
Copper as Dietary Supplement for Bone Metabolism: A Review

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Results
2.1. Blood Copper Concentrations in Relation to Bone Metabolism
2.2. Copper Intake in Relation to Bone Metabolism
2.3. Copper Supplementation in Relation to Bone Metabolism
3. Discussion
4. Materials and Methods
- Configuration of the working group: two operators, experts in clinical nutrition (one acting as a methodological operator and one participating as a clinical operator).
- Formulation of the questions based on the considerations indicated in the abstract: the correlation of blood copper, daily copper intake, and copper supplementation with bone mineral density.
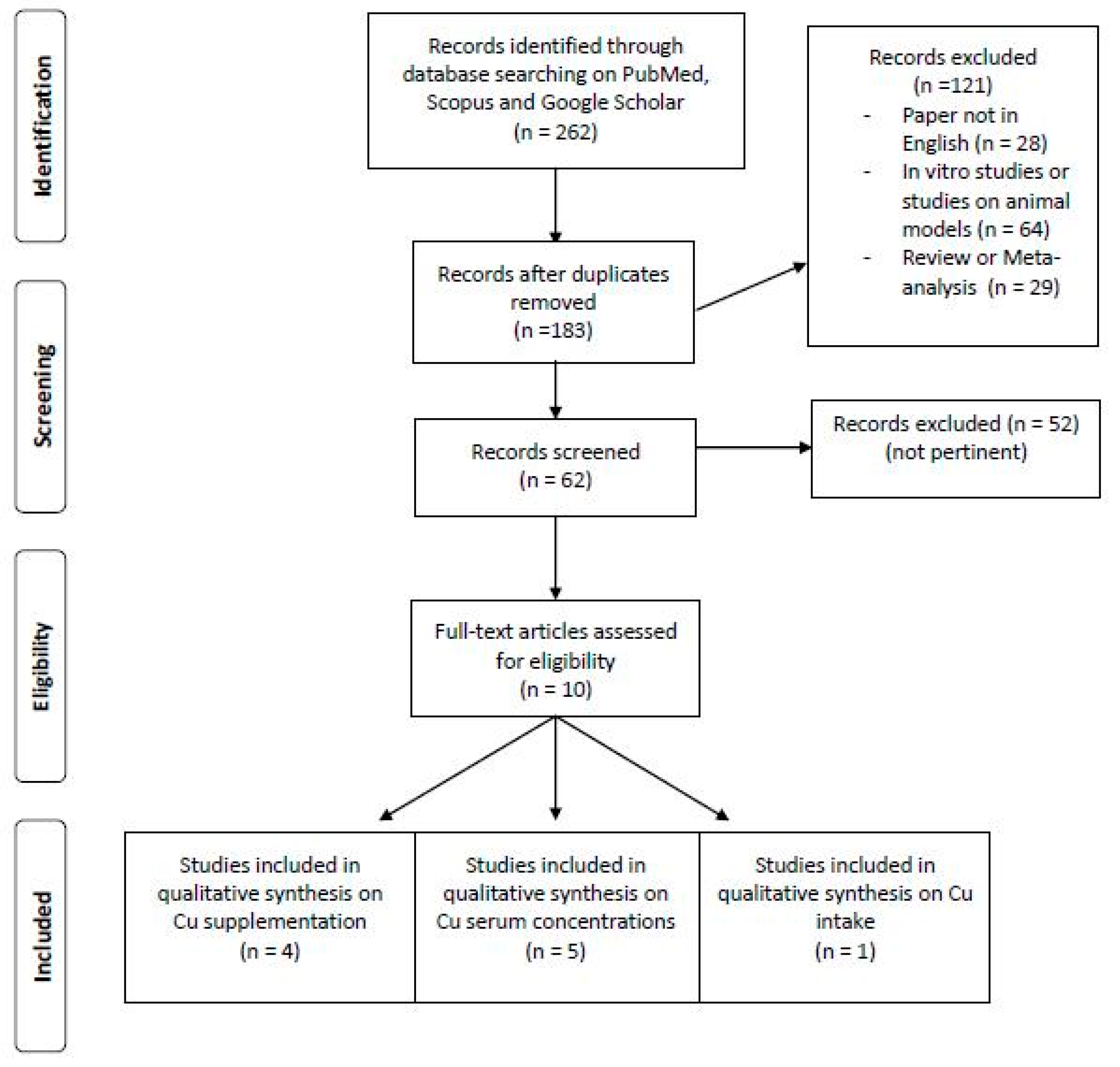
- Recognition of the relevant studies. Research was carried out on PubMed (Public Medline run by the National Center of Biotechnology Information (NCBI) of the National Library of Medicine of Bethesda (USA)) as follows: (a) definition of the keywords (copper, humans, bone health, bone mineral density, supplementation), inserting the interest field of the documents to be searched, grouped in quotation marks (“…”), and used separately or in combination; (b) use of the Boolean variable (true or false) AND operator, that allows for the establishment of logical relations among concepts; (c) research modalities: advanced search; (d) limits: papers published in the last 20 years; humans; adults; languages: English; (e) manual search performed by the researchers experienced in clinical nutrition through the revision of articles, focusing on the effectiveness of copper supplementation (alone or with other micronutrients) on the growth and maintenance of bone in humans, in order to suggest a daily dosage for copper supplementation.
- Published in journals qualified in the Index Medicus.
- Analysis and presentation of the outcomes: paragraphs about effectiveness of copper supplementation alone or in combination with other nutrients were created, and the data extrapolated from the “revised studies” were collocated in tables; in particular, the author, year of publication, and the characteristics of the study were specified for each study.
