
Long-Term Effect of a Gluten-Free Diet on Diarrhoea- or Bloating-Predominant Functional Bowel Disease: Role of the ‘Low-Grade Coeliac Score’ and the ‘Coeliac Lymphogram’ in the Response Rate to the Diet

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Response to a GFD
2.2. Coeliac Serology
2.3. Histological Studies
2.4. Flow Cytometry
2.5. Coeliac Genetics
2.6. Low-Grade Coeliac Score and Definition of Low-Grade Coeliac Enteropathy
2.7. Statistical Analysis
2.8. Ethical Issues
3. Results
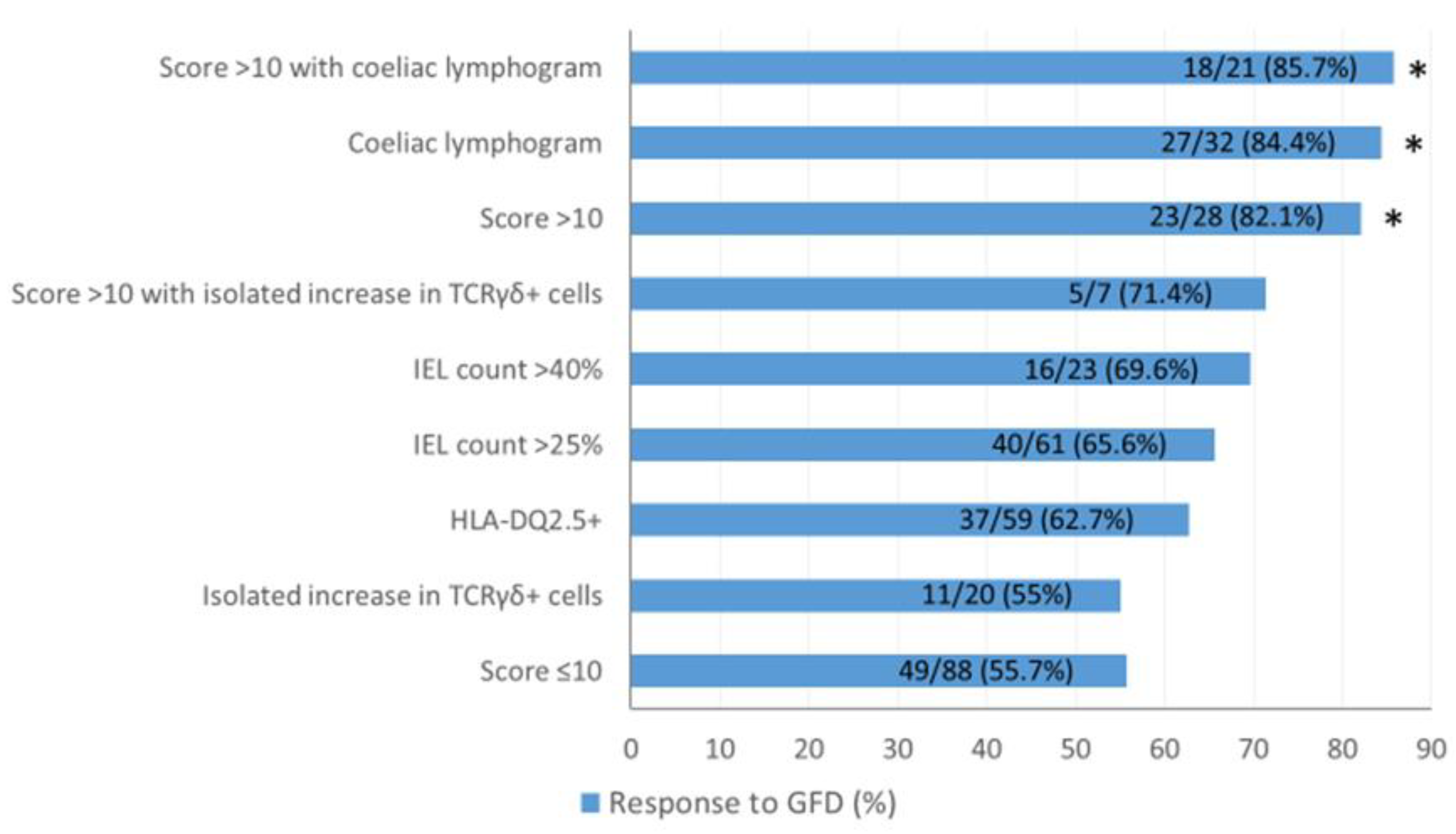
3.1. Response to Gluten-Free Diet
3.2. Frequency of Low-Grade Coeliac Enteropathy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Writing Assistance
Appendix A
Appendix A.1. Flow Cytometry
Appendix A.2. HLA Genotyping
Appendix B

{kind=link}
| Variable | GFD (n = 116) | No Diet (n = 144) | p Value |
|---|---|---|---|
| Age (years) | 42.4 ± 1.2 | 41.2 ± 1.1 | 0.48 |
| Sex (% female) | 77.6% | 64.6% | 0.022 |
| FBD type | |||
| SII-D/diarrhoea (%) Abdominal bloating (%) | 58.6% 41.4% | 58.3% 41.7% | 0.96 |
| HLA-DQ2.5+ (%) | 51.8% | 58.3% | 0.29 |
| Histology (IEL > 25%) (%) | 54.8% | 36.9% | 0.016 |
| Cytometry pattern | |||
| IEL coeliac pattern (%) | 43.8% | 11.2% | <0.0005 |
| Coeliac lymphogram (%) | 27.6% | 4.9% | <0.0005 |
| Low-grade coeliac score >10 (%) | 25% | 6.3% | <0.0005 |
| Score > 10 and coeliac lymphogram (%) | 18.1% | 2% | <0.0001 |
References
- Mearin, F.; Lacy, B.E.; Chang, L.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J.; et al. Diagnosis of non-celiac gluten sensitivity (NCGS): The Salerno experts’ criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef] [PubMed]
- Rej, A.; Aziz, I.; Tornblom, H.; Sanders, D.S.; Simrén, M. The role of diet in irritable bowel syndrome: Implications for dietary advice. J. Intern. Med. 2019, 286, 490–502. [Google Scholar] [CrossRef] [Green Version]
- Rej, A.; Aziz, I.; Sanders, D.S. A gluten-free diet: The express route to fructan reduction. Am. J. Gastroenterol. 2019, 114, 1553. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Alaedini, A.; Bojarski, C.; Bonaz, B.; Bouma, G.; Carroccio, A.; Carroccio, A.; Castillejo, G.; De Magistris, L.; Dieterich, W.; et al. The overlapping area of non-celiac gluten sensitivity (NCGS) and wheat-sensitive irritable bowel syndrome (IBS): An update. Nutrients 2017, 9, 1268. [Google Scholar] [CrossRef] [Green Version]
