
A Method to Estimate the Efficacy vs. Effectiveness in Meta-Analysis of Clinical Trials with Different Adherence Scenarios: A Monte Carlo Simulation Study in Nutrition


Abstract
:1. Introduction
2. Materials and Methods
2.1. Deduction of Statistics per Protocol from Those Reported by ITT
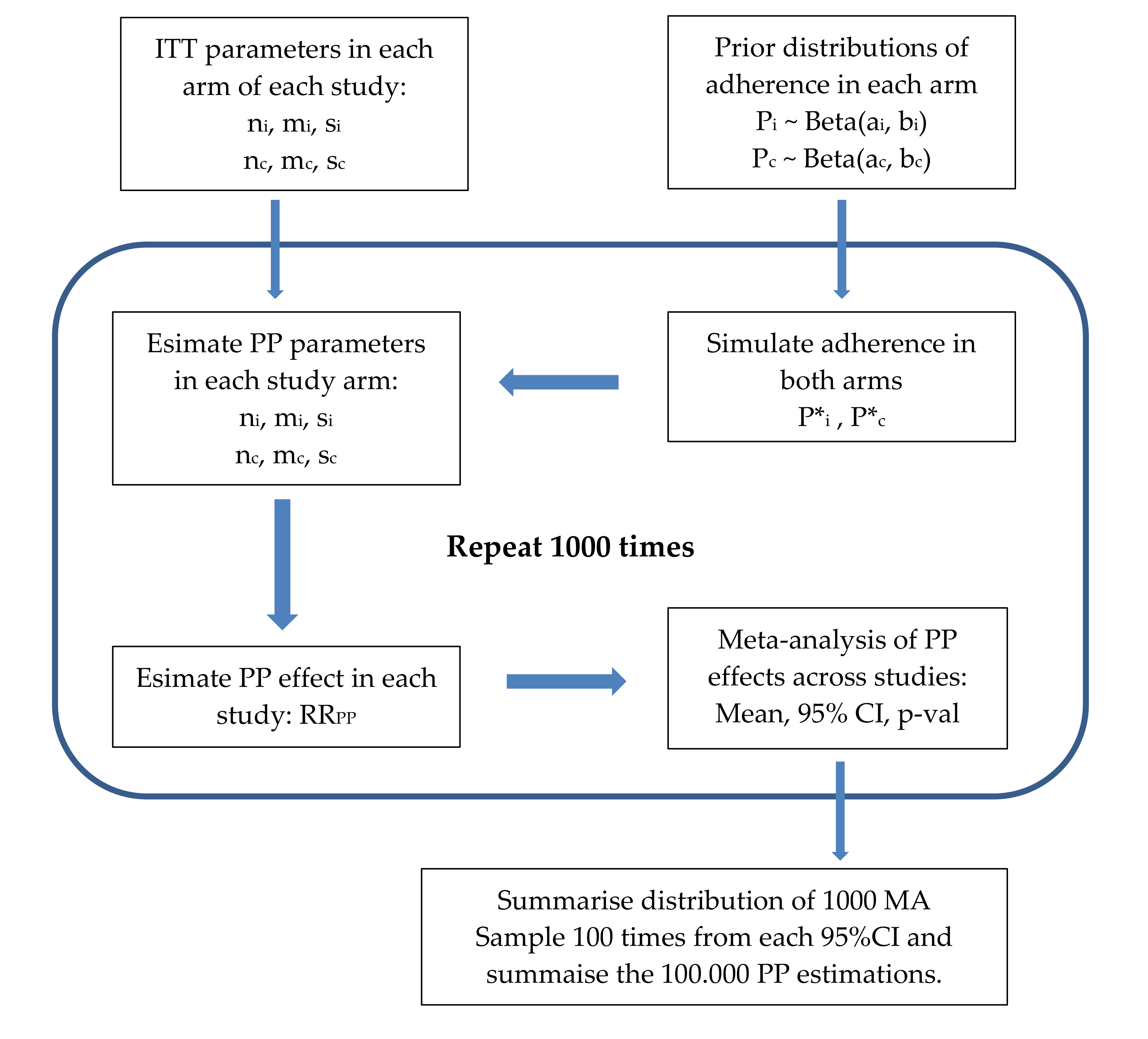
2.2. Simulation of an MA Per Protocol
2.3. Data
3. Results
3.1. MA for Diastolic Blood Pressure (DBP)
3.2. MA for Low Density Lipoproteins
3.3. MA for High Density Lipoproteins
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harman, D. Aging: A Theory on Free Radical Radiation Chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.H.; Engineer, A. Denis Burkitt and the origins of the dietary fibre hypothesis. Nutr. Res. Rev. 2018, 31, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Zheng, J.; Li, Y.; Xu, D.P.; Li, S.; Chen, Y.M.; LI, H.B. Natural polyphenols for prevention and treatment of cancer. Nutrients 2016, 8, 515. [Google Scholar] [CrossRef] [PubMed]
- Maleki, S.J.; Crespo, J.F.; Cabanillas, B. Anti-inflammatory effects of flavonoids. Food Chem. 2019, 299, 125124. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Zhong, L.; Song, Y.; Hu, Y.; Wang, G.; Sun, S. Consumption of citrus and cruciferous vegetables with incident type 2 diabetes mellitus based on a meta-analysis of prospective study. Prim. Care Diabetes 2016, 10, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Angelino, D.; Godos, J.; Ghelfi, F.; Tieri, M.; Titta, L.; Lafranconi, A.; Marventano, S.; Alonzo, E.; Gambera, A.; Sciacca, S.; et al. Fruit and vegetable consumption and health outcomes: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2019, 70, 652–667. [Google Scholar] [CrossRef]
- Frank, S.M.; Webster, J.; McKenzie, B.; Geldsetzer, P.; Manne-Goehler, J.; Andall-Brereton, G.; Houehanou, C.; Houinato, D.; Gurung, M.S.; Bicaba, B.W.; et al. Consumption of fruits and vegetables among individuals 15 years and older in 28 low- and middle-income countries. J. Nutr. 2019, 149, 1252–1259. [Google Scholar] [CrossRef]
- Mazidi, M.; Katsiki, N.; Banach, M. A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies. Nutrients 2020, 12, 2350. [Google Scholar] [CrossRef]