- An analysis of the reports in the form of a narrative review was carried out. At the beginning of each section, the type of studies chosen and the keywords considered are reported. Studies of any design which considered the effectiveness of copper supplementation (alone or with other micronutrients) on the growth and maintenance of bone in humans were evaluated.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olivares, M.; Uauy, R. Limits of metabolic tolerance to copper and biological basis for present recommendations and regulations. Am. J. Clin. Nutr. 1996, 63, 846S–852S. [Google Scholar] [CrossRef] [PubMed]
- Turnlund, J.R.; Keyes, W.R.; Peiffer, G.L.; Scott, K.C. Copper absorption, excretion, and retention by young men consuming low dietary copper determined by using the stable isotope 65Cu. Am. J. Clin. Nutr. 1998, 67, 1219–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnlund, J.R. Human whole-body copper metabolism. Am. J. Clin. Nutr. 1998, 67, 960S–964S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, D. Copper. In Handbook of Nutritionally Essential Mineral Elements; O’Dell, B., Sunde, R., Eds.; Marcel Dekker: New York, NY, USA, 1997; pp. 231–273. [Google Scholar]
- Turnlund, J. Copper. In Modern Nutrition in Health and Disease; Shike, M., Ross, A., Eds.; Williams & Wilkins: Baltimore, MD, USA, 1999; pp. 241–252. [Google Scholar]
- Roggi, C.; Turconi, G. Igiene Degli Alimenti e Della Nutrizione Umana-La Sicurezza Alimentare; EMSI: Rome, Italy, 2003. [Google Scholar]
- Prasad, A.; Brewer, G.; Schoomaker, E.; Rabbani, P. Hypocupremia induced by zinc therapy in adults. J. Am. Med. Assoc. 1978, 240, 2166–2168. [Google Scholar] [CrossRef]
- Simon, S.R.; Branda, R.F.; Tindle, B.H.; Burns, S.L. Copper deficiency and sideroblastic anemia associated with zinc ingestion. Am. J. Hematol. 1988, 28, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Food and Nutrition Board Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium; National Academies Press: Washington, DC, USA, 2001.
