
A Meta-Analysis of Obesity and Risk of Colorectal Cancer in Patients with Lynch Syndrome: The Impact of Sex and Genetics

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
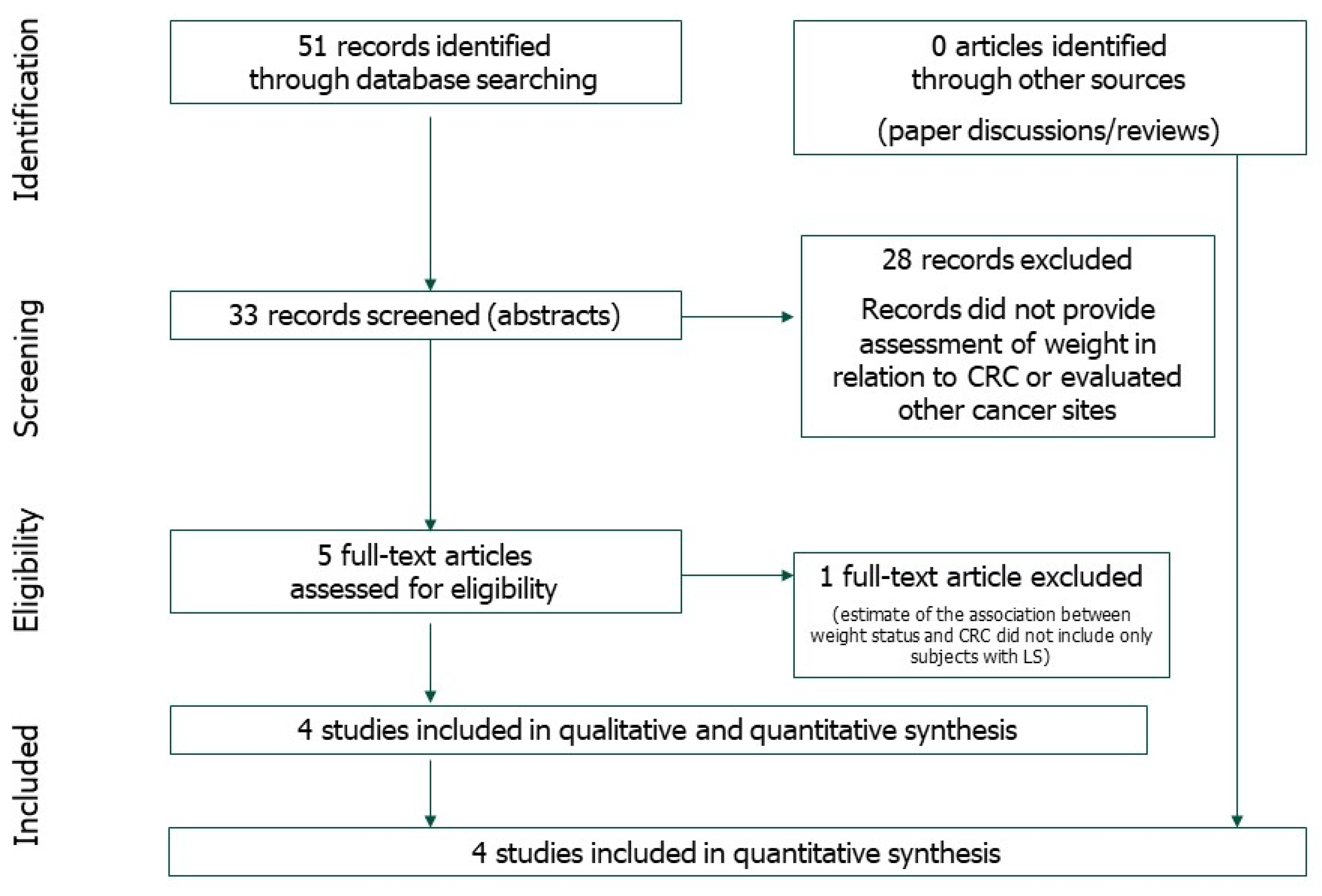
2.1. Eligibility Criteria and Study Selection
2.2. Statistical Analysis
2.3. Search Strategy
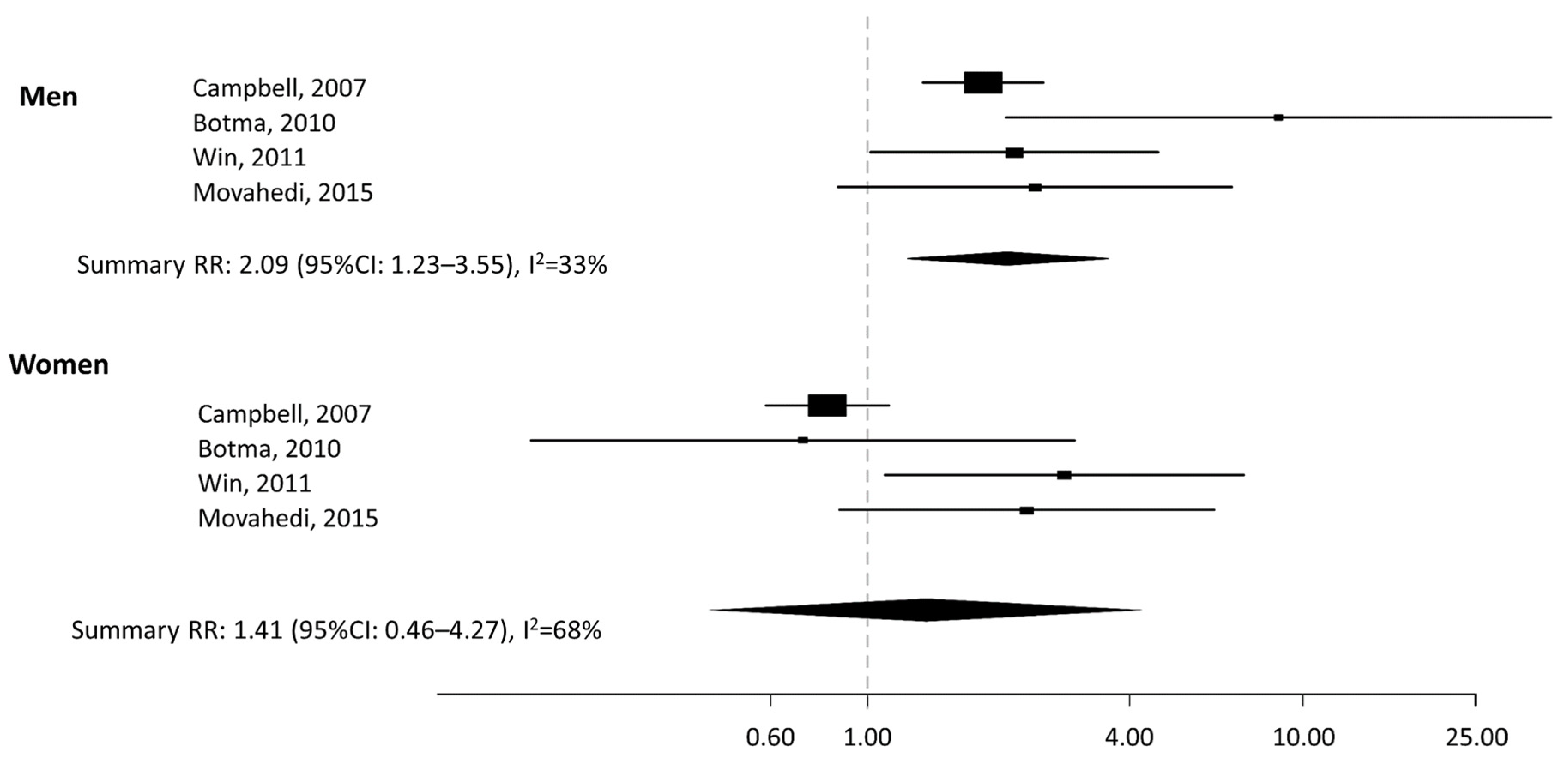
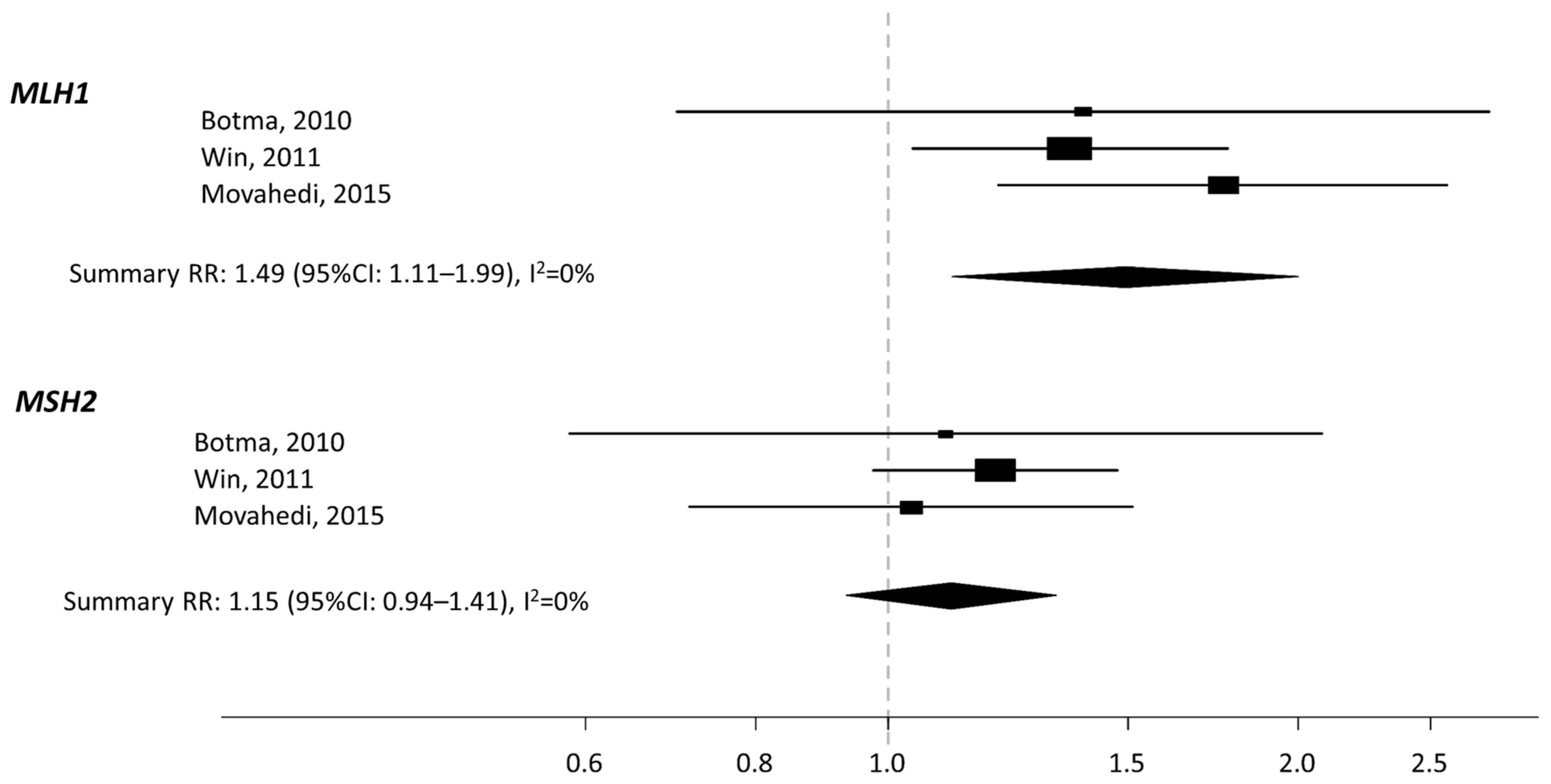
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Win, A.K.; Jenkins, M.A.; Dowty, J.G.; Antoniou, A.C.; Lee, A.; Giles, G.G.; Buchanan, D.D.; Clendenning, M.; Rosty, C.; Ahnen, D.J.; et al. Prevalence and Penetrance of Major Genes and Polygenes for Colorectal Cancer. Cancer Epidemiol. Biomark. Prev. 2017, 26, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinicrope, F.A. Lynch Syndrome–associated Colorectal Cancer. N. Engl. J. Med. 2018, 379, 764–773. [Google Scholar] [CrossRef]
- Lynch, H.T.; Snyder, C.L.; Shaw, T.G.; Heinen, C.D.; Hitchins, M.P. Milestones of Lynch Syndrome: 1895–2015. Nature Rev. Cancer 2015, 15, 181–194. [Google Scholar] [CrossRef]
- Ligtenberg, M.J.; Kuiper, R.P.; Chan, T.L.; Goossens, M.; Hebeda, K.M.; Voorendt, M.; Lee, T.Y.; Bodmer, D.; Hoenselaar, E.; Hendriks-Cornelissen, S.J. Heritable Somatic Methylation and Inactivation of MSH2 in Families with Lynch Syndrome due to Deletion of the 3′ Exons of TACSTD1. Nat. Genet. 2009, 41, 112. [Google Scholar] [CrossRef]
- Kohlmann, W.; Gruber, S.B. Lynch Syndrome. In GeneReviews(R); Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Stephens, K., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Lok, P.; Dijk, S. Offer daily aspirin to cut risk of colorectal cancer in people with Lynch syndrome, says NICE. BMJ 2019, 366, l5010. [Google Scholar] [CrossRef]