- Tomanic, M.; Belojevic, G.; Jovanovic, A.; Vasiljevic, N.; Davidovic, D.; Maksimovic, K. Dietary Factors and Tinnitus among Adolescents. Nutrients 2020, 12, 3291. [Google Scholar] [CrossRef] [PubMed]
- Gisbert-Mullor, R.; Ceccanti, C.; Gara Padilla, Y.; López-Galarza, S.; Calatayud, Á.; Conte, G.; Guidi, L. Effect of Grafting on the Production, Physico-Chemical Characteristics and Nutritional Quality of Fruit from Pepper Landraces. Antioxidants 2020, 9, 501. [Google Scholar] [CrossRef] [PubMed]
- Jakše, B.; Jakše, B.; Pinter, S.; Jug, B.; Godnov, U.; Pajek, J.; Fidler Mis, N. Dietary Intakes and Cardiovascular Health of Healthy Adults in Short-, Medium-, and Long-Term Whole-Food Plant-Based Lifestyle Program. Nutrients 2019, 12, 55. [Google Scholar] [CrossRef] [Green Version]
- Abraha, I.; Cozzolino, F.; Orso, M.; Marchesi, M.; Germani, A.; Lombardo, G.; Eusebi, P.; De Florio, R.; Luchetta, M.; Iorio, A.; et al. A systematic review found that deviations from intention-to-treat are common in randomized trials and systematic reviews. J. Clin. Epidemiol. 2017, 84, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Manterola, C.; Asenjo-Lobos, C.; Otzen, T. Jerarquización de la evidencia: Niveles de evidencia y grados de recomendación de uso actual. Rev. Chil. Infectol. 2014, 31, 705–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unnebrink, K.; Windeler, J. Intention-to-treat: Methods for dealing with missing values in clinical trials of progressively deteriorating diseases. Stat. Med. 2001, 20, 3931–3946. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Schulz, K.F.; Altman, D.G. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel group randomized trials. BMC Med. Res. Methodol. 2001, 357, 1191–1194. [Google Scholar]
- Centro Cochrane Iberoamericano. Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J., Green, S., Eds.; Centro Cochrane Iberoamericano: Barcelona, Spain, 2011; pp. 1–639. Available online: http://www.cochrane-handbook.org (accessed on 24 September 2020). (In Spanish) Manual Cochrane de revisiones sistemáticas de intervenciones.
