
Extensive Study of Breast Milk and Infant Growth: Protocol of the Cambridge Baby Growth and Breastfeeding Study (CBGS-BF)

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
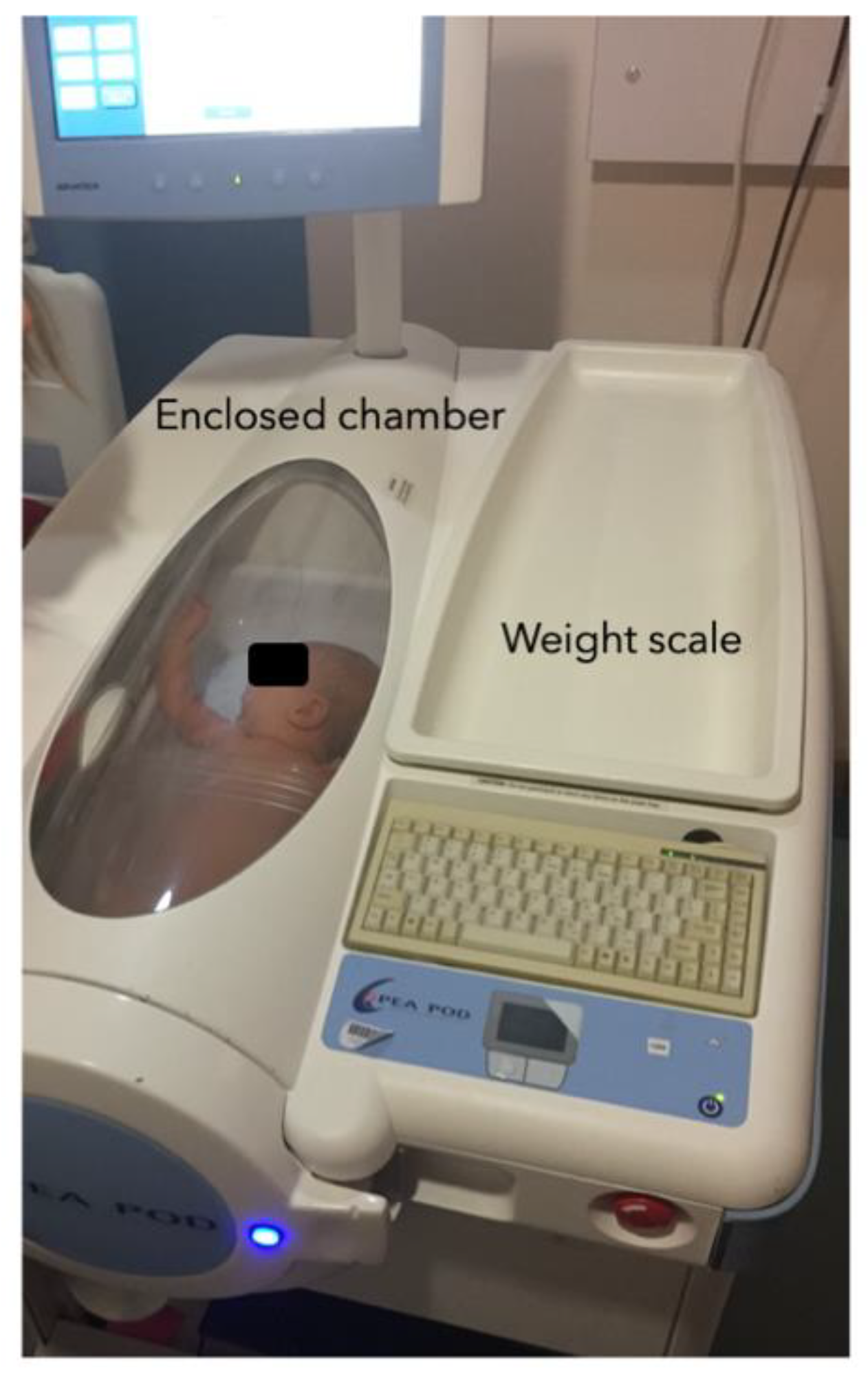
2.1. Growth and Adiposity Measurement
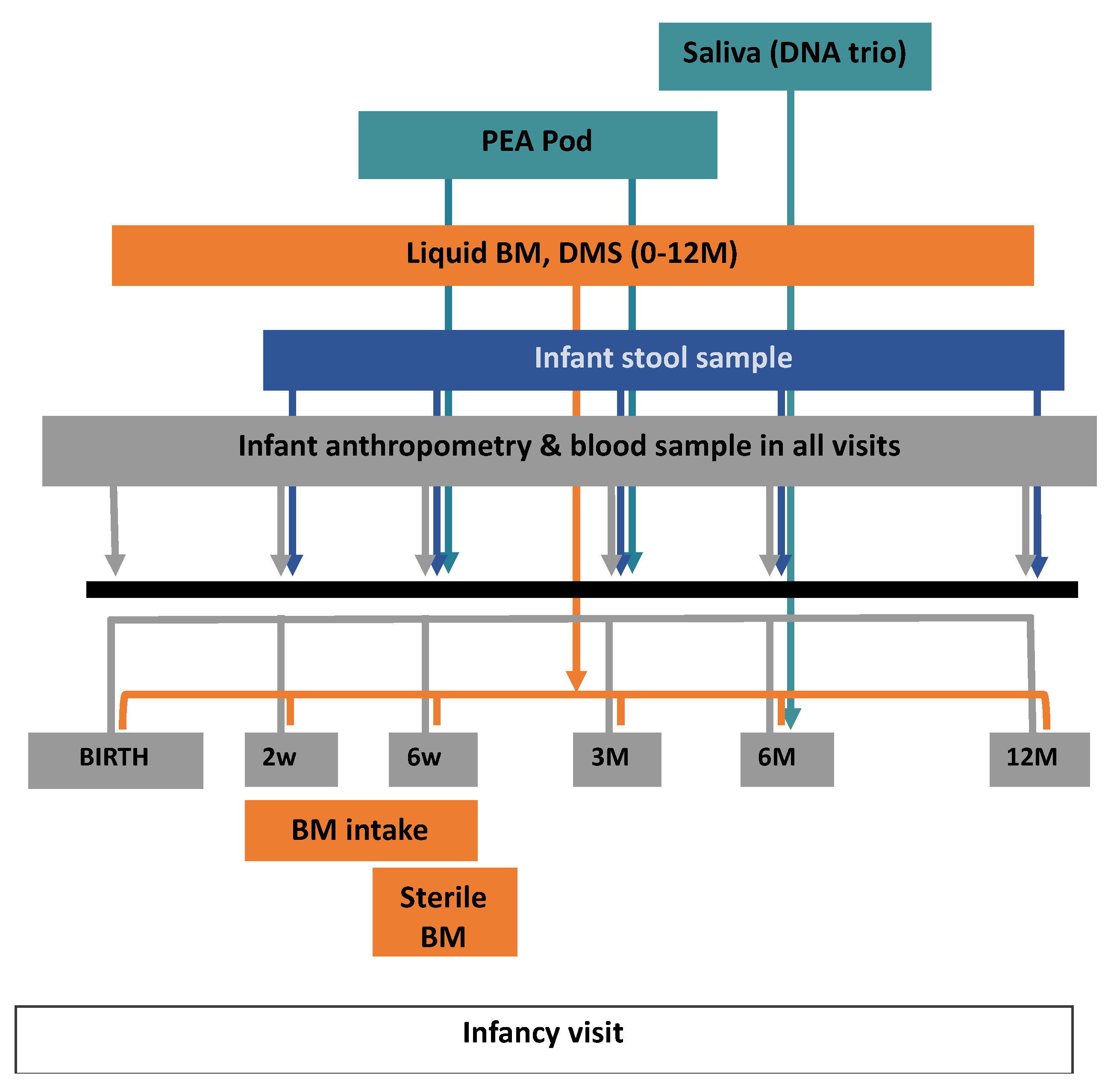
2.2. Biological Sample Collection
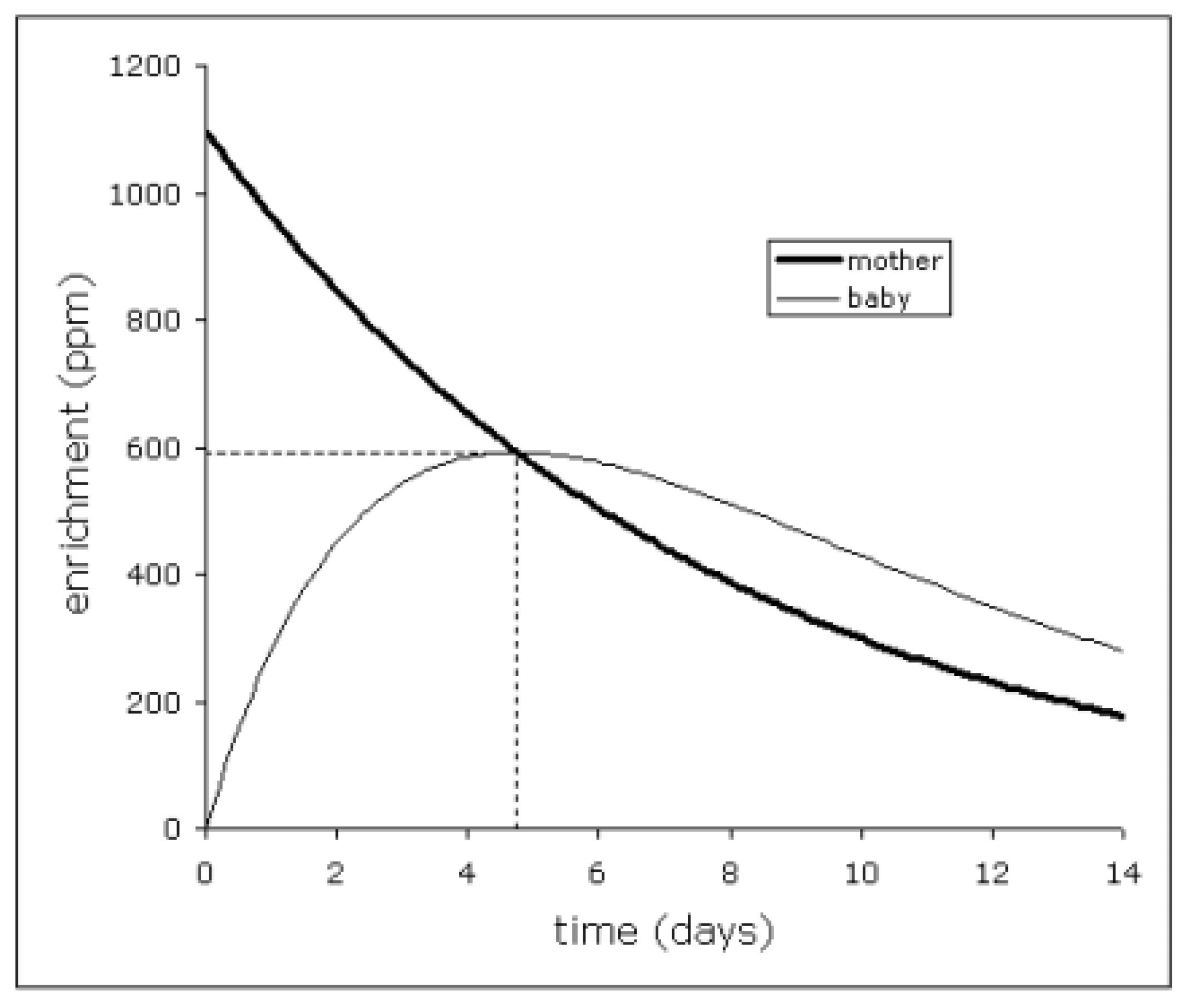
2.3. BM Intake Volume Measurement
2.4. BM Macronutrient and Butyrate Analyses
2.5. Human Milk Oligosaccharides Measurement
2.6. Fucosyltransferase 2 (FUT2) Genotyping Study
2.7. Microbiota Analysis
3. Results
3.1. The Relationship between Exclusive Breastfeeding and Infant Growth
3.2. BM Intake Volume, BM Macronutrient Composition, and Infant Growth
3.3. Factors Influencing HMOs Abundance and Its Relation to Infant Growth
3.4. Infant Gut and BM Microbiota
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prentice, P.; Acerini, C.L.; Eleftheriou, A.; Hughes, I.A.; Ong, K.K.; Dunger, D.B. Cohort profile: The Cambridge Baby Growth Study (CBGS). Int. J. Epidemiol. 2016, 45, 35. [Google Scholar] [CrossRef]
- Petry, C.J.; Sanz Marcos, N.; Pimentel, G.; Hayes, M.G.; Nodzenski, M.; Scholtens, D.M.; Hughes, I.A.; Acerini, C.L.; Ong, K.K.; Lowe, W.L.; et al. Associations between Fetal Imprinted Genes and Maternal Blood Pressure in Pregnancy. Hypertension 2016, 68, 1459–1466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petry, C.; Mooslehner, K.; Prentice, P.; Hayes, M.; Nodzenski, M.; Scholtens, D.; Hughes, I.; Acerini, C.; Ong, K.; Lowe, W.; et al. Associations between a fetal imprinted gene allele score and late pregnancy maternal glucose concentrations. Diabetes Metab. 2017, 43, 323–331. [Google Scholar] [CrossRef]
