
Effects of Milk Protein in Resistance Training-Induced Lean Mass Gains for Older Adults Aged ≥ 60 y: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Assessment of Risk of Bias
2.5. Statistical Analysis
3. Results
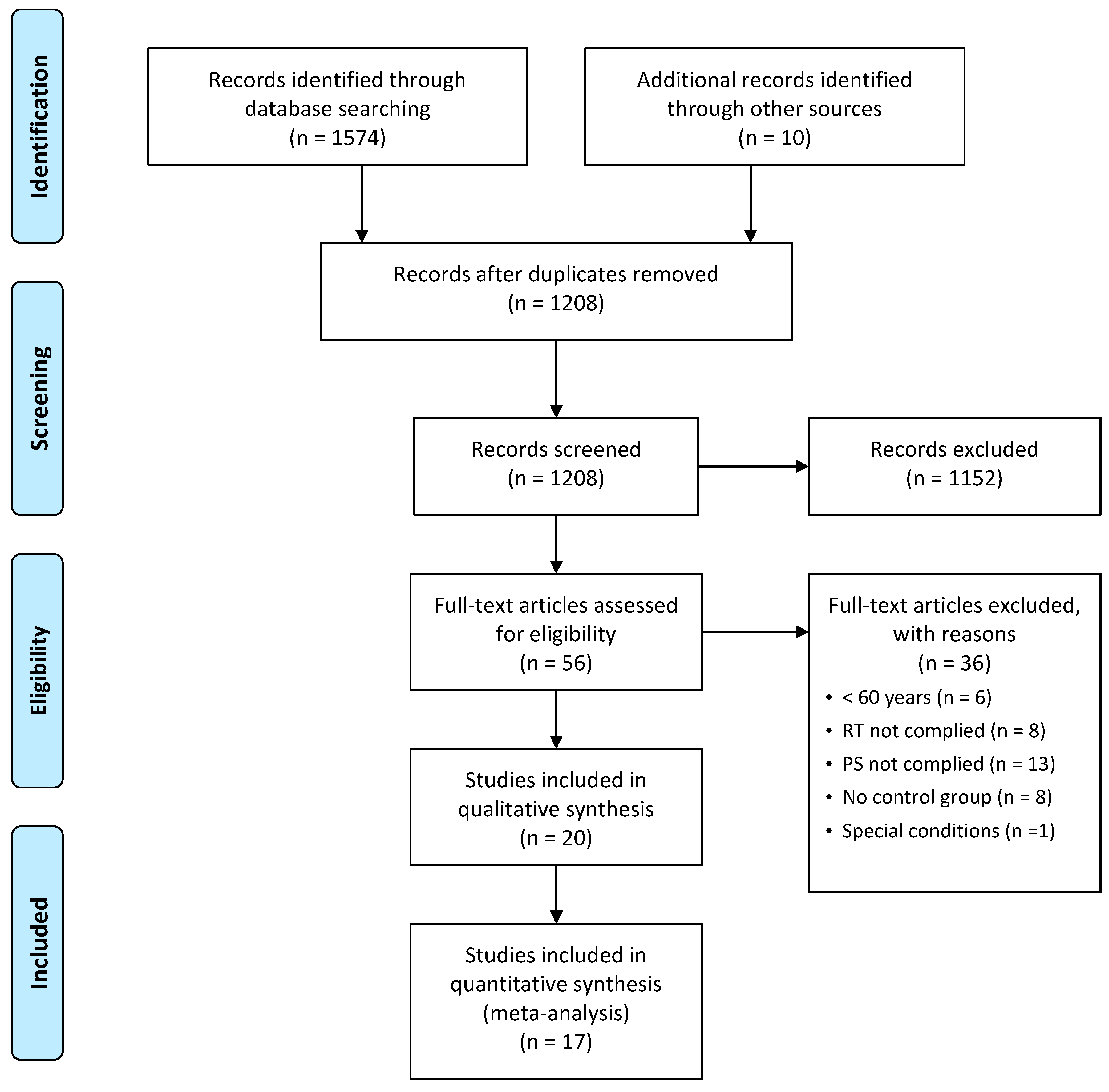
3.1. Literature Search
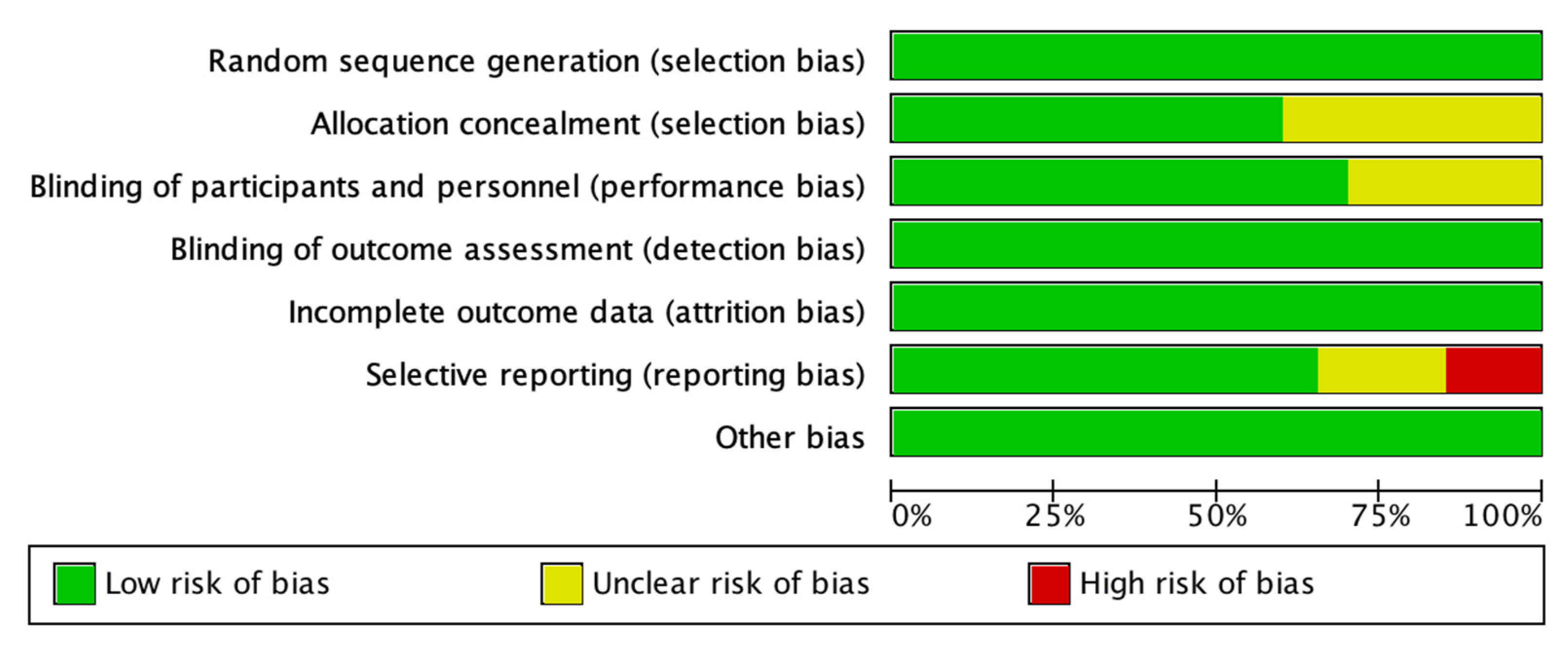
3.2. Risk of Bias Assessment
3.3. Participants Characteristics
3.4. RT Characteristics
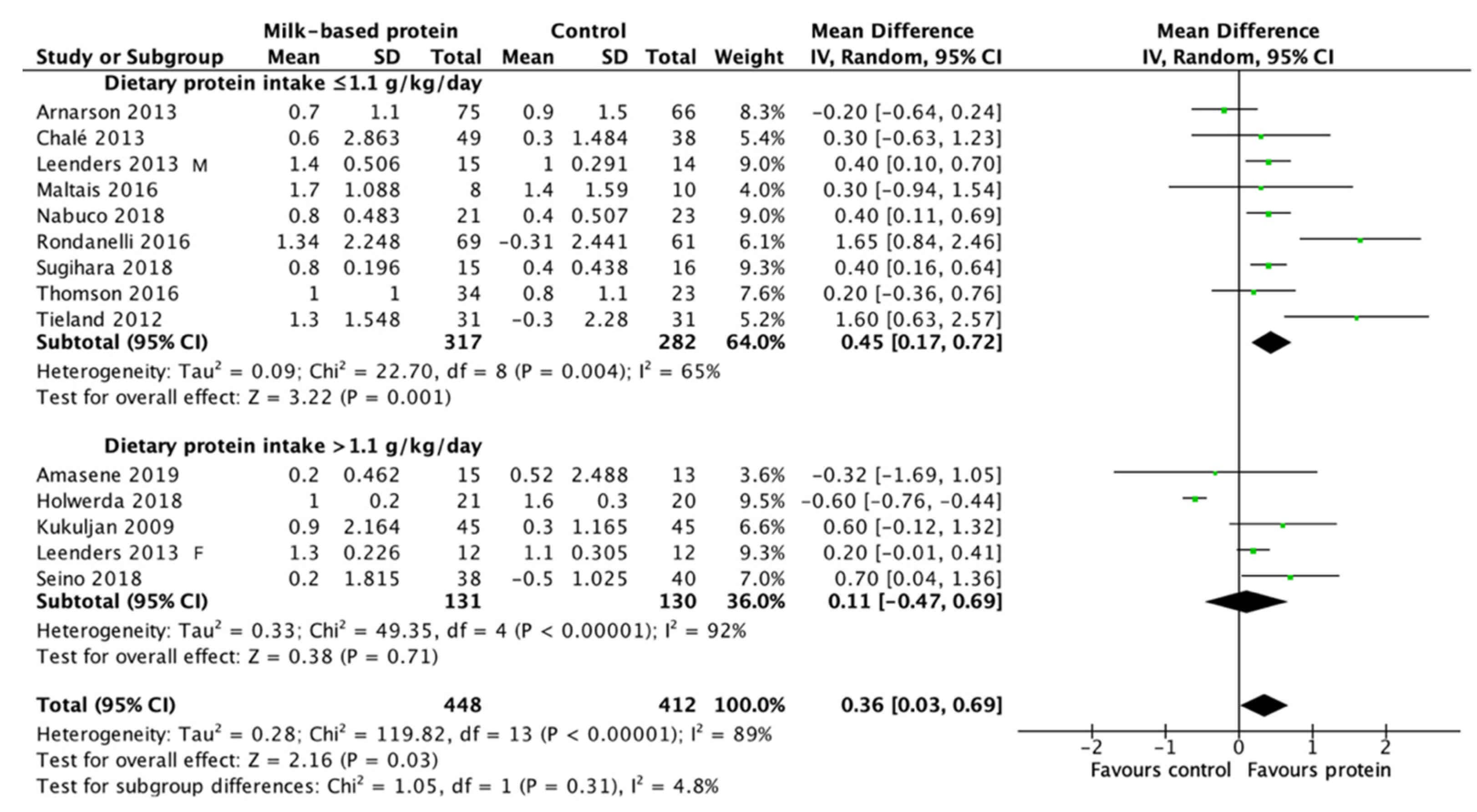
3.5. Effect of Daily Protein Intake on the RT-induced LBM/FFM Gains
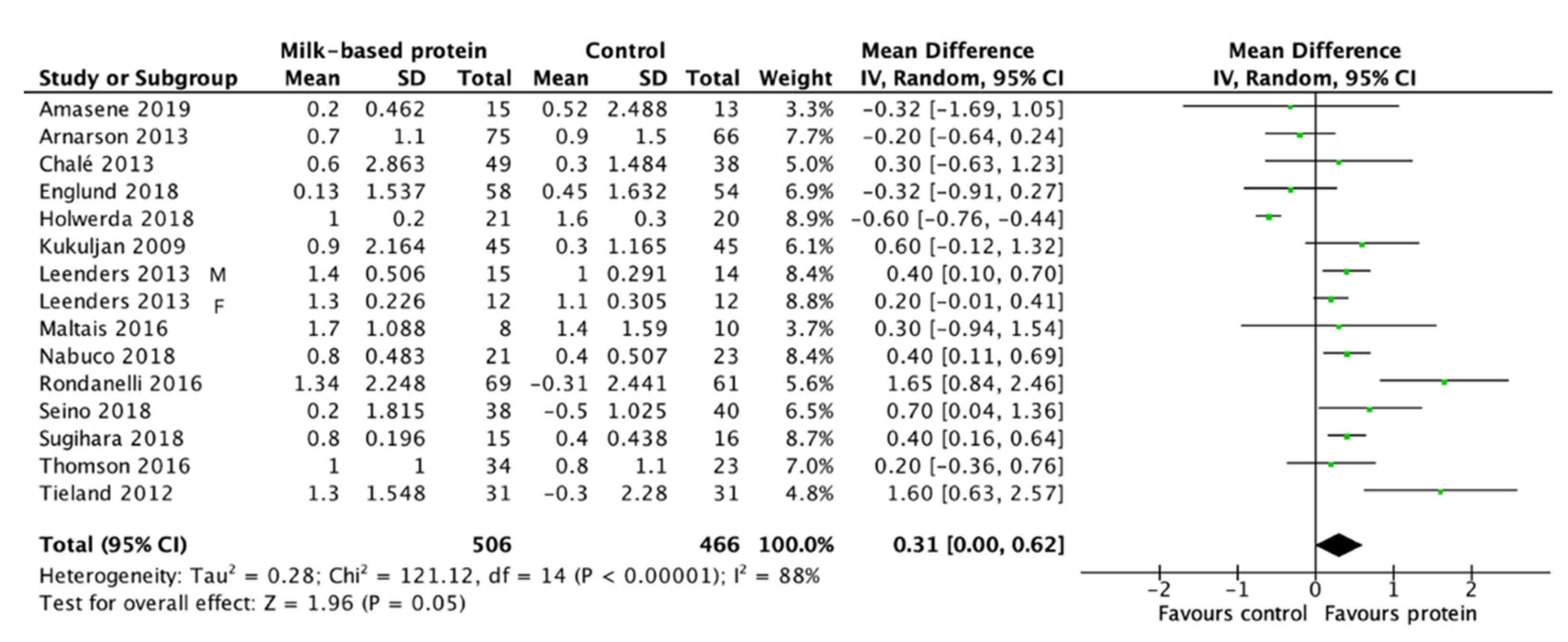
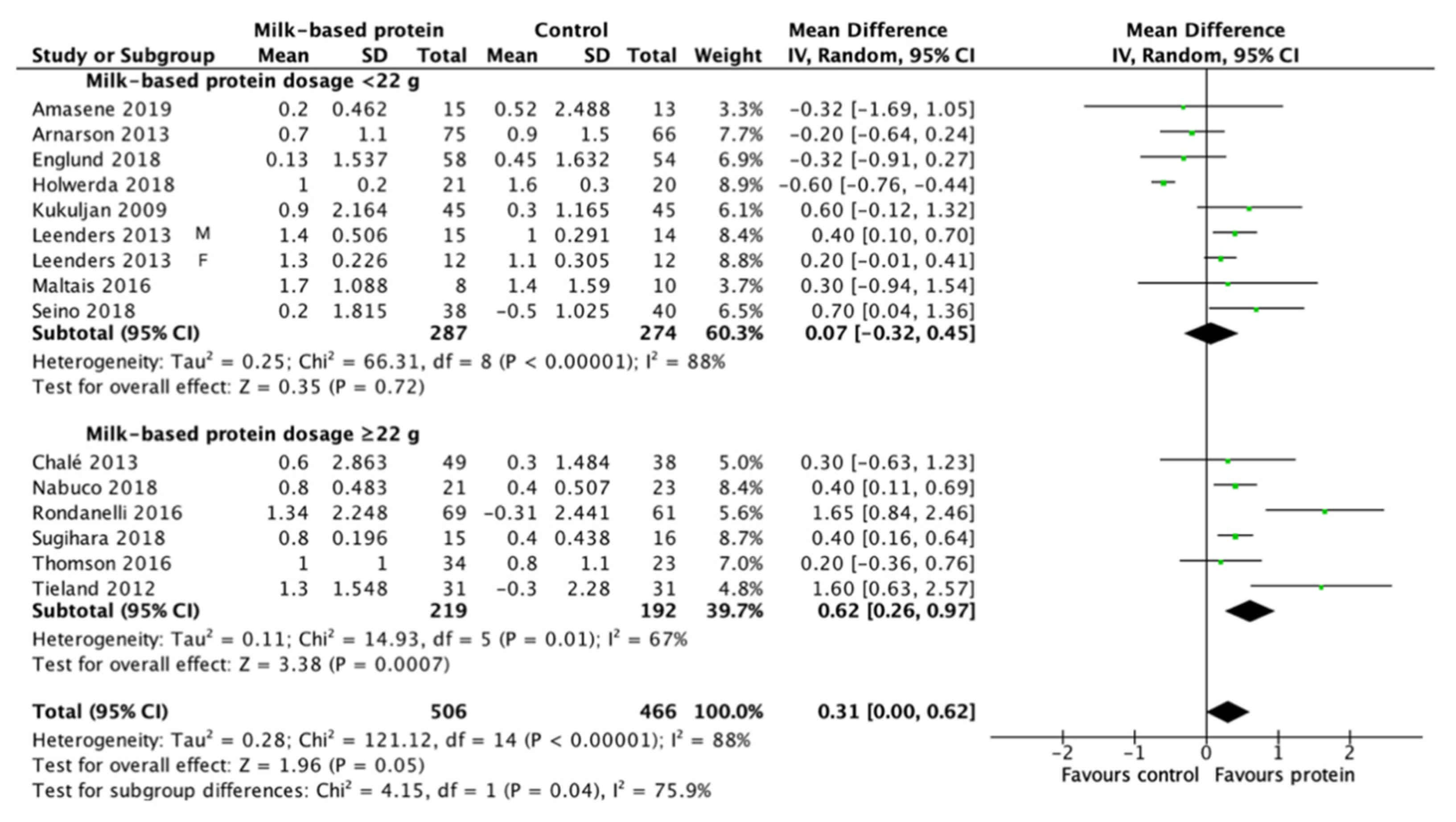
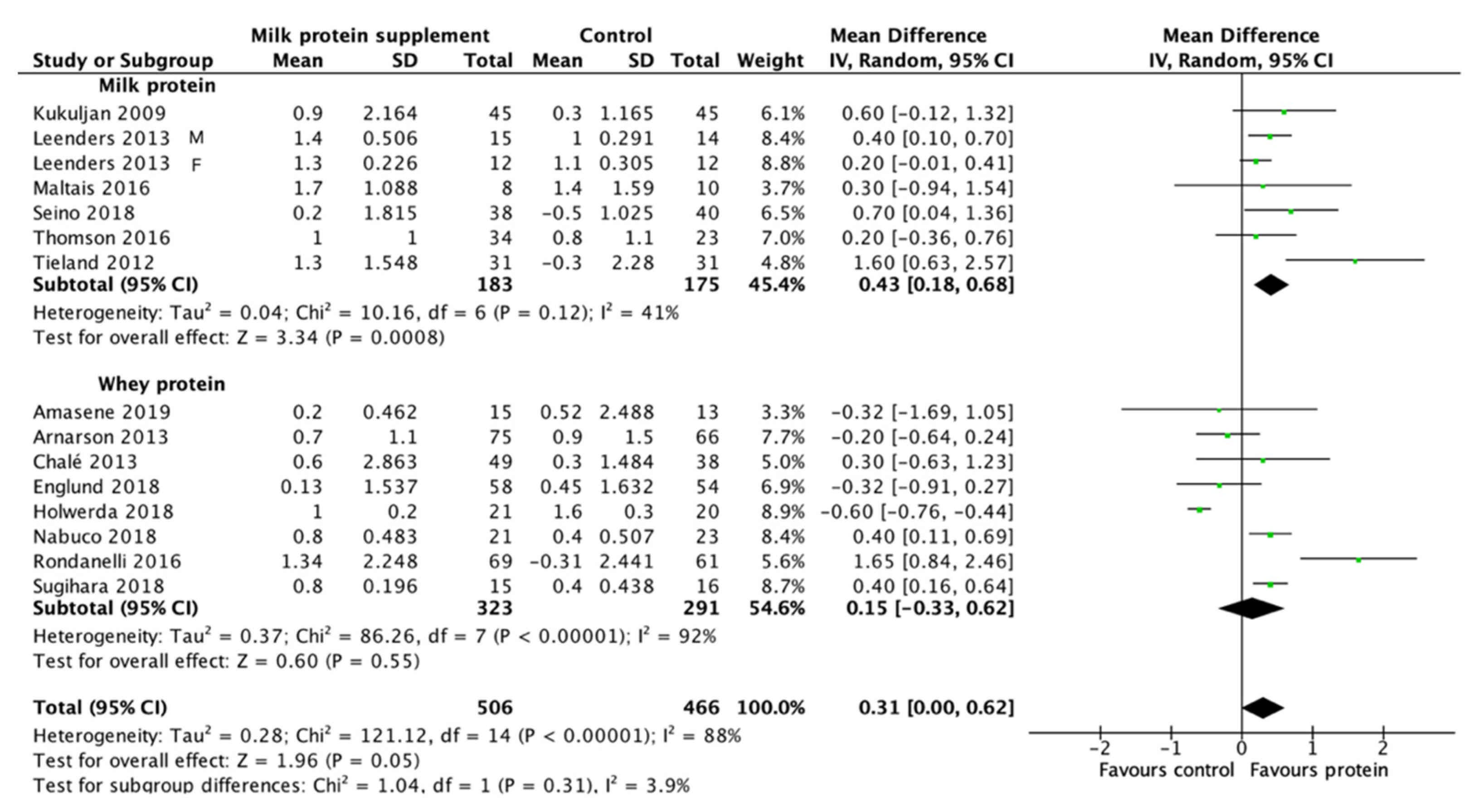
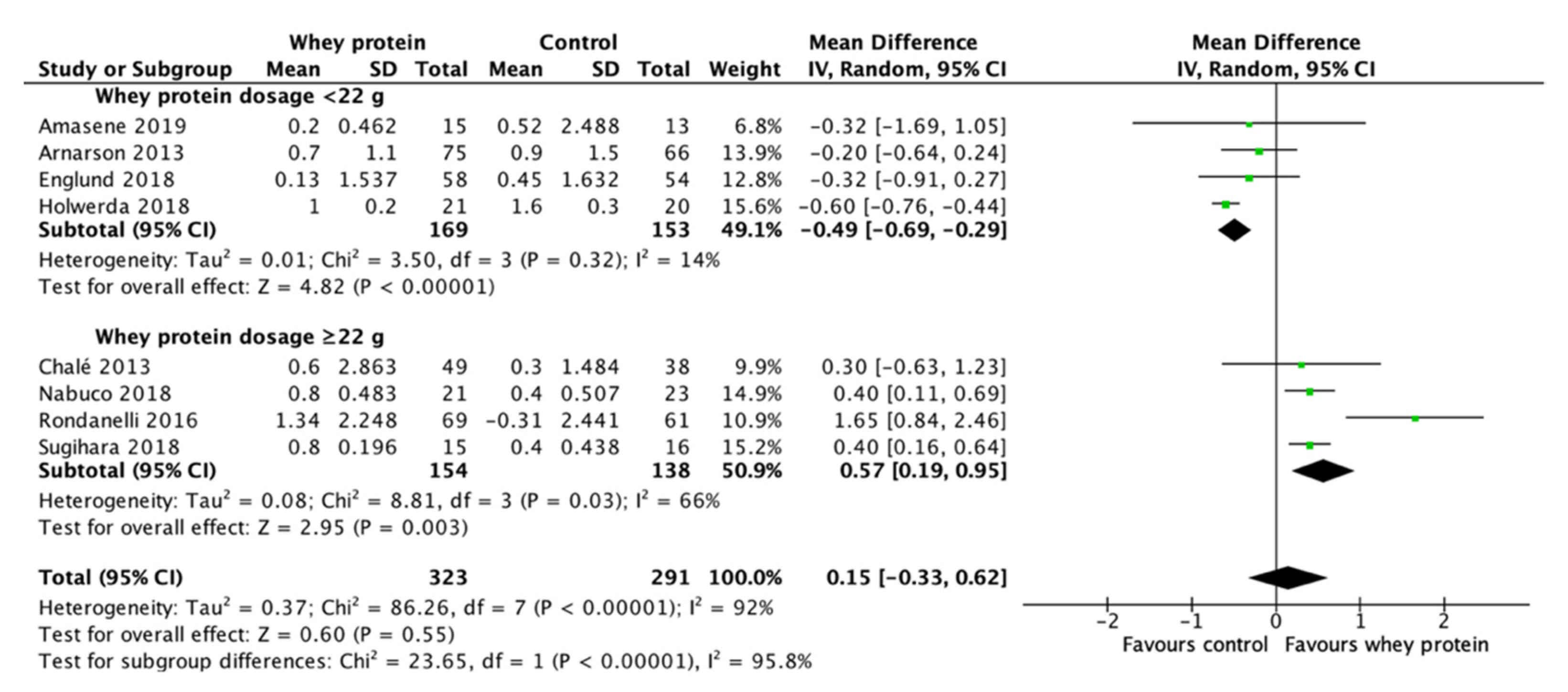
3.6. Effect of Milk-Based Protein Supplementation on LBM/FFM
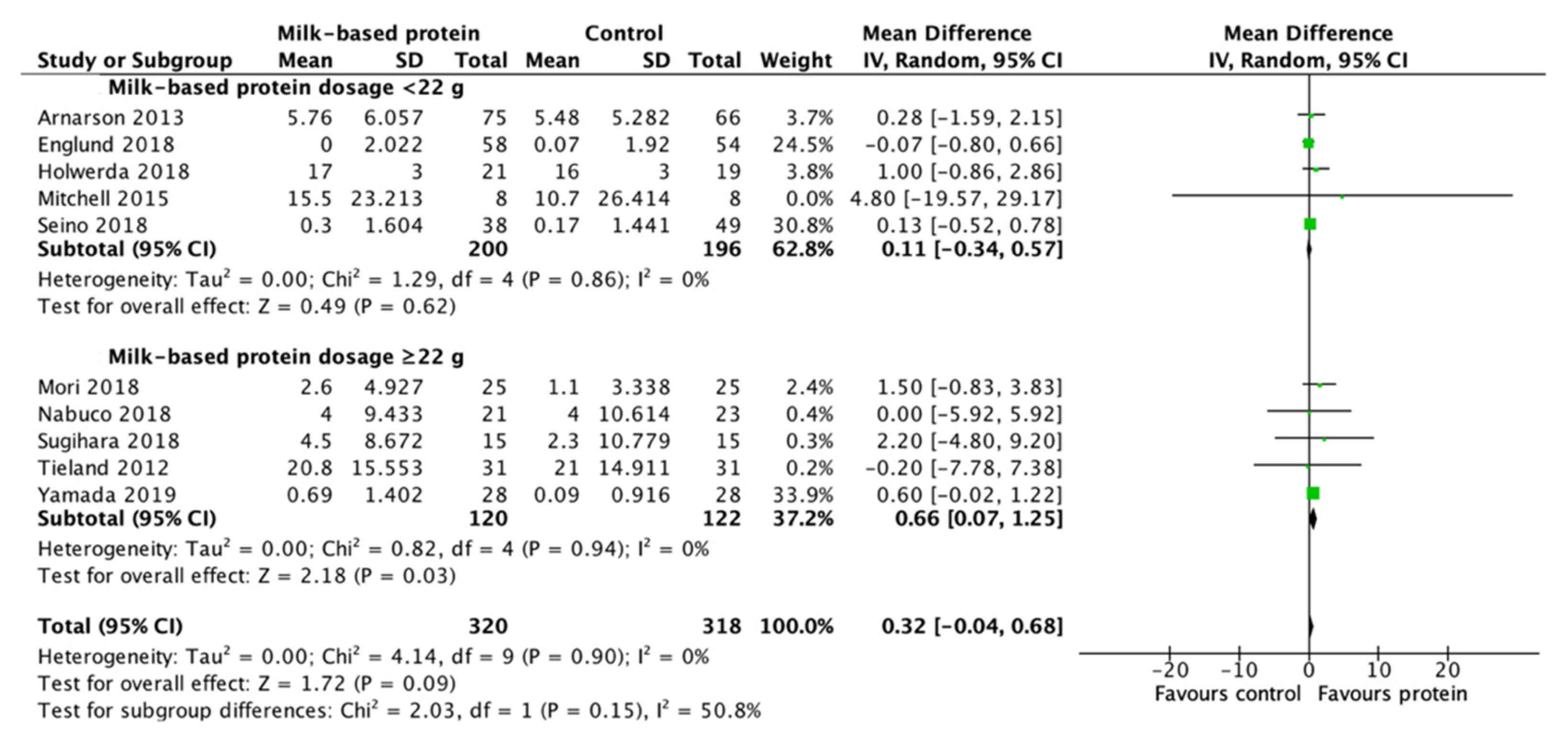
3.7. Effect of Milk-Based Protein Supplementation on Muscle Strength
4. Discussion
4.1. Effect of Milk-Based Protein Supplementation Type
4.2. Effect of Milk-Based Protein Supplementation on RT-Induced LBM/FFM Gains
4.3. Effect of Milk-Based Protein Supplementation on RT-Induced Muscle Strength
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Von Haehling, S.; Morley, J.E.; Anker, S.D. An overview of sarcopenia: Facts and numbers on prevalence and clinical impact. J. Cachexia Sarcopenia Muscle 2010, 1, 129–133. [Google Scholar] [CrossRef]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. A Biol. Sci. Med. 2006, 61, 72–77. [Google Scholar] [CrossRef]
- Sasaki, H.; Kasagi, F.; Yamada, M.; Fujita, S. Grip strength predicts cause-specific mortality in middle-aged and elderly persons. Am. J. Med. 2007, 120, 337–342. [Google Scholar] [CrossRef]
- Go, S.W.; Cha, Y.H.; Lee, J.A.; Park, H.S. Association between sarcopenia, bone density, and health-related quality of life in Korean men. Korean J. Fam. Med. 2013, 34, 281–288. [Google Scholar] [CrossRef]
- Chuang, S.Y.; Chang, H.Y.; Lee, M.S.; Chia-Yu Chen, R.; Pan, W.H. Skeletal muscle mass and risk of death in an elderly population. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Volaklis, K.A.; Halle, M.; Meisinger, C. Muscular strength as a strong predictor of mortality: A narrative review. Eur. J. Intern. Med. 2015, 26, 303–310. [Google Scholar] [CrossRef]
- Verlaan, S.; Aspray, T.J.; Bauer, J.M.; Cederholm, T.; Hemsworth, J.; Hill, T.R.; McPhee, J.S.; Piasecki, M.; Seal, C.; Sieber, C.C.; et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: A case-control study. Clin. Nutr. 2017, 36, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Xia, J.; Zhang, X.I.; Gathirua-Mwangi, W.G.; Guo, J.; Li, Y.; McKenzie, S.; Song, Y. Associations of muscle mass and strength with all-cause mortality among US older adults. Med. Sci. Sports Exerc. 2018, 50, 458–467. [Google Scholar] [CrossRef]
- Fiatarone, M.A.; Marks, E.C.; Ryan, N.D.; Meredith, C.N.; Lipsitz, L.A.; Evans, W.J. High-intensity strength training in nonagenarians: Effects on skeletal muscle. JAMA 1990, 263, 3029–3034. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 2010, 9, 226–237. [Google Scholar] [CrossRef] [Green Version]
- Peterson, M.D.; Sen, A.; Gordon, P.M. Influence of resistance exercise on lean body mass in aging adults: A meta-analysis. Med. Sci. Sports Exerc. 2011, 43, 249–258. [Google Scholar] [CrossRef] [Green Version]
