y.; Wu, W.; Huang, J.; Jiang, S.P.; Lin, Y. Magnesium affects the cytokine secretion of CD4+ T lymphocytes in asthma. J. Asthma. 2012, 49, 1012–1015. [Google Scholar] [CrossRef]
- Brandao, K.; Deason-Towne, F.; Perraud, A.L.; Schmitz, C. The role of Mg2+ in immune cells. Immunol. Res. 2013, 55, 261–269. [Google Scholar] [CrossRef]
- Li, F.Y.; Chaigne-Delalande, B.; Kanellopoulou, C.; Davis, J.C.; Matthews, H.F.; Douek, D.C.; Cohen, J.I.; Uzel, G.; Su, H.C.; Lenardo, M.J. Second messenger role for Mg2+ revealed by human T-cell immunodeficiency. Nature 2011, 475, 471–476. [Google Scholar] [CrossRef]
- Van Laecke, S.; Van Biesen, W. Hypomagnesaemia in kidney transplantation. Transplant. Rev. 2015, 29, 154–160. [Google Scholar] [CrossRef]
- Barton, C.H.; Vaziri, N.D.; Martin, D.C.; Choi, S.; Alikhani, S. Hypomagnesemia and renal magnesium wasting in renal transplant recipients receiving cyclosporine. Am. J. Med. 1987, 83, 693–699. [Google Scholar] [CrossRef]
- Markell, M.S.; Altura, B.T.; Sarn, Y.; Barbour, R.; Friedman, E.A.; Altura, B.M. Relationship of ionized magnesium and cyclosporine level in renal transplant recipients. Ann. N. Y. Acad. Sci. 1993, 696, 408–411. [Google Scholar] [CrossRef]
- Nijenhuis, T.; Hoenderop, J.G.; Bindels, R.J. Downregulation of Ca(2+) and Mg(2+) transport proteins in the kidney explains tacrolimus (FK506)-induced hypercalciuria and hypomagnesemia. J. Am. Soc. Nephrol. 2004, 15, 549–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navaneethan, S.D.; Sankarasubbaiyan, S.; Gross, M.D.; Jeevanantham, V.; Monk, R.D. Tacrolimus associated hypomagnesemia in renal transplant recipients. Transplant. Proc. 2006, 38, 1320–1322. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A. Infection in solid-organ transplant recipients. N. Eng. J. Med. 2007, 357, 2601–2614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karuthu, S.; Blumberg, E.A. Common infections in kidney transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cippà, P.E.; Schiesser, M.; Ekberg, H.; van Gelder, T.; Mueller, N.J.; Cao, C.A.; Fehr, T.; Bernasconi, C. Risk stratification for rejection and infection after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2015, 10, 2213–2220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney. Int. 2014, 85, 174–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaigne-Delalande, B.; Li, F.Y.; O’Connor, G.M.; Lukacs, M.J.; Jiang, P.; Zheng, L.; Shatzer, A.; Biancalana, M.; Pittaluga, S.; Matthews, H.F.; et al. Mg2+ regulates cytotoxic functions of NK and CD8 T cells in chronic EBV infection through NKG2D. Science 2013, 341, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Van Laecke, S.; Vermeiren, P.; Nagler, E.V.; Caluwe, R.; De Wilde, M.; Van der Vennet, M.; Peeters, P.; Randon, C.; Vermassen, F.; Vanholder, R.; et al. Magnesium and infection risk after kidney transplantation: An observational cohort study. J. Infect. 2016, 73, 8–17. [Google Scholar] [CrossRef]
- Deak, A.T.; Ionita, F.; Kirsch, A.H.; Odler, B.; Rainer, P.P.; Kramar, R.; Kubatzki, M.P.; Eberhard, K.; Berghold, A.; Rosenkranz, A.R. Impact of cardiovascular risk stratification strategies in kidney transplantation over time. Nephrol. Dial. Transplant. 2020, 35, 1810–1818. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [Green Version]
- Schröppel, B.; Legendre, C. Delayed kidney graft function: From mechanism to translation. Kidney. Int. 2014, 86, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Weinrauch, L.A.; D’Elia, J.A.; Weir, M.R.; Bunnapradist, S.; Finn, P.V.; Liu, J.; Claggett, B.; Monaco, A.P. Infection and Malignancy Outweigh Cardiovascular Mortality in Kidney Transplant Recipients: Post Hoc Analysis of the FAVORIT Trial. Am. J. Med. 2018, 131, 165–172. [Google Scholar] [CrossRef]