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; van Tol, E.A.F.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast milk nutrient content and infancy growth. Acta Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prentice, P.M.; Schoemaker, M.H.; Vervoort, J.; Hettinga, K.; Lambers, T.T.; van Tol, E.A.F.; Acerini, C.L.; Olga, L.; Petry, C.J.; Hughes, I.A.; et al. Human Milk Short-Chain Fatty Acid Composition is Associated with Adiposity Outcomes in Infants. J. Nutr. 2019, 149, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Prentice, P.; Koulman, A.; Matthews, L.; Acerini, C.L.; Ong, K.K.; Dunger, D.B. Lipidomic analyses, breast- and formula-feeding, and growth in infants. J. Pediatr. 2015, 166, 276–281.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furse, S.; Snowden, S.G.; Olga, L.; Prentice, P.; Ong, K.K.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B.; Koulman, A. Evidence from 3-month-old infants shows that a combination of postnatal feeding and exposures in utero shape lipid metabolism. Sci. Rep. 2019, 9, 14321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, K.K.; Cheng, T.S.; Olga, L.; Prentice, P.M.; Petry, C.J.; Hughes, I.A.; Dunger, D.B. Which infancy growth parameters are associated with later adiposity? The Cambridge Baby Growth Study. Ann. Hum. Biol. 2020, 47, 142–149. [Google Scholar] [CrossRef]
- Prentice, P.M.; Olga, L.; Petry, C.J.; Simmons, D.; Murphy, H.R.; Hughes, I.A.; Acerini, C.L.; Ong, K.K.; Dunger, D.B. Reduced size at birth and persisting reductions in adiposity in recent, compared with earlier, cohorts of infants born to mothers with gestational diabetes mellitus. Diabetologia 2019, 62, 1977–1987. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, E.E. Growth of Breast-Fed and Formula-Fed Infants. Nestlé Nutr. Work. Ser. Pediatr. Progr. 2006, 58, 51–63. [Google Scholar]
