
Effects of 60-Day Saccharomyces boulardii and Superoxide Dismutase Supplementation on Body Composition, Hunger Sensation, Pro/Antioxidant Ratio, Inflammation and Hormonal Lipo-Metabolic Biomarkers in Obese Adults: A Double-Blind, Placebo-Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
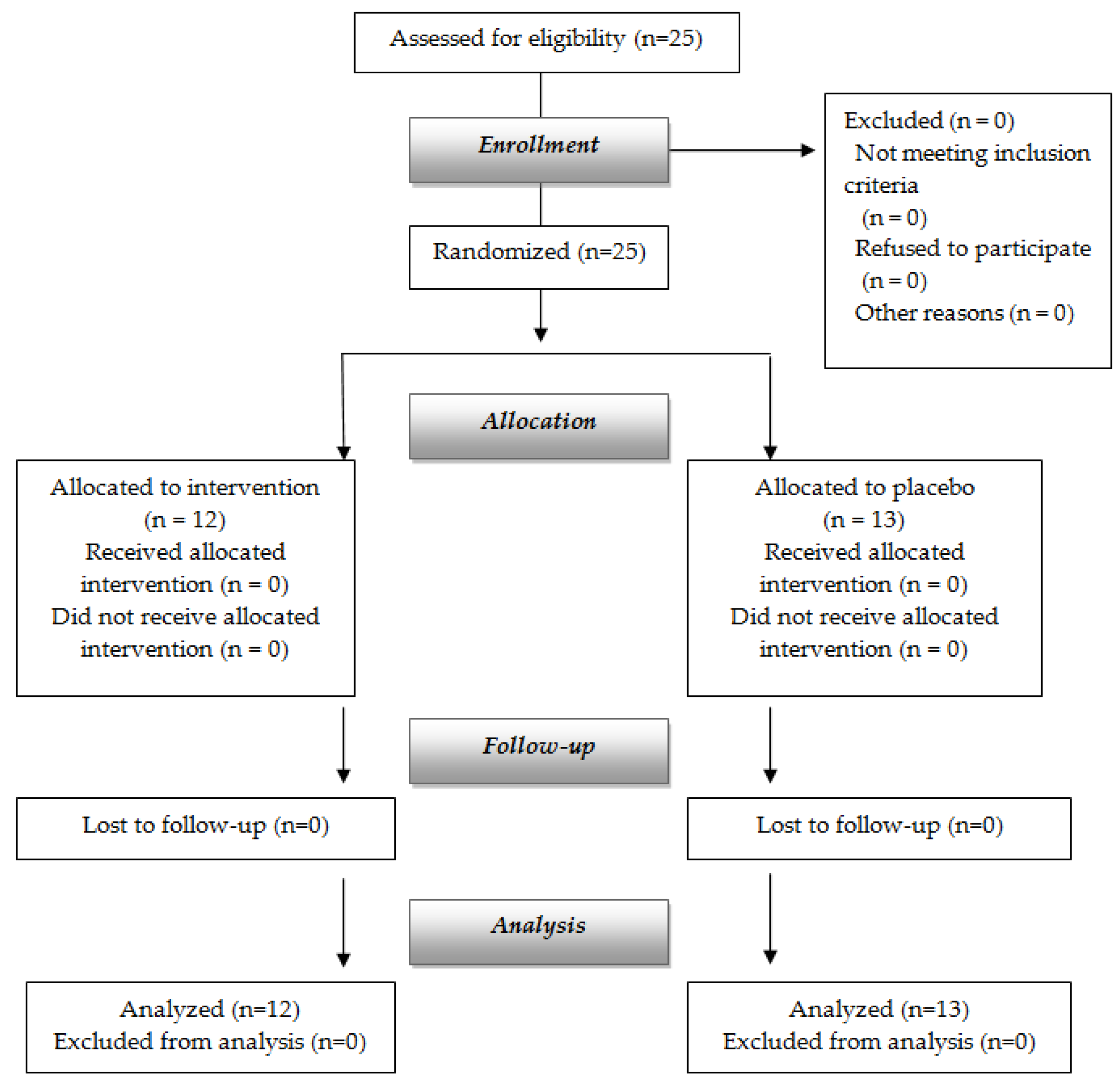
2.1. Design
2.2. Subjects
2.3. Dietary Treatment and Supplementation
2.4. Body Composition and Visceral Adipose Tissue (VAT) Assessment
2.5. Biochemical Analyses
2.6. Circulating Cytokines Evaluation
2.7. Determination of TMA and TMAO
2.8. Food Frequency Questionnaire (FFQ)
2.9. Eating Motivation Visual Analogue Scale (VAS)
2.10. Beck Depression Inventory Questionnaire (BQ)
2.11. Safety
2.12. Statistical Analysis
3. Results
4. Discussion
4.1. Effects of Supplementation on Body Composition
4.2. Effects of Supplementation on Metabolism
4.3. Effects of Supplementation on Vitamin D Levels
4.4. Effects of Supplementation on Uric Acid Levels
4.5. Role of Superoxide Dismutase
4.6. Effects of Supplementation on Other Parameters
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Tennyson, C.A.; Friedman, G. Microecology, obesity, and probiotics. Curr. Opin. Endocrinol. Diabetes Obes. 2008, 15, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Fantuzzi, G. Adipose tissue, adipokines, and inflammation. J. Allergy Clin. Immunol. 2005, 115, 911–919, quiz 920. [Google Scholar] [CrossRef]
- Cani, P.; Delzenne, N. The Role of the Gut Microbiota in Energy Metabolism and Metabolic Disease. Curr. Pharm. Des. 2009, 15, 1546–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bäckhed, F.; Ding, H.; Wang, T.; Hooper, L.V.; Koh, G.Y.; Nagy, A.; Semenkovich, C.F.; Gordon, J.I. The gut microbiota as an environmental factor that regulates fat storage. Proc. Natl. Acad. Sci. USA 2004, 101, 15718–15723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Everard, A.; Matamoros, S.; Geurts, L.; Delzenne, N.M.; Cani, P.D. Saccharomyces boulardii administration changes gut microbiota and reduces hepatic steatosis, low-grade inflammation, and fat mass in obese and type 2 diabetic db/db mice. MBio 2014, 5, e01011-14. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.-H.; Yun, S.-I.; Park, H.-O. Effects of Lactobacillus gasseri BNR17 on body weight and adipose tissue mass in diet-induced overweight rats. J. Microbiol. 2010, 48, 712–714. [Google Scholar] [CrossRef]
- Mourey, F.; Sureja, V.; Kheni, D.; Shah, P.; Parikh, D.; Upadhyay, U.; Satia, M.; Shah, D.; Troise, C.; Decherf, A. A multicenter, randomized, double-blind, placebo-controlled trial of saccharomyces boulardii in infants and children with acute diarrhea. Pediatr. Infect. Dis. J. 2020, 39, E347–E351. [Google Scholar] [CrossRef]