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Barretto, K.; Thiruvenkatachari, B.; O’Brien, K. Intention-to-treat analysis: Are we managing dropouts and missing data properly in research on orthodontic treatment? A systematic review. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 19–27. [Google Scholar] [CrossRef] [PubMed]
- DeMets, D.L.; Cook, T. Challenges of Non–Intention-to-Treat Analyses. JAMA 2019, 321, 145–146. [Google Scholar] [CrossRef]
- Johnston, B.C.; Guyatt, G.H. Best (but oft-forgotten) practices: Intention-to-treat, treatment adherence, and missing participant outcome data in the nutrition literature. Am. J. Clin. Nutr. 2016, 104, 1197–1201. [Google Scholar] [CrossRef] [Green Version]
- McCoy, C.E. Understanding the Intention-to-treat Principle in Randomized Controlled Trials. West. J. Emerg. Med. 2017, 18, 1075–1078. [Google Scholar] [CrossRef]
- Bell, M.L.; Fiero, M.; Horton, N.J.; Hsu, C.H. Handling missing data in RCTs; A review of the top medical journals. BMC Med. Res. Methodol. 2014, 14, 118. [Google Scholar] [CrossRef] [Green Version]
- Dossing, A.; Tarp, S.; Furst, D.E.; Gluud, C.; Wells, G.A.; Beyene, J.; Hansen, B.; Bliddal, H.; Christensenet, R. Modified intention-to-treat analysis did not bias trial results. J. Clin. Epidemiol. 2016, 72, 66–74. [Google Scholar] [CrossRef] [PubMed]
- John, E.R.; Abrams, K.R.; Brightling, C.E.; Sheehan, N.A. Assessing causal treatment effect estimation when using large observational datasets. BMC Med. Res. Methodol. 2019, 19, 207. [Google Scholar] [CrossRef] [PubMed]
- Yelland, L.N.; Sullivan, T.R.; Voysey, M.; Lee, K.J.; Cook, J.A.; Forbes, A.B. Applying the intention-to-treat principle in practice: Guidance on handling randomisation errors. Clin. Trials 2015, 12, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Detry, M.A.; Lewis, R.J. The intention-to-treat principle: How to assess the true effect of choosing a medical treatment. JAMA 2014, 312, 85–86. [Google Scholar] [CrossRef] [PubMed]
- Tufanaru, C. Demystifying intention-to-treat analyses. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 853–854. [Google Scholar] [CrossRef] [PubMed]
- Montori, V.M.; Guyatt, G.H. Intention-to-treat principle. CMAJ 2001, 165, 1339–1341. [Google Scholar]
- Lewis, J.; Machin, D. Intention to treat–who should use ITT? Br. J. Cancer 1993, 68, 647–650. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.Y.; Kim, J.Y.; Kang, H.T.; Han, K.H.; Shim, J.Y. Effect of fruits and vegetables on metabolic syndrome: A systematic review and meta-analysis of randomized controlled trials. Int. J. Food Sci. Nutr. 2015, 66, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; de Koning, L.; Delgado-Lista, J.; Díaz-López, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibbons, H.; Brennan, L. Metabolomics as a tool in the identification of dietary biomarkers. Proc. Nutr. Soc. 2017, 76, 42–53. [Google Scholar] [CrossRef]
- Hartley, L.; Igbinedion, E.; Holmes, J.; Flowers, N.; Thorogood, M.; Clarke, A.; Stranges, S.; Hooper, L.; Rees, K. Increased consumption of fruit and vegetables for the primary prevention of cardiovascular diseases. Cochrane Database Syst. Rev. 2013, CD009874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.R-project.org/ (accessed on 24 September 2020).
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/ (accessed on 24 September 2020).