- Rzehak, P.; Oddy, W.H.; Mearin, M.; Grote, V.; Mori, T.; Szajewska, H.; Shamir, R.; Koletzko, S.; Weber, M.; Beilin, L.J.; et al. Infant feeding and growth trajectories in childhood and body composition in adulthood. Am. J. Clin. Nutr. 2017, 106, 568–580. [Google Scholar] [CrossRef] [Green Version]
- Ballard, O.; Morrow, A. Human Milk Composition: Nutrients and Bioactive Factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koletzko, B.; Demmelmair, H.; Grote, V.; Totzauer, M. Optimized protein intakes in term infants support physiological growth and promote long-term health. Semin. Perinatol. 2019, 43, 151153. [Google Scholar] [CrossRef]
- Korpela, K.; Zijlmans, M.A.C.; Kuitunen, M.; Kukkonen, K.; Savilahti, E.; Salonen, A.; de Weerth, C.; de Vos, W.M. Childhood BMI in relation to microbiota in infancy and lifetime antibiotic use. Microbiome 2017, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, W.A.; Iyengar, R.S. Breast milk, microbiota, and intestinal immune homeostasis. Pediatr. Res. 2015, 77, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Exclusive Breastfeeding for Optimal Growth, Development and Health of Infants. Available online: https://www.who.int/elena/titles/exclusive_breastfeeding/en/ (accessed on 10 August 2021).
- De Lucia Rolfe, E.; Modi, N.; Uthaya, S.; Hughes, I.A.; Dunger, D.B.; Acerini, C.; Stolk, R.P.; Ong, K.K. Ultrasound estimates of visceral and subcutaneous-abdominal adipose tissues in infancy. J. Obes. 2013, 2013, 951954. [Google Scholar] [CrossRef]
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Leinhard, O.D. Advanced body composition assessment: From body mass index to body composition profiling. J. Investig. Med. 2018, 66, 887–895. [Google Scholar] [CrossRef]
