
Feasibility Study of a Newly Developed Technology-Mediated Lifestyle Intervention for Overweight and Obese Young Adults

 , ,
, ,  ,
,
Abstract
:1. Introduction
- (1)
- Design, test, and assess a new technology-based lifestyle intervention for overweight and obese students in two major universities in the UAE.
- (2)
- Evaluate the impact of a lifestyle program delivered via information technology on weight loss and body composition (such as percent body fat and lean mass), nutrition knowledge, physical activity, perceived social support, and self-efficacy of overweight and obese university students.
2. Materials and Methods
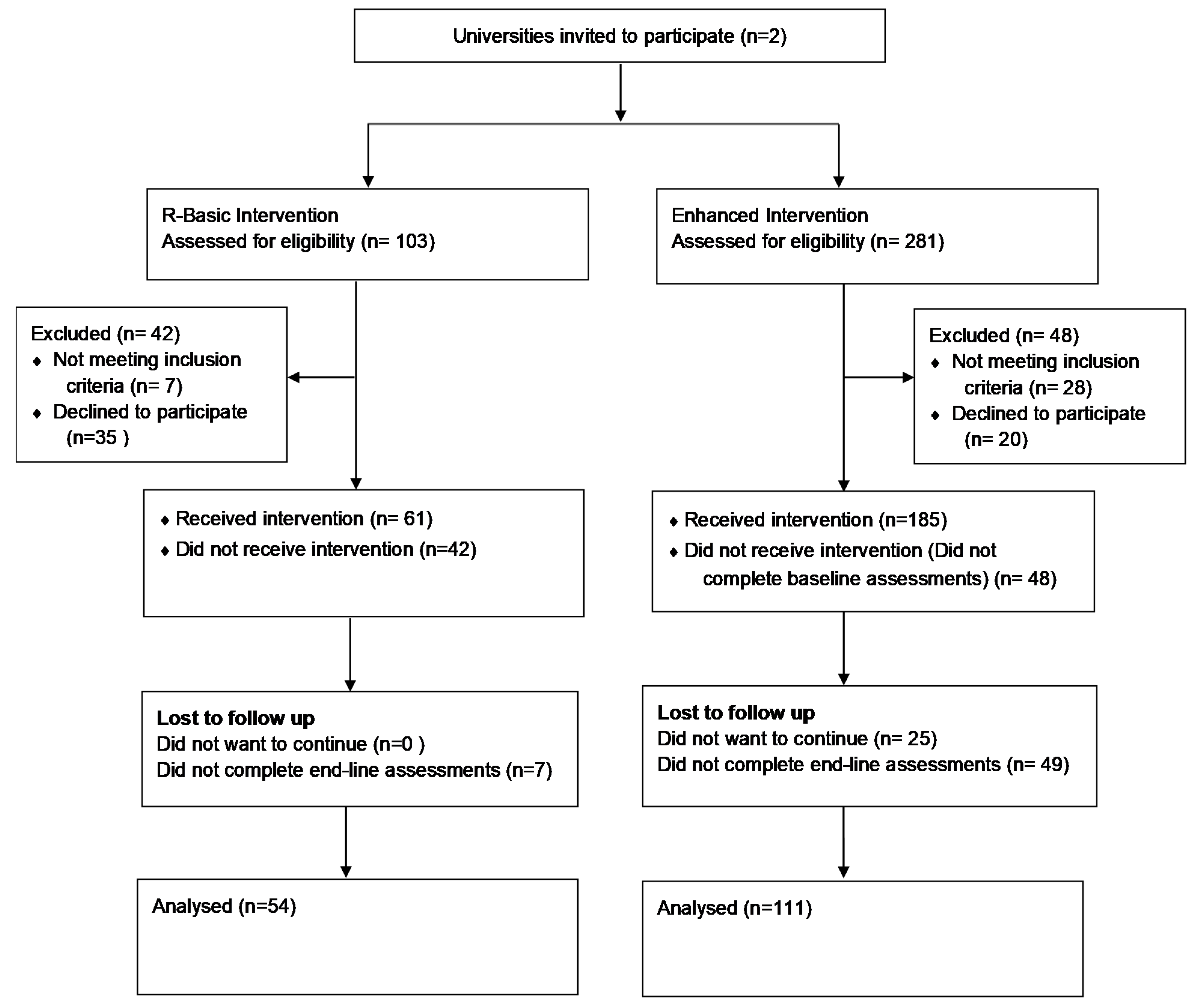
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Recruitment of Eligible Participants
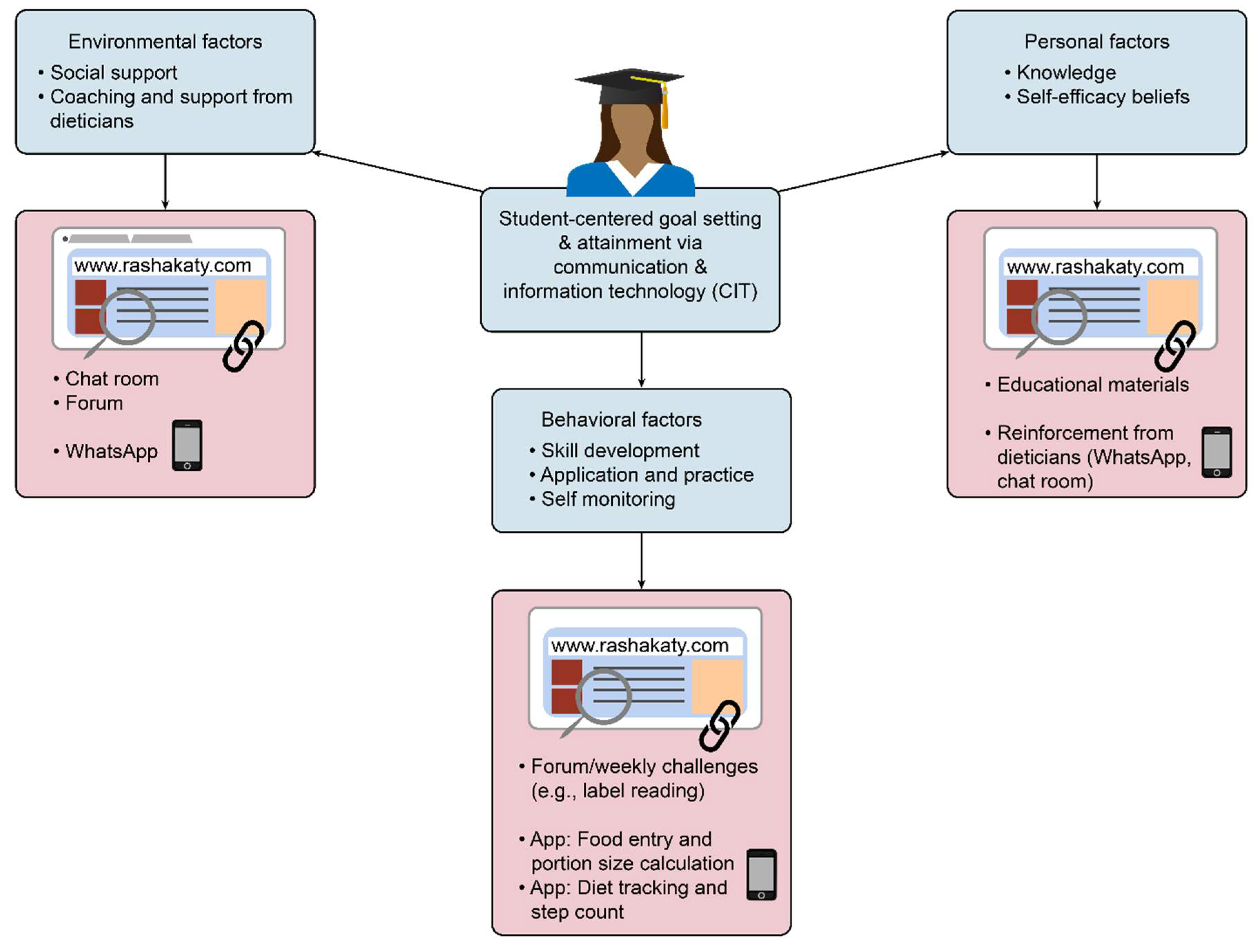
2.5. Theoretical Framework of the Intervention
2.6. Intervention Components
2.6.1. Website
2.6.2. Self-Monitoring Strategies: Mobile Applications
2.7. Measures
2.7.1. Anthropometric Measurements
2.7.2. Nutrition Knowledge
2.7.3. Physical Activity
2.7.4. Psychosocial Questionnaire
2.8. Participant Feedback
2.9. Statistical Analysis
3. Results
3.1. Anthropometric Data
3.2. Nutrition Knowledge
3.3. Physical Activity
3.4. Social Support and Self-Efficacy
3.5. Adapting the Program to the Need of the Participants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Rashakaty Website Tabs
References
- Ng, S.W.; Zaghloul, S.; Ali, H.I.; Harrison, G.; Popkin, B.M. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes. Rev. 2011, 12, 1–13. [Google Scholar] [CrossRef]
- Hajat, C.; Harrison, O.; Shather, Z. A profile and approach to chronic disease in Abu Dhabi. Glob. Health 2012, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Loney, T.; Aw, T.-C.; Handysides, D.G.; Ali, R.; Blair, I.; Grivna, M.; Shah, S.M.; Sheek-Hussein, M.; El-Sadig, M.; Sharif, A.A.; et al. An analysis of the health status of the United Arab Emirates: The ‘Big 4’ public health issues. Glob. Health Action 2013, 6, 20100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018. 2018. Available online: https://apps.who.int/iris/handle/10665/274512 (accessed on 24 June 2021).