- Viechtbauer, W. Conducting Meta-Analyses in R with The metafor Package. J. Stat. Softw. 2010, 36. [Google Scholar] [CrossRef] [Green Version]
- De Deus Mendonça, R.; Guimarães, L.M.F.; Mingoti, S.A.; Magalhaes, K.A.; Lopes, A.C.S. Barriers to and Facilitators for Adherence to Nutritional Intervention: Consumption of Fruits and Vegetables. Nutrition 2019, 67, 110568. [Google Scholar] [CrossRef]
- Herghelegiu, A.M.; Wenzel, K.M.; Moser, A.; Prada, G.I.; Nuta, C.R.; Stuck, A.E. Effects of Health Risk Assessment and Counselling on Fruit and Vegetable Intake in Older People: A Pragmatic Randomised Controlled Trial. J. Nutr. Health Aging 2020, 24, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neville, C.E.; McKinley, M.C.; Draffin, C.R.; Gallagher, N.E.; Appleton, K.M.; Young, I.S.; Edgar, J.D.; Woodside, J.V. Participating in a Fruit and Vegetable Intervention Trial Improves Longer Term Fruit and Vegetable Consumption and Barriers to Fruit and Vegetable Consumption: A Follow-up of the ADIT Study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardo, M.; Bellia, A.; Mattiuzzo, F.; Franchi, A.; Ferri, C.; Elvira, P. Frequent follow-up visits reduce weight regain in long-term management after bariatric surgery. Bariatr. Surg. Pract. Patient Care 2015, 10, 119–125. [Google Scholar] [CrossRef]
- Di Noia, J.; Cullen, K.W.; Monica, D. Social Desirability Trait Is Associated with Self-Reported Vegetable Intake among Women Enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children. J. Acad. Nutr. Diet. 2016, 116, 1942–1950. [Google Scholar] [CrossRef]
- Storm, V.; Reinwand, D.; Wienert, J.; Kuhlmann, T.; De Vries, H.; Lippke, S. Brief Report: Compensatory Health Beliefs Are Negatively Associated with Intentions for Regular Fruit and Vegetable Consumption When Self-Efficacy Is Low. J. Health Psychol. 2017, 22, 1094–1100. [Google Scholar] [CrossRef] [Green Version]
- Appleton, K.M.; Passmore, D.; Burn, I.; Pidgeon, H.; Nation, P.; Boobyer, C.; Jiang, N. An Interactive Mobile Phone App (SMART 5-A-DAY) for Increasing Knowledge of and Adherence to Fruit and Vegetable Recommendations: Development and Pilot Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e14380. [Google Scholar] [CrossRef] [Green Version]
- Ronda-Pérez, E.; Campos-Mora, J.; de Juan, A.; Gea, T.; Reid, A.; Caballero, P. Differences in the Prevalence of Fruit and Vegetable Consumption in Spanish Workers. Nutrients 2020, 12, 3848. [Google Scholar] [CrossRef] [PubMed]
- Fleary, S.A.; Joseph, P.; Chang, H. Corrigendum to “Applying the Information-Motivation-Behavioral Skills Model to Explain Adolescents’ Fruits and Vegetables Consumption”. Appetite 2020, 150, 104674. [Google Scholar] [CrossRef] [PubMed]
- Di Daniele, N.; Marrone, G.; Di Lauro, M.; Di Daniele, F.; Palazzetti, D.; Guerriero, C.; Noce, A. Effects of Caloric Restriction Diet on Arterial Hypertension and Endothelial Dysfunction. Nutrients 2021, 13, 274. [Google Scholar] [CrossRef] [PubMed]