- Deng, T.; Lyon, C.J.; Bergin, S.; Caligiuri, M.A.; Hsueh, W.A. Obesity, Inflammation, and Cancer. Annu. Rev. Pathol. Mech. Dis. 2016, 11, 421–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathers, J.C. Obesity and bowel cancer: From molecular mechanisms to interventions. Nutr. Res. 2019, 70, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Bull, C.J.; Bell, J.A.; Murphy, N.; Sanderson, E.; Smith, G.D.; Timpson, N.J.; Banbury, B.L.; Albanes, D.; Berndt, S.I.; Bézieau, S.; et al. Adiposity, metabolites, and colorectal cancer risk: Mendelian randomization study. BMC Med. 2020, 18, 1–16. [Google Scholar] [CrossRef]
- Thrift, A.P.; Gong, J.; Peters, U.; Chang-Claude, J.; Rudolph, A.; Slattery, M.L.; Chan, A.T.; Locke, A.E.; Kahali, B.; Justice, A.E.; et al. Mendelian Randomization Study of Body Mass Index and Colorectal Cancer Risk. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1024–1031. [Google Scholar] [CrossRef] [Green Version]
- Jarvis, D.; Mitchell, J.S.; Law, P.J.; Palin, K.; Tuupanen, S.; Gylfe, A.; A Hänninen, U.; Cajuso, T.; Tanskanen, T.; Kondelin, J.; et al. Mendelian randomisation analysis strongly implicates adiposity with risk of developing colorectal cancer. Br. J. Cancer 2016, 115, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Dombrowski, S.U.; Knittle, K.; Avenell, A.; Araujo-Soares, V.; Sniehotta, F.F. Long term maintenance of weight loss with non-surgical interventions in obese adults: Systematic review and meta-analyses of randomised controlled trials. BMJ 2014, 348, g2646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunter, M.J.; Riboli, E. Obesity and Gastrointestinal Cancers—where do we Go from here? Nature Rev. Gastroenterol. Hepatol. 2018, 15, 651–652. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Umar, A.; Boland, C.R.; Terdiman, J.P.; Syngal, S.; Chapelle, A.d.l.; Rüschoff, J.; Fishel, R.; Lindor, N.M.; Burgart, L.J.; Hamelin, R. Revised Bethesda Guidelines for Hereditary Nonpolyposis Colorectal Cancer (Lynch Syndrome) and Microsatellite Instability. J. Natl. Cancer Inst. 2004, 96, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Coleman, H.G.; Loughrey, M.B.; Murray, L.J.; Johnston, B.T.; Gavin, A.T.; Shrubsole, M.J.; Bhat, S.K.; Allen, P.B.; McConnell, V.; Cantwell, M.M. Colorectal Cancer Risk Following Adenoma Removal: A Large Prospective Population Based Cohort Study. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1373–1380. [Google Scholar] [CrossRef] [Green Version]
- Greenland, S. Quantitative methods in the review of epidemiologic literature1. Epidemiol. Rev. 1987, 9, 1–30. [Google Scholar] [CrossRef]
- Van Houwelingen, H.C.; Arends, L.R.; Stijnen, T. Advanced methods in meta-analysis: Multivariate approach and meta-regression. Stat. Med. 2002, 21, 589–624. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Macaskill, P.; Walter, S.D.; Irwig, L. A comparison of methods to detect publication bias in meta-analysis. Stat. Med. 2001, 20, 641–654. [Google Scholar] [CrossRef]
- Diergaarde, B.; Braam, H.; Vasen, H.F.; Nagengast, F.M.; Van Muijen, G.N.; Kok, F.J.; Kampman, E. Environmental Factors and Colorectal Tumor Risk in Individuals with Hereditary Nonpolyposis Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2007, 5, 736–742.e1. [Google Scholar] [CrossRef] [PubMed]
- Botma, A.; Nagengast, F.M.; Braem, M.G.; Hendriks, J.C.M.; Kleibeuker, J.H.; Vasen, H.F.; Kampman, E. Body Mass Index Increases Risk of Colorectal Adenomas in Men With Lynch Syndrome: The GEOLynch Cohort Study. J. Clin. Oncol. 2010, 28, 4346–4353. [Google Scholar] [CrossRef] [PubMed]
- Win, A.K.; Dowty, J.G.; English, D.R.; Campbell, P.T.; Young, J.P.; Winship, I.; A Macrae, F.; Lipton, L.; Parry, S.; Young, G.P.; et al. Body mass index in early adulthood and colorectal cancer risk for carriers and non-carriers of germline mutations in DNA mismatch repair genes. Br. J. Cancer 2011, 105, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Movahedi, M.; Bishop, D.T.; Macrae, F.; Mecklin, J.; Moeslein, G.; Olschwang, S.; Eccles, D.; Evans, D.G.; Maher, E.R.; Bertario, L. Obesity, Aspirin, and Risk of Colorectal Cancer in Carriers of Hereditary Colorectal Cancer: A Prospective Investigation in the CAPP2 Study. J. Clin. Oncol. 2015. [Google Scholar] [CrossRef]