- Cermak, N.M.; Res, P.T.; de Groot, L.C.; Saris, W.H.; van Loon, L.J. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: A meta-analysis. Am. J. Clin. Nutr. 2012, 96, 1454–1464. [Google Scholar] [CrossRef] [Green Version]
- Finger, D.; Goltz, F.R.; Umpierre, D.; Meyer, E.; Rosa, L.H.; Schneider, C.D. Effects of protein supplementation in older adults undergoing resistance training: A systematic review and meta-analysis. Sports Med. 2015, 45, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.K.; Quinn, M.A.; Saunders, D.H.; Greig, C.A. Protein supplementation does not significantly augment the effects of resistance exercise training in older adults: A systematic review. J. Am. Med. Dir. Assoc. 2016, 17, 951.e1–959.e9. [Google Scholar] [CrossRef] [Green Version]
- Liao, C.D.; Lee, P.H.; Hsiao, D.J.; Huang, S.W.; Tsauo, J.Y.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with exercise intervention on frailty indices, body composition, and physical function in frail older adults. Nutrients 2018, 10, 1916. [Google Scholar] [CrossRef] [Green Version]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]
- Churchward-Venne, T.A.; Breen, L.; Di Donato, D.M.; Hector, A.J.; Mitchell, C.J.; Moore, D.R.; Stellingwerff, T.; Breuille, D.; Offord, E.A.; Baker, S.K. Leucine supplementation of a low-protein mixed macronutrient beverage enhances myofibrillar protein synthesis in young men: A double-blind, randomized trial. Am. J. Clin. Nutr. 2014, 99, 276–286. [Google Scholar] [CrossRef] [Green Version]
- Phillips, S.M.; Tipton, K.; Ferrando, A.A.; Wolfe, R.R. Resistance training reduces the acute exercise-induced increase in muscle protein turnover. Am. J. Physiol. 1999, 276, E118–E124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorissen, S.H.; Phillips, S.M. Branched-chain amino acids (leucine, isoleucine, and valine) and skeletal muscle. In Nutrition and Skeletal Muscle; Academic Press: Cambridge, MA, USA, 2019; pp. 283–298. [Google Scholar]
- Devries, M.C.; McGlory, C.; Bolster, D.R.; Kamil, A.; Rahn, M.; Harkness, L.; Baker, S.K.; Phillips, S.M. Leucine, not total protein, content of a supplement is the primary determinant of muscle protein anabolic responses in healthy older women. J. Nutr. 2018, 148, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Pennings, B.; Boirie, Y.; Senden, J.M.; Gijsen, A.P.; Kuipers, H.; van Loon, L.J. Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older men. Am. J. Clin. Nutr. 2011, 93, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Hanach, N.I.; McCullough, F.; Avery, A. The impact of dairy protein intake on muscle mass, muscle strength, and physical performance in middle-aged to older adults with or without existing sarcopenia: A systematic review and meta-analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: www.handbook.cochrane.org (accessed on 15 January 2021).
- American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Candow, D.G.; Chilibeck, P.D.; Facci, M.; Abeysekara, S.; Zello, G.A. Protein supplementation before and after resistance training in older men. Eur. J. Appl. Physiol. 2006, 97, 548–556. [Google Scholar] [CrossRef]