- Molina-Jiménez, T.; Gutiérrez-García, A.G.; Hernández-Domínguez, L.; Contreras, C.M. Estrés psicosocial: Algunos aspectos clínicos y experimentales. An. Psicol 2008, 24, 353–360. [Google Scholar]
- Timlin, D.; McCormack, J.M.; Kerr, M.; Keaver, L.; Simpson, E.E.A. Are Dietary Interventions with a Behaviour Change Theoretical Framework Effective in Changing Dietary Patterns? A Systematic Review. BMC Public Health 2020, 20, 1857. [Google Scholar] [CrossRef]
- Grasso, A.C.; Olthof, M.R.; van Dooren, C.; Roca, M.; Gili, M.; Visser, M.; Cabout, M.; Bot, M.; Penninx, B.W.J.H.; van Grootheest, G.; et al. Effect of Food-Related Behavioral Activation Therapy on Food Intake and the Environmental Impact of the Diet: Results from the MooDFOOD Prevention Trial. Eur. J. Nutr. 2020, 59, 2579–2591. [Google Scholar] [CrossRef] [Green Version]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P. Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11, 160. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adherence | n1 * | n0 * | Difference ** | p-Value * | I2 * | Prop of p < 0.05 | |
|---|---|---|---|---|---|---|---|
| 0.70 | 0.10 | 356 (317; 394) | 535 (497; 574) | −4.25 (−8.33; −0.26) | 0.0266 (0.0027; 0.0727) | 57.25 (29.35; 75.73) | 85.1 |
| 0.20 | 400 (362; 441) | 491 (450; 529) | −4.91 (−9.85; −0.26) | 0.0380 (0.0033; 0.1070) | 70.36 (44.27; 86.18) | 68.1 | |
| 0.30 | 446 (400; 488) | 445 (403; 491) | −5.91 (−12.04; 0.09) | 0.0453 (0.0009; 0.1358) | 80.24 (48.77; 93.21) | 55.5 | |
| 0.80 | 0.10 | 400 (365; 437) | 491 (454; 526) | −3.82 (−6.92; −0.56) | 0.0153 (0.0016; 0.0515) | 41.72 (16.83; 63.85) | 97.3 |
| 0.20 | 444 (407; 485) | 447 (406; 484) | −4.25 (−8.06; −0.66) | 0.0257 (0.0023; 0.0806) | 56.06 (27.58; 76.91) | 85.7 | |
| 0.30 | 489 (448; 532) | 402 (359; 443) | −4.92 (−9.84; −0.05) | 0.0365 (0.0027; 0.1035) | 68.60 (40.57; 85.51) | 69.5 | |
| 0.90 | 0.10 | 444 (414; 474) | 447 (417; 177) | −3.52 (−6.08; −0.96) | 0.0059 (0.0004; 0.0281) | 22.66 (0; 45.32) | 99.9 |
| 0.20 | 488.5 (455; 523) | 402.5 (368; 436) | −3.84 (−7.14; −0.78) | 0.0139 (0.0007; 0.0503) | 38.55 (10.13; 61.45) | 97.3 | |
| 0.30 | 533.5 (496; 571) | 357.5 (320; 395) | −4.31 (−8.14; −0.70) | 0.0234 (0.0012; 0.0735) | 52.58 (20.76; 73.54) | 87.9 | |
| 0.95 | 0.10 | 467 (441; 493) | 424 (398; 450) | −3.52 (−5.92; −1.13) | 0.0003 (0.0001; 0.0007) | <0.0001 (<0.0001; 0.0002) | 100 |
| 0.20 | 512 (480; 544) | 379 (347; 411) | −3.70 (−6.53; −0.62) | 0.0086 (0.0004; 0.0366) | 28.83 (2.73; 52.46) | 99.4 | |
| 0.30 | 557 (521; 591) | 334 (300; 370) | −4.10 (−7.76; −0.58) | 0.0169 (0.00045; 0.0574) | 43.34 (11.12; 65.54) | 95 | |
| original ITT MA (two RCTs) | 444 | 447 | −3.00 (−4.92; −1.09) | 0.0021 | 0 | -- | |
| Adherence | n1 * | n0 * | Difference ** | p-Value * | I2 * | Prop of p < 0.05 | |