- Campbell, P.T.; Cotterchio, M.; Dicks, E.; Parfrey, P.; Gallinger, S.; McLaughlin, J.R. Excess Body Weight and Colorectal Cancer Risk in Canada: Associations in Subgroups of Clinically Defined Familial Risk of Cancer. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1735–1744. [Google Scholar] [CrossRef] [Green Version]
- Hampel, H.; de la Chapelle, A. How do we Approach the Goal of Identifying Everybody with Lynch Syndrome? Fam. Cancer 2013, 12, 313–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tognetto, A.; Pastorino, R.; Castorina, S.; Condorelli, D.F.; DeCensi, A.; De Vito, C.; Magnano, A.; Scaldaferri, F.; Villari, P.; Genuardi, M.; et al. The Current Practice of Lynch Syndrome Diagnosis and Management in Italy: A Qualitative Assessment. Public. Health Genom. 2019, 22, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Valentin, M.; Sampson, J.R.; Seppälä, T.T.; Ten Broeke, S.W.; Plazzer, J.; Nakken, S.; Engel, C.; Aretz, S.; Jenkins, M.A.; Sunde, L. Cancer Risks by Gene, Age, and Gender in 6350 Carriers of Pathogenic Mismatch Repair Variants: Findings from the Prospective Lynch Syndrome Database. Genet. Med. 2020, 22, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Xue, K.; Li, F.; Chen, Y.; Zhou, Y.; He, J. Body Mass Index and the Risk of Cancer in Women Compared with Men: A Meta-Analysis of Prospective Cohort Studies. Eur. J. Cancer Prev. 2017, 26, 94–105. [Google Scholar] [CrossRef]
- Terrazas, S.; Brashear, L.; Escoto, A.; Lynch, S.; Slaughter, D.; Xavier, N.; Estes, N.R., II; Giordano-Mooga, S. Sex Differences in Obesity-Induced Inflammation. In Translational Studies on Inflammation; Anonymous, Ed.; IntechOpen: London, UK, 2019. [Google Scholar]
- Ecaiazza, F.; Ryan, E.J.; Doherty, G.; Winter, D.C.; Esheahan, K. Estrogen Receptors and Their Implications in Colorectal Carcinogenesis. Front. Oncol. 2015, 5, 19. [Google Scholar] [CrossRef]