- Verdijk, L.B.; Jonkers, R.A.; Gleeson, B.G.; Beelen, M.; Meijer, K.; Savelberg, H.H.; Wodzig, W.K.; Dendale, P.; van Loon, L.J. Protein supplementation before and after exercise does not further augment skeletal muscle hypertrophy after resistance training in elderly men. Am. J. Clin. Nutr. 2009, 89, 608–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirk, B.; Mooney, K.; Amirabdollahian, F.; Khaiyat, O. Exercise and dietary-protein as a countermeasure to skeletal muscle weakness: Liverpool Hope University—Sarcopenia Aging Trial (LHU-SAT). Front. Physiol. 2019, 10, 445. [Google Scholar] [CrossRef] [Green Version]
- Tieland, M.; Dirks, M.L.; van der Zwaluw, N.; Verdijk, L.B.; Van De Rest, O.; de Groot, L.C.; Van Loon, L.J. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 713–719. [Google Scholar] [CrossRef]
- Arnarson, A.; Gudny Geirsdottir, O.; Ramel, A.; Briem, K.; Jonsson, P.V.; Thorsdottir, I. Effects of whey proteins and carbohydrates on the efficacy of resistance training in elderly people: Double blind, randomised controlled trial. Eur. J. Clin. Nutr. 2013, 67, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Chale, A.; Cloutier, G.J.; Hau, C.; Phillips, E.M.; Dallal, G.E.; Fielding, R.A. Efficacy of whey protein supplementation on resistance exercise-induced changes in lean mass, muscle strength, and physical function in mobility-limited older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 682–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leenders, M.; Verdijk, L.B.; Van der Hoeven, L.; Van Kranenburg, J.; Nilwik, R.; Wodzig, W.K.; Senden, J.M.; Keizer, H.A.; Van Loon, L.J. Protein supplementation during resistance-type exercise training in the elderly. Med. Sci. Sports Exerc. 2013, 45, 542–552. [Google Scholar] [CrossRef]
- Mitchell, C.J.; Oikawa, S.Y.; Ogborn, D.I.; Nates, N.J.; MacNeil, L.G.; Tarnopolsky, M.; Phillips, S.M. Daily chocolate milk consumption does not enhance the effect of resistance training in young and old men: A randomized controlled trial. Appl. Physiol. Nutr. Metab. 2015, 40, 199–202. [Google Scholar] [CrossRef]
- Maltais, M.L.; Perreault, K.; Courchesne-Loyer, A.; Lagacé, J.-C.; Barsalani, R.; Dionne, I.J. Effect of resistance training and various sources of protein supplementation on body fat mass and metabolic profile in sarcopenic overweight older adult men: A pilot study. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef]
- Englund, D.A.; Kirn, D.R.; Koochek, A.; Zhu, H.; Travison, T.G.; Reid, K.F.; von Berens, A.; Melin, M.; Cederholm, T.; Gustafsson, T.; et al. Nutritional supplementation with physical activity improves muscle composition in mobility-limited older adults, the VIVE2 study: A randomized, double-blind, placebo-controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 73, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Holwerda, A.M.; Overkamp, M.; Paulussen, K.J.M.; Smeets, J.S.J.; van Kranenburg, J.; Backx, E.M.P.; Gijsen, A.P.; Goessens, J.P.B.; Verdijk, L.B.; van Loon, L.J.C. Protein supplementation after exercise and before sleep does not further augment muscle mass and strength gains during resistance exercise training in active older men. J. Nutr. 2018, 148, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Nabuco, H.C.G.; Tomeleri, C.M.; Sugihara Junior, P.; Fernandes, R.R.; Cavalcante, E.F.; Antunes, M.; Ribeiro, A.S.; Teixeira, D.C.; Silva, A.M.; Sardinha, L.B.; et al. Effects of whey protein supplementation pre- or post-resistance training on muscle mass, muscular strength, and functional capacity in pre-conditioned older women: A randomized clinical trial. Nutrients 2018, 10, 563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugihara Junior, P.; Ribeiro, A.S.; Nabuco, H.C.G.; Fernandes, R.R.; Tomeleri, C.M.; Cunha, P.M.; Venturini, D.; Barbosa, D.S.; Schoenfeld, B.J.; Cyrino, E.S. Effects of whey protein supplementation associated with resistance training on muscular strength, hypertrophy, and muscle quality in preconditioned older women. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 528–535. [Google Scholar] [CrossRef]
