
The Role of BMI, Body Fat Mass and Visceral Fat in Executive Function in Individuals with Overweight and Obesity

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Procedure
2.2. Ethical Considerations
2.3. Anthropometrics, Body Composition, and Clinical Parameters
2.4. Physical Activity
2.5. Cognitive Function
2.6. Statistical Analyses
3. Results
3.1. Sociodemographic Variables
3.2. Anthropometrics, Body Composition, and Clinical Parameters
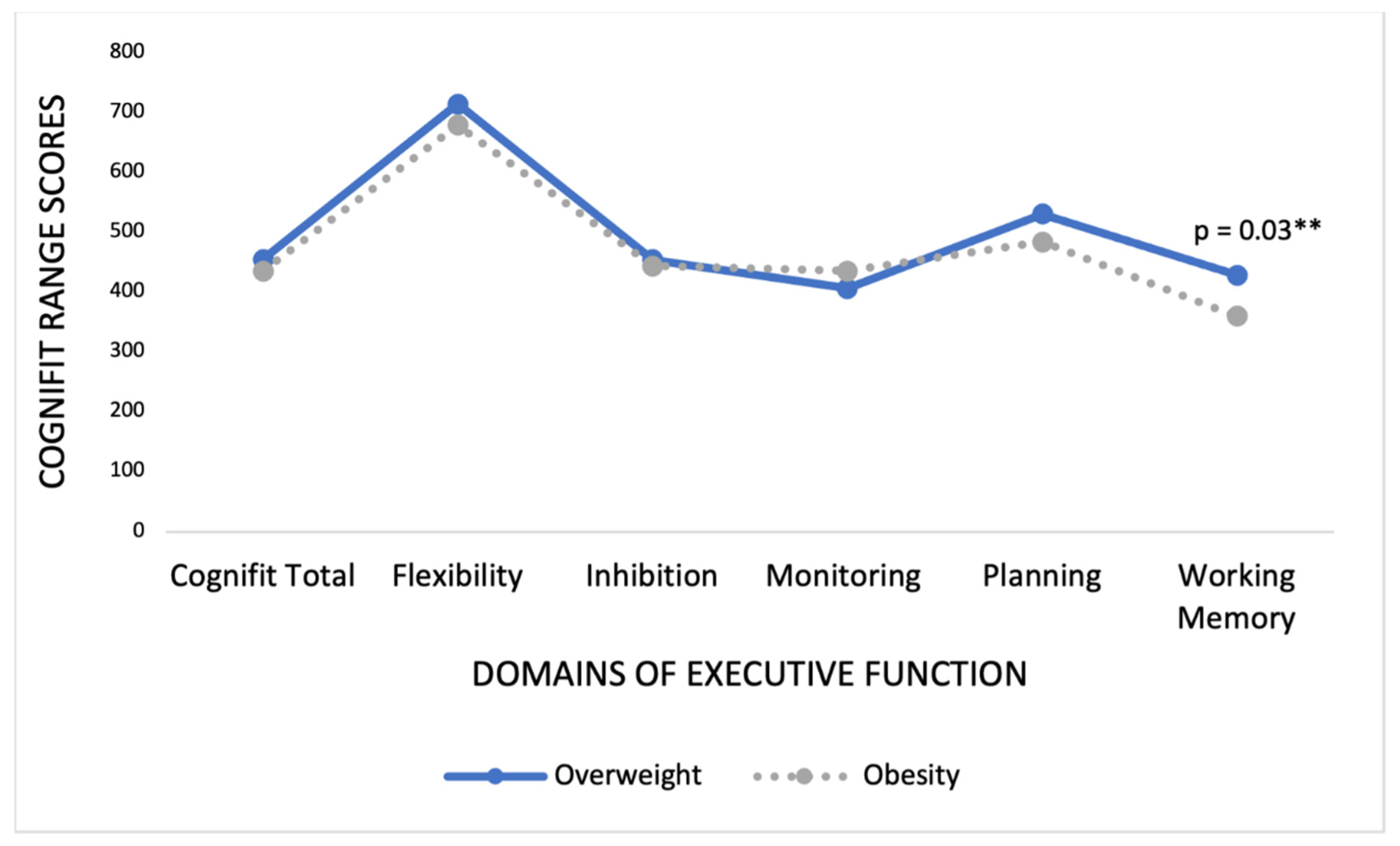
3.3. Differences in Executive Function between Individuals with Overweight and Obesity
3.4. Anthropometrics, Body Composition, and Clinical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Lavie, C.L.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease: Risk factor, paradox, and impact of weight loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef] [Green Version]
- Shai, I.; Jiang, R.; Manson, J.E.; Stampfer, M.J.; Willett, W.C.; Colditz, G.A.; Hu, F.B. Ethnicity, obesity, and risk of type 2 diabetes in women: A 20-year follow-up study. Diabetes Care 2006, 29, 1585–1590. [Google Scholar] [CrossRef] [Green Version]
- Winter, Y.; Rohrmann, S.; Linseisen, J.; Lanczik, O.; Ringleb, P.A.; Hebebrand, J.; Back, T. Contribution of obesity and abdominal fat mass to risk of stroke and transient ischemic attacks. Stroke 2008, 39, 3145–3151. [Google Scholar] [CrossRef] [Green Version]
- Flegal, K.M.; Carroll, M.D.; Kit, B.K.; Ogden, C.L. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA 2012, 307, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Pedditizi, E.; Peters, R.; Beckett, N. The risk of overweight/obesity in mid-life and late life for the development of dementia: A systematic review and meta-analysis of longitudinal studies. Age Ageing 2016, 45, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Shields, G.S.; Moons, W.G.; Slavich, G.M. Inflammation, self-regulation, and health: An immunologic model of self-regulatory failure. Perspect. Psychol. Sci. 2017, 12, 588–612. [Google Scholar] [CrossRef] [PubMed]
- Pratchayasakul, W.; Kerdphoo, S.; Petsophonsakul, P.; Pongchaidecha, A.; Chattipakorn, N.; Chattipakorn, S.C. Effects of high-fat diet on insulin receptor function in rat hippocampus and the level of neuronal corticosterone. Life Sci. 2011, 88, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Bartholdy, S.; Dalton, B.; O’Daly, O.G.; Campbell, I.C.; Schmidt, U. A systematic review of the relationship between eating, weight and inhibitory control using the stop signal task. Neurosci. Biobehav. Rev. 2016, 64, 35–62. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Shields, G.S.; Guo, C.; Liu, Y. Executive function performance in obesity and overweight individuals: A meta-analysis and review. Neurosci. Biobehav. Rev. 2018, 84, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.; Gilbert, S.; Serpell, L. Systematic review: Are overweight and obese individuals impaired on behavioural tasks of executive functioning? Neuropsychol. Rev. 2013, 23, 138–156. [Google Scholar] [CrossRef]
