
24-h Potassium Excretion Is Associated with Components of the Metabolic Syndrome: Results from a National Survey Based on Urine Collection in Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Sampling
Assessment of Eligibility
2.2. Study Flow and Protocol
2.3. Data Collection and Definition–Main Exposure Variables
2.3.1. Potassium and Sodium Assessments
2.3.2. A Standardized Questionnaire for Assessment of Other Explanatory Variables
2.3.3. Drug Therapy
2.4. Data Collection: Main Outcome—Metabolic Syndrome and Its Components
2.5. Data Handling and Analysis
3. Results
3.1. Subjects’ General and Lifestyle Characteristics and Electrolytes Levels
3.2. Subjects’ Health and Metabolic Characteristics
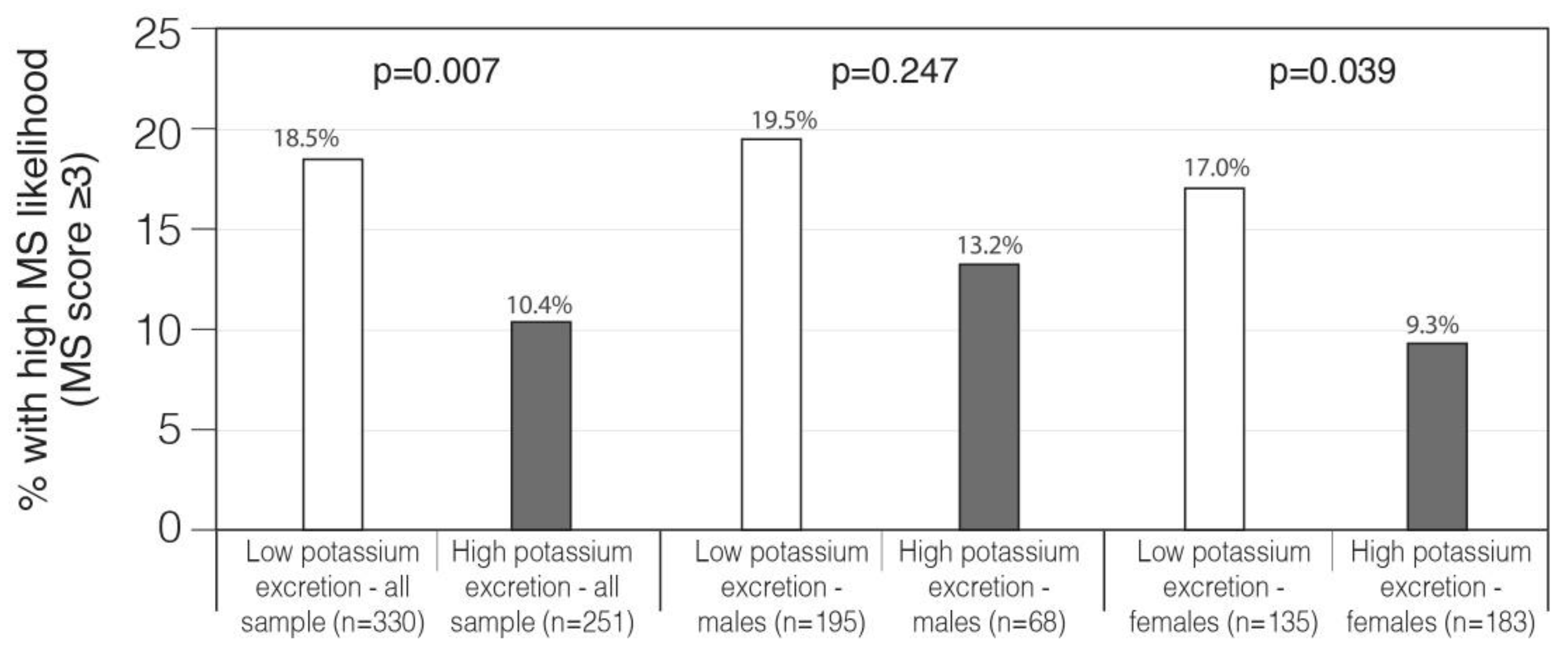
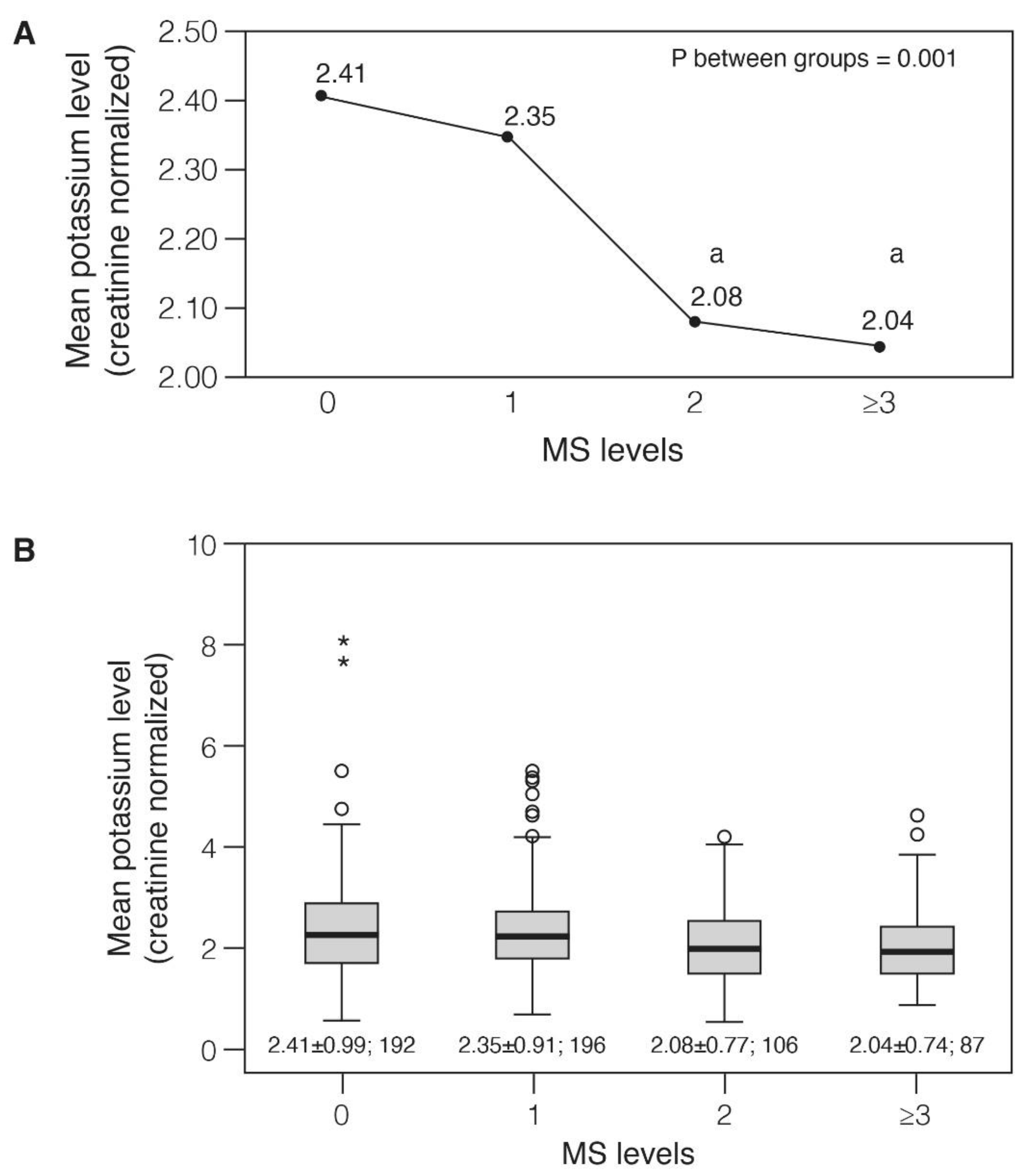
3.3. Associations of Potassium Excretion with the Metabolic Syndrome Components
3.4. The Relation of Potassium and Sodium Excretion and Intake with Other Metabolic Syndrome Variables
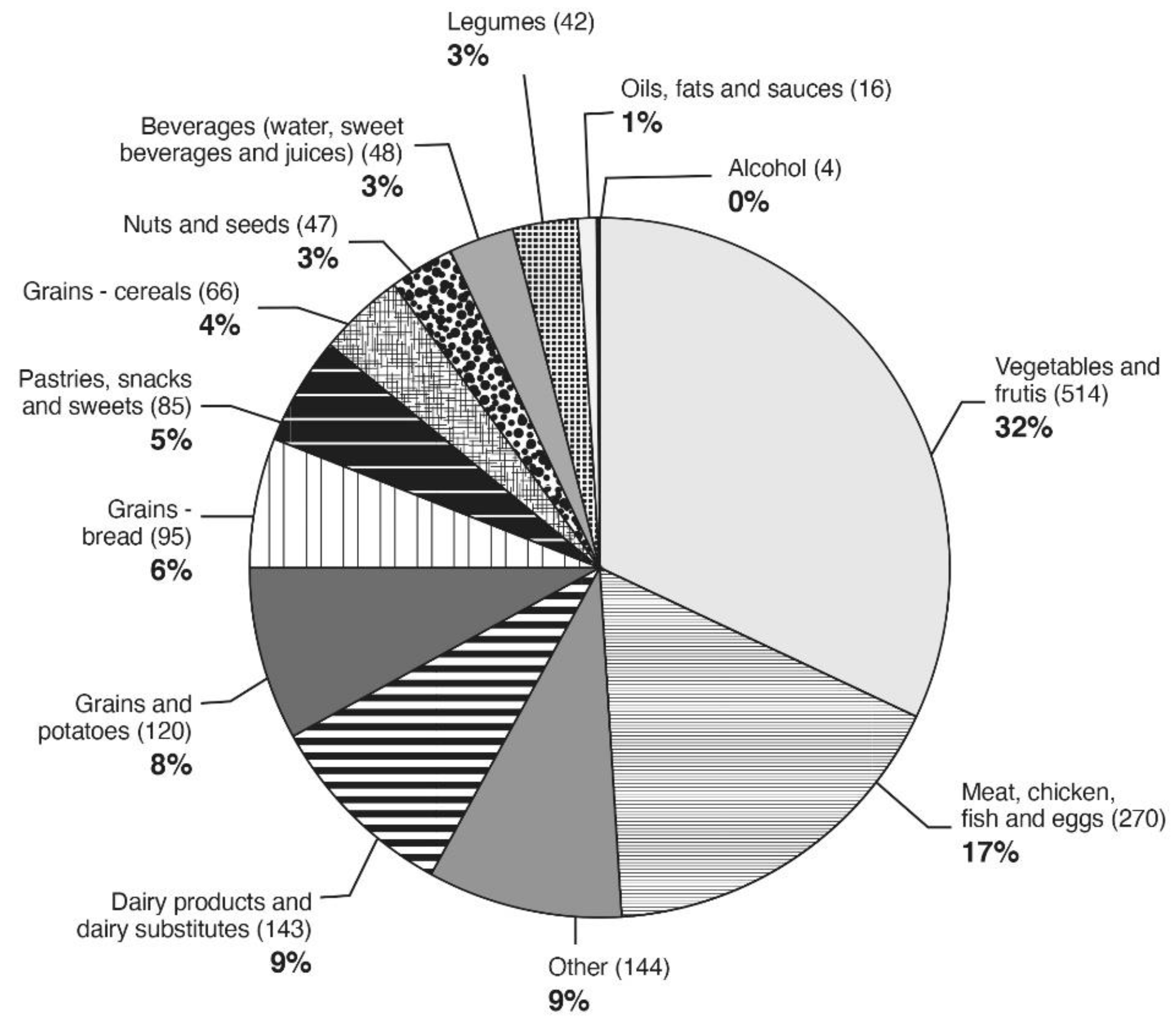
3.5. The Contribution of Food Groups to the Potassium Intake as Reported in 24-h Recalls
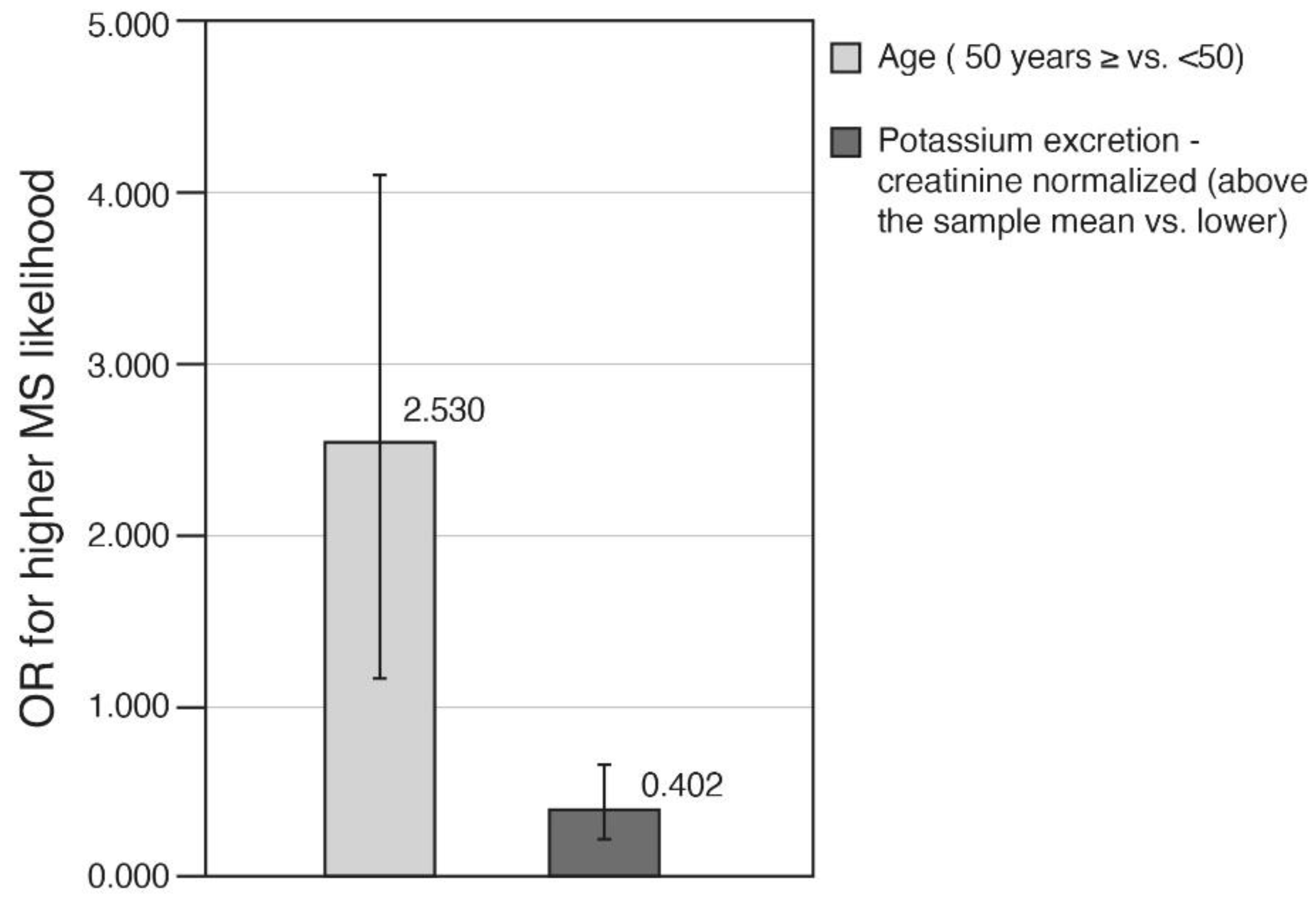
3.6. Multivariate Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmet, P.; Magliano, D.; Matsuzawa, Y.; Alberti, G.; Shaw, J. The Metabolic Syndrome: A Global Public Health Problem and A New Definition. J. Atheroscler. Thromb. 