- Ieo BDA. Banca Dati di Composizione degli Alimenti per studi Epidemiologici in Italia. Available online: http://www.bda-ieo.it (accessed on 20 September 2007).
- Turnlund, J.R.; Scott, K.C.; Peiffer, G.L.; Jang, A.M.; Keyes, W.R.; Keen, C.L.; Sukanashi, T.M. Copper status of young men consuming a low-copper diet. Am. J. Clin. Nutr. 1997, 65, 72–78. [Google Scholar] [CrossRef] [Green Version]
- da Silva, F.; Williams, R. Copper: Extracytoplasmic oxidases and matrix formation. In The Biological Chemistry of the Elements: The Inorganic Chemistry of Life; da Silva, F., Williams, R., Eds.; Clarendon Press: Oxford, UK, 1991; pp. 388–399. [Google Scholar]
- Kubiak, K.; Klimczak, A.; Dziki, Ł.; Modranka, R.; Malinowska, K. Influence of copper (II) complex on the activity of selected oxidative enzymes. Pol. Merkur. Lekarski 2010, 28, 22–25. [Google Scholar]
- Dahl, S.; Rucker, R.; Niklason, L. Effects of copper and cross-linking on the extracellular matrix of tissue-engineered arteries. Cell Transpl. 2005, 14, 861–868. [Google Scholar] [CrossRef] [Green Version]
- John, J. Nutrition and bone health. In Escott-Stump Krause’s Food, Nutrition & the Nutrition Care Process; Mahan, L., Ed.; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Rucker, R.B.; Murray, J.; Riggins, R.S. Nutritional copper deficiency and penicillamine administration: Some effects on bone collagen and arterial elastin crosslinking. Adv. Exp. Med. Biol. 1977, 86, 619–648. [Google Scholar]
- Rucker, R.; Kosonen, T.; Clegg, M.; Mitchell, A.; Rucker, B.; Uriu-Hare, J.; Keen, C. Copper, lysyl oxidase, and extracellular matrix protein cross-linking. Am. J. Clin. Nutr. 1998, 67, 996S–1002S. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Yu, S. In vitro study of the effects of copper ion on osteoclastic resorption in various dental mineralized tissues. Chin. J. Stomatol. 2007, 42, 110–113. [Google Scholar]
- Milkovic, L.; Hoppe, A.; Detsch, R.; Boccaccini, A.R.; Zarkovic, N. Effects of Cu-doped 45S5 bioactive glass on the lipid peroxidation- associated growth of human osteoblast-like cells in vitro. J. Biomed. Mater. Res. Part A 2014, 102, 3556–3561. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Gao, Y.-S.; Wang, Y.; Hu, C.; Sun, Y.; Zhang, C. Dimethyloxaloylglycine increases the bone healing capacity of adipose-derived stem cells by promoting osteogenic differentiation and angiogenic potential. Stem Cells Dev. 2014, 23, 990–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milne, D. Assessment of copper nutritional status. Clin. Chem. 1994, 40, 1479–1484. [Google Scholar] [CrossRef]
- Rucker, R.; Riggins, R.; Laughlin, R.; Chan, M.; Chen, M.; Tom, K. Effects of nutritional copper deficiency on the biomechanical properties of bone and arterial elastin metabolism in the chick. J. Nutr. 1975, 105, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.; Burns, J.; Abel, E.W.; Cresswell, M.J.; Strain, J.J.; Paterson, C.R. Impaired mechanical strength of bone in experimental copper deficiency. Ann. Nutr. Metab. 1993, 37, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Gaffney-Stomberg, E. The Impact of Trace Minerals on Bone Metabolism. Biol. Trace Elem. Res. 2019, 188, 26–34. [Google Scholar] [CrossRef]