- Wells, J.C.K.; Jonsdottir, O.H.; Hibberd, P.L.; Fewtrell, M.S.; Thorsdottir, I.; Eaton, S.; Lucas, A.; Gunnlaugsson, G.; Kleinman, R.E. Randomized controlled trial of 4 compared with 6 mo of exclusive breastfeeding in Iceland: Differences in breast-milk intake by stable-isotope probe. Am. J. Clin. Nutr. 2012, 96, 73–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haisma, H.; Coward, W.A.; Albernaz, E.; Visser, G.H.; Wells, J.C.K.; Wright, A.; Victora, C.G. Breast milk and energy intake in exclusively, predominantly, and partially breast-fed infants. Eur. J. Clin. Nutr. 2003, 57, 1633–1642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durham, S.; Robinson, R.; Olga, L.; Ong, K.; Chichlowski, M.; Dunger, D.; Barile, D. A one-year study of human milk oligosaccharide profiles in the milk of healthy UK mothers and their relationship to maternal FUT2 genotype. Glycobiology 2021, cwab057. [Google Scholar] [CrossRef]
- Ferrer-Admetlla, A.; Sikora, M.; Laayouni, H.; Esteve, A.; Roubinet, F.; Blancher, A.; Calafell, F.; Bertranpetit, J.; Casals, F. A natural history of FUT2 polymorphism in humans. Mol. Biol. Evol. 2009, 26, 1993–2003. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Tao, J.; Zhou, J.; Fan, Q.; Liu, M.; Hu, Y.; Xu, Y.; Zhang, L.; Yuan, J.; Li, W.; et al. Fucosylated Human Milk Oligosaccharides and N-Glycans in the Milk of Chinese Mothers Regulate the Gut Microbiome of Their Breast-Fed Infants during Different Lactation Stages. MSystems 2018, 3, e00206-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haschke, F.; Grathwohl, D.; Detzel, P.; Steenhout, P.; Wagemans, N.; Erdmann, P. Postnatal High Protein Intake