- Bohn, L.; Storsrud, S.; Tornblom, H.; Bengtsson, U.; Simren, M. Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life. Am. J. Gastroenterol. 2013, 108, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Morcos, A.; Dinan, T.; Quigley, E.M. Irritable bowel syndrome: Role of food in pathogenesis and management. J. Dig. Dis. 2009, 10, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Rej, A.; Buckle, R.L.; Shaw, C.C.; Trott, N.; Aziz, I.; Sanders, D.S. Letter: The gluten-free diet as a bottom-up approach for irritable bowel syndrome. Aliment. Pharmacol. Ther. 2020, 51, 184–195. [Google Scholar] [CrossRef] [Green Version]
- Aziz, I.; Trott, N.; Briggs, R.; North, J.R.; Hadjivassiliou, M.; Sanders, D.S. Efficacy of a gluten-free diet in subjects with irritable bowel syndrome-diarrhea unaware of their HLA-DQ2/8 genotype. Clin. Gastroenterol. Hepatol. 2016, 14, 696–703. [Google Scholar] [CrossRef] [Green Version]
- Barmeyer, C.; Schumann, M.; Meyer, T.; Zielinski, C.; Zuberbier, T.; Siegmund, B.; Schulzke, J.D.; Daum, S.; Ullrich, R. Long-term response to gluten-free diet as evidence for non-celiac wheat sensitivity in one third of patients with diarrhea-dominant and mixed-type irritable bowel syndrome. Int. J. Colorectal. Dis. 2017, 32, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. ESPGHAN Working Group on Coeliac Disease Diagnosis; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef]
- Husby, S.; Murray, J.A. Gluten sensitivity: Celiac lite versus celiac like. J. Pediatr. 2014, 164, 436–438. [Google Scholar] [CrossRef] [PubMed]
- Ferch, C.C.; Chey, W.D. Irritable bowel syndrome and gluten sensitivity without celiac disease: Separating the wheat from the chaff. Gastroenterology 2012, 142, 664–666. [Google Scholar] [CrossRef]
- Mooney, P.D.; Aziz, I.; Sanders, S. Non-celiac gluten sensitivity: Clinical relevance and recommendations for future research. Neurogastroenterol. Motil. 2013, 25, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Popp, A.; Mäki, M. Gluten-Induced Extra-Intestinal Manifestations in Potential Celiac Disease—Celiac Trait. Nutrients 2019, 11, 320. [Google Scholar] [CrossRef] [Green Version]
- Kurppa, K.; Collin, P.; Viljamaa, M.; Haimila, K.; Saavalainen, P.; Partanen, J.; Laurila, K.; Huhtala, H.; Paasikivi, K.; Mäki, M.; et al. Diagnosing mild enteropathy celiac disease: A randomized, controlled clinical study. Gastroenterology 2009, 136, 816–823. [Google Scholar] [CrossRef]
- Rosinach, M.; Fernández-Bañares, F.; Carrasco, A.; Ibarra, M.; Temiño, R.; Salas, A.; Esteve, M. Double-blind randomized clinical trial: Gluten versus placebo rechallenge in patients with lymphocytic enteritis and suspected celiac disease. PLoS ONE 2016, 11, e0157879. [Google Scholar] [CrossRef]