- McFarland, L.V.; Bernasconi, P. Saccharomyces boulardii’. A Review of an Innovative Biotherapeutic Agent. Microb. Ecol. Health Dis. 1993, 6, 157–171. [Google Scholar] [CrossRef] [Green Version]
- Brun, P.; Castagliuolo, I.; Di Leo, V.; Buda, A.; Pinzani, M.; Palù, G.; Martines, D. Increased intestinal permeability in obese mice: New evidence in the pathogenesis of nonalcoholic steatohepatitis. Am. J. Physiol. Liver Physiol. 2007, 292, G518–G525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira-Potter, V.J. Inflammation and macrophage modulation in adipose tissues. Cell. Microbiol. 2014, 16, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- John, L.J.; Fromm, M.; Schulzke, J.-D. Epithelial Barriers in Intestinal Inflammation. Antioxid. Redox Signal. 2011, 15, 1255–1270. [Google Scholar] [CrossRef]
- Fernández-Sánchez, A.; Madrigal-Santillán, E.; Bautista, M.; Esquivel-Soto, J.; Morales-González, Á.; Esquivel-Chirino, C.; Durante-Montiel, I.; Sánchez-Rivera, G.; Valadez-Vega, C.; Morales-González, J.A. Inflammation, oxidative stress, and obesity. Int. J. Mol. Sci. 2011, 12, 3117–3132. [Google Scholar] [CrossRef] [Green Version]
- Yasui, K.; Baba, A. Therapeutic potential of superoxide dismutase (SOD) for resolution of inflammation. Inflamm. Res. 2006, 55, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Carillon, J.; Romain, C.; Bardy, G.; Fouret, G.; Feillet-Coudray, C.; Gaillet, S.; Lacan, D.; Cristol, J.P.; Rouanet, J.M. Cafeteria diet induces obesity and insulin resistance associated with oxidative stress but not with inflammation: Improvement by dietary supplementation with a melon superoxide dismutase. Free Radic. Biol. Med. 2013, 65, 254–261. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association; Biondi, M.; Maj, M. DSM-V: Manuale Diagnostico e Statistico dei Disturbi Mentali: Text Revisiion; Raffaello Cortina: Milan, Italy, 2014. [Google Scholar]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Mohammad, A.; De Lucia Rolfe, E.; Sleigh, A.; Kivisild, T.; Behbehani, K.; Wareham, N.J.; Brage, S.; Mohammad, T. Validity of visceral adiposity estimates from DXA against MRI in Kuwaiti men and women. Nutr. Diabetes 2017, 7, e238. [Google Scholar] [CrossRef]
- Haffner, S.M.; Kennedy, E.; Gonzalez, C.; Stern, M.P.; Miettinen, H. A prospective analysis of the HOMA model. The Mexico City Diabetes Study. Diabetes Care 1996, 19, 1138–1141. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Grinberga, S.; Dambrova, M.; Latkovskis, G.; Strele, I.; Konrade, I.; Hartmane, D.; Sevostjanovs, E.; Liepinsh, E.; Pugovics, O. Determination of trimethylamine-N-oxide in combination with l-carnitine and γ-butyrobetaine in human plasma by UPLC/MS/MS. Biomed. Chromatogr. 2015, 29, 1670–1674. [Google Scholar] [CrossRef]