Can Contribute to Accelerated Weight Gain of Infants and Increased Obesity Risk. Nestle Nutr. Inst. Workshop Ser. 2016, 85, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, C.; Mølgaard, C.; Thomsen, B.L.; Juul, A.; Michaelsen, K.F. Protein intake at 9 mo of age is associated with body size but not with body fat in 10-y-old Danish children. Am. J. Clin. Nutr. 2004, 79, 494–501. [Google Scholar] [CrossRef]
- Desclée de Maredsous, C.; Oozeer, R.; Barbillon, P.; Mary-Huard, T.; Delteil, C.; Blachier, F.; Tomé, D.; van der Beek, E.M.; Davila, A.-M. High-Protein Exposure during Gestation or Lactation or after Weaning Has a Period-Specific Signature on Rat Pup Weight, Adiposity, Food Intake, and Glucose Homeostasis up to 6 Weeks of Age. J. Nutr. 2016, 146, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Azad, M.B.; Robertson, B.; Atakora, F.; Becker, A.B.; Subbarao, P.; Moraes, T.J.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; et al. Human Milk Oligosaccharide Concentrations Are Associated with Multiple Fixed and Modifiable Maternal Characteristics, Environmental Factors, and Feeding Practices. J. Nutr. 2018, 148, 1733–1742. [Google Scholar] [CrossRef]
- Sprenger, N.; Lee, L.Y.; De Castro, C.A.; Steenhout, P.; Thakkar, S.K. Longitudinal change of selected human milk oligosaccharides and association to infants’ growth, an observatory, single center, longitudinal cohort study. PLoS ONE 2017, 12, e0171814. [Google Scholar] [CrossRef] [Green Version]
- Sprenger, N.; Binia, A.; Austin, S. Human Milk Oligosaccharides: Factors Affecting Their Composition and Their Physiological Significance. Nestle Nutr. Inst. Workshop Ser. 2019, 90, 43–56. [Google Scholar] [CrossRef]