- Fernández-Bañares, F.; Carrasco, A.; Rosinach, M.; Arau, B.; García-Puig, R.; González, C.; Tristán, E.; Zabana, Y.; Esteve, M. A scoring system for identifying patients likely to be diagnosed with low-grade coeliac enteropathy. Nutrients 2019, 11, 1050. [Google Scholar] [CrossRef] [Green Version]
- Leon, F. Flow cytometry of intestinal intraepithelial lymphocytes in celiac disease. J. Immunol. Methods 2011, 363, 177–186. [Google Scholar] [CrossRef]
- Leon, F.; Eiras, P.; Roy, G.; Camarero, C. Intestinal intraepithelial lymphocytes and anti-transglutaminase in a screening algorithm for coeliac disease. Gut 2002, 50, 740–741. [Google Scholar] [CrossRef]
- Fernández-Bañares, F.; Carrasco, A.; García-Puig, R.; Rosinach, M.; González, C.; Alsina, M.; Loras, C.; Salas, A.; Viver, J.M.; Esteve, M.; et al. Intestinal intraepithelial lymphocyte cytometric pattern is more accurate than subepithelial deposits of anti-tissue transglutaminase IgA for the diagnosis of coeliac disease in lymphocytic enteritis. PLoS ONE 2014, 9, e101249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Bañares, F.; Carrasco, A.; Martín, A.; Esteve, M. Systematic Review and Meta-Analysis: Accuracy of Both Gamma Delta+ Intraepithelial Lymphocytes and Coeliac Lymphogram Evaluated by Flow Cytometry for Coeliac Disease Diagnosis. Nutrients 2019, 11, 1992. [Google Scholar] [CrossRef] [Green Version]
- Sapone, A.; Lammers, K.M.; Casolaro, V.; Cammarota, M.; Giuliano, M.T.; De Rosa, M.; Stefanile, R.; Mazzarella, G.; Tolone, C.; Russo, M.I.; et al. Divergence of gut permeability and mucosal immune gene expression in two gluten-associated conditions: Celiac disease and gluten sensitivity. BMC Med. 2011, 9, 23. [Google Scholar] [CrossRef] [Green Version]
- Esteve, M.; Rosinach, M.; Fernández-Bañares, F.; Farré, C.; Salas, A.; Alsina, M.; Vilar, P.; Abad-Lacruz, A.; Forné, M.; Santaolalla, R.; et al. Spectrum of gluten-sensitive enteropathy in first-degree relatives of patients with coeliac disease: Clinical relevance of lymphocytic enteritis. Gut 2006, 55, 1739–1745. [Google Scholar] [CrossRef] [Green Version]
- Rosinach, M.; Esteve, M.; González, C.; Temiño, R.; Mariné, M.; Monzón, H.; Sainz, E.; Loras, C.; Espinós, J.C.; Forné, M.; et al. Lymphocytic duodenosis: Aetiology and long-term response to specific treatment. Dig. Liver Dis. 2012, 44, 643–648. [Google Scholar] [CrossRef]
- Aziz, I.; Evans, K.E.; Hopper, A.D.; Smillie, D.M.; Sanders, D.S. A prospective study into the aetiology of lymphocytic duodenosis. Aliment. Pharmacol. Ther. 2010, 32, 1392–1397. [Google Scholar] [CrossRef]
