
Hepcidin and Iron Deficiency in Women One Year after Sleeve Gastrectomy: A Prospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Setting
2.2. Endpoints
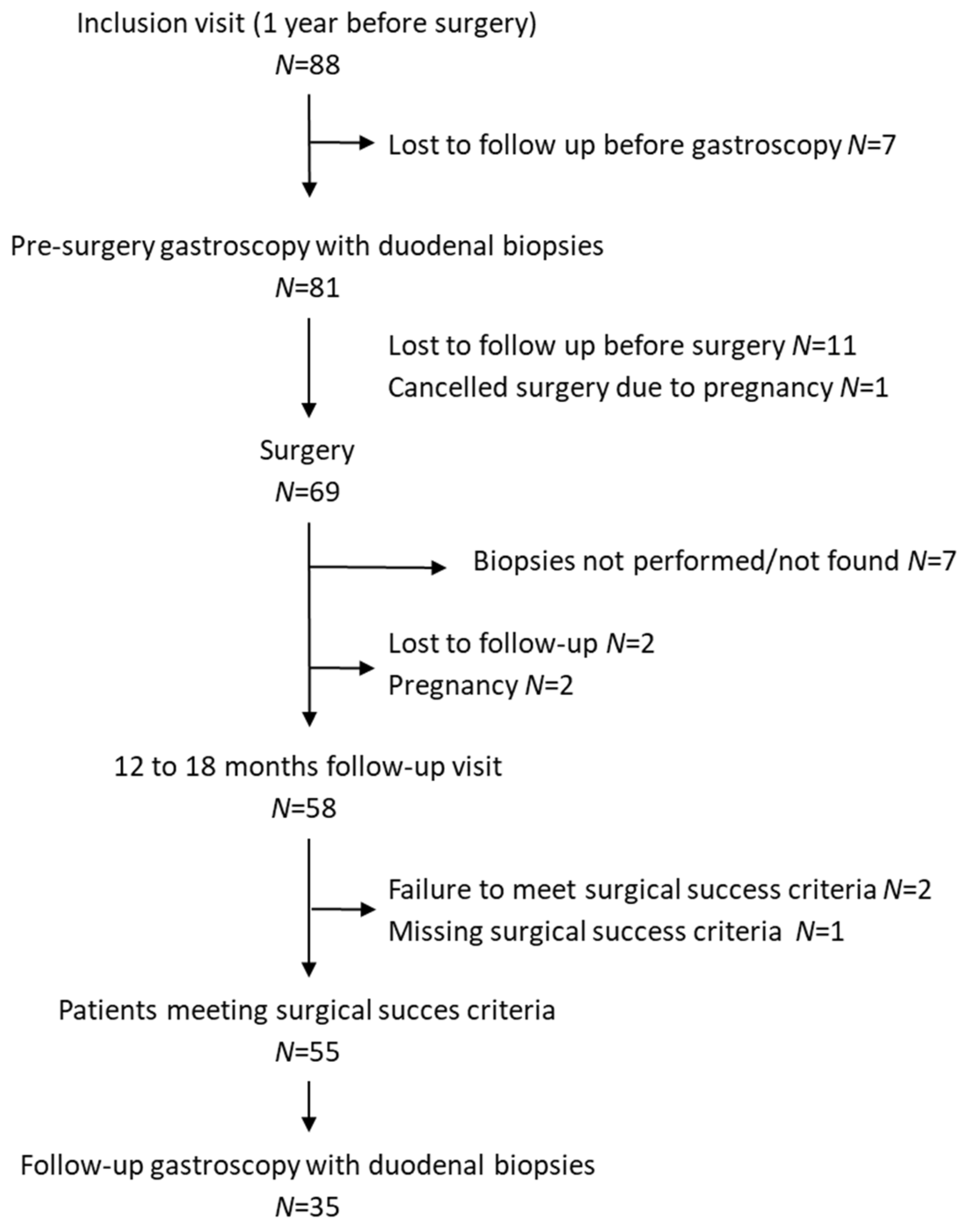
2.3. Inclusion and Follow-Up
2.4. Hematological and Biochemical Analysis
2.5. ARN, RT-qPCR
2.6. Extraction Protein, Western Blot
2.7. Statistical Analyses
3. Results
3.1. Characteristics of the SG Patients
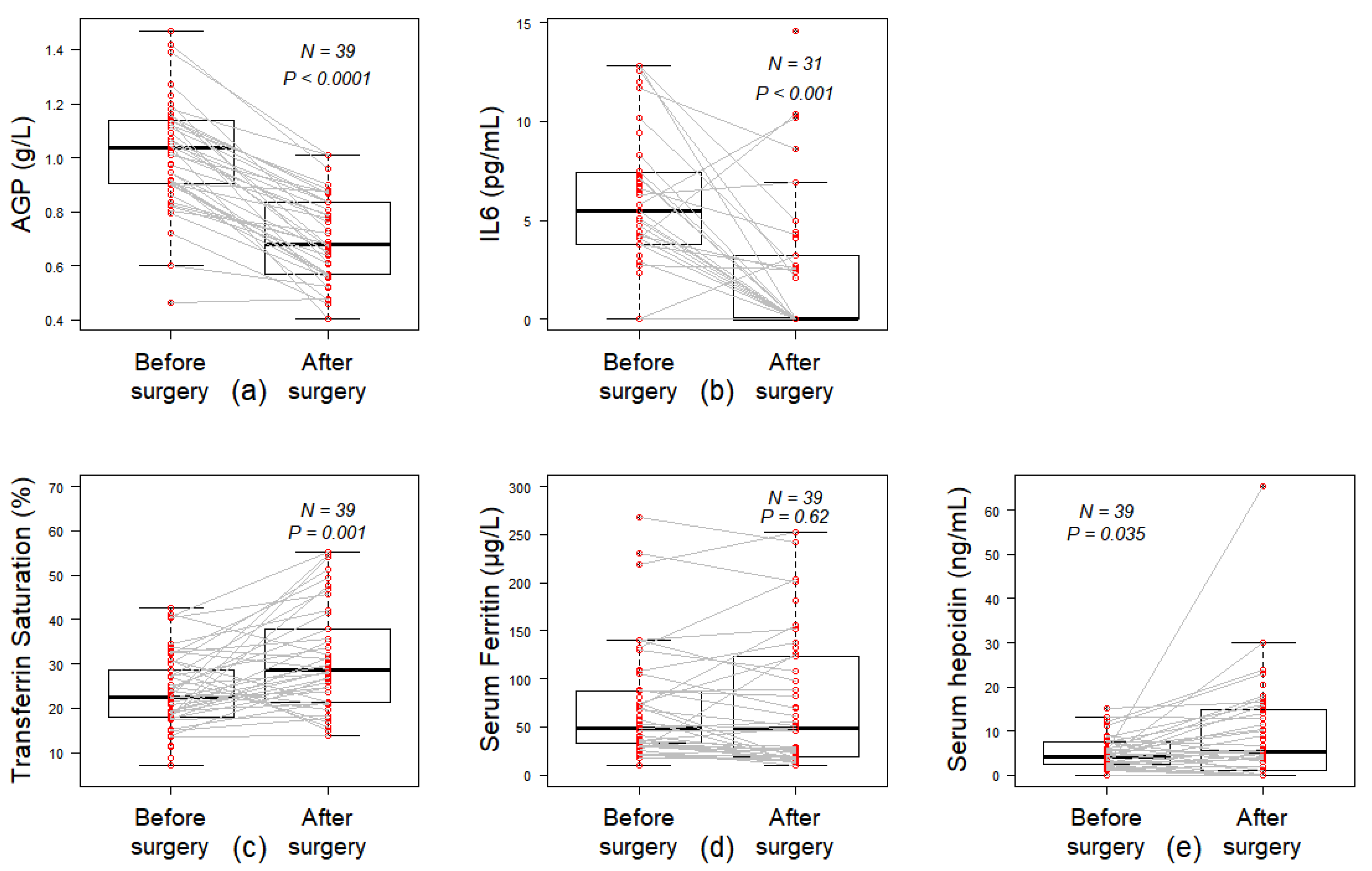
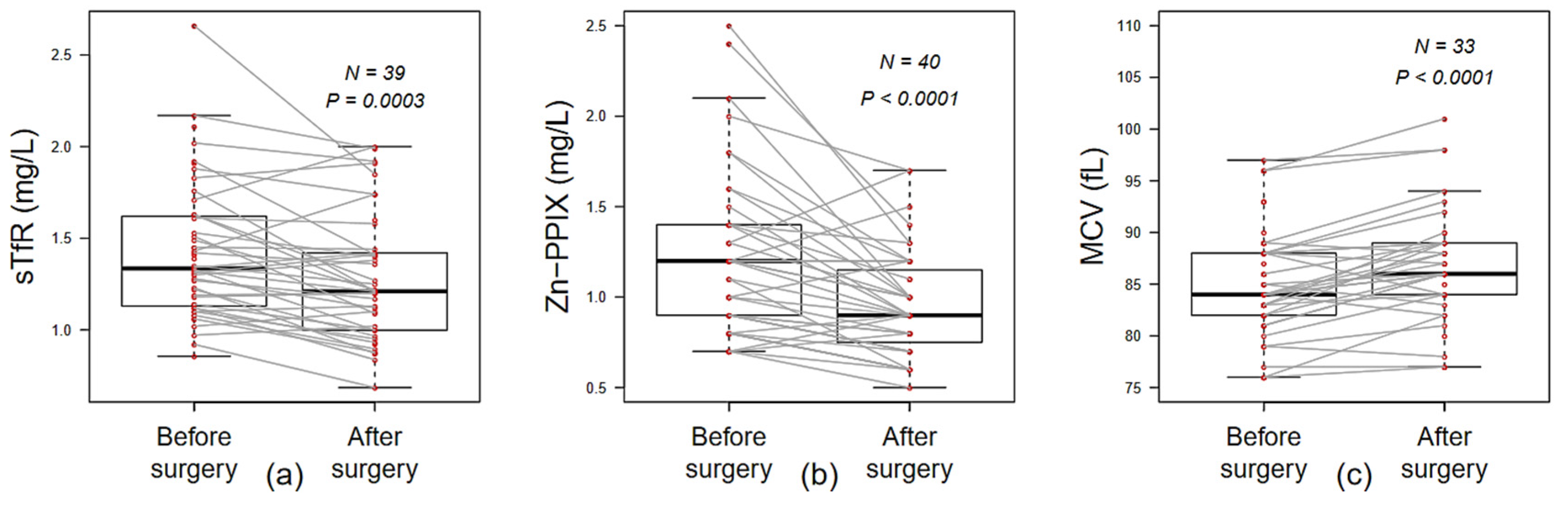
3.2. Recovery from Systemic and Erythroid Iron Deficiency
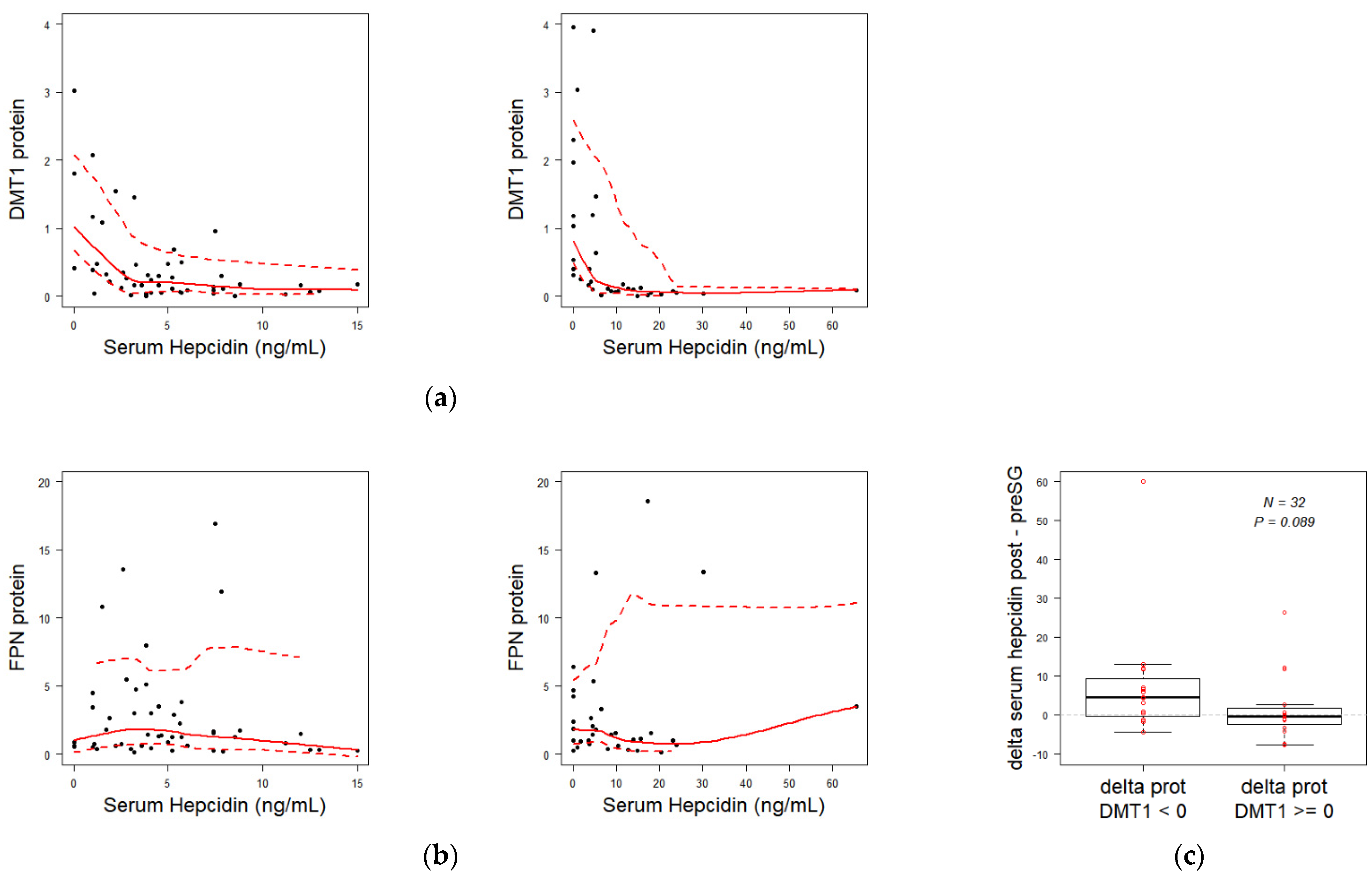
3.3. Duodenal Iron Intake Explorations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 14 July 2021).
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef]
- Khanbhai, M.; Dubb, S.; Patel, K.; Ahmed, A.; Richards, T. The Prevalence of Iron Deficiency Anaemia in Patients Undergoing Bariatric Surgery. Obes. Res. Clin. Pract. 2015, 9, 45–49. [Google Scholar] [CrossRef]
- Yanoff, L.B.; Menzie, C.M.; Denkinger, B.; Sebring, N.G.; McHugh, T.; Remaley, A.T.; Yanovski, J.A. Inflammation and Iron Deficiency in the Hypoferremia of Obesity. Int. J. Obes. 2005 2007, 31, 1412–1419. [Google Scholar] [CrossRef] [Green Version]
- Aigner, E.; Feldman, A.; Datz, C. Obesity as an Emerging Risk Factor for Iron Deficiency. Nutrients 2014, 6, 3587–3600. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, X.; Shen, Y.; Fang, X.; Wang, Y.; Wang, F. Obesity and Iron Deficiency: A Quantitative Meta-Analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 1081–1093. [Google Scholar] [CrossRef]
- Enani, G.; Bilgic, E.; Lebedeva, E.; Delisle, M.; Vergis, A.; Hardy, K. The Incidence of Iron Deficiency Anemia Post-Roux-En-Y Gastric Bypass and Sleeve Gastrectomy: A Systematic Review. Surg. Endosc. 2020, 34, 3002–3010. [Google Scholar] [CrossRef]
