
Triglyceride-Rich Lipoproteins and Their Remnants as Silent Promoters of Atherosclerotic Cardiovascular Disease and Other Metabolic Disorders: A Review



Abstract
:1. Epidemiological Background
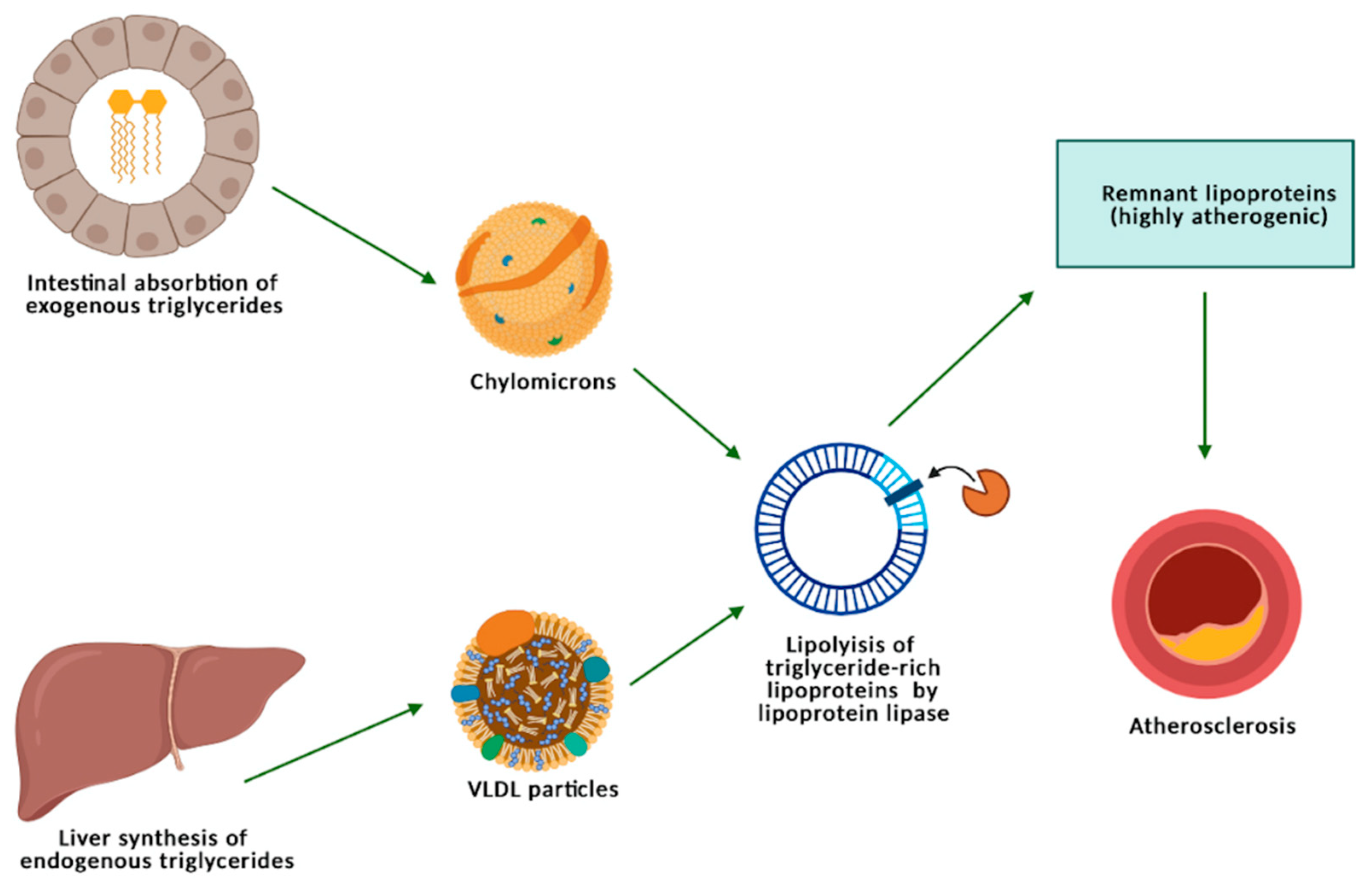
2. Metabolism of Triglycerides, Triglyceride-Rich Lipoproteins, and Remnants
3. The Association between Triglyceride-Rich Lipoproteins and Peripheral Artery Disease
4. The Linkage between Triglycerides and Atherosclerotic Cerebrovascular Disease
5. An Insight into Other Implications of Hypertriglyceridemia, Beyond Atherosclerosis
6. New Therapeutic Perspectives for Hypertriglyceridemia
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mourikis, P.; Zako, S.; Dannenberg, L.; Nia, A.M.; Heinen, Y.; Busch, L.; Richter, H.; Hohlfeld, T.; Zeus, T.; Kelm, M.; et al. Lipid lowering therapy in cardiovascular disease: From myth to molecular reality. Pharmacol. Ther. 2020, 213, 107592. [Google Scholar] [CrossRef]
- van der Ende, M.Y.; Hartman, M.H.; Hagemeijer, Y.; Meems, L.M.; de Vries, H.S.; Stolk, R.P.; de Boer, R.A.; Sijtsma, A.; van der Meer, P.; Rienstra, M.; et al. The LifeLines Cohort Study: Prevalence and treatment of cardiovascular disease and risk factors. Int. J. Cardiol. 2017, 228, 495–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiner, Ž. Hypertriglyceridaemia and risk of coronary artery disease. Nat. Rev. Cardiol. 2017, 14, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Carroll, M.; Kit, B.; Lacher, D. Trends in Elevated Triglyceride in Adults: United States, 2001–2012; NCHS Data Brief; National Center for Health Statistics, United States of America (USA): Hyattsville, MD, USA, 2015; Volume 198. [Google Scholar]
- Aberra, T.; Peterson, E.D.; Pagidipati, N.J.; Mulder, H.; Wojdyla, D.M.; Philip, S.; Granowitz, C.; Navar, A.M. The association between triglycerides and incident cardiovascular disease: What is “optimal”? J. Clin. Lipidol. 2020, 14, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P. Triglyceride-rich lipoproteins as a causal factor for cardiovascular disease. Vasc. Health Risk Manag. 2016, 12, 171–183. [Google Scholar] [CrossRef] [Green Version]
- Boden, W.E.; Bhatt, D.L.; Toth, P.P.; Ray, K.K.; Chapman, M.J.; Lüscher, T.F. Profound reductions in first and total cardiovascular events with icosapent ethyl in the REDUCE-IT trial: Why these results usher in a new era in dyslipidaemia therapeutics. Eur. Heart J. 2020, 41, 2304–2312. [Google Scholar] [CrossRef] [Green Version]
- Tada, H.; Nomura, A.; Yoshimura, K.; Itoh, H.; Komuro, I.; Yamagishi, M.; Takamura, M.; Kawashiri, M.A. Fasting and Non-Fasting Triglycerides and Risk of Cardiovascular Events in Diabetic Patients under Statin Therapy. Circ. J. 2020, 84, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Park, J.B.; Hwang, I.C.; Yoon, Y.E.; Park, H.E.; Choi, S.Y.; Kim, Y.J.; Cho, G.Y.; Han, K.; Kim, H.K. Association of four lipid components with mortality, myocardial infarction, and stroke in statin-naïve young adults: A nationwide cohort study. Eur. J. Prev. Cardiol. 2020, 27, 870–881. [Google Scholar] [CrossRef]