- Veronese, N.; Facchini, S.; Stubbs, B.; Luchini, C.; Solmi, M.; Manzato, E.; Sergi, G.; Maggi, S.; Cosco, T.; Fontana, L. Weight loss is associated with improvements in cognitive function among overweight and obese people: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 72, 87–94. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Physical Status: The Use and Interpretation of Anthropometry; World Health Organization (WHO): Geneva, Switzerland, 1995. [Google Scholar]
- WHO. Report of a WHO Expert Committee; WHO Technical Report Series 854; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Rodríguez-Muñoz, S.; Corella, C.; Abarca-Sos, A.; Zaragoza, J. Validation of three short physical activity questionnaires with accelerometers among university students in Spain. J. Sports Med. Phys. Fit. 2017, 57, 1660–1668. [Google Scholar]
- Shatil, E. Does combined cognitive training and physical activity training enhance cognitive abilities more than either alone? A four-condition randomized controlled trial among healthy older adults. Front. Aging Neurosci. 2013, 5, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siberski, J.; Shatil, E.; Siberski, C.; Eckroth-Bucher, M.; French, A.; Horton, S.; Loefflad, R.F.; Rouse, P. Computer-based cognitive training for individuals with intellectual and developmental disabilities: Pilot study. Am. J. Alzheimers. Dis. Other Demen. 2015, 30, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Horowitz-Kraus, T.; Breznitz, Z. Can the error detection mechanism benefit from training the working memory? A comparison between dyslexics and controls—An ERP study. PLoS ONE 2009, 4, e7141. [Google Scholar]
- Haimov, I.; Hanuka, E.; Horowitz, Y. Chronic insomnia and cognitive functioning among older adults. Behav. Sleep Med. 2008, 6, 32–54. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, W.; Schmeichel, B.J.; Baddeley, A.D. Executive functions and self-regulation. Trends Cogn. Sci. 2012, 16, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Dohle, S.; Diel, K.; Hofmann, W. Executive functions and the self-regulation of eating behavior: A review. Appetite 2018, 124, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, A.B.; O’Brien, S.; Lavender, J.M.; Pearson, C.M.; Le Grange, D.; Hunter, S.J. Executive functioning in a racially diverse sample of children who are overweight and at risk for eating disorders. Appetite 2018, 124, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Riggs, N.; Chou, C.P.; Spruijt-Metz, D.; Pentz, M.A. Executive cognitive 749 function as a correlate and predictor of child food intake and physical activity. Child Neuropsychol. 