- Buscemi, S.; Rosafio, G.; Vasto, S.; Massenti, F.M.; Grosso, G.; Galvano, F.; Rini, N.; Barile, A.M.; Maniaci, V.; Cosentino, L.; et al. Validation of a food frequency questionnaire for use in Italian adults living in Sicily. Int. J. Food Sci. Nutr. 2015, 66, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.; de Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; van der Knaap, H.; et al. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. 2010, 11, 251–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubbs, R.J.; Hughes, D.A.; Johnstone, A.M.; Rowley, E.; Reid, C.; Elia, M.; Stratton, R.; Delargy, H.; King, N.; Blundell, J.E. The use of visual analogue scales to assess motivation to eat in human subjects: A review of their reliability and validity with an evaluation of new hand-held computerized systems for temporal tracking of appetite ratings. Br. J. Nutr. 2000, 84, 405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharafedtinov, K.K.; Plotnikova, O.A.; Alexeeva, R.I.; Sentsova, T.B.; Songisepp, E.; Stsepetova, J.; Smidt, I.; Mikelsaar, M. Hypocaloric diet supplemented with probiotic cheese improves body mass index and blood pressure indices of obese hypertensive patients—A randomized double-blind placebo-controlled pilot study. Nutr. J. 2013, 12, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus, S.P.; Ellero, S.L.; Berger, B.; Krause, L.; Bruttin, A.; Molina, J.; Paris, A.; Want, E.J.; de Waziers, I.; Cloarec, O.; et al. Colonization-induced host-gut microbial metabolic interaction. MBio 2011, 2, e00271-10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cani, P.D. Metabolism in 2013: The gut microbiota manages host metabolism. Nat. Rev. Endocrinol. 2014, 10, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Petschow, B.; Doré, J.; Hibberd, P.; Dinan, T.; Reid, G.; Blaser, M.; Cani, P.D.; Degnan, F.H.; Foster, J.; Gibson, G.; et al. Probiotics, prebiotics, and the host microbiome: The science of translation. Ann. N. Y. Acad. Sci. 2013, 1306, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.M.; Blaser, M.J. Pathways in microbe-induced obesity. Cell Metab. 2013, 17, 883–894. [Google Scholar] [CrossRef] [Green Version]
- Delzenne, N.M.; Neyrinck, A.M.; Bäckhed, F.; Cani, P.D. Targeting gut microbiota in obesity: Effects of prebiotics and probiotics. Nat. Rev. Endocrinol. 2011, 7, 639–646. [Google Scholar] [CrossRef]
- Molinaro, F.; Paschetta, E.; Cassader, M.; Gambino, R.; Musso, G. Probiotics, prebiotics, energy balance, and obesity: Mechanistic insights and therapeutic implications. Gastroenterol. Clin. N. Am. 2012, 41, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, L.; Huang, Y.; Parini, P.; Korach-André, M.; Håkansson, J.; Gustafsson, J.-Å.; Pettersson, S.; Arulampalam, V.; Rafter, J. Decreased fat storage by Lactobacillus paracasei is associated with increased levels of angiopoietin-like 4 protein (ANGPTL4). PLoS ONE 2010, 5, e13087. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Anastasovska, J.; Gibson, G.; Tuohy, K.; Sharma, R.K.; Bell, J.; Frost, G. Effect of Lactobacillus acidophilus NCDC 13 supplementation on the progression of obesity in diet-induced obese mice. Br. J. Nutr. 2012, 108, 1382–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fåk, F.; Bäckhed, F. Lactobacillus reuteri Prevents Diet-Induced Obesity, but not Atherosclerosis, in a Strain Dependent Fashion in Apoe-/- Mice. PLoS ONE 2012, 7, e46837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.J.; Wang, R.; Li, X.; Wang, R. Bifidobacterium longum supplementation improved high-fat-fed-induced metabolic syndrome and promoted intestinal Reg I gene expression. Exp. Biol. Med. (Maywood) 2011, 236, 823–831. [Google Scholar] [CrossRef]
- Gauffin Cano, P.; Santacruz, A.; Moya, Á.; Sanz, Y. Bacteroides uniformis CECT 7771 ameliorates metabolic and immunological dysfunction in mice with high-fat-diet induced obesity. PLoS ONE 2012, 7, e41079. [Google Scholar]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C.A.S.T.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, M.; Cesi, V.; Palone, F.; Pierdomenico, M.; Colantoni, E.; Leter, B.; Vitali, R.; Negroni, A.; Cucchiara, S.; Stronati, L. Krill oil, vitamin D and Lactobacillus reuteri cooperate to reduce gut inflammation. Benef. Microbes 2018, 9, 389–399. [Google Scholar] [CrossRef] [Green Version]
- Shang, M.; Sun, J. Vitamin D/VDR, Probiotics, and Gastrointestinal Diseases. Curr. Med. Chem. 2017, 24, 876–887. [Google Scholar] [CrossRef]
- Jones, M.L.; Martoni, C.J.; Prakash, S. Oral supplementation with probiotic L. reuteri NCIMB 30242 increases mean circulating 25-hydroxyvitamin D: A post hoc analysis of a randomized controlled trial. J. Clin. Endocrinol. Metab. 2013, 98, 2944–2951. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, L.F.; de Azevedo, L.G.; da Mota Santana, J.; de Sales, L.P.C.; Pereira-Santos, M. Obesity and overweight decreases the effect of vitamin D supplementation in adults: Systematic review and meta-analysis of randomized controlled trials. Rev. Endocr. Metab. Disord. 2020, 21, 67–76. [Google Scholar] [CrossRef]
- Tsushima, Y.; Nishizawa, H.; Tochino, Y.; Nakatsuji, H.; Sekimoto, R.; Nagao, H.; Shirakura, T.; Kato, K.; Imaizumi, K.; Takahashi, H.; et al. Uric acid secretion from adipose tissue and its increase in obesity. J. Biol. Chem. 2013, 288, 27138–27149. [Google Scholar] [CrossRef] [Green Version]