- Kaneko, H.; Itoh, H.; Kiriyama, H.; Kamon, T.; Fujiu, K.; Morita, K.; Michihata, N.; Jo, T.; Takeda, N.; Morita, H.; et al. Lipid Profile and Subsequent Cardiovascular Disease among Young Adults Aged < 50 Years. Am. J. Cardiol. 2021, 142, 59–65. [Google Scholar] [CrossRef]
- Burnett, J.R.; Hooper, A.J.; Hegele, R.A. Remnant Cholesterol and Atherosclerotic Cardiovascular Disease Risk. J. Am. Coll. Cardiol. 2020, 76, 2736–2739. [Google Scholar] [CrossRef]
- Krysa, J.A.; Vine, D.F.; Beilin, L.J.; Burrows, S.; Huang, R.C.; Mori, T.A.; Proctor, S.D. ApoB48-remnant lipoproteins are associated with increased cardiometabolic risk in adolescents. Atherosclerosis 2020, 302, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Generoso, G.; Janovsky, C.; Bittencourt, M.S. Triglycerides and triglyceride-rich lipoproteins in the development and progression of atherosclerosis. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Packard, C.J.; Boren, J.; Taskinen, M.R. Causes and Consequences of Hypertriglyceridemia. Front. Endocrinol. 2020, 11, 252. [Google Scholar] [CrossRef] [PubMed]
- Borén, J.; Williams, K.J. The central role of arterial retention of cholesterol-rich apolipoprotein-B-containing lipoproteins in the pathogenesis of atherosclerosis: A triumph of simplicity. Curr. Opin. Lipidol. 2016, 27, 473–483. [Google Scholar] [CrossRef]
- Hussain, A.; Ballantyne, C.M.; Saeed, A.; Virani, S.S. Triglycerides and ASCVD Risk Reduction: Recent Insights and Future Directions. Curr. Atheroscler. Rep. 2020, 22, 25. [Google Scholar] [CrossRef]
- Nakajima, K.; Nakano, T.; Tanaka, A. The oxidative modification hypothesis of atherosclerosis: The comparison of atherogenic effects on oxidized LDL and remnant lipoproteins in plasma. Clin. Chim. Acta 2006, 367, 36–47. [Google Scholar] [CrossRef]
- Nakajima, K.; Saito, T.; Tamura, A.; Suzuki, M.; Nakano, T.; Adachi, M.; Tanaka, A.; Tada, N.; Nakamura, H.; Campos, E.; et al. Cholesterol in remnant-like lipoproteins in human serum using monoclonal anti apo B-100 and anti apo A-I immunoaffinity mixed gels. Clin. Chim. Acta 1993, 223, 53–71. [Google Scholar] [CrossRef]
- Shin, H.K.; Kim, Y.K.; Kim, K.Y.; Lee, J.H.; Hong, K.W. Remnant lipoprotein particles induce apoptosis in endothelial cells by NAD(P)H oxidase-mediated production of superoxide and cytokines via lectin-like oxidized low-density lipoprotein receptor-1 activation: Prevention by cilostazol. Circulation 2004, 109, 1022–1028. [Google Scholar] [CrossRef] [Green Version]
- Olin-Lewis, K.; Krauss, R.M.; La Belle, M.; Blanche, P.J.; Barrett, P.H.; Wight, T.N.; Chait, A. ApoC-III content of apoB-containing lipoproteins is associated with binding to the vascular proteoglycan biglycan. J. Lipid Res. 2002, 43, 1969–1977. [Google Scholar] [CrossRef] [Green Version]
- Mahley, R.W.; Huang, Y. Atherogenic remnant lipoproteins: Role for proteoglycans in trapping, transferring, and internalizing. J. Clin. Investig. 2007, 117, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Salinas, C.A.A.; Chapman, M.J. Remnant lipoproteins: Are they equal to or more atherogenic than LDL? Curr. Opin. Lipidol. 2020, 31, 132–139. [Google Scholar] [CrossRef]