2005, 12, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnethon, M.R.; Loria, C.M.; Hill, J.O.; Sidney, S.; Savage, P.J.; Liu, K. Risk Factors for the Metabolic Syndrome: The Coronary Artery Risk Development in Young Adults (CARDIA) Study, 1985–2001. Diabetes Care 2004, 27, 2707–2715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Després, J.-P.; Lemieux, I.; Bergeron, J.; Pibarot, P.; Mathieu, P.; LaRose, E.; Rodés-Cabau, J.; Bertrand, O.F.; Poirier, P. Abdominal Obesity and the Metabolic Syndrome: Contribution to Global Cardiometabolic Risk. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Pitsavos, C.; Panagiotakos, D.; Weinem, M.; Stefanadis, C. Diet, Exercise and the Metabolic Syndrome. Rev. Diabet. Stud. 2006, 3, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Whelton, P.K.; Appel, L.J.; Sacco, R.L.; Anderson, C.A.; Antman, E.M.; Campbell, N.; Dunbar, S.B.; Frohlich, E.D.; Hall, J.E.; Jessup, M.; et al. Sodium, Blood Pressure, and Cardiovascular Disease. Circulation 2012, 126, 2880–2889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of Lower Sodium Intake on Health: Systematic Review and Meta-Analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [Green Version]
- Kotchen, T.A.; Cowley, A.W.; Frohlich, E.D. Salt in Health and Disease—A Delicate Balance. N. Engl. J. Med. 2013, 368, 1229–1237. [Google Scholar] [CrossRef]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of Increased Potassium Intake on Cardiovascular Risk Factors and Disease: Systematic Review and Meta-Analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [Green Version]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. Available online: https://www.nejm.org/doi/10.1056/NEJM199704173361601?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dwww.ncbi.nlm.nih.gov (accessed on 9 March 2020).