- Amasene, M.; Besga, A.; Echeverria, I.; Urquiza, M.; Ruiz, J.R.; Rodriguez-Larrad, A.; Aldamiz, M.; Anaut, P.; Irazusta, J.; Labayen, I. Effects of leucine-enriched whey protein supplementation on physical function in post-hospitalized older adults participating in 12-weeks of resistance training program: A randomized controlled trial. Nutrients 2019, 11, 2337. [Google Scholar] [CrossRef] [Green Version]
- Kukuljan, S.; Nowson, C.A.; Sanders, K.; Daly, R.M. Effects of resistance exercise and fortified milk on skeletal muscle mass, muscle size, and functional performance in middle-aged and older men: An 18-mo randomized controlled trial. J. Appl. Physiol. 2009, 107, 1864–1873. [Google Scholar] [CrossRef]
- Thomson, R.L.; Brinkworth, G.D.; Noakes, M.; Buckley, J.D. Muscle strength gains during resistance exercise training are attenuated with soy compared with dairy or usual protein intake in older adults: A randomized controlled trial. Clin. Nutr. 2016, 35, 27–33. [Google Scholar] [CrossRef]
- Mori, H.; Tokuda, Y. Effect of whey protein supplementation after resistance exercise on the muscle mass and physical function of healthy older women: A randomized controlled trial. Geriatr. Gerontol. Int. 2018, 18, 1398–1404. [Google Scholar] [CrossRef] [Green Version]
- Seino, S.; Sumi, K.; Narita, M.; Yokoyama, Y.; Ashida, K.; Kitamura, A.; Shinkai, S. Effects of low-dose dairy protein plus micronutrient supplementation during resistance exercise on muscle mass and physical performance in older adults: A randomized, controlled trial. J. Nutr. Health Aging 2018, 22, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Otobe, Y.; Tanaka, T.; Ohji, S.; Koyama, S.; Sato, A.; Suzuki, M.; et al. Synergistic effect of bodyweight resistance exercise and protein supplementation on skeletal muscle in sarcopenic or dynapenic older adults. Geriatr. Gerontol. Int. 2019, 19, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R.; Churchward-Venne, T.A.; Witard, O.; Breen, L.; Burd, N.A.; Tipton, K.D.; Phillips, S.M. Protein ingestion to stimulate myofibrillar protein synthesis requires greater relative protein intakes in healthy older versus younger men. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 57–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorissen, S.H.; Trommelen, J.; Kouw, I.W.; Holwerda, A.M.; Pennings, B.; Groen, B.B.; Wall, B.T.; Churchward-Venne, T.A.; Horstman, A.M.; Koopman, R. Protein type, protein dose, and age modulate dietary protein digestion and phenylalanine absorption kinetics and plasma phenylalanine availability in humans. J. Nutr. 2020, 150, 2041–2050. [Google Scholar] [CrossRef]
- Cribb, P.J.; Hayes, A. Effects of supplement-timing and resistance exercise on skeletal muscle hypertrophy. Med. Sci. Sports Exerc. 2006, 38, 1918–1925. [Google Scholar] [CrossRef] [Green Version]