- Wang, L.; Gill, R.; Pedersen, T.L.; Higgins, L.J.; Newman, J.W.; Rutledge, J.C. Triglyceride-rich lipoprotein lipolysis releases neutral and oxidized FFAs that induce endothelial cell inflammation. J. Lipid Res. 2009, 50, 204–213. [Google Scholar] [CrossRef] [Green Version]
- Doi, H.; Kugiyama, K.; Oka, H.; Sugiyama, S.; Ogata, N.; Koide, S.I.; Nakamura, S.I.; Yasue, H. Remnant lipoproteins induce proatherothrombogenic molecules in endothelial cells through a redox-sensitive mechanism. Circulation 2000, 102, 670–676. [Google Scholar] [CrossRef] [Green Version]
- Aviram, M.; Brook, J.G. Characterization of the effect of plasma lipoproteins on platelet function in vitro. Haemostasis 1983, 13, 344–350. [Google Scholar] [CrossRef]
- Olufadi, R.; Byrne, C.D. Effects of VLDL and remnant particles on platelets. Pathophysiol. Haemost. Thromb. 2006, 35, 281–291. [Google Scholar] [CrossRef]
- Langsted, A.; Madsen, C.M.; Nordestgaard, B.G. Contribution of remnant cholesterol to cardiovascular risk. J. Intern. Med. 2020, 288, 116–127. [Google Scholar] [CrossRef]
- Authors/Task Force Members; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [Green Version]
- Feng, M.; Darabi, M.; Tubeuf, E.; Canicio, A.; Lhomme, M.; Frisdal, E.; Lanfranchi-Lebreton, S.; Matheron, L.; Rached, F.; Ponnaiah, M.; et al. Free cholesterol transfer to high-density lipoprotein (HDL) upon triglyceride lipolysis underlies the U-shape relationship between HDL-cholesterol and cardiovascular disease. Eur. J. Prev. Cardiol. 2020, 27, 1606–1616. [Google Scholar] [CrossRef]
- Stock, J. Triglycerides and cardiovascular risk: Apolipoprotein B holds the key. Atherosclerosis 2019, 284, 221–222. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Sun, C.; Selvin, E.; Nambi, V.; Coresh, J.; Jia, X.; Ballantyne, C.M.; Hoogeveen, R.C. Triglyceride-rich lipoproteins, apolipoprotein C-III, angiopoietin-like protein 3, and cardiovascular events in older adults: Atherosclerosis Risk in Communities (ARIC) study. Eur. J. Prev. Cardiol. 2021. [Google Scholar] [CrossRef]
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef] [Green Version]
- Velescu, A.; Clara, A.; Peñafiel, J.; Grau, M.; Degano, I.R.; Martí, R.; Ramos, R.; Marrugat, J.; Elosua, R. Peripheral Arterial Disease Incidence and Associated Risk Factors in a Mediterranean Population-based Cohort. The REGICOR Study. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 696–705. [Google Scholar] [CrossRef]
- Kou, M.; Ding, N.; Ballew, S.H.; Salameh, M.J.; Martin, S.S.; Selvin, E.; Heiss, G.; Ballantyne, C.M.; Matsushita, K.; Hoogeveen, R.C. Conventional and Novel Lipid Measures and Risk of Peripheral Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1229–1238. [Google Scholar] [CrossRef]
- Toth, P.P.; Hull, M.; Granowitz, C.; Philip, S. Real-world analyses of patients with elevated atherosclerotic cardiovascular disease risk from the Optum Research Database. Future Cardiol. 2020. [Google Scholar] [CrossRef]
