
Effects of Anthocyanin Supplementation on Reduction of Obesity Criteria: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design of SR-MA
2.2. Data Collection
2.3. Inclusion and Exclusion Criteria
2.4. Quality Assessment (ROB)
2.5. Data Analysis
3. Results
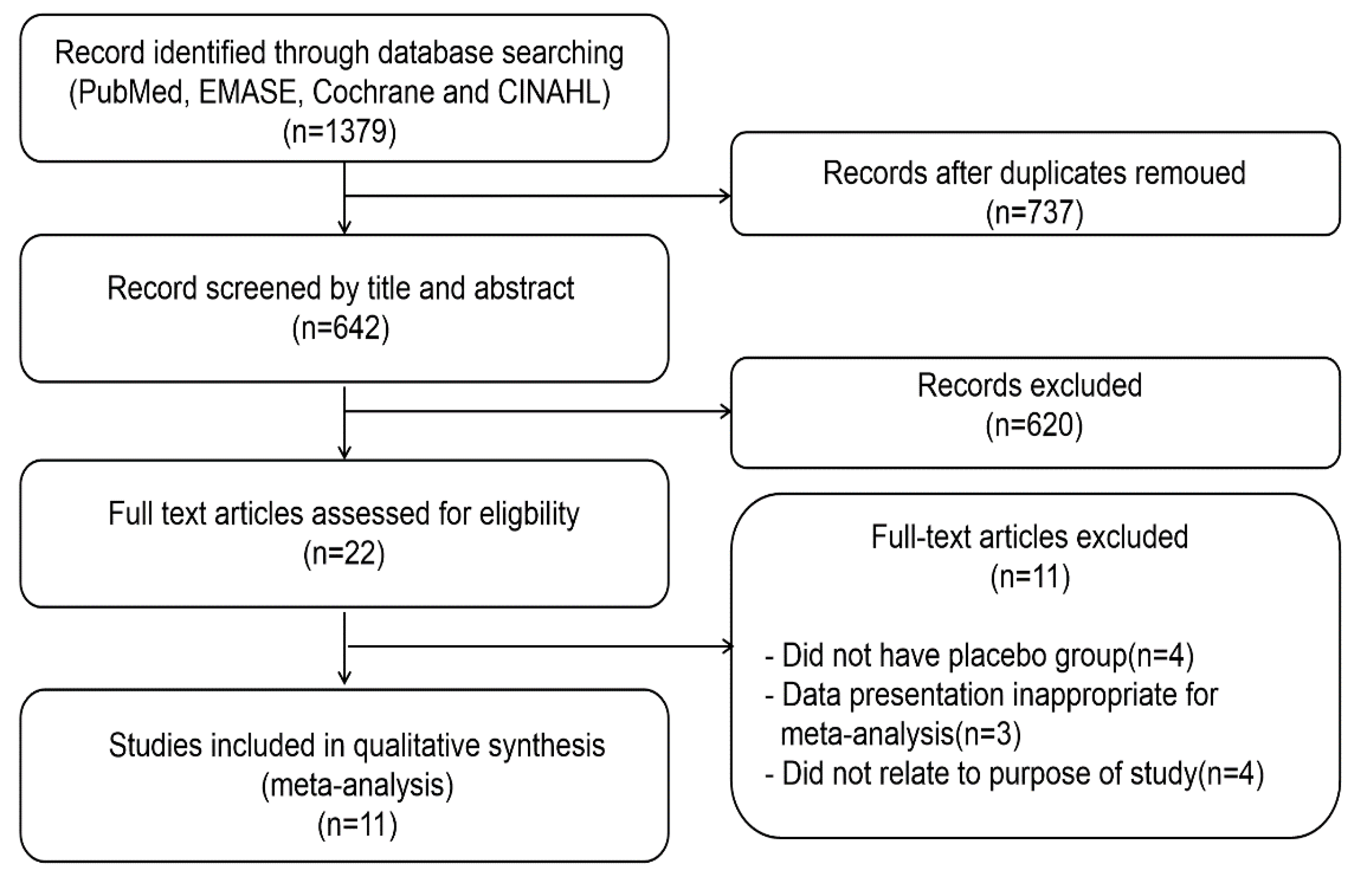
3.1. Study Selection
3.2. Characteristics of the Included RCTs
3.3. Quality Assessment; ROB
3.4. Anthocyanin Supplements on the Reduction of BMI
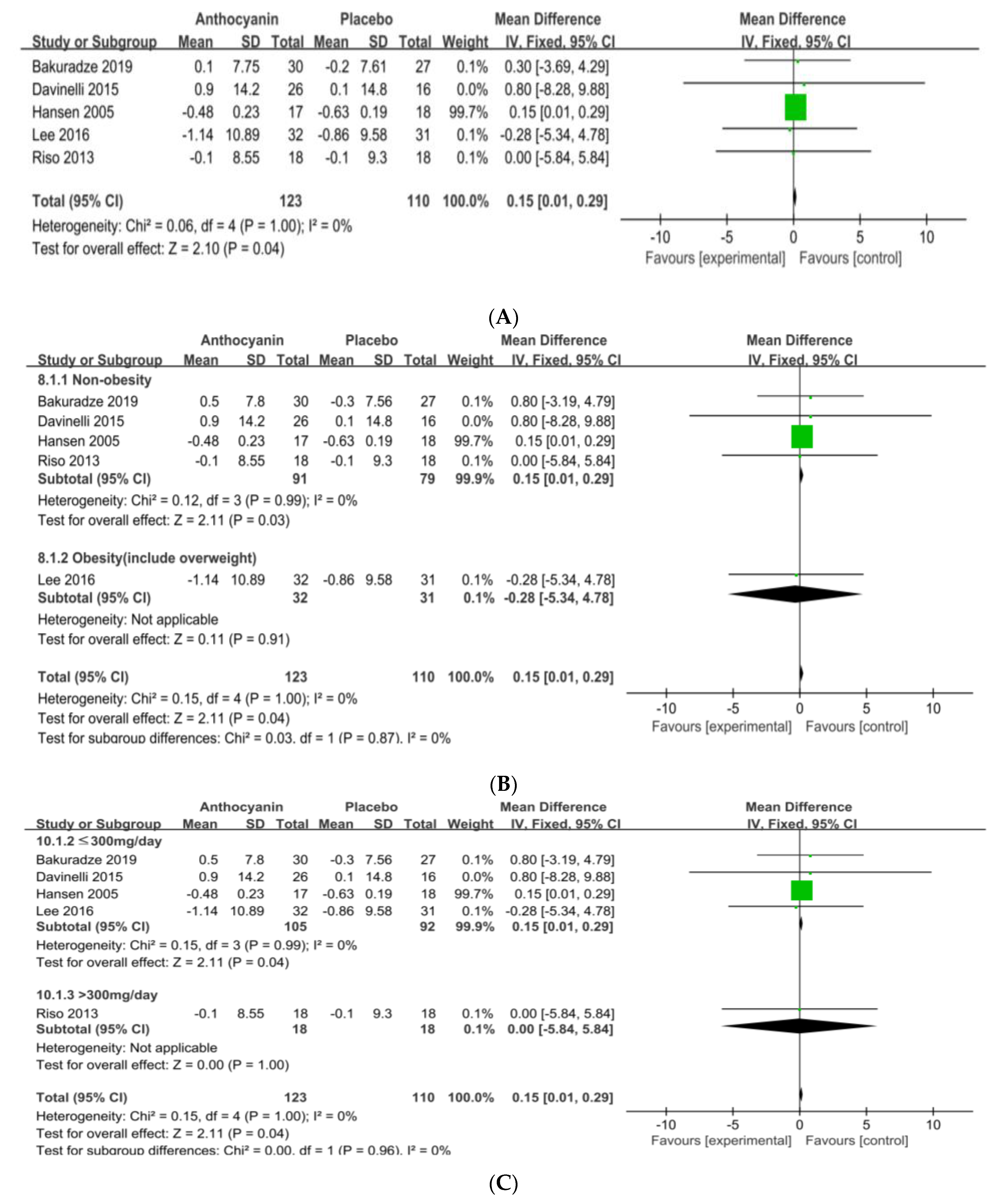
3.5. Anthocyanin Supplements on the Reduction of BW or WC
3.6. Anthocyanins Supplements on BMI and BW by National Origin
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pascual-Teres, S.; Sanchez-Ballesta, M.T. Anthocyanins: From plant to health. Phytochem. Rev. 2008, 7, 281–299. [Google Scholar] [CrossRef]
- He, J.; Giusti, M.M. Anthocyanins: Natural colorants with health-promoting properties. Annu. Rev. Food Sci. Technol. 2010, 1, 163–187. [Google Scholar] [CrossRef] [PubMed]
- Ryu, D.Y.; Koh, E.M. Estimated Dietary Anthocyanin Intakes and Major Food Sources of Koreans. J. East Asian Soc. Diet. Life 2017, 27, 378–386. [Google Scholar] [CrossRef]