- Bodro, M.; Linares, L.; Chiang, D.; Moreno, A.; Cervera, C. Managing recurrent urinary tract infections in kidney transplant recipients. Expert. Rev. Anti-Infect. Ther. 2018, 16, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Famure, O.; Li, Y.; Kim, S.J. Hypomagnesemia and the risk of new-onset diabetes mellitus after kidney transplantation. J. Am. Soc. Nephrol. 2016, 27, 1793–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Laecke, S.; Maréchal, C.; Verbeke, F.; Peeters, P.; Van Biesen, W.; Devuyst, O.; Jadoul, M.; Vanholder, R. The relation between hypomagnesaemia and vascular stiffness in renal transplant recipients. Nephrol. Dial. Transplant. 2011, 26, 2362–2369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisters, K.; Gremmler, B.; Hausberg, M. Magnesium and arterial stiffness. Hypertension 2006, 47, e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shechter, M.; Sharir, M.; Labrador, M.J.; Forrester, J.; Silver, B.; Bairey Merz, C.N. Oral magnesium therapy improves endothelial function in patients with coronary artery disease. Circulation 2000, 102, 2353–2358. [Google Scholar] [CrossRef] [Green Version]
- Feske, S.; Skolnik, E.Y.; Prakriya, M. Ion channels and transporters in lymphocyte function and immunity. Nat. Rev. Immunol. 2012, 12, 532–547. [Google Scholar] [CrossRef] [Green Version]
- Weglicki, W.B.; Phillips, T.M.; Freedman, A.M.; Cassidy, M.M.; Dickens, B.F. Magnesium deficiency elevates circulating levels of inflammatory cytokines and endothelia. Mol. Cell. Biochem. 1992, 110, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Weglicki, W.B.; Dickens, B.F.; Wagner, T.L.; Chmielinska, J.J.; Phillips, T.M. Immunoregulation by neuropeptides in magnesium deficiency ex vivo effect of enhanced substance P production on circulating T lymphocytes from magnesium-deficient mice. Magnes. Res. 1996, 9, 3–11. [Google Scholar] [PubMed]
- Malpuech-Brugère, C.; Nowacki, W.; Daveau, M.; Gueux, E.; Linard, C.; Rock, E.; Lebreton, J.P.; Mazur, A.; Rayssiguier, Y. Inflammatory response following acute magnesium deficiency in the rat. Biochim. Biophys. Acta 2000, 1501, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Kanellopoulou, C.; George, A.B.; Masutani, E.; Cannons, J.L.; Ravell, J.C.; Yamamoto, T.N.; Smelkinson, M.G.; Jiang, P.D.; Matsuda-Lennikov, M.; Reilley, J.; et al. Mg2+ regulation of kinase signaling and immune function. J. Exp. Med. 2019, 216, 1828–1842. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.K.; Dowdell, K.; Roy, A.; Niemela, J.E.; Wilson, W.; McElwee, J.J.; Hughes, J.D.; Cohen, J.I. Magnesium restores activity to peripheral blood cells in a patient with functionally impaired interleukin-2-inducible T cell kinase. Front. Immunol. 2019, 10, 2000. [Google Scholar] [CrossRef] [Green Version]
- Nolen, B.; Taylor, S.; Ghosh, G. Regulation of protein kinases; controlling activity through activation segment conformation. Mol. Cell 2004, 15, 661–675. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodriguez-Moran, M. Magnesium improves the beta-cell function to compensate variation of insulin sensitivity: Double-blind, randomized clinical trial. Eur. J. Clin. Investig. 2011, 41, 405–410. [Google Scholar] [CrossRef]
- Mooren, F.C. Magnesium and disturbances in carbohydrate metabolism. Diabetes Obes. Metab. 2015, 17, 813–823. [Google Scholar] [CrossRef]
- Chang, C.H.; Curtis, J.D.; Maggi, L.B., Jr.; Faubert, B.; Villarino, A.V.; O’Sullivan, D.; Huang, S.C.C.; Van Der Windt, G.J.; Blagih, J.; Qiu, J.; et al. Posttranscriptional control of T cell effector function by aerobic glycolysis. Cell 2013, 153, 1239–1251. [Google Scholar] [CrossRef] [Green Version]
- Fischer, H.J.; Sie, C.; Schumann, E.; Witte, A.K.; Dressel, R.; van den Brandt, J.; Reichardt, H.M. The insulin receptor plays a critical role in T cell function and adaptive immunity. J. Immunol. 2017, 198, 1910–1920. [Google Scholar] [CrossRef] [Green Version]
- Gommers, L.M.; Hoenderop, J.G.; Bindels, R.J.; de Baaij, J.H. Hypomagnesemia in type 2 diabetes: A vicious circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garnier, A.S.; Duveau, A.; Planchais, M.; Subra, J.F.; Sayegh, J.; Augusto, J.F. Serum magnesium after kidney transplantation: A systematic review. Nutrients 2018, 10, 729. [Google Scholar] [CrossRef] [Green Version]