- Hikita, M.; Ohno, I.; Mori, Y.; Ichida, K.; Yokose, T.; Hosoya, T. Relationship between hyperuricemia and body fat distribution. Intern. Med. 2007, 46, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Tamba, S.; Nishizawa, H.; Funahashi, T.; Okauchi, Y.; Ogawa, T.; Noguchi, M.; Fujita, K.; Ryo, M.; Kihara, S.; Iwahashi, H.; et al. Relationship between the serum uric acid level, visceral fat accumulation and serum adiponectin concentration in Japanese men. Intern. Med. 2008, 47, 1175–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.H.; Lee, S.S.; Yoo, J.H.; Kim, S.R.; Yoo, S.J.; Song, H.C.; Kim, Y.-S.; Choi, E.J.; Kim, Y.K. The relationship between the regional abdominal adipose tissue distribution and the serum uric acid levels in people with type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2012, 4, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathmann, W.; Haastert, B.; Icks, A.; Giani, G.; Roseman, J.M. Ten-year change in serum uric acid and its relation to changes in other metabolic risk factors in young black and white adults: The CARDIA study. Eur. J. Epidemiol. 2007, 22, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, T.A.; Turner, S.T.; Peyser, P.A.; Bielak, L.F.; Sheedy, P.F.; Kullo, I.J. Associations of serum uric acid with markers of inflammation, metabolic syndrome, and subclinical coronary atherosclerosis. Am. J. Hypertens. 2007, 20, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.D.; Tsai, D.H.; Hsu, S.R. Association between serum uric acid level and components of the metabolic syndrome. J. Chin. Med. Assoc. 2006, 69, 512–516. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International atherosclerosis society; And international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Matsuzawa, Y.; Funahashi, T.; Nakamura, T. The concept of metabolic syndrome: Contribution of visceral fat accumulation and its molecular mechanism. J. Atheroscler. Thromb. 2011, 18, 629–639. [Google Scholar] [CrossRef] [Green Version]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castañeda-Sanabria, J.; Coyfish, M.; Guillo, S.; Jansen, T.L.; Janssens, H.; et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2017, 76, 29–42. [Google Scholar] [CrossRef]
- Hosogai, N.; Fukuhara, A.; Oshima, K.; Miyata, Y.; Tanaka, S.; Segawa, K.; Furukawa, S.; Tochino, Y.; Komuro, R.; Matsuda, M.; et al. Adipose tissue hypoxia in obesity and its impact on adipocytokine dysregulation. Diabetes 2007, 56, 901–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenstein, A.S.; Khavandi, K.; Withers, S.B.; Sonoyama, K.; Clancy, O.; Jeziorska, M.; Laing, I.; Yates, A.P.; Pemberton, P.W.; Malik, R.A.; et al. Local inflammation and hypoxia abolish the protective anticontractile properties of perivascular fat in obese patients. Circulation 2009, 119, 1661–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nauck, M.A.; Meier, J.J. Incretin hormones: Their role in health and disease. Diabetes Obes. Metab. 2018, 20, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Karelis, A.D.; Brochu, M.; Rabasa-Lhoret, R. Can we identify metabolically healthy but obese individuals (MHO)? Diabetes Metab. 2004, 30, 569–572. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Intervention (Mean Values ± SD) | Placebo (Mean Values ± SD) | Total (Mean Values ± SD) | p-Value |