- Lu, K.H.; Dinh, M.; Kohlmann, W.; Watson, P.; Green, J.; Syngal, S.; Bandipalliam, P.; Chen, L.-M.; Allen, B.; Conrad, P.; et al. Gynecologic Cancer as a “Sentinel Cancer” for Women with Hereditary Nonpolyposis Colorectal Cancer Syndrome. Obstet. Gynecol. 2005, 105, 569–574. [Google Scholar] [CrossRef]
- Engel, C.; Ahadova, A.; Seppälä, T.; Aretz, S.; Bigirwamungu-Bargeman, M.; Bläker, H.; Bucksch, K.; Büttner, R.; Endris, V.; Holinski-Feder, E. Associations of Pathogenic Variants in MLH1, MSH2, and MSH6 with Risk of Colorectal Adenomas and Tumors and with Somatic Mutations in Patients with Lynch Syndrome. Gastroenterology 2020, 158, 1326–1333. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, T.; Kuchiba, A.; Lochhead, P.; Nishihara, R.; Yamauchi, M.; Imamura, Y.; Liao, X.; Qian, Z.R.; Ng, K.; Chan, A.T.; et al. Prospective Analysis of Body Mass Index, Physical Activity, and Colorectal Cancer Risk Associated with Beta-Catenin (CTNNB1) Status. Cancer Res. 2013, 73, 1600–1610. [Google Scholar] [CrossRef] [Green Version]
- Burn, J.; Mathers, J.C.; Bishop, D.T. Chemoprevention in Lynch syndrome. Fam. Cancer 2013, 12, 707–718. [Google Scholar] [CrossRef]
- Afshar, S.; Malcomson, F.; Kelly, S.B.; Seymour, K.; Woodcock, S.; Mathers, J.C. Biomarkers of Colorectal Cancer Risk Decrease 6 months After Roux-en-Y Gastric Bypass Surgery. Obes. Surg. 2018, 28, 945–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lean, M.E.J.; Astrup, A.; Roberts, S.B. Making progress on the global crisis of obesity and weight management. BMJ 2018, 361, k2538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.S.; Dunlop, J.; Gallant, S.; Macleod, M.; Miedzybrodzka, Z.; Mutrie, N.; O’Carroll, R.E.; Stead, M.; Steele, R.J.C.; Taylor, R.S.; et al. Feasibility Study to Assess the Impact of a Lifestyle Intervention (’LivingWELL’) in People hav-ing an Assessment of their Family History of Colorectal Or Breast Cancer. BMJ Open 2018, 8, e019410. [Google Scholar] [CrossRef] [PubMed]