- Valenti, L.; Riso, P.; Mazzocchi, A.; Porrini, M.; Fargion, S.; Agostoni, C. Dietary anthocyanins as nutritional therapy for nonalcoholic fatty liver disease. Oxid. Med. Cell. Longev. 2013, 2013, 145421. [Google Scholar] [CrossRef] [Green Version]
- Borges, G.; Roowi, S.; Rouanet, J.M.; Duthie, G.G.; Lean, M.E.; Crozier, A. The bioavailability of rasberry anthocyanins and ellagitannins in rats. Mol. Nutr. Food Res. 2007, 5196, 714–725. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Su, H.; Sun, C.; Zheng, X.; Chen, W. Recent advances in understanding the anti-obesity activity of anthocyanins and their biosynthesis in microorganisms. Trends Food Sci. Technol. 2018, 72, 13–24. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Knaze, V.; Lujan-Barroso, L.; Slimani, N.; Romieu, I.; Touillaud, M.; Kaaks, R.; Teucher, B.; Mattiello, A.; Grioni, S.; et al. Estimation of the intake of anthocyanidins and their food sources in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Br. J. Nutr. 2011, 106, 1090–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prior, R.L.; Wu, X. Anthocyanins: Structural characteristics that result in unique metabolic patterns and biological activities. Free Radic. Res. 2006, 40, 1014–1028. [Google Scholar] [CrossRef]