|---|---|---|---|---|
| General characteristics | ||||
| Gender (women/men) | 8/4 | 9/4 | 17/8 | Χ2 = 0.019 p = 0.891 |
| Age | 57.33 ± 8.86 | 50.31 ± 9.54 | 53.68 ± 9.71 | 0.644 |
| Body composition by DXA | ||||
| Free Fat Mass (kg) | 51.31 ± 7.60 | 51.42 ± 8.31 | 51.37 ± 7.81 | 0.569 |
| Fat Mass (kg) | 44.31 ± 10.05 | 43.65 ± 9.84 | 43.96 ± 9.72 | 0.922 |
| Android fat (%) | 51.71 ± 7.28 | 52.29 ± 7.33 | 52.01 ± 7.16 | 0.921 |
| Gynoid fat (%) | 45.42 ± 9.99 | 47.24 ± 8.93 | 46.36 ± 9.30 | 0.520 |
| VAT (g) | 1838.33 ± 699.33 | 1844.69 ± 931.57 | 1841.64 ± 811.22 | 0.561 |
| Weight (kg) | 96.63 ± 12.38 | 97.83 ± 11.76 | 97.26 ± 11.82 | 0.993 |
| Anthropometric measures | ||||
| Height (m) | 1.67 ± 0.06 | 1.67 ± 0.07 | 1.67 ± 0.07 | 0.360 |
| BMI (kg/m2) | 34.60 ± 3.03 | 35.04 ± 3.17 | 34.83 ± 3.05 | 0.889 |
| Others | ||||
| Homa index (points) | 2.20 ± 0.86 | 2.02 ± 1.25 | 2.21 ± 1.22 | 0.704 |
| Beck Questionnaire (points) | 5.55 ± 4.91 | 7.58 ± 5.50 | 6.61 ± 5.21 | 0.401 |
| Blood tests | ||||
| Total cholesterol (mg/dL) | 206.08 ± 20.57 | 215.60 ± 18.15 | 210.41 ± 19.66 | 0.263 |
| LDL cholesterol (mg/dL) | 132.33 ± 17.57 | 137.70 ± 21.90 | 134.87 ± 19.43 | 0.546 |
| HDL cholesterol (mg/dL) | 59.09 ± 10.32 | 61.10 ± 18.27 | 60.05 ± 14.30 | 0.764 |
| Triglycerides (mg/dL) | 79.00 ± 28.20 | 93.33 ± 27.71 | 86.17 ± 28.11 | 0.781 |
| Glycemia (mg/dL) | 89.75 ± 14.57 | 88.54 ± 10.19 | 89.12 ± 12.23 | 0.270 |
| Insulin (mcU/mL) | 9.90 ± 3.91 | 8.81 ± 4.93 | 9.82 ± 4.86 | 0.573 |
| Apolipoprotein A (mg/dL) | 163.08 ± 31.90 | 168.27 ± 37.72 | 165.57 ± 34.09 | 0.221 |
| Apolipoprotein B (mg/dL) | 115.50 ± 27.08 | 121.00 ± 21.87 | 118.37 ± 22.92 | 0.669 |
| AST (U/L) | 19.50 ± 5.92 | 20.69 ± 5.76 | 20.12 ± 5.75 | 0.736 |
| ALT (U/L) | 21.17 ± 12.22 | 22.00 ± 9.63 | 21.60 ± 10.72 | 0.210 |
| δGT (U/L) | 18.52 ± 10.30 | 17.12 ± 5.67 | 17.82 ± 8.16 | 0.149 |
| Creatinine (mg/dL) | 0.68 ± 0.18 | 0.78 ± 0.16 | 0.74 ± 0.17 | 0.806 |
| Total Proteins (g/dL) | 7.00 ± 0.48 | 7.00 ± 0.49 | 7.00 ± 0.48 | 0.782 |
| Albumin (g/dL) | 4.41 ± 0.36 | 4.33 ± 0.39 | 4.37 ± 0.37 | 0.657 |
| CRP (mg/dL) | 0.10 ± 0.09 | 0.25 ± 0.25 | 0.18 ± 0.20 | 0.078 |
| Uric acid (mg/dL) | 4.21 ± 1.29 | 4.35 ± 1.08 | 4.28 ± 1.16 | 0.265 |
| Fe (µg/dL) | 79.50 ± 28.61 | 82.38 ± 38.66 | 81.00 ± 33.53 | 0.307 |
| TSH (µU/dL) | 1.58 ± 1.19 | 1.73 ± 1.33 | 1.65 ± 1.23 | 0.860 |
| Leptin (ng/cL) | 3.94 ± 3.20 | 4.41 ± 2.91 | 4.19 ± 3.00 | 0.811 |
| Ghrelin (pg/mL) | 6.40 ± 1.35 | 5.77 ± 1.84 | 6.07 ± 1.62 | 0.566 |
| Adiponectin (pg/mL) | 149.50 ± 127.72 | 125.38 ± 69.49 | 135.54 ± 89.45 | 0.263 |
| Peptide YY (pg/mL) | 267.58 ± 46.77 | 283.58 ± 74.46 | 275.90 ± 61.98 | 0.073 |