2010, 16, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Whitelock, V.; Nouwen, A.; Van den Akker, O.; Higgs, S. The role of working memory sub-components in food choice and dieting success. Appetite 2018, 124, 24–32. [Google Scholar] [CrossRef]
- Marsland, A.L.; Gianaros, P.J.; Kuan, D.C.; Sheu, L.K.; Krajina, K.; Manuck, S.B. Brain morphology links systemic inflammation to cognitive function in midlife adults. Brain Behave. Immun. 2015, 48, 195–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottino-González, J.; Jurado, M.A.; García-García, I.; Caldú, X.; Prats-Soteras, X.; Tor, E.; Sender-Palacios, M.J.; Garolera, M. Allostatic load and executive functions in overweight adults. Psychoneuroendocrinology 2019, 106, 165–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farruggia, M.C.; Small, D.M. Effects of adiposity and metabolic dysfunction on cognition: A review. Physiol. Behav. 2019, 208, 112578. [Google Scholar] [CrossRef]
- Huang, T.; Chen, Z.; Shen, L.; Fan, X.; Wang, K. Associations of Cognitive Function with BMI, Body Fat Mass and Visceral Fat in Young Adulthood. Medicina 2019, 55, 221. [Google Scholar] [CrossRef] [Green Version]
- Verdejo-García, A.; Lawrence, A.J.; Clark, L. Impulsivity as a vulnerability marker for substance-use disorders: Review of findings from high-risk research, problem gamblers and genetic association studies. Neurosci. Biobehav. Rev. 2008, 32, 777–810. [Google Scholar] [CrossRef]
- Spitoni, G.F.; Ottaviani, C.; Petta, A.M.; Zingaretti, P.; Aragona, M.; Sarnicola, A.; Antonucci, G. Obesity is associated with lack of inhibitory control and impaired heart rate variability reactivity and recovery in response to food stimuli. Int. J. Psychophysiol. 2017, 116, 77–84. [Google Scholar] [CrossRef]
- Anderson, P. Assessment and development of executive function (EF) during childhood. Child Neuropsych. 2002, 8, 71–82. [Google Scholar] [CrossRef]
- Allan, J.L.; McMinn, D.; Daly, M. A bidirectional relationship between executive function and health behavior: Evidence, implications, and future directions. Front. Neurosci. 2016, 10, 386. [Google Scholar] [CrossRef] [PubMed]