- Ding, C.; Chen, Y.; Shi, Y.; Li, M.; Hu, L.; Zhou, W.; Wang, T.; Zhu, L.; Huang, X.; Bao, H.; et al. Association between nontraditional lipid profiles and peripheral arterial disease in Chinese adults with hypertension. Lipids Health Dis. 2020, 19, 231. [Google Scholar] [CrossRef] [PubMed]
- Alizargar, J.; Bai, C.H.; Hsieh, N.C.; Wu, S.V. Use of the triglyceride-glucose index (TyG) in cardiovascular disease patients. Cardiovasc. Diabetol. 2020, 19, 8. [Google Scholar] [CrossRef] [Green Version]
- da Silva, A.; Caldas, A.P.S.; Hermsdorff, H.H.M.; Bersch-Ferreira, Â.C.; Torreglosa, C.R.; Weber, B.; Bressan, J. Triglyceride-glucose index is associated with symptomatic coronary artery disease in patients in secondary care. Cardiovasc. Diabetol. 2019, 18, 89. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Han, K.; Park, C.Y. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: A population-based study. BMC Med. 2020, 18, 361. [Google Scholar] [CrossRef]
- Duran Karaduman, B.; Ayhan, H.; Keleş, T.; Bozkurt, E. The triglyceride-glucose index predicts peripheral artery disease complexity. Turk. J. Med. Sci. 2020, 50, 1217–1222. [Google Scholar] [CrossRef]
- Mesut, E.; Cihan, A.; Orhan, G. Is it possible to predict the complexity of peripheral artery disease with atherogenic index? Vascular 2020, 28, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, B.E.; Koopal, C.; Bots, M.L.; Asselbergs, F.W.; Westerink, J.; Visseren, F.L.J. The relation between VLDL-cholesterol and risk of cardiovascular events in patients with manifest cardiovascular disease. Int. J. Cardiol. 2021, 322, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Duran, E.K.; Aday, A.W.; Cook, N.R.; Buring, J.E.; Ridker, P.M.; Pradhan, A.D. Triglyceride-Rich Lipoprotein Cholesterol, Small Dense LDL Cholesterol, and Incident Cardiovascular Disease. J. Am. Coll. Cardiol. 2020, 75, 2122–2135. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Tang, B.; Zheng, J.; Larsson, S.C. Circulating Lipoprotein Lipids, Apolipoproteins and Ischemic Stroke. Ann. Neurol. 2020, 88, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.W.; Kwon, H.M.; Jeong, H.Y.; Park, J.H.; Kwon, H.; Jeong, S.M. High triglyceride-glucose index is associated with subclinical cerebral small vessel disease in a healthy population: A cross-sectional study. Cardiovasc. Diabetol. 2020, 19, 53. [Google Scholar] [CrossRef]
- Zhou, Y.; Pan, Y.; Yan, H.; Wang, Y.; Li, Z.; Zhao, X.; Li, H.; Meng, X.; Wang, C.; Liu, L.; et al. Triglyceride Glucose Index and Prognosis of Patients With Ischemic Stroke. Front. Neurol. 2020, 11, 456. [Google Scholar] [CrossRef]
- Masson, W.; Siniawski, D.; Lobo, M.; Molinero, G.; Huerín, M. Association between triglyceride/HDL cholesterol ratio and carotid atherosclerosis in postmenopausal middle-aged women. Endocrinol. Nutr. 2016, 63, 327–332. [Google Scholar] [CrossRef]