- Cogswell, M.E.; Zhang, Z.; Carriquiry, A.L.; Gunn, J.P.; Kuklina, E.V.; Saydah, S.H.; Yang, Q.; Moshfegh, A.J. Sodium and Potassium Intakes among US Adults: NHANES 2003–2008. Am. J. Clin. Nutr. 2012, 96, 647–657. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; The National Academies Press: Washington, DC, USA, 2005. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 7th ed.; U.S. Government Printing Office: Washington, DC, USA, 2010.
- Food Surveys Research Group: USDA ARS. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/ (accessed on 3 January 2019).
- Rumawas, M.E.; Dwyer, J.T.; Mckeown, N.M.; Meigs, J.B.; Rogers, G.; Jacques, P.F. The Development of the Mediterranean-Style Dietary Pattern Score and Its Application to the American Diet in the Framingham Offspring Cohort. J. Nutr. 2009, 139, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Nowson, C.A.; Worsley, A.; Margerison, C.; Jorna, M.K.; Godfrey, S.J.; Booth, A. Blood Pressure Change with Weight Loss Is Affected by Diet Type in Men. Am. J. Clin. Nutr. 2005, 81, 983–989. [Google Scholar] [CrossRef] [Green Version]
- Blumenthal, J.A.; Babyak, M.A.; Hinderliter, A.; Watkins, L.L.; Craighead, L.; Lin, P.-H.; Caccia, C.; Johnson, J.; Waugh, R.; Sherwood, A. Effects of the DASH Diet Alone and in Combination With Exercise and Weight Loss on Blood Pressure and Cardiovascular Biomarkers in Men and Women With High Blood Pressure: The ENCORE Study. Arch. Intern. Med. 2010, 170, 126–135. [Google Scholar] [CrossRef]