- Gehrer, S.; Kern, B.; Peters, T.; Christoffel-Courtin, C.; Peterli, R. Fewer Nutrient Deficiencies after Laparoscopic Sleeve Gastrectomy (LSG) than after Laparoscopic Roux-Y-Gastric Bypass (LRYGB)-a Prospective Study. Obes. Surg. 2010, 20, 447–453. [Google Scholar] [CrossRef]
- Patel, J.J.; Mundi, M.S.; Hurt, R.T.; Wolfe, B.; Martindale, R.G. Micronutrient Deficiencies After Bariatric Surgery: An Emphasis on Vitamins and Trace Minerals [Formula: See Text]. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2017, 32, 471–480. [Google Scholar] [CrossRef]
- Cook, J.D.; Skikne, B.S.; Lynch, S.R.; Reusser, M.E. Estimates of Iron Sufficiency in the US Population. Blood 1986, 68, 726–731. [Google Scholar] [CrossRef] [Green Version]
- Bothwell, T.H.; Charlton, R.W. A General Approach to the Problems of Iron Deficiency and Iron Overload in the Population at Large. Semin. Hematol. 1982, 19, 54–67. [Google Scholar]
- Seif, M.W.; Diamond, K.; Nickkho-Amiry, M. Obesity and Menstrual Disorders. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 516–527. [Google Scholar] [CrossRef] [PubMed]
- McCance, R.A.; Widdowson, E.M. The Absorption and Excretion of Iron Following Oral and Intravenous Administration. J. Physiol. 1938, 94, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Illing, A.C.; Shawki, A.; Cunningham, C.L.; Mackenzie, B. Substrate Profile and Metal-Ion Selectivity of Human Divalent Metal-Ion Transporter-1. J. Biol. Chem. 2012, 287, 30485–30496. [Google Scholar] [CrossRef] [Green Version]
- Gunshin, H.; Mackenzie, B.; Berger, U.V.; Gunshin, Y.; Romero, M.F.; Boron, W.F.; Nussberger, S.; Gollan, J.L.; Hediger, M.A. Cloning and Characterization of a Mammalian Proton-Coupled Metal-Ion Transporter. Nature 1997, 388, 482–488. [Google Scholar] [CrossRef]