- Devries, M.C.; Phillips, S.M. Supplemental protein in support of muscle mass and health: Advantage whey. J. Food Sci. 2015, 80, A8–A15. [Google Scholar] [CrossRef]
- Boirie, Y.; Dangin, M.; Gachon, P.; Vasson, M.-P.; Maubois, J.-L.; Beaufrère, B. Slow and fast dietary proteins differently modulate postprandial protein accretion. Proc. Natl. Acad. Sci. USA 1997, 94, 14930–14935. [Google Scholar] [CrossRef] [Green Version]
- Cholewa, J.M.; Newmire, D.E.; Zanchi, N.E. Carbohydrate restriction: Friend or foe of resistance-based exercise performance? Nutrition 2019, 60, 136–146. [Google Scholar] [CrossRef]
- Morton, R.W.; McGlory, C.; Phillips, S.M. Nutritional interventions to augment resistance training-induced skeletal muscle hypertrophy. Front. Physiol. 2015, 6, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elahi, D.; Muller, D.C.; Egan, J.M.; Andres, R.; Veldhuis, J.; Meneilly, G.S. Glucose tolerance, glucose utilization and insulin secretion in ageing. Novartis Found. Symp. 2002, 242, 222–242. [Google Scholar] [PubMed]
- US Department of Agriculture. FoodData Central. Available online: Fdc.nal.usda.gov (accessed on 15 January 2021).
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman, J.W.; Tang, J.E.; Wilkinson, S.B.; Tarnopolsky, M.A.; Lawrence, R.L.; Fullerton, A.V.; Phillips, S.M. Consumption of fat-free fluid milk after resistance exercise promotes greater lean mass accretion than does consumption of soy or carbohydrate in young, novice, male weightlifters. Am. J. Clin. Nutr. 2007, 86, 373–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year Country | Intervention Duration | Number of Participants | Participant Characteristics | Resistance Training | Protein Supplementation | Protein Intake Pre (Post) Intervention | Outcome Measured |
| Amasene et al., 2019 [39] Spain | 12 weeks | 28 | Female and male Post-hospitalization Age: 82 years. BMI: 27–30 kg/m2 | 2 days/week 2 sets to max reps 6 exercises 50–70% 1RM | 20 g whey (3 g leucine) post exercise | N/A | LBM |
| Arnarson et al., 2013 [32] Iceland | 12 weeks | 161 | Female and male Healthy, or hypertension, hyperlipidemia, diabetes type II Age: 65–91 years. BMI: 28–29 kg/m2 | 3 days/week 3 sets × 6–8 reps 10 exercises 75–80% 1RM | 20 g whey post RET | P: 1.00 ± 0.26 kg/d (1.06 ± 0.23 kg/d) CON: 0.92 ± 0.30 kg/d (0.89 ± 0.23 kg/d) | LBM KE |
| Candow et., 2006 [28] Canada | 12 weeks | 38 | Male Age: 59–76 years. BMI: 28.2 kg/m2 | 3 days/week 3 sets × 10 reps 8 exercises 70% 1RM | 0.3 g/kg (~25.6 g) whey post RET | P: 1.14 kg/d (1.38 kg/d) CON: 1.28 kg/d | LBM LP |
| Chale et al., 2013 [33] USA | 6 months | 80 | Female and male Mobility-limited Age: 70–85 years. BMI: 27 kg/m2 | 3 days/week 3 sets × 12 reps 5 exercises 80% 1RM | 40 g whey daily post RET | P: 0.96 kg/d (1.22 kg/d) CON: 0.92 kg/d | LBM LP |
| Englund et al., 2017 [38] USA | 6 months | 149 | Female and male Mobility-limited Age: 78 ± 5.4 years. BMI: 28 kg/m2 | 3 days/week 2 sets × 10 reps 5 leg-exercises 15 to 6 Borg’s scale | 20 g whey daily or post RET | N/A | LBM KE |
| Holwerda et al., 2018 [39] Netherlands | 12 weeks | 41 | Female and male Healthy Age: 70 ± 1 years. BMI: 25.3 ± 0.4 kg/m2 | 3 days/week 2–4 sets × 10 reps 6 exercises 70–80% 1RM | 21 g whey protein (3 g leucine) post RET and before sleep | P: 1.14 ± 0.05 kg/d (1.43 ± 0.04 kg/d) CON: 1.19 ± 0.06 kg/d (1.17 ± 0.06 kg/d) | LBM KE |