- Van Laecke, S.; Nagler, E.V.; Taes, Y.; Biesen, W.V.; Peetres, P.; Vanholder, R. The effect of magnesium supplements on early post-transplantation glucose metabolism: A randomized controlled trial. Transplant. Int. 2014, 27, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Caluwe, R.; Huybrechts, I.; Nagler, E.V.; Vanholder, R.; Peeters, P.; Van Vlem, B.; Van Biesen, W. Effects of magnesium supplements on insulin secretion after kidney transplantation: A randomized controlled trial. Ann. Transplant. 2017, 22, 524–531. [Google Scholar] [CrossRef]
- Kinnunen, S.; Karhapää, P.; Juutilainen, A.; Finne, P.; Helanterä, I. Secular trends in infection-related mortality after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2018, 13, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Nasser, R.; Mohammad, E.N.; Mashiach, T.; Azzam, Z.S.; Braun, E. The association between serum magnesium levels and community-acquired pneumonia 30-day mortality. BMC. Infect. Dis. 2018, 18, 698. [Google Scholar] [CrossRef]
- Elgendy, H.M.; El Moghazy, W.M.; Uemoto, S.; Fukuda, K. Pre transplant serum magnesium level predicts outcome after pediatric living donor liver transplantation. Ann. Transplant. 2012, 17, 29–37. [Google Scholar]
- Helanterä, I.; Egli, A.; Koskinen, P.; Lautenschlager, I.; Hirsch, H.H. Viral impact on long-term kidney graft function. Infect. Dis. Clin. N. Am. 2010, 24, 339–371. [Google Scholar] [CrossRef]
- Karpe, K.M.; Talaulikar, G.S.; Walters, G.D. Calcineurin inhibitor withdrawal or tapering for kidney transplant recipients. Cochrane Database Syst. Rev. 2017, 7, CD006750. [Google Scholar] [CrossRef] [PubMed]
- Mallat, S.G.; Tanios, B.Y.; Itani, H.S.; Lotfi, T.; McMullan, C.; Gabardi, S.; Akl, E.A.; Azzi, J.R. CMV and BKPyV infections in renal transplant recipients receiving an mTOR inhibitor-based versus a CNI-based regimen: A systematic review and meta-analysis of randomized, controlled trials. Clin. J. Am. Soc. Nephrol. 2017, 12, 1321–1336. [Google Scholar] [CrossRef]
- Gratreak, B.D.; Swanson, E.A.; Lazelle, R.A.; Jelen, S.K.; Hoenderop, J.; Bindels, R.J.; Yang, C.L.; Ellison, D.H. Tacrolimus-induced hypomagnesemia and hypercalciuria requires FKBP12 suggesting a role for calcineurin. Physiol. Rep. 2020, 8, e14316. [Google Scholar] [CrossRef]
- Ekberg, H.; Tedesco-Silva, H.; Demirbas, A.; Vítko, Š.; Nashan, B.; Gürkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced exposure to calcineurin inhibitors in renal transplantation. N. Eng. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gur, C.; Coppenhagen-Glazer, S.; Rosenberg, S.; Yamin, R.; Enk, J.; Glasner, A.; Bar-On, Y.; Fleissig, O.; Naor, R.; Abed, J.; et al. Natural killer cell-mediated host defense against uropathogenic E. coli is counteracted by bacterial hymolysinA-dependent killing of NK cells. Cell. Host Microbe 2013, 14, 664–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, S.N.; Miao, Y. The nature of immune responses to urinary tract infections. Nat. Rev. Immunol. 2015, 10, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Vangala, C.; Pan, J.; Cotton, R.T.; Ramanathan, V. Mineral and bone disorders after kidney transplantation. Front. Med. 2018, 5, 211. [Google Scholar] [CrossRef]
- Wolf, M.; Weir, M.R.; Kopyt, N.; Mannon, R.B.; Von Visger, J.; Deng, H.; Yue, S.; Vincenti, F. A prospective cohort study of mineral metablism after kidney transplantation. Transplantation 2016, 100, 184–193. [Google Scholar] [CrossRef] [Green Version]
- Ishimura, E.; Okuno, S.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum magnesium concentration is a significant predictor of mortality in maintenance hemodialysis patients. Magnes. Res. 2007, 20, 237–244. [Google Scholar]
- Lacson, E., Jr.; Wang, W.; Ma, L.; Passlick-Deetjen, J. Serum magnesium and mortality in hemodialysis patients in the United States: A cohort study. Am. J. Kidney Dis. 2015, 66, 1056–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. Am. J. Transplant. 2009, 9, S1–S155.