- Whelton, P.K.; He, J.; Cutler, J.A.; Brancati, F.L.; Appel, L.J.; Follmann, D.; Klag, M.J. Effects of Oral Potassium on Blood Pressure: Meta-Analysis of Randomized Controlled Clinical Trials. JAMA 1997, 277, 1624–1632. [Google Scholar] [CrossRef]
- He, J.; Gu, D.; Kelly, T.N.; Hixson, J.E.; Rao, D.C.; Jaquish, C.E.; Chen, J.; Zhao, Q.; Gu, C.; Huang, J.; et al. Genetic Variants in the Renin–Angiotensin–Aldosterone System and Blood Pressure Responses to Potassium Intake. J. Hypertens. 2011, 29, 1719–1730. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Li, X.; Fan, W.; Yu, W.; Wang, S.; Li, Z.; Scott, E.M.; Li, X. Potassium and Obesity/Metabolic Syndrome: A Systematic Review and Meta-Analysis of the Epidemiological Evidence. Nutrients 2016, 8, 183. [Google Scholar] [CrossRef] [Green Version]
- St-Jules, D.; Goldfarb, D.; Sevick, M. Nutrient Non-Equivalence: Does Restricting High-Potassium Plant Foods Help to Prevent Hyperkalemia in Hemodialysis Patients? J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2016, 26, 282–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protocol for Population Level Sodium Determination in 24-Hour Urine Samples. Prepared by WHO/PAHO Regional Expert Group for Cardiovascular Disease Prevention through Population—Wide Dietary Salt Reduction 2010. Available online: https://www.paho.org/hq/dmdocuments/2013/24h-urine-Protocol-eng.pdf (accessed on 7 September 2019).