- Mansikka, E.; Hervonen, K.; Kaukinen, K.; Collin, P.; Huhtala, H.; Reunala, T.; Salmi, T. Prognosis of dermatitis herpetiformis patients with and without villous atrophy at diagnosis. Nutrients 2018, 10, 641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäki, M.; Holm, K.; Collin, P.; Savilahti, E. Increase in γ/δ T cell receptor bearing lymphocytes in normal small bowel mucosa in latent celiac disease. Gut 1991, 32, 1412–1414. [Google Scholar] [CrossRef]
- Iltanen, S.; Holm, K.; Partanen, J.; Laippala, P.; Mäki, M. Increased density of jejunal γδ+ T cells in patients having normal mucosa—Marker of operative autoimmune mechanisms? Autoimmunity 1999, 29, 1787–1791. [Google Scholar] [CrossRef]
- Fernández-Bañares, F.; Crespo, L.; Núñez, C.; López-Palacios, N.; Tristán, E.; Vivas, S.; Farrais, S.; Arau, B.; Vidal, J.; Roy, G.; et al. Gamma delta+ intraepithelial lymphocytes and coeliac lymphogram in a diagnostic approach to coeliac disease in patients with seronegative villous atrophy. Aliment. Pharmacol. Ther. 2020, 51, 699–705. [Google Scholar] [CrossRef] [Green Version]
- Pellegrino, S.; Villanacci, V.; Sansotta, N.; Scarfì, R.; Bassotti, G.; Vieni, G.; Princiotta, A.; Sferlazzas, C.; Magazzù, G.; Tuccari, G. Redefining the intraepithelial lymphocytes threshold to diagnose gluten sensitivity in patients with architecturally normal duodenal histology. Aliment. Pharmacol. Ther. 2011, 33, 697–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergi, C.; Villanacci, V.; Carroccio, A. Non-celiac wheat sensitivity: Rationality and irrationality of a gluten-free diet in individuals affected with non-celiac disease: A review. BMC Gastroenterol. 2021, 21, 5. [Google Scholar] [CrossRef] [PubMed]
- Skodje, G.I.; Sarna, V.K.; Minelle, I.H.; Rolfsen, K.L.; Muir, J.G.; Gibson, P.R.; Veierød, M.B.; Henriksen, C.; Lundin, K.E.A. Fructan, Rather Than Gluten, Induces Symptoms in Patients with Self-Reported Non-Celiac Gluten Sensitivity. Gastroenterology 2018, 154, 529–539. [Google Scholar] [CrossRef] [Green Version]
- O’Keefe, M.; Jansen, C.; Martin, L.; Williams, M.; Seamark, L.; Staudacher, H.M.; Irving, P.M.; Whelan, K.; Lomer, M.C. Long-term impact of the low-FODMAP diet on gastrointestinal symptoms, dietary intake, patient acceptability, and health care utilization in irritable bowel syndrome. Neurogastroenterol. Motil. 2018, 30, e13154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.J.; Camilleri, M.; Vanner, S.; Tuck, C. Review article: Biological mechanisms for symptom causation by individual FODMAP subgroups—the case for a more personalised approach to dietary restriction. Aliment. Pharmacol. Ther. 2019, 50, 517–529. [Google Scholar] [CrossRef]