- Lassale, C.; Péneau, S.; Touvier, M.; Julia, C.; Galan, P.; Hercberg, S.; Kesse-Guyot, E. Validity of Web-Based Self-Reported Weight and Height: Results of the Nutrinet-Santé Study. J. Med. Internet Res. 2013, 15, e152. [Google Scholar] [CrossRef] [Green Version]
- De Jong, A.E.; Morreau, H.; Van Puijenbroek, M.; Eilers, P.H.; Wijnen, J.; Nagengast, F.M.; Griffioen, G.; Cats, A.; Menko, F.H.; Kleibeuker, J.H.; et al. The role of mismatch repair gene defects in the development of adenomas in patients with HNPCC. Gastroenterology 2004, 126, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Almazeedi, S.; El-Abd, R.; Al-Khamis, A.; Albatineh, A.N.; Al-Sabah, S. Role of bariatric surgery in reducing the risk of colorectal cancer: A meta-analysis. BJS 2020, 107, 348–354. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| FA | PY | Study Names | Country | Study Design | Controls/Size Cohort | Cases/Events | Contrast | Inclusion Criteria |
|---|---|---|---|---|---|---|---|---|
| Campbell | 2007 | Canada | CC | 2668 | 927 | Obese vs. normal, current weight | Member of AC-I or RBG families | |
| Botma * | 2010 | GEOLynch | The Netherlands | Cohort | 243 | 22 | Obese/overweight vs. normal, current weight | MLH1, MSH2, MSH6, PMS2 carriers |
| Win | 2011 | CCFR | Australia, North America | Cohort | 1324 | 659 | Obese vs. normal, at age 20 | MLH1, MSH2, MSH6, PMS2 carriers |
| Movahedi | 2015 | CAPP2 trial | Australia, China, Europe, South Africa, USA | Cohort | 896 | 54 | Obese vs. normal, current weight | MLH1, MSH2, MSH6 carriers or AC-I families |
| Author, PY | Data Source | Country | Study Design | Outcome | BMI Evaluation | Gene | HR (95%CI) |
|---|---|---|---|---|---|---|---|
| Botma et al. 2010 | GEOLynch | Netherlands | Cohort study | Colorectal Adenoma | Per 5 kg/m2, current Overweight or obese vs. normal, current | MLH1 | 1.39 (0.70–2.76) * |