- Canonne-Hergaux, F.; Gruenheid, S.; Ponka, P.; Gros, P. Cellular and Subcellular Localization of the Nramp2 Iron Transporter in the Intestinal Brush Border and Regulation by Dietary Iron. Blood 1999, 93, 4406–4417. [Google Scholar] [CrossRef]
- Shawki, A.; Knight, P.B.; Maliken, B.D.; Niespodzany, E.J.; Mackenzie, B. H(+)-Coupled Divalent Metal-Ion Transporter-1: Functional Properties, Physiological Roles and Therapeutics. Curr. Top. Membr. 2012, 70, 169–214. [Google Scholar] [CrossRef]
- Pigeon, C.; Ilyin, G.; Courselaud, B.; Leroyer, P.; Turlin, B.; Brissot, P.; Loréal, O. A New Mouse Liver-Specific Gene, Encoding a Protein Homologous to Human Antimicrobial Peptide Hepcidin, Is Overexpressed during Iron Overload. J. Biol. Chem. 2001, 276, 7811–7819. [Google Scholar] [CrossRef] [Green Version]
- Nicolas, G.; Bennoun, M.; Devaux, I.; Beaumont, C.; Grandchamp, B.; Kahn, A.; Vaulont, S. Lack of Hepcidin Gene Expression and Severe Tissue Iron Overload in Upstream Stimulatory Factor 2 (USF2) Knockout Mice. Proc. Natl. Acad. Sci. USA 2001, 98, 8780–8785. [Google Scholar] [CrossRef] [Green Version]
- Delaby, C.; Pilard, N.; Gonçalves, A.S.; Beaumont, C.; Canonne-Hergaux, F. Presence of the Iron Exporter Ferroportin at the Plasma Membrane of Macrophages Is Enhanced by Iron Loading and Down-Regulated by Hepcidin. Blood 2005, 106, 3979–3984. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Tuttle, M.S.; Powelson, J.; Vaughn, M.B.; Donovan, A.; Ward, D.M.; Ganz, T.; Kaplan, J. Hepcidin Regulates Cellular Iron Efflux by Binding to Ferroportin and Inducing Its Internalization. Science 2004, 306, 2090–2093. [Google Scholar] [CrossRef] [Green Version]