- Paduano, D.; Cingolani, A.; Tanda, E.; Usai, P. Effect of Three Diets (Low-FODMAP, Gluten-free and Balanced) on Irritable Bowel Syndrome Symptoms and Health-Related Quality of Life. Nutrients 2019, 11, 1566. [Google Scholar] [CrossRef] [Green Version]
- Tuck, C.J.; Reed, D.E.; Muir, J.G.; Vanner, S.J. Implementation of the low FODMAP diet in functional gastrointestinal symptoms: A real-world experience. Neurogastroenterol. Motil. 2020, 32, e13730. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Moayyedi, P. Meta-analysis: Factors affecting placebo response rate in the irritable bowel syndrome. Aliment. Pharmacol. Ther. 2010, 32, 144–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Predictors | Points |
|---|---|
| Serum anti-tTG2 | |
| >20 U/mL | 10 |
| >8–20 U/mL or >2–8 U/mL plus EmA+ | 6 |
| >2 to 8 U/mL plus EmA- | 2 |
| 2 U/mL | 0 |
| IEL cytometry pattern | |
| ↑TCRγδ+ cells | 7 |
| Histology (IEL count) | |
| >25% | 5 |
| 19–25% | 0 |
| <19% | −1 |
| Coeliac genetics: | |
| DQ2.5+ | 3 |
| DQ8+/DQ2.2+/Allele DQB1 of haplotype DQ2.5+ | 0 |
| 2 alleles DQ2.5- and DQ8- | −1 |
| Total (n = 116) | Response (n = 72) | Non-Response (n = 44) | p Value | |
|---|---|---|---|---|
| Type of FBD symptoms: | ||||
| -IBS-D or functional diarrhoea -Functional bloating | 68 (58.6%) 48 (41.4%) | 39 (54.2%) 33 (45.8%) | 29 (65.9%) 15 (34.1%) | 0.21 |
| Age (mean ± SEM) | 42.4 ± 1.24 | 41.7 ± 1.6 | 43.7 ± 2 | 0.44 |
| Sex (% female) | 90 (77.6%) | 55 (76.4%) | 35 (79.5%) | 0.69 |
| Coeliac genetics: | ||||
| -HLA-DQ2.5 -HLA-DQ8 -HLA-DQ2.2 -1 allele DQ2.5 -Negative | 59 (51.8%) 32 (27.6%) 11 (5%) 7 (3.2%) 7 (3.2%) | 37 (52.9%) 22 (30.5) 6 (8.3%) 2 (2.8%) 5 (6.9%) | 22 (50%) 10 (22.7%) 5 (11.3%) 5 (11.3%) 2 (4.5%) | 0.77 |
| Serology: | ||||
| -Detectable anti-tTG2 titers (EmA neg) | 3 (2.6%) | 2 (2.8%) | 1 (2.3%) | 0.87 |
| Histology (IEL count): | ||||
| >25% 19–25% <19% | 63 (54.8%) 18 (15.7%) 35 (30.2%) | 41 (56.9%) 11 (15.3%) 19 (26.4%) | 22 (50%) 7 (15.9%) 15 (34.1%) | 0.67 |
| Coeliac IEL cytometry pattern: | ||||
| -Non-coeliac -Isolated increase in TCRγδ+ cells -Coeliac lymphogram | 64 (55.2%) 20 (17.2%) 32 (27.6%) | 34 (47.2%) 11 (15.3%) 27 (37.5%) | 30 (68.2%) 9 (20.5) 5 (11.4%) | 0.019 |
| Low-grade coeliac score > 10 | 28 (24.1%) | 23 (31.9%) | 5 (11.4%) | 0.027 |
| Score > 10 and coeliac lymphogram | 21 (18.1%) | 18 (25%) | 3 (6.8%) | 0.023 |