- Nam, K.W.; Kwon, H.M.; Jeong, H.Y.; Park, J.H.; Kwon, H.; Jeong, S.M. High triglyceride/HDL cholesterol ratio is associated with silent brain infarcts in a healthy population. BMC Neurol. 2019, 19, 147. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Mai, J.; Li, Y.; Guo, M.; Wu, Y.; Gao, X.; Wu, Y.; Liu, X.; Zhao, L. Triglyceride to high-density lipoprotein cholesterol ratio and risk of atherosclerotic cardiovascular disease in a Chinese population. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1706–1713. [Google Scholar] [CrossRef]
- Garg, R.; Knox, N.; Prasad, S.; Zinzuwadia, S.; Rech, M.A. The Atherogenic Index of Plasma is Independently Associated with Symptomatic Carotid Artery Stenosis. J. Stroke Cerebrovasc. 2020, 29, 105351. [Google Scholar] [CrossRef]
- Ahn, S.S.; Lee, L.E.; Pyo, J.Y.; Song, J.J.; Park, Y.B.; Lee, S.W. Atherogenic index of plasma predicts cerebrovascular accident occurrence in antineutrophil cytoplasmic antibody-associated vasculitis. Lipids Health Dis. 2020, 19, 184. [Google Scholar] [CrossRef]
- Aung, N.; Sanghvi, M.M.; Piechnik, S.K.; Neubauer, S.; Munroe, P.B.; Petersen, S.E. The Effect of Blood Lipids on the Left Ventricle: A Mendelian Randomization Study. J. Am. Coll. Cardiol. 2020, 76, 2477–2488. [Google Scholar] [CrossRef]
- Sascău, R.; Zota, I.M.; Stătescu, C.; Boișteanu, D.; Roca, M.; Maștaleru, A.; Leon Constantin, M.M.; Vasilcu, T.F.; Gavril, R.S.; Mitu, F. Review of Echocardiographic Findings in Patients with Obstructive Sleep Apnea. Can. Respir. J. 2018, 2018, 1206217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaltoft, M.; Langsted, A.; Nordestgaard, B.G. Triglycerides and remnant cholesterol associated with risk of aortic valve stenosis: Mendelian randomization in the Copenhagen General Population Study. Eur. Heart J. 2020, 41, 2288–2299. [Google Scholar] [CrossRef] [PubMed]
- Hartz, J.; Krauss, R.M.; Göttsater, M.; Melander, O.; Nilsson, P.; Mietus-Snyder, M. Lipoprotein Particle Predictors of Arterial Stiffness after 17 Years of Follow Up: The Malmö Diet and Cancer Study. Int. J. Vasc. Med. 2020, 2020, 4219180. [Google Scholar] [CrossRef] [PubMed]
- Lăcătușu, C.M.; Grigorescu, E.D.; Stătescu, C.; Sascău, R.A.; Onofriescu, A.; Mihai, B.M. Association of Antihyperglycemic Therapy with Risk of Atrial Fibrillation and Stroke in Diabetic Patients. Medicana 2019, 55, 592. [Google Scholar] [CrossRef] [Green Version]
- Lim, T.K.; Lee, H.S.; Lee, Y.J. Triglyceride to HDL-cholesterol ratio and the incidence risk of type 2 diabetes in community dwelling adults: A longitudinal 12-year analysis of the Korean Genome and Epidemiology Study. Diabetes Res. Clin. Pract. 2020, 163, 108150. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, G.; Cheng, T.; Liu, J.; Song, G.; Ma, H. Association between triglyceride-glucose index and risk of incident diabetes: A secondary analysis based on a Chinese cohort study: TyG index and incident diabetes. Lipids Health Dis. 2020, 19, 236. [Google Scholar] [CrossRef]
- Wang, C.; Wang, L.; Liang, K.; Yan, F.; Hou, X.; Liu, F.; Chen, L. Poor Control of Plasma Triglycerides Is Associated with Early Decline of Estimated Glomerular Filtration Rates in New-Onset Type 2 Diabetes in China: Results from a 3-Year Follow-Up Study. J. Diabetes Res. 2020, 2020, 3613041. [Google Scholar] [CrossRef]