- Brasse-Lagnel, C.; Karim, Z.; Letteron, P.; Bekri, S.; Bado, A.; Beaumont, C. Intestinal DMT1 Cotransporter Is Down-Regulated by Hepcidin via Proteasome Internalization and Degradation. Gastroenterology 2011, 140, 1261–1271e1. [Google Scholar] [CrossRef]
- Mena, N.P.; Esparza, A.; Tapia, V.; Valdés, P.; Núñez, M.T. Hepcidin Inhibits Apical Iron Uptake in Intestinal Cells. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 294, G192–G198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemeth, E.; Rivera, S.; Gabayan, V.; Keller, C.; Taudorf, S.; Pedersen, B.K.; Ganz, T. IL-6 Mediates Hypoferremia of Inflammation by Inducing the Synthesis of the Iron Regulatory Hormone Hepcidin. J. Clin. Investig. 2004, 113, 1271–1276. [Google Scholar] [CrossRef] [Green Version]
- Weiss, G.; Goodnough, L.T. Anemia of Chronic Disease. N. Engl. J. Med. 2005, 352, 1011–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. Lond. Engl. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinhold, R.B. Late Results of Gastric Bypass Surgery for Morbid Obesity. J. Am. Coll. Nutr. 1994, 13, 326–331. [Google Scholar] [CrossRef]
- Deacon, A.C.; Elder, G.H. ACP Best Practice No 165: Front Line Tests for the Investigation of Suspected Porphyria. J. Clin. Pathol. 2001, 54, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefebvre, T.; Dessendier, N.; Houamel, D.; Ialy-Radio, N.; Kannengiesser, C.; Manceau, H.; Beaumont, C.; Nicolas, G.; Gouya, L.; Puy, H.; et al. LC-MS/MS Method for Hepcidin-25 Measurement in Human and Mouse Serum: Clinical and Research Implications in Iron Disorders. Clin. Chem. Lab. Med. CCLM FESCC 2015, 53, 1557–1567. [Google Scholar] [CrossRef]
- Love, A.L.; Billett, H.H. Obesity, Bariatric Surgery, and Iron Deficiency: True, True, True and Related. Am. J. Hematol. 2008, 83, 403–409. [Google Scholar] [CrossRef]