- Lloyd-Jones, D.M.; Liu, K.; Colangelo, L.A.; Yan, L.L.; Klein, L.; Loria, C.M.; Lewis, C.E.; Savage, P. Consistently stable or decreased body mass index in young adulthood and longitudinal changes in metabolic syndrome components: The coronary artery risk development in young adults study. Circulation 2007, 115, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Al Sabbah, H. Prevalence of overweight/obesity, anaemia and their associations among female university students in Dubai, United Arab Emirates: A cross-sectional study. J. Nutr. Sci. 2020, 9, e26. [Google Scholar] [CrossRef]
- Ismail, L.C.; Hashim, M.; Jarrar, A.H.; Mohamad, M.N.; Saleh, S.T.; Jawish, N.; Bekdache, M.; Albaghli, H.; Kdsi, D.; Aldarweesh, D.; et al. Knowledge, Attitude, and Practice on Salt and Assessment of Dietary Salt and Fat Intake among University of Sharjah Students. Nutrients 2019, 11, 941. [Google Scholar] [CrossRef] [Green Version]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, A.; Hondros, G.; AScott, J.; Kapsokefalou, M. Eating habits of university students living at, or away from home in Greece. Appetite 2007, 49, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Racette, S.B.; Deusinger, S.S.; Strube, M.J.; Highstein, G.R.; Deusinger, R.H. Weight changes, exercise, and dietary patterns during freshman and sophomore years of college. J. Am. Coll. Health 2005, 53, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khawaja, A.H.; Qassim, S.; Hassan, N.A.; Arafa, E.A. Added sugar: Nutritional knowledge and consumption pattern of a principal driver of obesity and diabetes among undergraduates in UAE. Diabetes Metab. Syndr. 2019, 13, 2579–2584. [Google Scholar] [CrossRef] [PubMed]
- Worsley, A. Nutrition knowledge and food consumption: Can nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11 (Suppl. 3), S579–S585. [Google Scholar] [CrossRef] [Green Version]
- Al Dhaheri, A.S.; Al Ma’awali, A.K.; Laleye, L.C.; Washi, S.A. Nutritional knowledge of Emirati traditional foods and body image perceptions among UAE University students. Emir. J. Food Agric. 2014, 26, 853. [Google Scholar] [CrossRef] [Green Version]
- Attlee, A.; Abu-Qiyas, S.; Obaid, R.S. Assessment of Nutrition Knowledge of a University Community in Sharjah, United Arab Emirates. Malays. J. Nutr. 2014, 20, 327–337. [Google Scholar]
- Bandura, A. Social cognitive theory: An agentive perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.S.; Winett, R.A.; Wojcik, J.R. Self-regulation, self-efficacy, outcome expectations, and social support: Social cognitive theory and nutrition behavior. Ann. Behav. Med. 2007, 34, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, E.; Kulinna, P.H.; Cothran, D. Constructs of physical activity behaviour in children: The usefulness of Social Cognitive Theory. Psychol. Sport Exerc. 2012, 13, 303–310. [Google Scholar] [CrossRef]