- McLean, R.M. Measuring Population Sodium Intake: A Review of Methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef]
- Tal, B.; Sack, J.; Yaron, M.; Shefer, G.; Buch, A.; Ben Haim, L.; Marcus, Y.; Shenkerman, G.; Sofer, Y.; Shefer, L.; et al. Increment in Dietary Potassium Predicts Weight Loss in the Treatment of the Metabolic Syndrome. Nutrients 2019, 11, 1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espeland, M.A.; Kumanyika, S.; Wilson, A.C.; Reboussin, D.M.; Easter, L.; Self, M.; Robertson, J.; Brown, W.M.; McFarlane, M. Statistical Issues in Analyzing 24-Hour Dietary Recall and 24-Hour Urine Collection Data for Sodium and Potassium Intakes. Am. J. Epidemiol. 2001, 153, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Commins, J.M.; Moler, J.E.; Willett, W.; Tinker, L.F.; Subar, A.F.; Spiegelman, D.; Rhodes, D.; Potischman, N.; Neuhouser, M.L.; et al. Pooled Results From 5 Validation Studies of Dietary Self-Report Instruments Using Recovery Biomarkers for Potassium and Sodium Intake. Am. J. Epidemiol. 2015, 181, 473–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Sodium Survey 2014–2016; Nutrition Division, Health Promotion Department and Public Health Services, Ministry of Health: Jerusalem, Israel; Institute of Endocrinology, Metabolism and Hypertension, Tel Aviv Sourasky Medical Center: Tel Aviv, Israel, 2017.
- Israel Center for Disease Control (ICDC). Rav Mabat—Second National Health and Nutrition Survey of Israeli Adults 2015–2016; Ministry of Health February Israel: Jerusalem, Israel, 2019; Volume 383.
- Whelton Paul, K.; Carey Robert, M.; Aronow Wilbert, S.; Casey Donald, E.; Collins Karen, J.; Cheryl, D.H.; DePalma Sondra, M.; Samuel, G.; Jamerson Kenneth, A.; Jones Daniel, W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e484–e594. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Klein, S.; Allison, D.B.; Heymsfield, S.B.; Kelley, D.E.; Leibel, R.L.; Nonas, C.; Kahn, R. Waist Circumference and Cardiometabolic Risk: A Consensus Statement from Shaping America’s Health: Association for Weight Management and Obesity Prevention; NAASO, The Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Diabetes Care 2007, 30, 1647–1652. [Google Scholar] [CrossRef] [Green Version]
- Musso, G.; Gambino, R.; Bo, S.; Uberti, B.; Biroli, G.; Pagano, G.; Cassader, M. Should Nonalcoholic Fatty Liver Disease Be Included in the Definition of Metabolic Syndrome?: A Cross-Sectional Comparison with Adult Treatment Panel III Criteria in Nonobese Nondiabetic Subjects. Diabetes Care 2008, 31, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Israel Ministry of Health. Tzameret 4—Dietary Analysis Software. In Nutrition Division; Israel Ministry of Health: Nitzan Horowitz, Israel, 2016. [Google Scholar]
- Dormann, C.F.; Elith, J.; Bacher, S.; Buchmann, C.; Carl, G.; Carré, G.; Marquéz, J.R.G.; Gruber, B.; Lafourcade, B.; Leitão, P.J.; et al. Collinearity: A Review of Methods to Deal with It and a Simulation Study Evaluating Their Performance. Ecography 2013, 36, 27–46. [Google Scholar] [CrossRef]
- Ge, Z.; Zhang, J.; Chen, X.; Guo, X.; Yan, L.; Tang, J.; Cai, X.; Xu, J.; Hou, L.; Ma, J. Association between 24 h urinary sodium to potassium ratio and metabolic syndrome in Chinese adults. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2015, 36, 790–793. [Google Scholar]
- Ge, Z.; Guo, X.; Chen, X.; Tang, J.; Yan, L.; Ren, J.; Zhang, J.; Lu, Z.; Dong, J.; Xu, J.; et al. Association between 24 h Urinary Sodium and Potassium Excretion and the Metabolic Syndrome in Chinese Adults: The Shandong and Ministry of Health Action on Salt and Hypertension (SMASH) Study. Br. J. Nutr. 2015, 113, 996–1002. [Google Scholar] [CrossRef] [Green Version]
- Teramoto, T.; Kawamori, R.; Miyazaki, S.; Teramukai, S. Sodium Intake in Men and Potassium Intake in Women Determine the Prevalence of Metabolic Syndrome in Japanese Hypertensive Patients: OMEGA Study. Hypertens. Res. 2011, 34, 957–962. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet. Available online: https://www.nejm.org/doi/10.1056/NEJM200101043440101?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dwww.ncbi.nlm.nih.gov (accessed on 7 February 2020).