- Russo, G.T.; De Cosmo, S.; Viazzi, F.; Pacilli, A.; Ceriello, A.; Genovese, S.; Guida, P.; Giorda, C.; Cucinotta, D.; Pontremoli, R.; et al. Plasma Triglycerides and HDL-C Levels Predict the Development of Diabetic Kidney Disease in Subjects with Type 2 Diabetes: The AMD Annals Initiative. Diabetes Care 2016, 39, 2278–2287. [Google Scholar] [CrossRef] [Green Version]
- Kaze, A.D.; Santhanam, P.; Musani, S.K.; Ahima, R.; Echouffo-Tcheugui, J.B. Metabolic Dyslipidemia and Cardiovascular Outcomes in Type 2 Diabetes Mellitus: Findings From the Look AHEAD Study. J. Am. Heart Assoc. 2021, 10, e016947. [Google Scholar] [CrossRef]
- Mantovani, A.; Danese, E.; Salvagno, G.L.; Gelati, M.; Turino, T.; Bovo, C.; Lippi, G.; Targher, G. Association between lower plasma adiponectin levels and higher plasma thrombin generation parameters in men with type 2 diabetes: Role of plasma triglycerides. J. Endocrinol. Investig. 2021, 44, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Anghel, L.; Sascău, R.; Radu, R.; Stătescu, C. From Classical Laboratory Parameters to Novel Biomarkers for the Diagnosis of Venous Thrombosis. Int. J. Mol. Sci. 2020, 21, 1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunninghake, D.B.; Stein, E.A.; Bays, H.E.; Rader, D.J.; Chitra, R.R.; Simonson, S.G.; Schneck, D.W. Rosuvastatin improves the atherogenic and atheroprotective lipid profiles in patients with hypertriglyceridemia. Coron. Artery Dis. 2004, 15, 115–123. [Google Scholar] [CrossRef]
- Gupta, M.; Blumenthal, C.; Chatterjee, S.; Bandyopadhyay, D.; Jain, V.; Lavie, C.J.; Virani, S.S.; Ray, K.K.; Aronow, W.S.; Ghosh, R.K. Novel emerging therapies in atherosclerosis targeting lipid metabolism. Expert Opin. Investig. Drugs 2020, 29, 611–622. [Google Scholar] [CrossRef]
- Nurmohamed, N.S.; Dallinga-Thie, G.M.; Stroes, E.S.G. Targeting apoC-III and ANGPTL3 in the treatment of hypertriglyceridemia. Expert Rev. Cardiovasc. Ther. 2020, 18, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Araki, E.; Yamashita, S.; Arai, H.; Yokote, K.; Satoh, J.; Inoguchi, T.; Nakamura, J.; Maegawa, H.; Yoshioka, N.; Tanizawa, Y.; et al. Efficacy and safety of pemafibrate in people with type 2 diabetes and elevated triglyceride levels: 52-week data from the PROVIDE study. Diabetes Obes. Metab. 2019, 21, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Yamashita, S.; Yokote, K.; Araki, E.; Suganami, H.; Ishibashi, S. Efficacy and Safety of Pemafibrate Versus Fenofibrate in Patients with High Triglyceride and Low HDL Cholesterol Levels: A Multicenter, Placebo-Controlled, Double-Blind, Randomized Trial. J. Atheroscler. Thromb. 2018, 25, 521–538. [Google Scholar] [CrossRef] [Green Version]