| GLP-1 (pmol/L) | 10.94 ± 23.18 | 7.30 ± 11.41 | 9.05 ± 17.74 | 0.311 |
| TNF-α (pg/mL) | 66.50 ± 110.18 | 40.20 ± 29.54 | 39.11 ± 22.58 | 0.185 |
| Variables | Intervention | Placebo | Difference between Groups (Confidence Interval) | p-Value between Groups |
|---|---|---|---|---|
| Δ T1-T0 (confidence interval) | Δ T1-T0 (confidence interval) | |||
| DXA | ||||
| Free Fat Mass (kg) | 0.04 (−0.85; 0.93) | 0.20 (−0.65; 1.05) | −0.15 (−1.44; 1.13) | 0.805 |
| Fat Mass (kg) | −3.13 (−5.22; −1.05) * | −1.88 (−3.78; 0.02) | −1.25 (−4.21; 1.70) | 0.385 |
| Android fat (%) | −2.13 (−3.63; −0.63) * | −0.62 (−2.06; 0.82) | −1.51 (−3.67; 0.65) | 0.160 |
| Gynoid fat (%) | −1.01 (−2.40; 0.38) | −0.64 (−1.97; 0.69) | −0.37 (−2.37; 1.63) | 0.702 |
| VAT (g) | −132.16 (−349.27; 84.94) | −135.00 (−342.80; 72.80) | 2.84 (−311.54; 317.22) | 0.985 |
| DXA Weight (kg) | −2.73 (−4.72; −0.74) * | −1.00 (−2.90; 0.90) | −1.73 (−4.60; 1.14) | 0.223 |
| Anthropometric measures | ||||
| BMI (kg/m2) | −0.97 (−1.70; −0.25) * | −0.36 (−1.05; 0.34) | −0.62 (−1.67; 0.43) | 0.235 |
| Others | ||||
| Homa index (points) | −0.48 (−0.87; −0.09) * | −0.16 (−0.06; 0.23) | −0.31 (−0.91; 0.28) | 0.280 |
| Beck Questionnaire (points) | −1.36 (−3.47; 0.75) | −0.59 (−2.59; 1.42) | −0.77 (−3.86; 2.32) | 0.606 |
| Blood tests | ||||
| Total cholesterol (mg/dL) | 7.31 (−0.83; 15.46) | −4.38 (−13.35; 4.60) | 11.69 (−0.82; 24.20) * | 0.065 |
| LDL cholesterol (mg/dL) | 6.08 (−3.15; 15.32) | −6.07 (−15.79; 3.65) | 12.15 (−1.80; 26.10) | 0.083 |
| HDL cholesterol (mg/dL) | 0.75 (−1.91; 3.40) | 0.58 (−2.22; 3.37) | 0.17 (−3.86; 4.20) | 0.930 |
| Triglycerides (mg/dL) | 2.27 (−10.30; 14.84) | 3.84 (−8.73; 16.41) | −1.57 (−20.06; 16.92) | 0.857 |
| Glycemia (mg/dL) | 1.49 (−2.86; 5.84) | −3.22 (−7.39; 0.94) | 4.72 (−1.54; 10.97) | 0.132 |
| Insulin (mcU/mL) | −2.27 (−3.83; −0.71) * | −0.55 (−2.11; 1.01) | −1.72 (−4.09; 0.65) | 0.145 |
| Apolipoprotein A (mg/dL) | 1.52 (−5.84; 8.87) | −1.75 (−9.46; 5.96) | 3.26 (−7.81; 14.34) | 0.544 |
| Apolipoprotein B (mg/dL) | 5.27 (−4.06; 14.59) | 7.03 (−1.81; 15.87) | −1.76 (−15.40; 11.87) | 0.787 |
| AST (U/L) | −1.46 (−3.49; 0.57) | −0.88 (−2.83; 1.06) | −0.58 (−3.51; 2.35) | 0.684 |
| ALT (U/L) | −2.11 (−4.55; 0.34) | −3.39 (−5.94; −0.83) * | −1.28 (−4.95; 2.39) | 0.475 |
| δGT (U/L) | −1.49 (−2.99; 0.02) | 0.01 (−1.49; 1.52) | −1.50 (−3.70; 0.70) | 0.170 |
| Creatinin (mg/dL) | −0.00 (−0.04; 0.04) | 0.02 (−0.02; 0.06) | −0.02 (−0.08; 0.04) | 0.566 |
| Total Proteins (g/dL) | 0.11 (−0.14; 0.36) | −0.18 (−0.44; 0.08) | 0.29 (−0.09; 0.67) | 0.131 |
| Albumin (g/dL) | −0.01 (−0.21; 0.19) | −0.17 (−0.39; 0.04) | 0.17 (−0.13; 0.47) | 0.249 |
| CRP (mg/dL) | 0.01 (−0.09; 0.08) | −0.01 (−0.08; 0.09) | 0.02 (−0.11; 0.15) | 0.799 |
| Uric acid (mg/dL) | −0.50 (−0.98; −0.02) * | −0.10 (−0.56; 0.36) | −0.40 (−1.09; 0.29) | 0.240 |