- Ferrannini, E.; Galvan, A.Q.; Santoro, D.; Natali, A. Potassium as a Link between Insulin and the Renin-Angiotensin-Aldosterone System. J. Hypertens. Suppl. Off. J. Int. Soc. Hypertens. 1992, 10, S5–S10. [Google Scholar] [CrossRef]
- Lee, H.; Lee, J.; Hwang, S.; Kim, S.; Chin, H.J.; Han, J.S.; Heo, N.J. Potassium Intake and the Prevalence of Metabolic Syndrome: The Korean National Health and Nutrition Examination Survey 2008–2010. PLoS ONE 2013, 8, e55106. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Joh, H.-K.; Kim, K.H.; Park, S.M. Benefits of Potassium Intake on Metabolic Syndrome: The Fourth Korean National Health and Nutrition Examination Survey (KNHANES IV). Atherosclerosis 2013, 230, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Guo, B.; Jin, D.; Wang, Y.; Jiang, Y.; Zhu, B.; Chen, Y.; Ma, L.; Zhou, H.; Xie, G. Association of Dietary Sodium:Potassium Ratio with the Metabolic Syndrome in Chinese Adults. Br. J. Nutr. 2018, 120, 612–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 581) | High Potassium Excretion (Creatinine Adjusted) 1 (n = 254) | Low Potassium Excretion (Creatinine Adjusted) 1 (n = 327) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Females (n = 318) | Males (n = 263) | All | Females (n = 185) | Males (n = 69) | All | Females (n = 133) | Males (n = 194) | |
| Age (years) | 46.27 ± 12.14 | 46.27 ± 11.61 | 46.36 ± 12.76 | 48.23 ± 11.74 ** | 47.23 ± 11.51 | 50.90 ± 12.01 ** | 44.82 ± 12.24 | 44.92 ± 11.65 | 44.74 ± 12.66 |
| Gender (% females) | 54.7 | --- | ---- | 72.8 ** | --- | ---- | 40.7 | ----- | ---- |
| Education (years) | 14.74 ± 3.15 | 14.88 ± 11.61 | 14.63 ± 3.08 | 14.95 ± 3.14 | 15.13 ± 3.31 | 14.68 ± 3.38 | 14.5 ± 2.91 | 14.53 ± 2.87 | 14.68 ± 3.38 |
| Marital status (% married/ living with a partner) 2 | 74.2 | 73.6 | 74.9 | 76.8 | 75.7 | 79.7 | 72.2 | 70.7 | 73.2 |
| Socioeconomic status 3 (% defined as high) | 28.1 | 18.3 | 39.5 | 26.2 | 17.4 | 49.1 | 29.5 | 19.6 | 36.2 |
| Socioeconomic status 3 (% defined as low) | 32.6 | 42.9 | 20.5 | 35.6 | 43.5 | 15.1 | 30.3 | 42.2 | 22.4 |
| Ethnicity/religion (% Jews and others [non-Arab Christians]) 4 | 94.7 | 97.2 | 91.6 | 97.6 ** | 97.8 | 97.1 | 92.4 | 96.2 | 89.7 |
| Smoking 5 (% current smokers) | 22.2 | 20.1 | 24.7 | 17.7 | 18.4 | 15.9 | 25.7 | 22.6 | 27.8 |
| Smoking 5 (% past smokers) | 17.4 | 14.5 | 20.9 | 18.5 | 16.8 | 23.2 | 16.5 | 11.3 | 20.1 |
| Any physical activity, at least 20 min, a week | 52.0 | 51.9 | 52.1 | 57.9 * | 58.9 ** | 55.1 | 47.4 | 42.1 | 51.0 |
| All activity, how often 6 (% performing at least three times a week) | 31.8 | 30.5 | 33.4 | 37 | 36.2 | 39 | 28 | 22.5 | 31.4 |
| % participating in intense physical activity in a week | 34.4 | 28.0 | 42.2 | 35.0 | 31.4 | 44.9 | 33.9 | 23.3 | 41.2 |
| Energy intake by 24 h recall (Kcals) (n = 567) | 1925.27 ± 764.35 | 1678.72 ± 599.77 | 2214.65 ± 840.96 | 1803.11 ± 682.81 ** | 1678.41 ± 580.44 | 1925.27 ± 764.35 | 2095.75 ± 836.71 | 1679.17 ± 628.73 | 2257.4778 ± 840.60 |
| Total Sample (n = 581) | High Potassium Excretion (Creatinine Adjusted) 1 (n= 254) | Low Potassium Excretion (Creatinine Adjusted) 1 (n= 327) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Females (n = 318) | Males (n = 263) | All | Females (n = 185) | Males (n = 69) | All | Females (n = 133) | Males (n = 194) | |