- Wang, H.; Cao, G.; Prior, R.L. Oxygen radical absorbing capacity of anthocyanins. J. Agric. Food Chem. 1997, 45, 304–309. [Google Scholar] [CrossRef]
- Azzini, E.; Giacometti, J.; Russo, G.L. Antiobesity Effects of Anthocyanins in Preclinical and Clinical Studies. Oxidative Med. Cell. Longev. 2017, 2017, 2740364. [Google Scholar] [CrossRef]
- Li, D.; Zhang, Y.; Liu, Y.; Sun, R.; Xia, M. Purified Anthocyanin Supplementation Reduces Dyslipidemia, Enhances Antioxidant Capacity, and Prevents Insulin Resistance in Diabetic Patients. J. Nutr. 2015, 145, 742–748. [Google Scholar] [CrossRef]
- Pokimica, B.; García-Conesa, M.T.; Zec, M.; Debeljak-Martačić, J.; Ranković, S.; Nevena Vidović, N.; Petrović-Oggiano, G.; Konić-Ristić, A.; Maria Glibetić, M. Chokeberry Juice Containing Polyphenols Does Not Affect Cholesterol or Blood Pressure but Modifies the Composition of Plasma Phospholipids Fatty Acids in Individuals at Cardiovascular Risk. Nutrients 2019, 11, 850. [Google Scholar] [CrossRef] [Green Version]
- Korean Society for the Study of Obesity. Obesity Common Knowledgy. Available online: http://general.kosso.or.kr/ (accessed on 1 April 2020).