- Dewar, D.L.; Lubans, D.R.; Morgan, P.J.; Plotnikoff, R.C. Development and evaluation of social cognitive measures related to adolescent physical activity. J. Phys. Act. Health 2013, 10, 544–555. [Google Scholar] [CrossRef]
- Cox, V.; Mann, L.; Blotnicky, K.; Rossiter, M. University Students’ Eating Behaviors: Implications for the Social Cognitive Theory. Int. J. Health Sci. 2017, 5, 25–37. [Google Scholar] [CrossRef]
- Clark, N.M.; Zimmerman, B.J. A social cognitive view of self-regulated learning about health. Health Educ. Behav. 2014, 41, 485–491. [Google Scholar] [CrossRef]
- Beleigoli, A.M.; Andrade, A.Q.; Cançado, A.G.; Paulo, M.N.; Diniz, M.F.H.; Ribeiro, A.L. Web-Based Digital Health Interventions for Weight Loss and Lifestyle Habit Changes in Overweight and Obese Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.M.; Poly, T.N.; Walther, B.A.; Jack Li, Y.C. Use of Mobile Phone App Interventions to Promote Weight Loss: Meta-Analysis. JMIR Mhealth Uhealth 2020, 8, e17039. [Google Scholar] [CrossRef] [PubMed]
- Patrick, K.; Raab, F.; Adams, M.A.; Dillon, L.; Zabinski, M.; Rock, C.L.; Griswold, W.G.; Norman, G.J. A text message-based intervention for weight loss: Randomized controlled trial. J. Med. Internet Res. 2009, 11, e1. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Spahn, J.M.; Reeves, R.S.; Keim, K.S.; Laquatra, I.; Kellogg, M.; Jortberg, B.; Clark, N.A. State of the evidence regarding behavior change theories and strategies in nutrition counseling to facilitate health and food behavior change. J. Am. Diet. Assoc. 2010, 110, 879–891. [Google Scholar] [CrossRef]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef] [Green Version]
- Booth, M. Assessment of physical activity: An international perspective. Res. Q. Exerc. Sport 2000, 71 (Suppl. 2), S114–S120. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Zaghloul, S.; Ali, H.; Harrison, G.; Yeatts, K.; El-Sadig, M.; Popkin, B.M. Nutrition transition in the United Arab Emirates. Eur. J. Clin. Nutr. 2011, 65, 1328–1337. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M. Health-enhancing physical activity among saudi adults using the International Physical Activity Questionnaire (IPAQ). Public Health Nutr. 2007, 10, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Latif, S.; Rana, R.; Qadir, J.; Ali, A.; Imran, M.A.; Younis, M.S. Mobile health in the developing world: Review of literature and lessons from a case study. IEEE Access 2017, 5, 11540–11556. [Google Scholar] [CrossRef]