- Gunstad, J.; Paul, R.H.; Cohen, R.A.; Tate, D.F.; Spitznagel, M.B.; Gordon, E. Elevated body mass index is associated with executive dysfunction in otherwise healthy adults. Compr. Psychiatry 2007, 48, 57–61. [Google Scholar] [CrossRef]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Fischer, J.S. Neuropsychological Assessment; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Cárdenas, D.; Madinabeitia, I.; Vera, J.; de Teresa, C.; Alarcón, F.; Jiménez, R.; Catena, A. Better brain connectivity is associated with higher total fat mass and lower visceral adipose tissue in military pilots. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overweight (n = 34, SD) | Obese (n = 53, SD) | p | |
|---|---|---|---|
| Sex | 0.82 | ||
| Female | 21 (38.2) | 34 (61.8) | |
| Male | 13 (40.6) | 19 (59.4) | |
| Age | 46.12 ± 10.23 | 47.43 ± 8.37 | 0.10 |
| Marital status | 0.59 | ||
| Single | 6 (17.64) | 5 (9.43) | |
| Married | 24 (70.59) | 41 (77.36) | |
| Divorced | 4 (11.77) | 6 (11.32) | |
| Other | 0 (0.0) | 1 (1.89) | |
| Educational level | 0.01 * | ||
| Primary studies | 1 (2.94) | 6 (11.32) | |
| Secondary studies | 7 (20.59) | 24 (45.28) | |
| University studies | 26 (76.47) | 23 (43.40) | |
| Alcohol consumption | 0.06 | ||
| Current use | 23 (70.59) | 31 (64.15) | |
| No | 10 (29.41) | 19 (35.85) | |
| Tobacco consumption | 0.28 | ||
| Current use | 6 (17.65) | 9 (16.98) | |
| No | 28 (82.35) | 44 (83.02) |
| Overweight (n = 34) | Obesity (n = 53) | Total (n = 87) | p | |
|---|---|---|---|---|
| Weight | 76.95 ± 10.00 | 99.28 ± 14.98 | 90.72 ± 17.15 | <0.00 ** |
| Height (m) | 1.65 ± 0.09 | 1.66 ± 0.08 | 1.66 ± 0.09 | 0.60 |
| WHR 1 | 0.87 ± 0.08 | 0.91 ± 0.11 | 32.83 ± 5.52 | 0.10 |
| Body fat | 30.72 ± 6.59 | 58.32 ± 83.16 | 48.10 ± 67.22 | 0.02 * |
| Visceral fat | 8.93 ± 4.30 | 11.46 ± 4.80 | 11.78 ± 5.10 | <0.00 ** |
| Muscle mass | 66.14 ± 6.37 | 68.57 ± 68.77 | 67.67 ± 54.60 | 0.84 |
| Glucose | 83.69 ± 21.84 | 80.33 ± 14.32 | 81.55 ± 17.37 | 0.41 |
| Cholesterol | 208.86 ± 40.00 | 201.28 ± 32.17 | 204.06 ± 35.18 | 0.36 |
| Triglycerides | 266.39 ± 183.21 | 251.91 ± 151.58 | 255.26 ± 157.27 | 0.80 |
| IPAQ 2 (MET/minute/week) | 2618.36 | 1216.82 | 1729.58 ± 2821.72 | 0.03 * |
| Overweight (n = 34) | Obesity (n = 53) | Total (n = 87) | t | p | |
|---|---|---|---|---|---|
| CogniFit total | 455.71 ± 114.65 | 436.62 ± 114.13 | 444.08 ± 114.05 | 7.70 | 0.45 |
| Flexibility | 715.09 ± 138.26 | 679.98 ± 154.05 | 693.70 ± 148.26 | 1.07 | 0.28 |
| Inhibition | 455.12 ± 341.42 | 444.81 ± 324.79 | 449.93 ± 329.42 | 0.01 | 0.99 |
| Monitoring | 407.06 ± 287.34 | 436.57 ± 267.75 | 425.03 ± 274.30 | −0.48 | 0.63 |
| Planning | 531.18 ± 202.14 | 485.08 ± 218.75 | 503.09 ± 212.43 | 0.98 | 0.33 |
| Working memory | 429.38 ± 129.44 | 360.66 ± 161.25 | 387.52 ± 152.60 | 2.08 | 0.03 ** |