- Riso, P.; Klimis-Zacas, D.; Del, B.C.; Martini, D.; Campolo, J.; Vendrame, S.; Porrini, M. Effect of a wild blueberry (Vaccinium angustifolium) drink intervention on markers of oxidative stress, inflammation and endothelial function in humans with cardiovascular risk factors. Eur. J. Nutr. 2012, 52, 949–961. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Sorn, S.R.; Park, Y.; Park, H.K. Anthocyanin Rich-Black Soybean Testa Improved Visceral Fat and Plasma Lipid Profiles in Overweight/Obese Korean Adults: A Randomized Controlled Trial. J. Med. Food 2016, 19, 995–1003. [Google Scholar] [CrossRef]
- Bakuradze, T.; Tausend, A.; Galan, J.; Maria Groh, I.A.; Berry, D.; Tur, J.A.; Richling, E. Antioxidative activity and health benefits of anthocyanin-rich fruit juice in healthy volunteers. Free Radic. Res. 2019, 53, 1045–1055. [Google Scholar] [CrossRef]
- Vendrame, S.; Del, B.C.; Ciappellano, S.; Riso, P.; Klimis-Zacas, D. Berry fruit consumption and metabolic syndrome. Antioxidants 2016, 5, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overall, J.; Bonney, S.A.; Wilson, M.; Beermann, A.; Grace, M.H.; Esposito, D.; Lila, M.A.; Komarnytsky, S. Metabolic effects of berries with structurally diverse anthocyanins. Int. J. Mol. Sci. 2017, 18, 422. [Google Scholar] [CrossRef] [Green Version]
- Davinelli, S.; Bertoglio, J.C.; Zarrelli, A.; Pina, R.; Scapagnini, G. A RandomizedClinical Trial Evaluating the Efficacy of an Anthocyanin–Maqui Berry Extract (Delphinol®) on Oxidative Stress Biomarkers. J. Am. Coll. Nutr. 2015, 34 (Suppl. 1) (Suppl. 1), 28–33. [Google Scholar] [CrossRef] [Green Version]
- Curtis, P.J.; Kroon, P.A.; Hollands, W.J.; Walls, R.; Jenkins, G.; Kay, C.D.; Cassidy, A. Cardiovascular Disease Risk Biomarkers and Liver and Kidney Function Are not Altered in Postmenopausal Women afterIngesting an Elderberry Extract Rich in Anthocyanins for 12 Weeks. J. Nutr. 2009, 139, 2266–2271. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.S.; Marckmann, P.; Dragsted, L.; Nielsen, I.L.F.; Nielsen, S.E.; Gronbaek, M. Effect of red wine and red grape extract on blood lipids, haemostatic factors, and other risk factors for cardiovascular disease. Eur. J. Clin. Nutr. 2005, 59, 449–455. [Google Scholar] [CrossRef] [Green Version]
- Santamarina, A.B.; Jamar, G.; Mennitti, L.V.; Cássia César, H.; Rosso, V.V.; Vasconcelos, J.R.; Pisani, L.P. Supplementation of Juçara Berry (Euterpe edulis Mart.) Modulates Epigenetic Markers in Monocytes from Obese Adults: A Double-Blind Randomized Trial. Nutrients 2018, 10, 1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, O.R.; Netzel, G.A.; Sakzewski, A.R. A randomized, double-blind, placebo-controlled trial of the effect of dried purple carrot on body mass, lipids, blood pressure, body composition, and inflammatory markers in overweight and obese adults: The QUENCH Trial. Can. J. Physiol. Pharmacol. 2013, 91, 480–488. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Ellwood, L.; Torun, G.; Bahar, Z.; Fernandez, R. Effects of flavonoid-rich fruits on hypertension in adults: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 2075–2105. [Google Scholar] [CrossRef]
- Otun, J.; Sahebkar, A.; Östlundh, L.; Atkin, S.L.; Sathyapalan, T. Systematic Review and Meta-analysis on the Effect of Soy on Thyroid Function. Sci. Rep. 2019, 9, 3964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, R.; Hakimi, M.; Asgary, S.; Ghanadian, S.M.; Keshvari, M.; Sarrafzadegan, N. Evaluation of the Effects of Vaccinium arctostaphylosL. Fruit Extract on Serum Lipids and hs-CRP Levels and Oxidative Stress in Adult Patients with Hyperlipidemia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Evid. -Based Complement. Altern. Med. 2014, 2014, 217451. [Google Scholar] [CrossRef]