- Aljuraiban, G.S. Use of Weight-Management Mobile Phone Apps in Saudi Arabia: A Web-Based Survey. JMIR Mhealth Uhealth 2019, 7, e12692. [Google Scholar] [CrossRef]
- Collins, C.E.; Morgan, P.J.; Jones, P.; Fletcher, K.; Martin, J.; Aguiar, E.J.; Lucas, A.; Neve, M.J.; Callister, R.; Patolia, S. A 12-week commercial web-based weight-loss program for overweight and obese adults: Randomized controlled trial comparing basic versus enhanced features. J. Med. Internet Res. 2012, 14, e57. [Google Scholar] [CrossRef]
- Collins, C.E.; Morgan, P.J.; Hutchesson, M.J.; Callister, R. Efficacy of standard versus enhanced features in a Web-based commercial weight-loss program for obese adults, part 2: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neve, M.; Morgan, P.J.; Jones, P.R.; Collins, C.E. Effectiveness of web-based interventions in achieving weight loss and weight loss maintenance in overweight and obese adults: A systematic review with meta-analysis. Obes. Rev. 2010, 11, 306–321. [Google Scholar] [CrossRef] [PubMed]
- Osei-Assibey, G.; Kyrou, I.; Adi, Y.; Kumar, S.; Matyka, K. Dietary and lifestyle interventions for weight management in adults from minority ethnic/non-White groups: A systematic review. Obes. Rev. 2010, 11, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Wieland, L.S.; Falzon, L.; Sciamanna, C.N.; Trudeau, K.J.; Folse, S.B.; Schwartz, J.; Davidson, K.W. Interactive computer-based interventions for weight loss or weight maintenance in overweight or obese people. Cochrane Database Syst. Rev. 2012, 8, CD007675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, D.M.; Savarimuthu, S.; Squires, A.; Nicholson, J.; Jay, M. Technology-assisted weight loss interventions in primary care: A systematic review. J. Gen. Intern. Med. 2014, 30, 107–117. [Google Scholar] [CrossRef] [Green Version]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Stewart, D.W.; Gabriele, J.M.; Fisher, E.B. Directive support, nondirective support, and health behaviors in a community sample. J. Behav. Med. 2012, 35, 492–499. [Google Scholar] [CrossRef]