- Pandor, A.; Ara, R.M.; Tumur, I.; Wilkinson, A.J.; Paisley, S.; Duenas, A.; Durrington, P.N.; Chilcott, J. Ezetimibe monotherapy for cholesterol lowering in 2722 people: Systematic review and meta-analysis of randomized controlled trials. J. Intern. Med. 2009, 265, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Vallejo-Vaz, A.J.; Corral, P.; Schreier, L.; Ray, K.K. Triglycerides and residual risk. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Ferrières, J. The return of triglycerides and revival of omega-3 fatty acids! Arch. Cardiovasc. Dis. 2020, 113, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Wong, N.D.; Fan, W.; Philip, S.; Granowitz, C.; Toth, P.P. REDUCE-IT Eligibility and Preventable Cardiovascular Events in the US Population (from the National Health and Nutrition Examination Survey [NHANES]). Am. J. Cardiol. 2020, 134, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; Cox, J.; et al. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- Fukumoto, K.; Takemoto, Y.; Yoshikawa, J.; Norioka, N.; Iguchi, T.; Namikawa, H.; Tochino, Y.; Yoshiyama, M.; Shuto, T. Predictors of endothelial function improvement in patients with mild hypertriglyceridemia without evidence of coronary artery disease treated with purified eicosapentaenoic acid. Atherosclerosis 2020, 309, 27–32. [Google Scholar] [CrossRef]
- Zhang, X.; Stiekema, L.C.A.; Stroes, E.S.G.; Groen, A.K. Metabolic effects of PCSK9 inhibition with Evolocumab in subjects with elevated Lp(a). Lipids Health Dis. 2020, 19, 91. [Google Scholar] [CrossRef]
- Taskinen, M.R.; Björnson, E.; Kahri, J.; Söderlund, S.; Matikainen, N.; Porthan, K.; Ainola, M.; Hakkarainen, A.; Lundbom, N.; Fermanelli, V.; et al. Effects of Evolocumab on the Postprandial Kinetics of Apo (Apolipoprotein) B100- and B48-Containing Lipoproteins in Subjects with Type 2 Diabetes. Arterioscler. Thromb. Vasc. Biol. 2020. [Google Scholar] [CrossRef]
- Wolska, A.; Yang, Z.H.; Remaley, A.T. Hypertriglyceridemia: New approaches in management and treatment. Curr. Opin. Lipidol. 2020, 31, 331–339. [Google Scholar] [CrossRef]
- Esan, O.; Wierzbicki, A.S. Volanesorsen in the Treatment of Familial Chylomicronemia Syndrome or Hypertriglyceridaemia: Design, Development and Place in Therapy. Drug Des. Dev. Ther. 2020, 14, 2623–2636. [Google Scholar] [CrossRef]
- Witztum, J.L.; Gaudet, D.; Freedman, S.D.; Alexander, V.J.; Digenio, A.; Williams, K.R.; Yang, Q.; Hughes, S.G.; Geary, R.S.; Arca, M.; et al. Volanesorsen and Triglyceride Levels in Familial Chylomicronemia Syndrome. N. Engl. J. Med. 2019, 381, 531–542. [Google Scholar] [CrossRef]
- Raal, F.J.; Kallend, D.; Ray, K.K.; Turner, T.; Koenig, W.; Wright, R.S.; Wijngaard, P.L.J.; Curcio, D.; Jaros, M.J.; Leiter, L.A.; et al. Inclisiran for the Treatment of Heterozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 382, 1520–1530. [Google Scholar] [CrossRef]
- Ray, K.K.; Wright, R.S.; Kallend, D.; Koenig, W.; Leiter, L.A.; Raal, F.J.; Bisch, J.A.; Richardson, T.; Jaros, M.; Wijngaard, P.L.J.; et al. Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol. N. Engl. J. Med. 2020, 382, 1507–1519. [Google Scholar] [CrossRef]
- Taskinen, M.R.; Björnson, E.; Matikainen, N.; Söderlund, S.; Pietiläinen, K.H.; Ainola, M.; Hakkarainen, A.; Lundbom, N.; Fuchs, J.; Thorsell, A.; et al. Effects of liraglutide on the metabolism of triglyceride-rich lipoproteins in type 2 diabetes. Diabetes Obes. Metab. 2021. [Google Scholar] [CrossRef]