- Okyay, E.; Ertugrul, C.; Acar, B.; Sisman, A.R.; Onvural, B.; Ozaksoy, D. Comparative evaluation of serum levels of main minerals and postmenopausal osteoporosis. Maturitas 2013, 76, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, M.; Argun, M.; Kilic, E.; Saraymen, R.; Yazar, S. Magnesium, zinc and copper status in osteoporotic, osteopenic and normal post-menopausal women. J. Int. Med. Res. 2007, 35, 692–695. [Google Scholar] [CrossRef] [Green Version]
- Arikan, D.C.; Coskun, A.; Ozer, A.; Kilinc, M.; Atalay, F.; Arikan, T. Plasma selenium, zinc, copper and lipid levels in postmenopausal Turkish women and their relation with osteoporosis. Biol. Trace Elem. Res. 2011, 144, 407–417. [Google Scholar] [CrossRef]
- Mahdavi-Roshan, M.; Ebrahimi, M.; Ebrahimi, A. Copper, magnesium, zinc and calcium status in osteopenic and osteoporotic post-menopausal women. Clin. Cases Miner. Bone Metab. 2015, 12, 18–21. [Google Scholar] [CrossRef]
- Liu, S.Z.; Yan, H.; Xu, P.; Li, J.P.; Zhuang, G.H.; Zhu, B.F.; Lu, S.M. Correlation analysis between bone mineral density and serum element contents of postmenopausal women in Xi’an urban area. Biol. Trace Elem. Res. 2009, 131, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.H.; Lukaski, H.C.; Johnson, L.K.; Roughead, Z.K. Reported zinc, but not copper, intakes influence whole-body bone density, mineral content and T score responses to zinc and copper supplementation in healthy postmenopausal women. Br. J. Nutr. 2011, 106, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Strause, L.; Saltman, P.; Smith, K.; Bracker, M.; Andon, M. Spinal bone loss in postmenopausal women supplemented with calcium and trace minerals. J. Nutr. 1994, 124, 1060–1064. [Google Scholar] [CrossRef] [Green Version]
- Eaton-Evans, J.; Mcllrath, E.; Jackson, W.; McCartney, H.; Strain, J. Copper supplementation and the maintenance of bone mineral density in middle-aged women. J. Trace Elem. Exp. Med. Off. Publ. Int. Soc. Trace Elem. Res. Hum. 2003, 9, 87–94. [Google Scholar] [CrossRef]
- Baker, A.; Harvey, L.; Majask-Newman, G.; Fairweather-Tait, S.; Flynn, A.; Cashman, K. Effect of dietary copper intakes on biochemical markers of bone metabolism in healthy adult males. Eur. J. Clin. Nutr. 1999, 53, 408–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Dickersin, K.; Smith, G.D. Problems and Limitations in Conducting Systematic Reviews. In Systematic Reviews in Health Care; BMJ Publishing Group: London, UK, 2008; pp. 43–68. [Google Scholar]


{kind=link}
| First Author, Year | Study Design | Institution and Country | Inclusion Criteria | Number of Subjects (M-F) Mean Age | Micronutrient Serum Concentration Osteoporosis | Micronutrient Serum Concentration Osteopenia | Micronutrient Serum Concentration Normal | Primary Outcomes | Results |
|---|---|---|---|---|---|---|---|---|---|
| Okyay E, 2013 [25] | Cross-sectional study | Dokuz Eylul University School of Medicine, Izmir, Turkey | Postmenopausal women between age 45 and 80 | 728 F 56.52 ± 6.14 y | Women at 45–59 years: (p value < 0.05) Cu (μg/mL):
| Women at 45–59 years: (p value < 0.05) CU (μg/mL):
| Relationship between serum main minerals and postmenopausal osteoporosis. | Low Cu serum levels were independent risk factors for development of OP especially in early menopausal period. | |
| Mutlu M, 2007 [26] | Cross-sectional study | Erciyes University, Kayseri, Turkey | Post-menopausal women | 120 F 40 OP 58 ± 8.40 y, osteopenic 57 ± 9 y and 40 healthy group 59 ± 6 y | Cu (mg/L) 1.54 ± 0.12 | Cu (mg/L) 1.59 ± 0.09 | Cu (mg/L) 1.60 ± 0.08 | Cu changes in osteoporotic, osteopenic, and normal postmenopausal women. | No statistically significant differences observed between the osteopenic, osteoporotic, and control groups with respect to copper levels. |