- Alnasser, A.A.; Alkhalifa, A.S.; Sathiaseelan, A.; Marais, D. What overweight women want from a weight loss app: A qualitative study on arabic women. JMIR Mhealth Uhealth 2015, 3, e41. [Google Scholar] [CrossRef]
- Kim, H.N.; Seo, K. Smartphone-Based Health Program for Improving Physical Activity and Tackling Obesity for Young Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 17, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MOHAP. UAE National Health Survey Report 2017–2018. 2018. Available online: https://www.mohap.gov.ae/Files/MOH_OpenData/1556/UAE_NHS_2018.pdf (accessed on 15 March 2021).
- Bataineh, M.F.; Attlee, A. Reliability and validity of Arabic version of revised general nutrition knowledge questionnaire on university students. Public Health Nutr. 2021, 24, 851–860. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Group | Baseline * | Endline * | Change ‡ |
|---|---|---|---|---|
| Waist circumference (cm) | R-Basic | 84.75 a (80.75–91.25) | 86.00 a (81.17–89.67) | −0.67 a (−3.08–3.67) |
| R-Enhanced | 91.00 a (82.00–98.00) | 87.50 b (78.38–94.00) | −2.00 b (−6.00–0.00) | |
| Weight (kg) | R-Basic | 75.65 a (71.60–82.5) | 76.93 a (72.30–82.68) | −0.37 a (−3.49–2.42) |
| R-Enhanced | 74.50 a (67.60–85.6) | 72.80 b (67.00–85.6) | −0.20 a (−1.50–0.90) | |
| BMI (kg/m2) | R-Basic | 28.65 a (26.78–32.47) | 29.36 a (27.76–31.64) | −0.14 a (−1.308–0.97) |
| R-Enhanced | 29.37 a (26.86–35.02) | 29.43 b (26.57–35.11) | −0.08 a (−0.63–0.37) | |
| Fat-free mass (kg) | R-Basic | 47.95 a (46.30–50.15) | 47.77 a (46.20–50.34) | −0.17 a (−1.27–0.78) |
| R-Enhanced | 47.10 a (44.50–49.20) | 47.10 b (44.20–50.00) | 0.20 a (−0.60–1.00) | |
| Body fat percent (%) | R-Basic | 36.10 a (33.90–40.13) | 36.58 a (34.61–39.45) | −0.07 a (−1.80–1.59) |
| R-Enhanced | 36.50 a (33.30–42.30) | 36.40 b (32.50–40.60) | −0.70 a (−1.70–0.60) | |
| Body fat (kg) | R-Basic | 27.00 a (23.03–32.48) | 27.83 a (25.21–32.18) | −0.13 a (−2.77–1.77) |
| R-Enhanced | 27.00 a (22.80–36.50) | 26.40 b (21.80–34.80) | −0.60 a (−1.90–0.50) |
| Nutrition Knowledge Category † | Group | Baseline * | Endline * | Change ‡ |
|---|---|---|---|---|
| Dietary recommendations | R-Basic | 7 a (4.75–8) | 10 b (7–11) | 3 a (1–4) |
| R-Enhanced | 7 a (6–8) | 10 b (9–11) | 3 a (2–4) | |
| Sources of nutrients | R-Basic | 24 a (17–27.25) | 23 a (20–28) | 1 a (−2.25–5.25) |
| R-Enhanced | 20 a (16–23) | 26.5 b (24–29) | 6 b (4.25–10) | |
| Choosing everyday foods | R-Basic | 3 a (2–3) | 3 b (2–4) | 0 a (0–1) |