- Humar, A.; Snydman, D. AST Infectious Diseases Community of Practice. Cytomegalovirus in solid organ transplant recipients. Am. J. Transplant. 2009, 9, S78–S86. [Google Scholar] [CrossRef]
- Bayraktar, A.; Catma, Y.; Akyildiz, A.; Demir, E.; Bakkaloglu, H.; Ucar, A.R.; Dirim, A.B.; Usta Akgul, S.; Temurhan, S.; Gok, A.F.K.; et al. Infectious complications of induction therapies in kidney transplantation. Ann. Transplant. 2019, 24, 412–417. [Google Scholar] [CrossRef]
- Bertrand, D.; Chavarot, N.; Gatault, P.; Garrouste, C.; Bouvier, N.; Grall-Jezequel, A.; Jaureguy, M.; Caillard, S.; Lemoine, M.; Colosio, C.; et al. Opportunistic infections after conversion to belatacept in kidney transplantation. Nephrol. Dial. Transplant. 2020, 35, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Hill, P.; Cross, N.B.; Barnett, A.N.R.; Palmer, S.C.; Webster, A.C. Polyclonal and monoclonal antibodies for induction therapy in kidney transplant recipients. Cochrane. Database Syst. Rev. 2017, 1, CD004759. [Google Scholar] [CrossRef] [PubMed]
- Hellemans, R.; Bosmans, J.L.; Abramowicz, D. Induction therapy for kidney transplant recipients: Do we still need anti-IL2 receptor monoclonal antibodies? Am. J. Transplant. 2017, 17, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Reddy, S.T.; Soman, S.S.; Yee, J. Magnesium balance and measurement. Adv. Chronic Kidney Dis. 2018, 25, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; Goldsmith, D.; Uyar, M.E.; Turgut, F.; Covic, A. Magnesium in chronic kidney disease: Challenges and opportunities. Blood Purif. 2010, 29, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Maddukuri, G.; Xie, Y. Proton pump inhibitors and kidney: Implications of current evidence for clinical practice and when and how to describe. Am. J. Kidney Dis. 2020, 75, 497–507. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Whole Study Population (N = 376) | Patients without Mg2+ Deficiency (N = 147) | Patients with Mg2+ Deficiency (N = 229) | p-Value | |
|---|---|---|---|---|
| Age at time of KT (years) | 52.0 (41.0–62.0) | 50.0 (40.0–61.0) | 53.0 (42.0–62.0) | 0.133 |
| Gender (female) | 118 (31.4) | 41 (27.9) | 77 (33.6) | 0.242 |
| BMI (kg/m2) | 24.9 (22.1–28.1) | 24.4 (22.1–28.1) | 25.2 (22.3–28.0) | 0.372 |
| Nicotine abuse | 169 (44.9) | 71 (48.3) | 98 (42.8) | 0.295 |
| Dialysis-related data | ||||
| Hemodialysis | 293 (77.9) | 114 (77.6) | 179 (78.2) | 0.888 |
| Peritoneal dialysis | 62 (16.5) | 25 (17.0) | 37 (16.2) | 0.829 |
| Preemptive KT | 21 (5.6) | 8 (5.4) | 13 (5.7) | 0.923 |
| Dialysis vintage (months) | 40.5 (22.0–71.0) | 35.0 (18.0–58.0) | 42.0 (22.0–75.0) | 0.208 |