| MSH2 | 1.14 (0.47–2.74) * | ||||||
| MSH6 | 2.77 (0.19–40.27) * | ||||||
| MLH1 | 2.64 (0.47–14.89) * | ||||||
| MSH2 | 1.08 (0.21–5.73) * | ||||||
| MSH6 | 4.69 (0.62–35.61) * | ||||||
| Movahedi et al. 2015 | CAPP2 trial | Australia, China, Europe, South Africa, USA | Cohort study | CRC | Per 1 kg/m2, current Overweight vs. normal, current Obese vs. normal, current | MLH1 | 1.12 (1.04–1.21) + |
| MSH2 | 1.01 (0.91–1.12) + | ||||||
| MLH1 | 1.19 (0.47–3.01) + | ||||||
| MSH2 | 1.26 (0.44–3.60) + | ||||||
| MLH1 | 3.72 (1.41–9.81) + | ||||||
| MSH2 | 1.59 (0.47–5.44) + | ||||||
| Win et al. 2011 | CCFR | Australia, North America | Cohort study | CRC | Per 5 kg/m2, at age 20 | MLH1 | 1.36 (1.04–1.77) # |
| MSH2 | 1.28 (0.96–1.70) # | ||||||
| MSH6 | 0.84 (0.38–1.80) # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazzeroni, M.; Bellerba, F.; Calvello, M.; Macrae, F.; Win, A.K.; Jenkins, M.; Serrano, D.; Marabelli, M.; Cagnacci, S.; Tolva, G.; et al. A Meta-Analysis of Obesity and Risk of Colorectal Cancer in Patients with Lynch Syndrome: The Impact of Sex and Genetics. Nutrients 2021, 13, 1736. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051736
Lazzeroni M, Bellerba F, Calvello M, Macrae F, Win AK, Jenkins M, Serrano D, Marabelli M, Cagnacci S, Tolva G, et al. A Meta-Analysis of Obesity and Risk of Colorectal Cancer in Patients with Lynch Syndrome: The Impact of Sex and Genetics. Nutrients. 2021; 13(5):1736. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051736
Chicago/Turabian StyleLazzeroni, Matteo, Federica Bellerba, Mariarosaria Calvello, Finlay Macrae, Aung Ko Win, Mark Jenkins, Davide Serrano, Monica Marabelli, Sara Cagnacci, Gianluca Tolva, and et al. 2021. "A Meta-Analysis of Obesity and Risk of Colorectal Cancer in Patients with Lynch Syndrome: The Impact of Sex and Genetics" Nutrients 13, no. 5: 1736. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051736