|---|---|---|---|---|---|---|---|
| 0.70 | 0.10 | 356 (317; 394) | 535 (497; 574) | −0.90 (−3.82; 1.77) | 0.5168 (0.4753; 0.5869) | 77.80 (71.41; 83.92) | 0 |
| 0.20 | 400 (362; 441) | 491 (450; 529) | −1.03 (−4.31; 2.59) | 0.5402 (0.4768; 0.6332) | 84.73 (77.95; 90.20) | 0 | |
| 0.30 | 446 (400; 488) | 445 (403; 491) | −1.22 (−5.99; 3.27) | 0.5581 (0.4721; 0.6914) | 89.87 (84.41; 94.68) | 0 | |
| 0.80 | 0.10 | 400 (365; 437) | 491 (454; 526) | −0.83 (−3.18; −1.62) | 0.4842 (0.4523; 0.5328) | 68.28(62.82; 76.48) | 0 |
| 0.20 | 444 (407; 485) | 447 (406; 484) | −0.91 (−3.79; 1.85) | 0.5097 (0.4653; 0.5743) | 77.00 (70.25; 84.01) | 0 | |
| 0.30 | 489 (448; 532) | 402 (359; 443) | −1.05 (−4.80; 2.40) | 0.5291 (0.4731; 0.6208) | 82.23 (76.66; 89.40) | 0 | |
| 0.90 | 0.10 | 444 (414; 474) | 447 (417, 477) | −0.79 (−2.93; 1.30) | 0.4441 (0.4203; 0.4825) | 58.89 (52.70; 66.01) | 0 |
| 0.20 | 489 (455; 523) | 403 (368; 436) | −0.86 (−3.09; 1.53) | 0.4707 (0.4412; 0.5166) | 67.36 (60.38; 74.73) | 0 | |
| 0.30 | 534 (496; 571) | 358 (320; 395) | −0.95 (−3.79; 1.98) | 0.4933 (0.4568; 0.5495) | 74.39 (67.40; 81.81) | 0 | |
| 0.95 | 0.10 | 467 (441; 493) | 424 (398, 450) | −0.78 (−2.63; 1.22) | 0.4201 (0.4000; 0.4513) | 52.90 (47.58; 59.61) | 0 |
| 0.20 | 512 (480; 544) | 379 (347; 411) | −0.84 (−2.97; 1.50) | 0.4477 (0.4252; 0.4827) | 61.66 (54.96; 69.19) | 0 | |
| 0.30 | 557 (521; 591) | 334 (300; 370) | −0.92 (−3.63; 1.82) | 0.4711 (0.4448; 0.5107) | 69.01 (61.61; 76.35) | 0 | |
| original ITT MA (two RCTs) | 444 | 447 | −0.74 * (−2.30; +0.83) | 0.3580 | 36.02 | -- | |
| Adherence | n1 * | n0 * | Difference ** | p-Value * | I2 * | Prop of p < 0.05 | |
|---|---|---|---|---|---|---|---|
| 0.70 | 0.10 | 100 (89; 111) | 151 (140; 162) | −0.28 (−0.52; −0.07) | 0.0099 (0.0026; 0.0209) | 0 (0; 0) † | 100 |
| 0.20 | 113 (101; 125) | 138 (126; 150) | −0.34 (−0.57; −0.14) | 0.00138 (0.00005; 0.0075) | 0 (0; 8.54) † | 99.9 | |
| 0.30 | 125 (112; 137) | 126 (114; 139) | −0.44 (−0.65; −0.26) | 0.00004 (<0.00001; 0.0156) | 0 (0; 67.90) † | 99.9 | |
| 0.80 | 0.10 | 113 (102; 123) | 138 (128; 149) | −0.24 (−0.46; −0.05) | 0.0223 (0.0097; 0.0367) | 0 (0; 0) | 100 |
| 0.20 | 125 (114; 137) | 126 (114; 137) | −0.29 (−0.50; −0.11) | 0.00602 (0.0012; 0.0152) | 0 (0; 0) | 100 | |
| 0.30 | 138 (125; 149) | 113 (102; 126) | −0.34 (−0.56; −0.15) | 0.00073 (0.000013; 0.0055) | 0 (0; 0) | 100 | |
| 0.90 | 0.10 | 125 (117; 134) | 126 (117; 134) | −0.21 (−0.42; −0.01) | 0.0408 (0.0248; 0.0575) | 0 (0; 0) | 85.1 |
| 0.20 | 137 (127; 147) | 114 (104; 124) | −0.24 (−0.45; −0.05) | 0.0177 (0.0067; 0.0322) | 0 (0; 0) | 100 | |
| 0.30 | 150 (139; 161) | 101 (90; 112) | −0.29 (−0.48; −0.10) | 0.0049 (0.0006; 0.0141) | 0 (0; 0) † | 100 | |
| 0.95 | 0.10 | 131 (124; 139) | 120 (112; 127) | −0.20 (−0.41; 0.02) | 0.0526 (0.0349; 0.0683) | 0 (0; 0) | 36.9 |