| Kirk et al., 2019 [30] United Kindom | 16 weeks | 46 | Female and male Non-frail healthy Age: 68 ± 5 years. BMI: 27.8 ± 6.2 kg/m2 | 2 days/week 2 sets to fatigue 6 exercises moderate weight | 1.5 g/kg/day whey 0.5 g × 3 times/day | P: 1.16 ± 0.4 kg/d (1.63 ± 0.5 kg/d) CON: 1.10 ± 0.4 kg/d (1.04 ± 0.3 kg/d) | LP |
| Kukuljan et al., 2009 [43] Australia | 18 months | 180 | Male Healthy Age: 50–79 years. BMI: 27.1 kg/m2 | 3 days/week 3–4 sets × 15–20 reps 10–14 exercises 60–85% 1RM | 13.2 g milk protein daily | P: 1.26 ± 0.32 kg/d (+0.06 kg/d) CON: 1.32 ± 0.32 kg/d (−0.1 kg/d) | LBM |
| Leenders et al., 2013 [34] | 24 weeks | 60 | Female and male Healthy Age: 78 ± 1 years. BMI: 24–27 kg/m2 | 3 days/week 3–4 sets × 8 reps 4 exercises 50–80% 1RM | 15 g milk protein daily after breakfast | Women: 1.2 kg/d P: (+0.24 kg/d) Men: 1.1 kg/d P: (+0.18 kg/d) | LBM LP |
| Maltais et al., 2016 [36] Canada | 16 weeks | 26 | Male Sarcopenic Age: 65 ± 5 years. BMI: 26–27 kg/m2 | 3 days/week 3 sets × 8 reps8 exercisers 80% 1RM | 13.53 g milk protein post RET | P: 1.03 kg/d (2.12 kg/d) CON: 1.25 kg/d (1.06 kg/d) | LBM |
| Mitchell et al., 2015 [35] Canada | 12 weeks | 16 | Male Healthy Age: 74.4 ± 5.4 years. BMI: 26.9 ± 3.2 kg/m2 | 2 days/week 4 × leg exercises 1 days/week 7 × upper body exercises 3–4 sets 75–80% 1RM | 14 g milk protein daily post RET or breakfast | N/A | KE |
| Mori and Tokuda, 2018 [45] Japan | 24 weeks | 81 | Female Healthy Age: 70.6 ± 4 years. BMI: 22–23 kg/m2 | 2 days/week > 40 min 7 exercises 50–70% 1RM | 22.3 g whey post RET | Both groups 1.3 ± 0.0 kg/d (1.4 ± 0.1 kg/d) | LLMM KE |
| Nabuco et al., 2018 [40] Brazil | 12 weeks | 70 | Female Healthy Age: > 60 years. BMI: 23–26.5 kg/m2 | 3 days/week 3 sets × 8–12 RM 8 exercises | 27.1 g whey post RET | P: 0.94 ± 0.36 kg/d (1.49 ± 0.46 kg/d) CON: 0.95 ± 0.27 kg/d (1.0 ± 0.25 kg/d) | SMM KE |
| Rondanelli et al., 2016 [37] Italy | 12 weeks | 130 | Female and male Sarcopenic Age: 80.3 years. BMI: 23.9 kg/m2 | 5 days/week 20-min/day 12–14 Borg Rate | 22 g whey daily | P: 0.9 g/kg (unchanged) CON: 1.0 g/kg (unchanged) | FFM HG |
| Seino et al., 2018 [46] Japan | 12 weeks | 82 | Female and male Non-disabled Age: 73.5 years. BMI: 22.9 ± 2 kg/m2 | 2 days/week 2 sets × 20 reps whole body somewhat hard | 10.5 g milk protein daily | P: 1.39 ± 0.36 kg/d (1.53 ± 0.33 kg/d) CON: 1.28 ± 0.26 kg/d (1.31 ± 0.26 kg/d) | LBM KE |
| Sugihara Junior et al., 2018 [41] Brazil | 12 weeks | 31 | Female Age: 67.4 ± 4.0 years. BMI: 25.5 ± 2.4 kg/m2 | 3 days/week 3 sets × 8–12 RM 8 exercises | 35 g whey post RET | P: 0.85 ± 0.1 kg/d (1.4 ± 0.1 kg/d) CON: 0.81 ± 0.1 kg/d (0.87 ± 0.1 kg/d) | SMM KE |
| Thomson et al., 2016 [44] Australia | 12 weeks | 125 | Female and male Healthy Age: 61.5 ± 7.4 years. BMI: 27.6 ± 3.6 kg/m2 | 3 days/week 3 sets × 8–12 reps 5 exercises 8RM | 27 g dairy protein spread to each main meal or post RET | P: 1.06 ± 0.10 kg/d (1.42 ± 0.14 kg/d) CON: 1.10 ± 0.10 kg/d | LBM KE |
| Tieland et al., 2012 [31] Netherlands | 24 weeks | 62 | Female and male Prefrailty and frailty Age: 78 ± 1 years. | 2 days/week 3–4 sets × 15–20 reps 6 exercises 50–75% 1RM | 30 g milk protein (15 g at breakfast and lunch) | P: 1.0 kg/d (1.3 kg/d) CON: 1.0 kg/d | LBM KE |
| Verdijk et al., 2009 [29] Netherlands | 12 weeks | 26 | Male Healthy Age: 72 ± 2 years. BMI: 26~27 kg/m2 | 3 days/week 4 sets × 8 reps Leg extension and leg press 75–80% 1RM | 20 g casein before and post RET | Both groups (unchanged) 1.1 ± 0.1 kg/d (unchanged) | LBM KE LP |