| Score > 10 and isolated increase in TCRγδ+ cells | 7 (6.0%) | 5 (6.9%) | 2 (4.5%) | 0.71 |
| Variable | LGCE (n = 23) | FBD-R (n = 46) | FBD-NR (n = 44) | p Value |
|---|---|---|---|---|
| Age (years) (mean ± SEM) | 44.6 ± 2.8 | 39.8 ± 1.8 | 43.7 ± 2.0 | 0.24 |
| Sex (% women) | 15 (65.2%) | 38 (82.6%) | 35 (79.5%) | 0.25 |
| Type of FBD: | ||||
| -IBS-D/functional diarrhoea -Functional bloating | 12 (52.2%) 11 (47.8%) | 26 (56.5%) 20 (43.5%) | 29 (65.9%) 15 (34.1%) | 0.49 |
| HLA-DQ2.5+ | 14 (63.6%) | 20 (44.4%) | 22 (50%) | 0.34 |
| LE (IEL > 25%) (%) | 23 (100%) | 19 (41.3%) | 22 (50%) | <0.001 |
| IEL count (mean ± SEM) | 38.4 ± 3.4 | 24.5 ± 1.9 | 26.1 ± 2.3 | 0.001 |
| Low-grade coeliac score >10 | 23 (100%) | 0 | 5 (11.4%) | <0.001 |
| Low-grade coeliac score (mean ± SEM) | 13.9 ± 0.4 | 4.7 ± 0.5 | 5.7 ± 0.4 | <0.001 |
| Coeliac IEL cytometry pattern: | ||||
| -Isolated increase in TCRγδ+ cells -Coeliac lymphogram | 5 (21.7%) 18 (78.3%) | 6 (14%) 7 (15.2%) | 9 (20.5%) 5 (11.4%) | <0.001 |
| TCRγδ+ cells (%) (mean ± SEM) | 20.6 ± 2.3 | 7.7 ± 1.4 | 6.9 ± 1.1 | <0.001 |
| CD3− cells (%) (mean ± SEM) | 6.6 ± 1.1 | 15.9 ± 1.9 | 18.3 ± 1.9 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Bañares, F.; Arau, B.; Raga, A.; Aceituno, M.; Tristán, E.; Carrasco, A.; Ruiz, L.; Martín-Cardona, A.; Ruiz-Ramírez, P.; Esteve, M. Long-Term Effect of a Gluten-Free Diet on Diarrhoea- or Bloating-Predominant Functional Bowel Disease: Role of the ‘Low-Grade Coeliac Score’ and the ‘Coeliac Lymphogram’ in the Response Rate to the Diet. Nutrients 2021, 13, 1812. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061812
Fernández-Bañares F, Arau B, Raga A, Aceituno M, Tristán E, Carrasco A, Ruiz L, Martín-Cardona A, Ruiz-Ramírez P, Esteve M. Long-Term Effect of a Gluten-Free Diet on Diarrhoea- or Bloating-Predominant Functional Bowel Disease: Role of the ‘Low-Grade Coeliac Score’ and the ‘Coeliac Lymphogram’ in the Response Rate to the Diet. Nutrients. 2021; 13(6):1812. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061812
Chicago/Turabian StyleFernández-Bañares, Fernando, Beatriz Arau, Agnès Raga, Montserrat Aceituno, Eva Tristán, Anna Carrasco, Laura Ruiz, Albert Martín-Cardona, Pablo Ruiz-Ramírez, and Maria Esteve. 2021. "Long-Term Effect of a Gluten-Free Diet on Diarrhoea- or Bloating-Predominant Functional Bowel Disease: Role of the ‘Low-Grade Coeliac Score’ and the ‘Coeliac Lymphogram’ in the Response Rate to the Diet" Nutrients 13, no. 6: 1812. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061812