| Arikan DC 2011 [27] | Case–control study | Medical Faculty of Kahramanmaras Sutcu Imam (Kahramanmaras, Turkey) | Natural menopause for more than 6 months | 107 F 35 healthy 48.17 ± 7.78 y, 37 osteopenic 55.32 ± 7.78 y and 35 OP 60.57 ± 8.65 y | Cu (μg/dL) 138.76 ± 37.21 | Cu (μg/dL) 137.58 ± 31.73 | Cu (μg/dL) 140.92 ± 32.74 | Serum Cu levels in postmenopausal women with osteoporosis, osteopenia, and in healthy controls, and the relationship between Cu and bone mineral density (BMD). | Plasma levels of all parameters were similar across each group (p > 0.05). |
| Mahdavi-Roshan, 2015 [28] | Cross-sectional study | Rheumatology clinic in Tabriz, Islamic Republic of Iran | women > 50 years old postmenopausal, having no history of hormone replacement therapy | 51 F 57.97 ± 1.2 y | Serum Cu (μg/dL): 27.29 ± 1.26 | Serum Cu (μg/dL) 26.75 ± 1.35 | Investigate and compare the mineral status between osteopenic and osteoporotic postmenopausal women. | No statistically significant differences between the osteopenic and osteoporotic groups with respect to serum levels of Cu. | |
| LIU SZ, 2009 [29] | Cross- sectional study | Xi’an urban area, China | 45 to 65-year-old females in natural and no hormone drug intake and osteoporosis treatment 6 months before investigation | 290 F 54.4 ± 5.5 y | Cu serum (mg/L) 0.8873 ± 0.2930 | Cu serum (mg/L) 0.8528 ± 0.2397 | Cu serum (mg/L) 0.8498 ± 0.3106 | Correlation between serum macroelement and trace element contents and BMD as well as the occurrence of osteoporosis. | There exist significant correlations between the contents of serum Cu, but no significant differences in this element content between the osteoporosis group, osteopenia group, and healthy group. |
| First Author, Year | Study Design | Institution and Country | Inclusion Criteria | Number of Subjects (M-F) Mean Age | Lowest Quintile Intake/RDA or EAR | % Subject in Lowest Quintile Intake/% Subject < RDA or EAR | Highest Quintile Intake | % Subject in Highest Quintile Intake | Primary Outcomes | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Mahdavi-Roshan, 2015 [28] | Cross-sectional study | Rheumatology clinic in Tabriz, Islamic Republic of Iran | Postmenopausal women > 50 years, having no history of hormone replacement therapy | 51 F 57.97 ± 1.2 y | The mean dietary intake (and percent from RDA) of copper in post-menopausal women with low bone density was 1.07 ± 0.08 mg/day (120 ± 12.2% RDA) | Investigate and compare the mineral status between osteopenic and osteoporotic postmenopausal women. | No statistically significant differences between the osteopenic and osteoporotic groups with respect to dietary intake copper. |
| First Author, Year | Study Design | Institution and Country | Inclusion Criteria | Intervention | Parallel Treatments | Number of Subjects (M-F) Mean Age | Duration of the Intervention | Primary Outcomes | Results |
|---|---|---|---|---|---|---|---|---|---|
| Nielsen FH, 2011 [30] | double-blind, placebo-controlled design. | University of North Dakota | postmenopausal women aged 51–80 y, BMI ≤ 32 kg/m2, BMD not more than 2·5 standard deviations below that for young adults | 600 mg calcium (Ca) supplement plus a 2 mg Cu (copper gluconate) and 12 mg Zn (zinc gluconate) supplement. | supplement containing 600 mg Ca plus a maize starch placebo | 649 F | 2 years | How Cu and Zn intakes would reduce the risk for bone loss. | Cu supplementation apparently did not have an impact on whole-body bone contents, BMD. |