- Liu, C.; Sun, J.; Lu, Y.; Bo, Y. Effects of Anthocyanin on Serum Lipids in Dyslipidemia Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e01620. [Google Scholar] [CrossRef] [PubMed]
- Fallah, A.A.; Sarmast, E.; Fatehi, P.; Jafari, T. Impact of dietary anthocyanins on systemic and vascular inflammation: Systematic review and meta-analysis on randomised clinical trials. Food Chem. Toxicol. 2020, 135, 110922. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Shah, P. Effect of Anthocyanin Supplement on Lipid Profile and Inflammatory Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cholesterol 2018, 2018, 8450793. [Google Scholar] [CrossRef] [PubMed]
- Daneshzad, E.; Shab-Bidar, S.; Mohammadpour, Z.; Djafarian, K. Effect of anthocyanin supplementation on cardio-metabolic biomarkers: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2018, 38, 1153–1165. [Google Scholar] [CrossRef]
- Serban, C.; Sahebkar, A.; Ursoniu, S.; Andrica, F.; Banach, M. Effect of sour tea (Hibiscus sabdariffa L) on arterial hypertension: A systematic review and meta-analysis of randomized controlled trials. J Hypertens. 2015, 33, 1119–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godos, J.; Vitale, M.; Micek, A.; Ray, S.; Martini, D.; Del Rio, D.; Riccardi, G.; Galvano, F.; Grosso, G. Dietary Polyphenol Intake, Blood Pressure, and Hypertension: A Systematic Review and Meta-Analysis of Observational Studies. Antioxidants 2019, 318, 152. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Yang, B.; Tan, J.; Jiang, J.; Li, D. Associations of dietary intakes of anthocyanins and berry fruits with risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective cohort studies. Eur. J. Clin. Nutr. 2016, 70, 1360–1367. [Google Scholar] [CrossRef]
- Wang, X.; Yang, D.Y.; Yang, L.Q.; Zhao, W.Z.; Cai, L.Y.; Shi, H.P. Anthocyanin Consumption and Risk of Colorectal Cancer: A Meta-Analysis of Observational Studies. J. Am. Coll. Nutr. 2019, 38, 470–477. [Google Scholar] [CrossRef]
- Akhlaghi, M.; Ghobadi, S.; Mohammad Hosseini, M.; Gholami, Z.; Mohammadian, F. Flavanols are potential anti-obesity agents, a systematic review and meta-analysis of controlled clinical trials. Nutrition. Metab. Cardiovasc. Dis. 2018, 28, 675–690. [Google Scholar] [CrossRef]
- Tabrizi, R.; Tamtaji, O.R.; Lankarani, K.B.; Akbari, M.; Dadgostar, E.; Dabbaghmanesh, M.H.; Asemi, Z. The effects of resveratrol intake on weight loss: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 375–390. [Google Scholar] [CrossRef]
- García-Conesa, M.T.; Chambers, K.; Combet, E.; Pinto, P.; Garcia-Aloy, M.; Andrés-Lacueva, C.; González-Sarrías, A. Meta-Analysis of the Effects of Foods and Derived Products Containing Ellagitannins and Anthocyanins on Cardiometabolic Biomarkers: Analysis of Factors Influencing Variability of the Individual Responses. Int. J. Mol. Sci. 2018, 19, 694. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population | Intervention | Bio-Markers of Obesity | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Author (Country) | Year | Case | Mean Age (int/cont) (1) | Sex (M/F) (2) | BMI (int/cont) | Sample Size (int/cont) | Duration (weeks) | Dose (mg/day) | |
| Bakuradze et al. [16] (Germany) | 2019 | Healthy male volunteers | 23/24 | 57/0 | 23.0/23.0 | 30/27 | 8 | 205.875 (anthocyanin fruit juice) | BW |
| Curtis et al. [20] (U.K) | 2009 | Healthy postmenopausal women | 58.1/58.3 | 0/52 | 25.1/24.3 | 26/26 | 12 | 500 (elderberry extract) | BMI |
| Davinelli et al. [19] (Italy) | 2015 | Healthy | 55/55 | 29/13 | 28.9/28.5 | 26/16 | 4 | 162 (maqui berry extract) | BW BMI WC |