| Fe (µg/dL) | 7.13 (−12.93; 27.19) | −1.97 (−21.17; 17.24) | 9.10 (−19.81; 38.00) | 0.519 |
| TSH (µU/dL) | −0.30 (−0.59; 0.00) | −0.12 (−0.43; 0.20) | −0.18 (−0.64; 0.28) | 0.420 |
| Leptin (ng/cL) | −0.45 (−1.60; 0.71) | −0.24 (−1.34; 0.87) | −0.21 (−1.88; 1.46) | 0.796 |
| Ghrelin (pg/mL) | −0.48 (−1.64; 0.67) | −1.28 (−2.39; −0.18) * | 0.80 (−0.88; 2.48) | 0.331 |
| Adiponectin (pg/mL) | 7.68 (−73.60; 88.97) | −7.88 (−74.50; 58.73) | 15.57 (−95.33; 126.46) | 0.765 |
| Peptide YY (pg/mL) | −15.12 (−39.56; 9.32) | 4.03 (−19.38; 27.43) | −19.14 (−54.37; 16.08) | 0.270 |
| GLP-1 (pmol/L) | −2.39 (−3.27; −1.51) * | −2.05 (−2.89; −1.21) * | −0.34 (−1.60; 0.92) | 0.576 |
| TNF-α (pg/mL) | −5.46 (−14.88; 3.95) | −8.79 (−17.81; 0.23) | 3.33 (−10.23; 16.89) | 0.614 |
| IL-1β (pg/mL) | −0.56 (−2.16; 1.03) | 0.54 (−0.92; 2.00) | −1.11 (−3.35; 1.14) | 0.315 |
| IL-6 (pg/mL) | −3.84 (−58.70; 51.01) | −5.24 (−62.75; 52.26) | 1.40 (−81.35; 84.15) | 0.972 |
| TMA (µM) | 0.67 (−6.76; 8.10) | 4.86 (−1.72; 11.45) | −4.19 (−14.48; 6.10) | 0.395 |
| TMAO (µM) | −1.42 (−3.54; 0.70) | 1.36 (−0.87; 3.59) | −2.78 (−5.99; 0.42) | 0.084 |
| Vitamin D (ng/mL) | 5.22 (1.56; 8.88) * | 1.27 (−2.24; 4.77) | 3.95 (−1.33; 9.24) | 0.134 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rondanelli, M.; Miraglia, N.; Putignano, P.; Castagliuolo, I.; Brun, P.; Dall’Acqua, S.; Peroni, G.; Faliva, M.A.; Naso, M.; Nichetti, M.; et al. Effects of 60-Day Saccharomyces boulardii and Superoxide Dismutase Supplementation on Body Composition, Hunger Sensation, Pro/Antioxidant Ratio, Inflammation and Hormonal Lipo-Metabolic Biomarkers in Obese Adults: A Double-Blind, Placebo-Controlled Trial. Nutrients 2021, 13, 2512. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082512
Rondanelli M, Miraglia N, Putignano P, Castagliuolo I, Brun P, Dall’Acqua S, Peroni G, Faliva MA, Naso M, Nichetti M, et al. Effects of 60-Day Saccharomyces boulardii and Superoxide Dismutase Supplementation on Body Composition, Hunger Sensation, Pro/Antioxidant Ratio, Inflammation and Hormonal Lipo-Metabolic Biomarkers in Obese Adults: A Double-Blind, Placebo-Controlled Trial. Nutrients. 2021; 13(8):2512. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082512
Chicago/Turabian StyleRondanelli, Mariangela, Niccolò Miraglia, Pietro Putignano, Ignazio Castagliuolo, Paola Brun, Stefano Dall’Acqua, Gabriella Peroni, Milena Anna Faliva, Maurizio Naso, Mara Nichetti, and et al. 2021. "Effects of 60-Day Saccharomyces boulardii and Superoxide Dismutase Supplementation on Body Composition, Hunger Sensation, Pro/Antioxidant Ratio, Inflammation and Hormonal Lipo-Metabolic Biomarkers in Obese Adults: A Double-Blind, Placebo-Controlled Trial" Nutrients 13, no. 8: 2512. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082512