| 24 h urine volume (mL/day) | 1800.88 ± 840.82 | 1827.75 ± 872.66 | 1756.16 ± 769.86 | 2033.50 ± 849.03 | 2023.19 ± 850.93 ** | 2061.16 ± 849.50 ** | 1610.35 ± 762.32 | 1555.90 ± 831.57 | 1647.68 ± 710.79 |
| 24 h sodium excretion (creatinine adjusted) | 3.13 ± 1.38 (0.3–14.37) | 3.34 ± 1.27 (0.86–10.32) | 2.88 ± 1.46 (0.3–14.77) | 3.58 ± 1.65 ** | 3.61 ± 1.35 ** | 3.50 ± 2.29 ** | 2.78 ± 0.99 | 2.96 ± 1.04 | 2.66 ± 0.93 |
| Sodium/potassium excretion ratio | 1.50 ± 0.64 (0.13–4.96) | 1.41 ± 0.56 (0.36–3.58) | 1.62 ± 0.72 (0.13–4.96) | 1.20 ± 0.52 | 1.20 ± 0.44 ** | 3.50 ± 2.29 ** | 1.74 ± 0.63 | 1.70 ± 0.57 | 2.66 ± 0.93 |
| BMI (kg/m2) (n = 579) (range) | 26.78 ± 5.08 (13.77–52.4) | 26.55 ± 5.50 (13.77–52.40) | 27.17 ± 4.56 (16.82–49.35) | 26.01 ± 4.87 ** | 25.76 ± 5.17 ** | 26.65 ± 3.94 | 27.47 ± 5.18 | 27.63 ± 5.76 | 27.36 ± 4.76 |
| %with BMI ≥ 28.5 kg/m2 (n = 566) | 32.5 (189) | 32 (101) | 33 (88) | 24 (60) ** | 24 (45) ** | 22 (15) * | 39 (129) | 42 (56) | 37 (73) |
| % defined with elevated blood pressure according to MS criteria 2 | 52.3 | 42.4 (129) | 64.6 (157) | 46.9 * | 40.9 | 63.1% | 56.5 | 44.5 | 65.2% |
| Systolic blood pressure (mm/Hg) (range) | 125.02 ± 18.57 (86–198) | 120.50 ± 17.99 (86.00–180) | 130.47 ± 17.42 (98.50–198) | 122.24 ± 17.35 | 119.99 ± 17.06 | 128.36 ± 16.77 | 127.05 ± 18.95 | 121.21 ± 19.25 | 131.24 ± 17.64 |
| Diastolic blood pressure (mm/Hg) (range) | 80.96 ± 11.81 (48–136) | 78.15 ± 11.17 (48–136) | 84.46 ± 11.79 (58.00–133.00) | 79.09 ± 11.27 | 77.92 ± 11.14 | 82.25 ± 11.08 | 82.42 ± 12.12 | 78.47 ± 11.25 | 85.27 ± 11.96 |
| % treated with blood pressure drugs | 5.9 (34) | 5 (16) | 6.8 (18) | 7.1 (18) | 5.9 | 10.1 | 4.9 (16) | 3.8 | 5.7 |
| % reporting diabetes (n) | 11 (64) | 9.4 (30) | 12.9 (34) | 10.6 (27) | 8.6 | 15.9 | 11.3 (37) | 10.5 | 11.9 |
| % treated with diabetes drugs (n) | 2.9 (17) | 1.3 (4) | 4.9 (13) | 3.5 (9) | 1.6 | 8.7 | 2.4 (8) | 0.8 | 3.6 |
| % reporting fatty liver | 10.8 (63) | 7.9 (25) | 14.4 (38) | 7.5 (19) * | 5.9 | 11.6 | 13.5 (44) | 10.5 | 15.5 |
| % reporting diagnosis of hypertriglyceridemia | 17.0 (99) | 16.4 (52) | 17.9 (47) | 15.4 (39) | 14.6 | 17.4 | 18.3 (60) | 18.8 | 18.0 |
| % treated with lipid- lowering drugs (n) | 6.7 (39) | 5.7 (18) | 8 (21) | 7.9 (20) | 5.4 | 14.5 * | 5.8 (19) | 6.0 | 5.7 |
| % treated with anti- platelet drugs (n) | 4.8 (28) | 2.5 (8) | 7.6 (20) | 5.1 (13) | 2.7 | 11.6 | 4.6 (15) | 2.3 | 6.2 |
| Mean MS score | 1.21 ± 1.18 | 1.07 ± 1.16 | 1.39 ± 1.19 | 1.02 ± 1.11 ** | 0.94 ± 1.07 * | 1.26 ± 1.16 | 1.36 ± 1.22 | 1.25 ± 1.25 | 1.44 ± 1.20 |
| % with high likelihood for MS (n) | 15 (87) | 12.6 (40) | 18 (47) | 10.4 (26) | 9.3 (17) | 13.2 (9) | 18.5 (61) | 17 (23) | 19.5 (38) |
| Potassium Excretion (Creatinine Adjusted) (n = 581) | Potassium intake by 24-h ReCall (Adjusted for Energy) (n = 556) | Potassium Intake by FFQ (Adjusted for Energy) (n = 510) | Sodium/Potassium Excretion Ratio (n = 580) | Sodium Excretion (Creatinine Adjusted) (n = 580) | |
|---|---|---|---|---|---|