| Yamada et al., 2019 [47] Japan | 12 weeks | 112 | Female and male sarcopenic or dynapenic Age: 84.2 ± 5.5 years. BMI: 22 kg/m2 | 2 days/week 7 exercises 3 sets × 20 reps | 10 g whey protein, daily | N/A | AMM KE |
| Study, Year Country | Duration | Sample Size | Participant Characteristics | Resistance Training | Protein Supplementation | Daily Protein Intake Pre (Post) | Outcome Measured |
| Amasene et al., 2019 [39] Spain | 12 weeks | 28 | Female and male Post-hospitalization Age: 82 years. BMI: 27–30 kg/m2 | 2 days/week 2 sets to max reps 6 exercises 50–70% 1RM | 20 g whey (3 g leucine) post exercise | N/A | LBM |
| Arnarson et al., 2013 [32] Iceland | 12 weeks | 161 | Female and male Healthy, or hypertension, hyperlipidemia, diabetes type II Age: 65–91 years. BMI: 28–29 kg/m2 | 3 days/week 3 sets × 6–8 reps 10 exercises 75–80% 1RM | 20 g whey post RET | P: 1.00 ± 0.26 kg/d (1.06 ± 0.23 kg/d) CON: 0.92 ± 0.30 kg/d (0.89 ± 0.23 kg/d) | LBM KE |
| Candow et al., 2006 [28] Canada | 12 weeks | 38 | Male Age: 59–76 years. BMI: 28.2 kg/m2 | 3 days/week 3 sets × 10 reps 8 exercises 70% 1RM | 0.3 g/kg (~25.6 g) whey post RET | P: 1.14 kg/d (1.38 kg/d) CON: 1.28 kg/d | LBM LP |
| Chale et al., 2013 [33] USA | 6 months | 80 | Female and male Mobility-limited Age: 70–85 years. BMI: 27 kg/m2 | 3 days/week 3 sets × 12 reps 5 exercises 80% 1RM | 40 g whey daily post RET | P: 0.96 kg/d (1.22 kg/d) CON: 0.92 kg/d | LBM LP |
| Englund et al., 2017 [38] USA | 6 months | 149 | Female and male Mobility-limited Age: 78 ± 5.4 years. BMI: 28 kg/m2 | 3 days/week 2 sets × 10 reps 5 leg-exercises 15 to 6 Borg’s scale | 20 g whey daily or post RET | N/A | LBM KE |
| Holwerda et al., 2018 [39] Netherlands | 12 weeks | 41 | Female and male Healthy Age: 70 ± 1 years. BMI: 25.3 ± 0.4 kg/m2 | 3 days/week 2–4 sets × 10 reps 6 exercises 70–80% 1RM | 21 g whey protein (3 g leucine) post RET and before sleep | P: 1.14 ± 0.05 kg/d (1.43 ± 0.04 kg/d) CON: 1.19 ± 0.06 kg/d (1.17 ± 0.06 kg/d) | LBM KE |
| Kirk et al., 2019 [30] UK | 16 weeks | 46 | Female and male Non-frail healthy Age: 68 ± 5 years. BMI: 27.8 ± 6.2 kg/m2 | 2 days/week 2 sets to fatigue 6 exercises moderate weight | 1.5 g/kg/day whey 0.5 g × 3 times/day | P: 1.16 ± 0.4 kg/d (1.63 ± 0.5 kg/d) CON: 1.10 ± 0.4 kg/d (1.04 ± 0.3 kg/d) | LP |
| Kukuljan et al., 2009 [43] Australia | 18 months | 180 | Male Healthy Age: 50–79 years. BMI: 27.1 kg/m2 | 3 days/week 3–4 sets × 15–20 reps 10–14 exercises 60–85% 1RM | 13.2 g milk protein daily | P: 1.26 ± 0.32 kg/d (+0.06 kg/d) CON: 1.32 ± 0.32 kg/d (−0.1 kg/d) | LBM |
| Leenders et al., 2013 [34] | 24 weeks | 60 | Female and male Healthy Age: 78 ± 1 years. BMI: 24–27 kg/m2 | 3 days/week 3–4 sets × 8 reps 4 exercises 50–80% 1RM | 15 g milk protein daily after breakfast | Women: 1.2 kg/d P: (+0.24 kg/d) Men: 1.1 kg/d P: (+0.18 kg/d) | LBM LP |
| Maltais et al., 2016 [36] Canada | 16 weeks | 26 | Male Sarcopenic Age: 65 ± 5 years. BMI: 26–27 kg/m2 | 3 days/week 3 sets × 8 reps8 exercisers 80% 1RM | 13.53 g milk protein post RET | P: 1.03 kg/d (2.12 kg/d) CON: 1.25 kg/d (1.06 kg/d) | LBM |