- von Drygalski, A.; Andris, D.A. Anemia after Bariatric Surgery: More than Just Iron Deficiency. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2009, 24, 217–226. [Google Scholar] [CrossRef]
- Anty, R.; Dahman, M.; Iannelli, A.; Gual, P.; Staccini-Myx, A.; Amor, I.B.; Luciani, N.; Saint-Paul, M.-C.; Huet, P.-M.; Sadoul, J.-L.; et al. Bariatric Surgery Can Correct Iron Depletion in Morbidly Obese Women: A Link with Chronic Inflammation. Obes. Surg. 2008, 18, 709–714. [Google Scholar] [CrossRef]
- Wu, W.; Song, Y.; He, C.; Liu, C.; Wu, R.; Fang, L.; Cong, Y.; Miao, Y.; Liu, Z. Divalent Metal-Ion Transporter 1 Is Decreased in Intestinal Epithelial Cells and Contributes to the Anemia in Inflammatory Bowel Disease. Sci. Rep. 2015, 5, 16344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Laftah, A.H.; Brookes, M.J.; Cooper, B.; Iqbal, T.; Tselepis, C. A Role for Tumour Necrosis Factor Alpha in Human Small Bowel Iron Transport. Biochem. J. 2005, 390, 437–446. [Google Scholar] [CrossRef] [Green Version]
- Laftah, A.H.; Sharma, N.; Brookes, M.J.; McKie, A.T.; Simpson, R.J.; Iqbal, T.H.; Tselepis, C. Tumour Necrosis Factor Alpha Causes Hypoferraemia and Reduced Intestinal Iron Absorption in Mice. Biochem. J. 2006, 397, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolas, G.; Chauvet, C.; Viatte, L.; Danan, J.L.; Bigard, X.; Devaux, I.; Beaumont, C.; Kahn, A.; Vaulont, S. The Gene Encoding the Iron Regulatory Peptide Hepcidin Is Regulated by Anemia, Hypoxia, and Inflammation. J. Clin. Investig. 2002, 110, 1037–1044. [Google Scholar] [CrossRef]
- Bode, J.G.; Albrecht, U.; Häussinger, D.; Heinrich, P.C.; Schaper, F. Hepatic Acute Phase Proteins—Regulation by IL-6- and IL-1-Type Cytokines Involving STAT3 and Its Crosstalk with NF-ΚB-Dependent Signaling. Eur. J. Cell Biol. 2012, 91, 496–505. [Google Scholar] [CrossRef]