| Age (years) | 0.184 ** (M: 0.174 **) (F: 0.217 **) | 0.212 ** | 0.086 | −0.125 ** (M: −0.176 **) | 0.068 (F: 0.122 *) |
| Caloric intake (Kcals) | −0.164 ** | NR | NR | 0.129 ** | −0.037 |
| BMI (kg/m2) | −0.142 ** (F: −0.142 *) | 0.017 | −0.055 | 0.151 ** (F: 0.216 **) | 0.022 |
| Mean systolic blood pressure (mm/Hg) | −0.095 * | 0.028 | 0.02 | 0.095 * | 0.018 (F: 0.136 *) |
| Mean diastolic blood pressure (mm/Hg) | −0.143 ** (M: −0.186 **) | −0.031 | −0.02 | 0.095 * | −0.016 |
| Elevated blood pressure-measured (yes/no) | −0.108 * | 0.073 (F: 0.131 *) | 0.021 | 0.113 ** | 0.037 (F: 0.118 *) |
| All physical activity frequency 1 | −0.113* | −0.078 | −0.219 ** (M: −0.227 *) (F: −0.247 **) | 0.065 | −0.027 |
| Fatty liver (yes/no) | −0.132 ** | −0.05 | −0.210 ** (M: −0.214 **) (F: −0.131 *) | 0.100 * | −0.022 |
| Diabetes (yes/no) | −0.001 | −0.03 | 0.023 | 0.048 | 0.051 |
| Overweight/obese (BMI ≥ 28.5 kg/m2) (yes/no) | −0.162 ** | 0.029 | −0.062 | 0.157 ** | 0.018 |
| Hypertriglyceridemia (yes/no) | 0.003 | 0.052 | −0.022 | −0.059 | −0.042 |
| MS score | −0.161 ** (M: −0.127 *) (F: −0.119 *) | −0.055 | −0.051 | 0.119 ** (F: 0.126 *) | −0.018 |
| Model Including Potassium Excretion (Creatinine Adjusted) (n = 554) | Model Including Sodium/Potassium Excretion Ratio (n = 554) | Model Including Sodium Excretion (Creatinine Adjusted) (n = 554) | |
|---|---|---|---|
| Variables included in the model (order in regression/level of “impact”) | (1) Age; and (2) potassium excretion | (1) Age; ( 2) Sodium/potassium excretion ratio; and (3) Sex | (1) Age; (2) Sex; and (3) Physical activity |
| Variables excluded from the model | Caloric intake; Sex; Physical activity | Caloric intake; Physical activity | Sodium excretion; Caloric intake |
| Coefficients for each variable (95% CI) | Age, 0.032 (0.025, 0.04); Potassium excretion, (−0.285–0.387, −0.183) | Age, 0.030 (0.022, 0.038); Sodium/potassium ratio, 0.255 (0.109, 0.402); and Sex, 0.275 (0.087, 0.462) | Age, 0.029 (0.021, 0.037); Sex, 0.326 (0.140, 0.512); and Physical activity, −0.201 (−0.387, −0.015) |
| Total R square of the model (% related to the electrolytes excretion) | 13.4 (4.8) | 12.4 (2.5) | 11.3 (NI) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buch, A.; Goldsmith, R.; Nitsan, L.; Margaliot, M.; Shefer, G.; Marcus, Y.; Stern, N. 24-h Potassium Excretion Is Associated with Components of the Metabolic Syndrome: Results from a National Survey Based on Urine Collection in Adults. Nutrients 2021, 13, 2689. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082689
Buch A, Goldsmith R, Nitsan L, Margaliot M, Shefer G, Marcus Y, Stern N. 24-h Potassium Excretion Is Associated with Components of the Metabolic Syndrome: Results from a National Survey Based on Urine Collection in Adults. Nutrients. 2021; 13(8):2689. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082689
Chicago/Turabian StyleBuch, Assaf, Rebecca Goldsmith, Lesley Nitsan, Miri Margaliot, Gabi Shefer, Yonit Marcus, and Naftali Stern. 2021. "24-h Potassium Excretion Is Associated with Components of the Metabolic Syndrome: Results from a National Survey Based on Urine Collection in Adults" Nutrients 13, no. 8: 2689. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082689