| Strause L, 1994 [31] | double-blind, placebo-controlled trial. | San Diego greater Metropolitan area | >50 y old and in good general health | (1) placebo Ca + active trace minerals, (2) active Ca + placebo trace minerals, (3) active Ca + active trace mineral: 1000 mg elemental calcium/d in the form of Ca citrate malate and active supplement contained 15.0 mg of Zn as sulfate salt, 2.5 mg of Cu, and 5.0 mg of manganese as gluconate salts. | placebo calcium + placebo trace minerals | 59 F 66 ± 7 y | 2 years | Impact of supplementary Ca with and without the addition of a combination trace elements on spinal bone loss. | Supplementation with 1000 mg of Ca, 15 mg of Zn, 5 mg of manganese, and 2.5 mg of Cu maintained spinal bone density and differed significantly from a placebo group that lost bone density. |
| Eaton-Evans 2003 [32] | random and double-blind study | Royal Victoria Hospital, north Belfast | healthy women, aged 45–56 years | 3 mg Cu as amino acid chelate | placebo | 73 F Cu group: 49.97± 3.1 Placebo group: 50.8 ± 3.5 | 2 years | Effects of Cu supplementation over 2 years on vertebral trabecular bone mineral density (VTBMD). | Cu supplementation appeared to have reduced the loss of VTBMD in these middle-aged women over a 2-year period. |
| Baker A 1999 [33] | longitudinal intervention trial | Institute of Food Research, Norwich, UK | Subjects without any history of bone or articular disease, and with no intake of medicine that could affect bone or cartilage metabolism | Medium (1.6 mg/d), low (0.7 mg/d) and high (6.0 mg/d) intakes of Cu, in that order. A 7 d rotating low Cu menu was formulated and analysed for Cu content. This low Cu diet (0.7 mg/d) was fed throughout the three dietary periods and was supplemented to the appropriate level of Cu (as a CuSO4 solution dissolved in de-mineralised water taken with a meal) to achieve the medium (1.6 mg/d) and high (6.0 mg/d) Cu intakes. | ////////// | 11 M 30.9 y | 8-week dietary periods with a minimum of 4-week washout periods. | Effects of changing from a medium (1.6 mg Cu/d) to a low (0.7 mg Cu/d) or a high (6.0 mg/d) Cu intake on biochemical indices of bone turnover in healthy adult males. | Biomarkers of bone resorption were significantly increased when subjects were switched from the medium to the low Cu diet. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rondanelli, M.; Faliva, M.A.; Infantino, V.; Gasparri, C.; Iannello, G.; Perna, S.; Riva, A.; Petrangolini, G.; Tartara, A.; Peroni, G. Copper as Dietary Supplement for Bone Metabolism: A Review. Nutrients 2021, 13, 2246. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072246
Rondanelli M, Faliva MA, Infantino V, Gasparri C, Iannello G, Perna S, Riva A, Petrangolini G, Tartara A, Peroni G. Copper as Dietary Supplement for Bone Metabolism: A Review. Nutrients. 2021; 13(7):2246. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072246
Chicago/Turabian StyleRondanelli, Mariangela, Milena Anna Faliva, Vittoria Infantino, Clara Gasparri, Giancarlo Iannello, Simone Perna, Antonella Riva, Giovanna Petrangolini, Alice Tartara, and Gabriella Peroni. 2021. "Copper as Dietary Supplement for Bone Metabolism: A Review" Nutrients 13, no. 7: 2246. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072246