| Mitchell et al., 2015 [35] Canada | 12 weeks | 16 | Male Healthy Age: 74.4 ± 5.4 years. BMI: 26.9 ± 3.2 kg/m2 | 2 days/week 4 × leg exercises 1 days/week 7 × upper body exercises 3–4 sets 75–80% 1RM | 14 g milk protein daily post RET or breakfast | N/A | KE |
| Mori and Tokuda, 2018 [45] Japan | 24 weeks | 81 | Female Healthy Age: 70.6 ± 4 years. BMI: 22–23 kg/m2 | 2 days/week > 40 min 7 exercises 50–70% 1RM | 22.3 g whey post RET | Both groups 1.3 ± 0.0 kg/d (1.4 ± 0.1 kg/d) | LLMM KE |
| Nabuco et al., 2018 [40] Brazil | 12 weeks | 70 | Female Healthy Age: > 60 years. BMI: 23–26.5 kg/m2 | 3 days/week 3 sets × 8–12RM 8 exercises | 27.1 g whey post RET | P: 0.94 ± 0.36 kg/d (1.49 ± 0.46 kg/d) CON: 0.95 ± 0.27 kg/d (1.0 ± 0.25 kg/d) | SMM KE |
| Rondanelli et al., 2016 [37] Italy | 12 weeks | 130 | Female and male Sarcopenic Age: 80.3 years. BMI: 23.9 kg/m2 | 5 days/week 20-min/day 12–14 Borg Rate | 22 g whey daily | P: 0.9 g/kg (unchanged) CON: 1.0 g/kg (unchanged) | FFM HG |
| Seino et al., 2018 [46] Japan | 12 weeks | 82 | Female and male Non-disabled Age: 73.5 years. BMI: 22.9 ± 2 kg/m2 | 2 days/week 2 sets × 20 reps whole body somewhat hard | 10.5 g milk protein daily | P: 1.39 ± 0.36 kg/d (1.53 ± 0.33 kg/d) CON: 1.28 ± 0.26 kg/d (1.31 ± 0.26 kg/d) | LBM KE |
| Sugihara Junior et al., 2018 [41] Brazil | 12 weeks | 31 | Female Age: 67.4 ± 4.0 years. BMI: 25.5 ± 2.4 kg/m2 | 3 days/week 3 sets × 8–12RM 8 exercises | 35 g whey post RET | P: 0.85 ± 0.1 kg/d (1.4 ± 0.1 kg/d) CON: 0.81 ± 0.1 kg/d (0.87 ± 0.1 kg/d) | SMM KE |
| Thomson et al., 2016 [44] Australia | 12 weeks | 125 | Female and male Healthy Age: 61.5 ± 7.4 years. BMI: 27.6 ± 3.6 kg/m2 | 3 days/week 3 sets × 8–12 reps 5 exercises 8 RM | 27 g dairy protein spread to each main meal or post RET | P: 1.06 ± 0.10 kg/d (1.42 ± 0.14 kg/d) CON: 1.10 ± 0.10 kg/d | LBM KE |
| Tieland et al., 2012 [31] Netherlands | 24 weeks | 62 | Female and male Prefrailty and frailty Age: 78 ± 1 years. | 2 days/week 3–4 sets × 15–20 reps 6 exercises 50–75% 1RM | 30 g milk protein (15 g at breakfast and lunch) | P: 1.0 kg/d (1.3 kg/d) CON: 1.0 kg/d | LBM KE |
| Verdijk et al., 2009 [29] Netherlands | 12 weeks | 26 | Male Healthy Age: 72 ± 2 years. BMI: 26~27 kg/m2 | 3 days/week 4 sets × 8 reps Leg extension and leg press 75–80% 1RM | 20 g casein before and post RET | Both groups (unchanged) 1.1 ± 0.1 kg/d (unchanged) | LBM KE LP |
| Yamada et al., 2019 [47] Japan | 12 weeks | 112 | Female and male sarcopenic or dynapenic Age: 84.2 ± 5.5 years. BMI: 22 kg/m2 | 2 days/week 7 exercises 3 sets × 20 reps | 10 g whey protein, daily | N/A | AMM KE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, L.-P.; Condello, G.; Kuo, C.-H. Effects of Milk Protein in Resistance Training-Induced Lean Mass Gains for Older Adults Aged ≥ 60 y: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2815. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082815
Huang L-P, Condello G, Kuo C-H. Effects of Milk Protein in Resistance Training-Induced Lean Mass Gains for Older Adults Aged ≥ 60 y: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(8):2815. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082815
Chicago/Turabian StyleHuang, Ling-Pi, Giancarlo Condello, and Chia-Hua Kuo. 2021. "Effects of Milk Protein in Resistance Training-Induced Lean Mass Gains for Older Adults Aged ≥ 60 y: A Systematic Review and Meta-Analysis" Nutrients 13, no. 8: 2815. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082815