| R-Enhanced | 2 a (1–3) | 3 b (2–3.75) | 0 b (0–1) | |
| Diet–disease relationships | R-Basic | 5 a (4–5) | 5 a (4–5) | 0 a (0–0) |
| R-Enhanced | 4 a (3–5) | 5 b (4–5) | 0 b (0–1) |
| Variable | Group | Baseline * | Endline * | Change ‡ |
|---|---|---|---|---|
| Days of vigorous physical activity | R-Basic | 0 a (0–2) | 0 a (0–2) | 0 a (−2–0) |
| R-Enhanced | 1 a (0–2) | 1 a (1–2) | 1 b (−1–1) | |
| Minutes of vigorous physical activity | R-Basic | 0 a (0–30) | 0 b (0 -28.75) | 0 a (0-5) |
| R-Enhanced | 10 a (0–42.5) | 30 b (10–40) | 5 b (0–26.25) | |
| Days of moderate physical activity | R-Basic | 0 a (0–2) | 0 a (0–3) | 0 a (−1–0.75) |
| R-Enhanced | 1 a (0–3) | 3 b (0–4) | 1 b (0–2) | |
| Minutes of moderate physical activity | R-Basic | 0 a (0–20) | 0 a (0–20) | 0 a (0–22.5) |
| R-Enhanced | 15 a (0–30) | 15 b (0–45) | 10 a (0–28.75) | |
| Days of walking | R-Basic | 4 a (2.5–6) | 5 a (3.25–7) | 1 a (0–2.75) |
| R-Enhanced | 7 a (4–7) | 6 a (4–7) | 0 a (−1–1) | |
| Minutes of walking | R-Basic | 30 a (20–40) | 20 a (11.5–48.75) | −5 a (−20–8) |
| R-Enhanced | 25 a (15–36.25) | 40 b (20–60) | 15 b (0–35) | |
| Sitting time (hours) | R-Basic | 5 a (3–7) | 8.5 a (4–14.25) | 0 a (0–1) |
| R-Enhanced | 6 a (5–10) | 5 b (3–7) | 0 a (0–0.25) |
| Variable † | Group | Baseline * | Endline * | Change ‡ |
|---|---|---|---|---|
| Perceived support from family to reduce fat intake | R-Basic | 3.22 a (2.78–3.58) | 3.44 a (3.00–3.78) | 0.17 a (−0.19–0.56) |
| R-Enhanced | 3.11 a (2.67–3.44) | 3.44 b (3.11–3.89) | 0.33 a (0.00–0.78) | |
| Perceived support from friends to reduce fat intake | R-Basic | 3.11 a (2.64–3.33) | 3.22 b (2.78–3.56) | 0.22 a (−0.08–0.44) |
| R-Enhanced | 2.78 a (2.44–3.11) | 3.22 b (2.89–3.75) | 0.44 b (0–0.78) | |
| Perceived support from family to increase fruit and vegetable intake | R-Basic | 3.23 a (2.86–3.57) | 3.57 a (2.89–3.71) | 0.29 a (−0.29–0.57) |
| R-Enhanced | 3.00 a (2.71–3.43) | 3.43 b (3–3.86) | 0.29 a (0.00–0.71) | |
| Perceived support from friends to increase fruit and vegetable intake | R-Basic | 3.00 a (2.71–3.30) | 3.14 b (2.75–3.57) | 0.29 a (0.00–0.68) |
| R-Enhanced | 2.71 a (2.29–3.14) | 3.29 b (2.86–3.68) | 0.43 a (0.14–0.86) | |
| Perceived support from family to increase physical activity | R-Basic | 2.86 a (2.57–3.14) | 2.86 a (2.57–3.14) | 0.00 a (−0.29–0.29) |
| R-Enhanced | 2.57 a (2.14–3.00) | 3.14 b (2.86–3.86) | 0.57 b (0.00–1.29) | |