- Zhang, D.-L.; Wu, J.; Shah, B.N.; Greutélaers, K.C.; Ghosh, M.C.; Ollivierre, H.; Su, X.-Z.; Thuma, P.E.; Bedu-Addo, G.; Mockenhaupt, F.P.; et al. Erythrocytic Ferroportin Reduces Intracellular Iron Accumulation, Hemolysis, and Malaria Risk. Science 2018, 359, 1520–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aschemeyer, S.; Qiao, B.; Stefanova, D.; Valore, E.V.; Sek, A.C.; Ruwe, T.A.; Vieth, K.R.; Jung, G.; Casu, C.; Rivella, S.; et al. Structure-Function Analysis of Ferroportin Defines the Binding Site and an Alternative Mechanism of Action of Hepcidin. Blood 2018, 131, 899–910. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 88 | N = 55 | N = 35 | |
|---|---|---|---|
| Age (year) | 37.08 (9.42) | 37.09 (9.02) | 39.17 (8.23) |
| Weight (kg) | 114.15 (16.42) | 112.78 (14.41) | 109.74 (11.89) |
| BMI (kg/m2) | 42.31 (5.08) | 42.08 (5.02) | 41.26 (4.36) |
| Duration of obesity (year) | 14.54 (8.79) | 14.85 (8.5) | 13.96 (7.71) |
| waist/hip ratio | 0.91 (0.11) | 0.91 (0.11) | 0.89 (0.08) |
| Before Surgery | After Surgery | p-Value | Reference Range | |
|---|---|---|---|---|
| Hemoglobin (g/dL) | 12.9 (1.1) | 12.6 (0.9) | 0.215 | 11.5–14.9 |
| Red blood cells (T/L) | 4.51 (0.35) | 4.37 (0.38) | 0.118 | 3.93-5.09 |
| Hematocrit (%) | 39.1 (3.0) | 38.5 (3.1) | 0.447 | 34.4–43.9 |
| MCV (fL) | 85.2 (4.9) | 86.6 (6.0) | <0.001 | 77.9–95.3 |
| Platelets (G/L) | 261.7 (44.7) | 247.6 (57.1) | 0.519 | 185–445 |
| Leucocytes (G/L) | 6.57 (1.76) | 5.64 (1.60) | <0.001 | 4.02–11.42 |
| Folate (μg/L) | 6.0 (4.6) | 8.7 (5.4) | 0.001 | 3–20 |
| Vitamin B12 (ng/L) | 426.6 (162.5) | 394.2 (171.7) (171.69) | 0.004 | 189–883 |
| ASAT (U/L) | 20.7 (6.4) | 18.9 (10.2) | 0.152 | 15–37 |
| ALAT (U/L) | 29.9 (10.5) | 25.5 (14.1) | 0.142 | 14–59 |