| Comorbidities | ||||
| Diabetes mellitus | 58 (15.4) | 28 (19.0) | 30 (13.1) | 0.119 |
| Dyslipidemia | 197 (52.4) | 75 (51.0) | 122 (53.3) | 0.669 |
| Hypertension | 357 (94.9) | 138 (93.9) | 219 (95.6) | 0.448 |
| Coronary heart disease | 37 (9.8) | 16 (10.9) | 21 (9.2) | 0.586 |
| Transplantation-related data | ||||
| Living kidney donation | 47 (12.5) | 19 (12.9) | 28 (12.2) | 0.842 |
| Previous KT | 80 (21.3) | 27 (18.4) | 53 (23.1) | 0.269 |
| Donor CMV seropositivity | 170 (46.8) | 55 (39.0) | 115 (51.8) | 0.017 |
| Recipient CMV seropositivity | 225 (61.8) | 85 (59.9) | 140 (63.1) | 0.539 |
| GN as primary renal disease | 130 (34.6) | 50 (34.0) | 80 (34.9) | 0.855 |
| Delayed graft function | 133 (35.4) | 56 (38.1) | 77 (33.6) | 0.376 |
| Immunosuppression | ||||
| CNI | 374 (99.5) | 145 (98.6) | 229 (100) | 0.077 |
| mTOR inhibitor | 3 (0.8) | 2 (1.4) | 1 (0.4) | 0.326 |
| Antiproliferative agents | 372 (98.9) | 144 (98.0) | 228 (99.6) | 0.139 |
| Laboratory data * | ||||
| Leukocytes (10 × 9/L) | 8.3 (6.3–10.7) | 8.7 (6.4–10.6) | 8.1 (6.3–10.7) | 0.471 |
| C-reactive protein (mg/dL) | 2.7 (1.0–5.9) | 2.8 (1.0–7.2) | 2.4 (1.0–4.9) | 0.151 |
| Parathyroid hormone (pg/mL) | 155.2 (105.8–234.8) | 155.7 (94.6–237.1) | 153.6 (108.5–228.7) | 0.644 |
| Calcium, total (mmol/L) | 2.4 (2.3–2.5) | 2.4 (2.3–2.5) | 2.4 (2.3–2.5) | 0.239 |
| Phosphate (mg/dL) | 2.3 (1.9–2.9) | 2.5 (2.0–3.3) | 2.2 (1.7–2.7) | <0.001 |
| Bicarbonate (mmol/L) | 22.1 (20.1–24.5) | 22.2 (19.9–24.9) | 22.0 (20.3–24.2) | 0.594 |
| Creatinine (mg/dL) | 1.5 (1.3–1.9) | 1.7 (1.3–2.3) | 1.5 (1.3–1.8) | 0.001 |
| eGFR (ml/min/1.73 m2) | 47.0 (35.5–59.8) | 41.7 (31.0–59.6) | 49.2 (38.4–60.4) | 0.009 |
| Albumin (g/dL) | 3.9 (3.5–4.3) | 3.8 (3.4–4.4) | 3.9 (3.5–4.3) | 0.950 |
| 25(OH)-vitamin D (ng/mL) | 23.7 (15.2–31.4) | 21.1 (14.0–29.2) | 25.2 (17.3–32.8) | 0.007 |
| Magnesium supplementation | 57 (15.2) | 25 (17.0) | 32 (14.0) | 0.424 |
| Type of Infections | Whole Study Population | Patients without Mg2+ Deficiency | Patients with Mg2+ Deficiency | |||
|---|---|---|---|---|---|---|
| N = 376 | N = 364 | N = 147 | N = 143 | N = 229 | N = 221 | |
| 0–12 Months | 12–24 Months | 0–12 Months | 12–24 Months | 0–12 Months | 12–24 Months | |
| Urinary tract infections | 204 (54.3) | 69 (19.0) | 70 (47.6) | 28 (19.6) | 134 (58.5) | 41 (18.6) |
| Viral infections | 236 (62.8) | 41 (11.3) | 76 (51.7) | 14 (9.8) | 160 (69.9) | 27 (12.2) |
| Detailed viral infections | ||||||
| CMV | 182 (48.4) | 31 (8.5) | 57 (38.8) | 10 (7.0) | 125 (54.6) | 21 (9.5) |
| Polyoma | 33 (8.8) | 5 (1.4) | 8 (5.4) | 1 (0.7) | 25 (10.9) | 4 (1.8) |