| Perceived support from friends to increase physical activity | R-Basic | 2.86 a (2.57–3.04) | 3.00 a (2.57–3.25) | 0.00 a (−0.25–0.43) |
| R-Enhanced | 2.71 a (2.29–3.00) | 3.14 b (2.86–3.71) | 0.43 b (0.00–1.14) |
| Variable † | Group | Baseline * | Endline * | Change ‡ |
|---|---|---|---|---|
| Perceived self-efficacy to reduce fat | R-Basic | 75.00 a (66.07–86.61) | 71.43 a (50.89–85.71) | −3.57 a (−16.96–9.82) |
| R-Enhanced | 71.43 a (57.14–82.14) | 67.86 a (55.36–78.57) | 0.00 a (−10.71–14.29) | |
| Perceived self-efficacy to reduce sugar | R-Basic | 58.33 a (41.67–75.00) | 66.67 a (50–83.33) | 0.00 a (−16.67–16.67) |
| R-Enhanced | 58.33 a (50.00–75.00) | 66.67 b (50.00–75.00) | 8.30 a (−8.33–20.83) | |
| Perceived self-efficacy to increase fruits, vegetables and fiber | R-Basic | 60.92 ± 21.46 a | 63.29 ± 22.43 a | 2.37 ± 22.77 a |
| R-Enhanced | 59.10 ± 20.20 a | 63.41 ± 19.09 a | 4.31 ± 23.44 a | |
| Perceived self-efficacy to overcome barriers to physical activity | R-Basic | 40.91 a (27.27–50) | 45.45 a (27.27–59.09) | 0.00 a (−13.64–17.05) |
| R-Enhanced | 40.91 a (31.82–59.09) | 50.00 b (36.36–63.64) | 4.55 a (−9.09–20.45) | |
| Perceived self-efficacy to integrate physical activity into daily routine | R-Basic | 57.69 a (50–69.23) | 57.69 a (47.12–82.69) | 0.00 a (−11.54–15.38) |
| R-Enhanced | 69.23 a (53.85–80.77) | 69.23 a (50.96–84.62) | 0.00 a (−11.54–11.54) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, H.I.; Attlee, A.; Alhebshi, S.; Elmi, F.; Al Dhaheri, A.S.; Stojanovska, L.; El Mesmoudi, N.; Platat, C. Feasibility Study of a Newly Developed Technology-Mediated Lifestyle Intervention for Overweight and Obese Young Adults. Nutrients 2021, 13, 2547. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082547
Ali HI, Attlee A, Alhebshi S, Elmi F, Al Dhaheri AS, Stojanovska L, El Mesmoudi N, Platat C. Feasibility Study of a Newly Developed Technology-Mediated Lifestyle Intervention for Overweight and Obese Young Adults. Nutrients. 2021; 13(8):2547. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082547
Chicago/Turabian StyleAli, Habiba I., Amita Attlee, Salma Alhebshi, Fadima Elmi, Ayesha S. Al Dhaheri, Lily Stojanovska, Najoua El Mesmoudi, and Carine Platat. 2021. "Feasibility Study of a Newly Developed Technology-Mediated Lifestyle Intervention for Overweight and Obese Young Adults" Nutrients 13, no. 8: 2547. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082547