| Gamma GT (U/L) | 34.0 (14.1) | 34.2 (38.3) | 0.326 | 5–55 |
| ALP (U/100mL) | 75.0 (19.0) | 69.4 (22.4) | <0.001 | 50–136 |
| Total Bilirubin (µmol/L) | 6.7 (3.3) | 9.7 (4.8) | <0.001 | 0–17 |
| Ferritin (µg/L) | 68.7 (55.9) | 73.8 (68.6) | 0.619 | 8–252 |
| Transferrin (g/L) | 2.55 (0.37) | 2.47 (0.42) | 0.673 | 2.00–3.65 |
| Transferrin Iron Binding Capacity | 62.7 (9.7) | 61.8 (10.5) | 0.746 | 50–80 |
| Transferrin Saturation (%) | 23.5 (8.5) | 31.2 (11.7) | 0.001 | 20–40 |
| Soluble Transferrin Receptor (mg/L) | 1.42 (0.37) | 1.27 (0.35) | <0.001 | 0–1.76 |
| Ceruloplasmin (g/L) | 0.29 (0.05) | 0.28 (0.07) | 0.009 | 0.2–0.4 |
| Haptoglobin (g/L) | 1.18 (0.41) | 0.91 (0.34) | <0.001 | 0.56–2.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lefebvre, T.; Coupaye, M.; Esposito-Farèse, M.; Gault, N.; Talbi, N.; Quintin, C.; Schmitt, C.; Bekri, S.; Bado, A.; Puy, H.; et al. Hepcidin and Iron Deficiency in Women One Year after Sleeve Gastrectomy: A Prospective Cohort Study. Nutrients 2021, 13, 2516. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082516
Lefebvre T, Coupaye M, Esposito-Farèse M, Gault N, Talbi N, Quintin C, Schmitt C, Bekri S, Bado A, Puy H, et al. Hepcidin and Iron Deficiency in Women One Year after Sleeve Gastrectomy: A Prospective Cohort Study. Nutrients. 2021; 13(8):2516. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082516
Chicago/Turabian StyleLefebvre, Thibaud, Muriel Coupaye, Marina Esposito-Farèse, Nathalie Gault, Neila Talbi, Caroline Quintin, Caroline Schmitt, Soumeya Bekri, André Bado, Hervé Puy, and et al. 2021. "Hepcidin and Iron Deficiency in Women One Year after Sleeve Gastrectomy: A Prospective Cohort Study" Nutrients 13, no. 8: 2516. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082516