| EBV | 96 (25.5) | 10 (2.7) | 37 (25.2) | 4 (2.8) | 59 (25.8) | 6 (2.7) |
| Test Variable | Urinary Tract Infections | Viral Infections | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age at the time of KT (years) | 1.01 | 0.99–1.04 | 0.179 | 1.00 | 0.98–1.02 | 0.982 |
| Gender (female) | 4.57 | 2.56–8.16 | <0.001 | 1.14 | 0.66–1.98 | 0.635 |
| BMI (kg/m2) | 1.06 | 0.99–1.13 | 0.090 | 1.05 | 0.98–1.12 | 0.179 |
| Nicotine abuse | 1.36 | 0.83–2.22 | 0.217 | 1.65 | 1.00–2.74 | 0.051 |
| Serum Mg2+ (deficiency) | 1.73 | 1.04–2.86 | 0.035 | 2.05 | 1.23–3.41 | 0.006 |
| eGFR | 1.00 | 0.98–1.01 | 0.603 | 0.99 | 0.98–1.00 | 0.150 |
| Albumin | 0.74 | 0.49–1.12 | 0.155 | 0.73 | 0.48–1.12 | 0.146 |
| CNI serum level (highest tertile) | 0.98 | 0.59–1.63 | 0.940 | 1.68 | 0.98–2.86 | 0.059 |
| Dialysis vintage (<1 year) | 1.06 | 0.43–2.59 | 0.898 | 0.66 | 0.27–1.61 | 0.362 |
| Hemodialysis | 0.85 | 0.47–1.53 | 0.587 | 0.91 | 0.50–1.66 | 0.760 |
| Previous KT | 0.84 | 0.46–1.54 | 0.573 | 0.88 | 0.47–1.64 | 0.681 |
| Living kidney donation | 0.53 | 0.21–1.38 | 0.194 | 1.57 | 0.61–4.07 | 0.349 |
| Donor CMV seropositivity | 1.12 | 0.69–1.82 | 0.650 | 2.54 | 1.54–4.18 | <0.001 |
| Recipient CMV seropositivity | 0.67 | 0.41–1.11 | 0.123 | 1.66 | 1.00–2.76 | 0.051 |
| Delayed graft function | 1.47 | 0.83–2.60 | 0.190 | 1.19 | 0.97–2.13 | 0.552 |
| Diabetes mellitus | 1.06 | 0.52–2.18 | 0.877 | 0.82 | 0.40–1.69 | 0.589 |
| GN as primary kidney disease | 0.72 | 0.44–1.20 | 0.205 | 0.80 | 0.48–1.34 | 0.387 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odler, B.; Deak, A.T.; Pregartner, G.; Riedl, R.; Bozic, J.; Trummer, C.; Prenner, A.; Söllinger, L.; Krall, M.; Höflechner, L.; et al. Hypomagnesemia Is a Risk Factor for Infections after Kidney Transplantation: A Retrospective Cohort Analysis. Nutrients 2021, 13, 1296. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041296
Odler B, Deak AT, Pregartner G, Riedl R, Bozic J, Trummer C, Prenner A, Söllinger L, Krall M, Höflechner L, et al. Hypomagnesemia Is a Risk Factor for Infections after Kidney Transplantation: A Retrospective Cohort Analysis. Nutrients. 2021; 13(4):1296. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041296
Chicago/Turabian StyleOdler, Balazs, Andras T. Deak, Gudrun Pregartner, Regina Riedl, Jasmin Bozic, Christian Trummer, Anna Prenner, Lukas Söllinger, Marcell Krall, Lukas Höflechner, and et al. 2021. "Hypomagnesemia Is a Risk Factor for Infections after Kidney Transplantation: A Retrospective Cohort Analysis" Nutrients 13, no. 4: 1296. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13041296