- Sawada, T.; Uzu, K.; Hashimoto, N.; Onishi, T.; Takaya, T.; Shimane, A.; Taniguchi, Y.; Yasaka, Y.; Ohara, T.; Kawai, H. Empagliflozin’s Ameliorating Effect on Plasma Triglycerides: Association with Endothelial Function Recovery in Diabetic Patients with Coronary Artery Disease. J. Atheroscler. Thromb. 2020, 27, 644–656. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Drug | Action on TGs Levels |
|---|---|
| Statins | Lower TGs levels by 20% [18,54] First-line therapy |
| Fibrates (e.g., pemafibrate) | The most potent drugs in managing hypertriglyceridemia Produce a decrease of up to 50% in TGs concentrations [58] Pemafibrate is non-inferior to other fibrates and has a more favorable safety profile Their potency to decrease overall cardiovascular risk is modest |
| Omega 3 fatty acids (e.g., Icosapent Ethyl) | Demonstrated a 25% relative risk reduction in adverse cardiovascular events both in primary and secondary prevention when administrated at a high dose [63] Exert a beneficial effect on endothelial function assessed via flow-mediated dilation [66] |
| Ezetimibe | Produces only a slight decrease in TGs levels [59] |
| PCSK9 inhibitors (e.g., evolocumab) | Controversial data Reduction in VLDL, IDL, LDL, and Lp(a) levels The decrease in VLDL levels is dependent on baseline Lp(a) values [67] The lowering effect is more pronounced on VLDL2 levels than on VLDL1 [68] |
| Volanesorsen | A second-generation chimeric antisense therapeutic oligonucleotide that decreases plasma apoCIII and TGs levels in a dose-dependent manner [71] |
| Inclisiran | Small interfering RNA agent Majorly effective in reducing LDL concentration but also lowered TGs levels in ORION 9, 10, and 11 trials [72,73] |
| GLP-1 receptor agonists (e.g., liraglutide) | Decreases apoB48 synthesis in CMs Apparently decreased production of atherogenic remnants in diabetic patients [74] |
| SGLT2 inhibitors (e.g., empagliflozin) | Decrease in fasting and post-prandial TGs concentration and a flow-mediated dilation improvement [75] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sascău, R.; Clement, A.; Radu, R.; Prisacariu, C.; Stătescu, C. Triglyceride-Rich Lipoproteins and Their Remnants as Silent Promoters of Atherosclerotic Cardiovascular Disease and Other Metabolic Disorders: A Review. Nutrients 2021, 13, 1774. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061774
Sascău R, Clement A, Radu R, Prisacariu C, Stătescu C. Triglyceride-Rich Lipoproteins and Their Remnants as Silent Promoters of Atherosclerotic Cardiovascular Disease and Other Metabolic Disorders: A Review. Nutrients. 2021; 13(6):1774. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061774
Chicago/Turabian StyleSascău, Radu, Alexandra Clement, Rodica Radu, Cristina Prisacariu, and Cristian Stătescu. 2021. "Triglyceride-Rich Lipoproteins and Their Remnants as Silent Promoters of Atherosclerotic Cardiovascular Disease and Other Metabolic Disorders: A Review" Nutrients 13, no. 6: 1774. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061774