| 0.20 | 144 (135; 153) | 107 (98; 116) | −0.23 (−0.42; −0.03) | 0.0266 (0.0132; 0.0422) | 0 (0; 0) | 99.4 | |
| 0.30 | 156 (147; 167) | 95 (84; 104) | −0.26 (−0.48; −0.06) | 0.0095 (0.0024; 0.0208) | 0 (0; 0) † | 100 | |
| original ITT MA (two RCTs) | 125 | 126 | −0.17 ** (−0.38; 0.03) | 0.1026 | 0 | --- | |
| Adherence | n1 * | n0 * | Difference ** | p-Value * | I2 * | Prop of p < 0.05 | |
|---|---|---|---|---|---|---|---|
| 0.70 | 0.10 | 100 (89; 111) | 151 (140; 162) | −0.02 (−0.023; −0.018) | 0.6702 (0.6194; 0.7040) | 0 (0; 0) | 0 |
| 0.20 | 113 (101; 125) | 138 (126; 150) | −0.02 (−0.030; −0.021) | 0.6016 (0.5146; 0.6548) | 0 (0; 0) | 0 | |
| 0.30 | 125 (112; 137) | 126 (114; 139) | −0.03 (−0.042; −0.026) | 0.5051 (0.3710; 0.5848) | 0 (0; 0) | 0 | |
| 0.80 | 0.10 | 113 (102; 123) | 138 (128; 149) | −0.02 (−0.019; 0.016) | 0.7087 (0.6748; 0.7323) | 0 (0; 0) | 0 |
| 0.20 | 125 (114; 137) | 126 (114; 137) | −0.021 (−0.024; −0.018) | 0.6562 (0.6089; 0.6942) | 0 (0; 0) | 0 | |
| 0.30 | 138 (125; 149) | 113 (102; 126) | −0.03 (−0.031; −0.02) | 0.5911 (0.5105; 0.6489) | 0 (0; 0) | 0 | |
| 0.90 | 0.10 | 125 (117; 134) | 126 (117; 134) | −0.02 (−0.017; −0.015) | 0.7406 (0.7188; 0.7502) | 0 (0; 0) | 0 |
| 0.20 | 137 (127; 147) | 114 (104; 124) | −0.02 (−0.020; −0.016) | 0.7030 (0.6689; 0.7299) | 0 (0; 0) | 0 | |
| 0.30 | 150 (139; 161) | 101 (90; 112) | −0.02 (−0.025; −0.019) | 0.6550 (0.6019; 0.6933) | 0 (0; 0) | 0 | |
| 0.95 | 0.10 | 131 (124; 139) | 120 (112; 127) | −0.01 (−0.016; −0.014) | 0.7544 (0.7377; 0.7671) | 0 (0; 0) | 0 |
| 0.20 | 144 (135; 153) | 107 (98; 116) | −0.02 (−0.017; −0.016) | 0.7229 (0.6958; 0.7425) | 0 (0; 0) | 0 | |
| 0.30 | 156 (147; 167) | 95 (84; 104) | −0.02 (−0.047; −0.050) | 0.6824 (0.6429; 0.7103) | 0 (0; 0) | 0 | |
| original ITT MA (two RCTs) | 125 | 126 | −0.01 * (−0.10; 0.08) | 0.7907 | 0 | --- | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Espinoza, M.Á.; Lozano-Lozano, J.A.; Prieto-Merino, D. A Method to Estimate the Efficacy vs. Effectiveness in Meta-Analysis of Clinical Trials with Different Adherence Scenarios: A Monte Carlo Simulation Study in Nutrition. Nutrients 2021, 13, 2352. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072352
López-Espinoza MÁ, Lozano-Lozano JA, Prieto-Merino D. A Method to Estimate the Efficacy vs. Effectiveness in Meta-Analysis of Clinical Trials with Different Adherence Scenarios: A Monte Carlo Simulation Study in Nutrition. Nutrients. 2021; 13(7):2352. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072352
Chicago/Turabian StyleLópez-Espinoza, Miguel Ángel, José Antonio Lozano-Lozano, and David Prieto-Merino. 2021. "A Method to Estimate the Efficacy vs. Effectiveness in Meta-Analysis of Clinical Trials with Different Adherence Scenarios: A Monte Carlo Simulation Study in Nutrition" Nutrients 13, no. 7: 2352. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072352