| WHR | Body Fat (%) | Visceral fat | ||||
|---|---|---|---|---|---|---|
| Standardized β (95% CI) | p | Standardized β (95% CI) | p | Standardized β (95% CI) | p | |
| CogniFit total score | ||||||
| Overweight | 0.33 (−83.70, 98.10) | 0.86 | −3.81 (−12.69, −1.10) | 0.07 | −0.13 (−13.61, 7.17) | 0.51 |
| Obesity | −0.06 (−83.65, 54.17) | 0.66 | −0.12 (−0.55, 0.23) | 0.42 | 0.01 (−7.41, 7.10) | 0.96 |
| Cognitive flexibility | ||||||
| Overweight | 0.07 (−101.18, 144.55) | 0.72 | −0.09 (−11.21, 7.21) | 0.65 | −0.18 (−19.12, 7.51) | 0.37 |
| Obesity | −0.21 (−143.47, 126.35) | 0.17 | −0.09 (−0.06, 0.33) | 0.51 | 0.08 (−6.46, 11.42) | 0.58 |
| Inhibition | ||||||
| Overweight | −0.12 (−54.54, −83.93) | 0.52 | −0.35 (−3.43, −1.96) | 0.05 | −0.22 (−46.91, 11.45) | 0.22 |
| Obesity | 0.26 (−14.55, −35.09) | 0.07 | −0.32 (−2.27, −0.14) | 0.02 | 0.15 (−8.51, 30.40) | 0.26 |
| Monitoring | ||||||
| Overweight | 0.01 (−207.61, 225.42) | 0.93 | −0.44 (−35.28, −2.80) | 0.02 | −0.28 (−41.97, 4.96) | 0.12 |
| Obesity | 0.17 (−62.75, 156.53) | 0.23 | −0.22 (−1.68, 0.15) | 0.10 | 0.17 (−6.71, 26.40) | 0.23 |
| Planning | ||||||
| Overweight | 0.10 (−129.92, 212.05) | 0.62 | −0.37 (−24.29, 1.36) | 0.07 | 0.10 (−13.72, 23.34) | 0.59 |
| Obesity | 0.12 (−225.97, 42.25) | 0.17 | −0.01 (−0.07, 0.77) | 0.99 | 0.17 (13.34, 14.89) | 0.91 |
| Working memory | ||||||
| Overweight | 0.02 (−102.31, 114.57) | 0.91 | −0.60 (−0.68, 0.48) | 0.79 | −0.17 (−16.69, 6.81) | 0.39 |
| Obesity | −0.15 (−126.18, 66.48) | 0.53 | −0.09 (−1.88, 0.38) | 0.04 | −0.15 (−15.31, 4.92) | 0.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-SanSegundo, M.; Zaragoza-Martí, A.; Martin-LLaguno, I.; Berbegal, M.; Ferrer-Cascales, R.; Hurtado-Sánchez, J.A. The Role of BMI, Body Fat Mass and Visceral Fat in Executive Function in Individuals with Overweight and Obesity. Nutrients 2021, 13, 2259. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072259
Sánchez-SanSegundo M, Zaragoza-Martí A, Martin-LLaguno I, Berbegal M, Ferrer-Cascales R, Hurtado-Sánchez JA. The Role of BMI, Body Fat Mass and Visceral Fat in Executive Function in Individuals with Overweight and Obesity. Nutrients. 2021; 13(7):2259. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072259
Chicago/Turabian StyleSánchez-SanSegundo, Miriam, Ana Zaragoza-Martí, Iciar Martin-LLaguno, Marina Berbegal, Rosario Ferrer-Cascales, and José Antonio Hurtado-Sánchez. 2021. "The Role of BMI, Body Fat Mass and Visceral Fat in Executive Function in Individuals with Overweight and Obesity" Nutrients 13, no. 7: 2259. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072259