| Hansen et al. [21] (Denmark) | 2005 | Healthy | 51/5 | 16/19 | 25.8/24.6 | 17/18 | 4 | M: 71/F: 48 (red grape extract) | BW |
| Lee et al. [15] (South Korea) | 2016 | Overweight, obese Korean Adults | 30.88/30.30 | 50/30 | 27.74/28.00 | 32/31 | 8 | 31.45 (black soybean extract) | BW BMI WC |
| Li et al. [11] (China) | 2015 | T2DM | 58.1/57.6 | 34/24 | 24.2/23.9 | 29/29 | 24 | 320 (mixture of blueberry and black currant) | BMI |
| Pokimica et al. [12] (Serbia) | 2019 | Overweight or obese people | 40.6/40.6 | NA | 26.59/27.29 | 28/29 | 4 | 28.3 (choke berry juice) | BMI |
| Riso et al. [14] (Italy) | 2013 | CVD | 47.8 | 18/0 | 24.9/24.9 | 18/18 (cross-over) | 6 | 375 (blueberry juice) | BW BMI |
| Santamarina et al. [22] (Brazil) | 2018 | Obese Adults | 44.26/45.07 | 11/16 | 34.63/33.82 | 13/14 | 6 | 131.2 (Juçara berry freeze-dried pulp) | BMI WC |
| Soltani et al. [25] (Iran) | 2014 | Hyperlipidemia | 47.93/46.36 | 20/30 | 25.40/25.21 | 25/25 | 4 | 180 (Vaccinium extract) | BMI |
| Wright et al. [23] (Australia) | 2013 | Overweight and obese Adults | 51.4/55.0 | 16/0 | 32.4/34.0 | 8/8 | 4 | 118.5 (Dried purple carrot) | BMI WC |
| Quantitative Synthesis of Data | Heterogeneity of Data | |||||||
|---|---|---|---|---|---|---|---|---|
| Biomarkers | No. of RCTs | MD | 95% CI | Z-Value | p-Value | I2 | p-Value | |
| BMI | 9 | −0.36 | −0.58, −0.13 | 3.14 | 0.002 | 0% | 0.96 | |
| Non-obese | 5 | −0.40 | −0.64, −0.16 | 3.26 | 0.001 | 0% | 0.80 | |
| Obese | 4 | −0.10 | −0.68, 0.48 | 0.33 | 0.74 | 0% | 1.00 | |
| ≤300 mg/day | 6 | −0.37 | −0.60, −0.14 | 3.15 | 0.002 | 0% | 0.79 | |
| >300 mg/day | 3 | −0.14 | −1.11, 0.82 | 0.29 | 0.77 | 0% | 0.99 | |
| ≤4 weeks | 4 | −0.41 | −0.66, −0.16 | 3.27 | 0.001 | 0% | 0.67 | |
| 6–8 weeks | 3 | −0.11 | −0.67, 0.45 | 0.38 | 0.70 | 0% | 1.00 | |
| ≥12 weeks | 2 | −0.16 | −1.34, 1.01 | 0.27 | 0.78 | 0% | 0.94 | |
| Europe | 4 | 0.13 | −0.97, 1.23 | 0.23 | 0.82 | 0% | 0.86 | |
| Asia | 2 | −0.14 | −0.91, 0.64 | 0.34 | 0.73 | 0% | 0.92 | |
| Middle East | 1 | −0.43 | −0.68, −0.18 | 3.38 | 0.0007 | - | - | |
| South America | 1 | −0.11 | −0.90, 0.68 | 0.27 | 0.78 | - | - | |
| Oceania | 1 | 0.20 | −4.42, 4.82 | 0.08 | 0.93 | - | - | |
| BW | 5 | 0.15 | 0.01, 0.29 | 2.10 | 0.04 | 0% | 1.00 | |
| Non-obese | 4 | 0.15 | 0.01, 0.29 | 2.11 | 0.03 | 0% | 0.99 | |
| Obese | 1 | −0.28 | −5.34, 4.78 | 0.11 | 0.91 | - | - | |
| ≤300 mg/d | 4 | 0.15 | 0.01, 0.29 | 2.11 | 0.04 | 0% | 0.99 | |
| >300 mg/d | 1 | 0.00 | −5.84, 5.84 | 0.00 | 1.00 | - | - | |
| ≤4 weeks | 2 | 0.15 | 0.01, 0.29 | 2.10 | 0.04 | 0% | 0.89 | |
| >4 weeks | 3 | 0.30 | −2.46, 3.06 | 0.21 | 0.83 | 0% | 0.94 | |
| South Korea | 1 | −0.28 | −5.34, 4.78 | 0.11 | 0.91 | - | - | |
| Europe | 4 | 0.15 | 0.01, 0.29 | 2.11 | 0.03 | 0% | 0.99 | |
| WC | 4 | 0.55 | −0.01, 2.11 | 0.69 | 0.49 | 0% | 0.57 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Choi, M.; Lee, M. Effects of Anthocyanin Supplementation on Reduction of Obesity Criteria: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 2121. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13062121
Park S, Choi M, Lee M. Effects of Anthocyanin Supplementation on Reduction of Obesity Criteria: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2021; 13(6):2121. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13062121
Chicago/Turabian StylePark, Seongmin, Munji Choi, and Myoungsook Lee. 2021. "Effects of Anthocyanin Supplementation on Reduction of Obesity Criteria: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 13, no. 6: 2121. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13062121