- Olga, L.; van Beijsterveldt, I.A.L.P.; Hughes, I.A.; Dunger, D.B.; Ong, K.K.; Hokken-Koelega, A.C.S.; De Lucia Rolfe, E. Anthropometry-based prediction of body composition in early infancy compared to air-displacement plethysmography. Pediatr. Obes. 2021, e12818. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Birth | 2w | 6w | 3M | 6M | 12M | 24M | 36M | |
|---|---|---|---|---|---|---|---|---|
| Consent and recruitment | + | |||||||
| Collection of perinatal questionnaire and parental demographics | + | |||||||
| Infant’s anthropometry and body composition | ||||||||
| Weight, length, head circumference, waist circumference | + | + | + | + | + | + | + | + |
| Skinfold thicknesses | + | + | + | + | + | + | + | |
| Abdominal ultrasound | + | + | + | + | + | |||
| ADP-Pea Pod | + | + | ||||||
| Infancy questionnaires | ||||||||
| Allergy, infection/antibiotics exposure, probiotic exposure, feeding history | + | + | + | + | + | + | ||
| Food diary | + | + | + | + | ||||
| Biological samples | ||||||||
| Infant’s stool sample for gut microbiota | + | + | + | + | + | |||
| Sterile collection of BM for milk microbiota | + | |||||||
| Other (non-sterile collection of) BM liquid sample and DMS | + | + | + | + | + | + | ||
| Mother’s and infant’s urine for BM intake volume measurement | + | |||||||
| (4–6 w) | ||||||||
| Infant’s blood sample (DBS and small amount of plasma) | + | + | + | + | + | + | ||
| Parents’ and infant’s saliva (DNA trio) | + | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olga, L.; Petry, C.J.; van Diepen, J.A.; Prentice, P.M.; Hughes, I.A.; Vervoort, J.; Boekhorst, J.; Chichlowski, M.; Gross, G.; Dunger, D.B.; et al. Extensive Study of Breast Milk and Infant Growth: Protocol of the Cambridge Baby Growth and Breastfeeding Study (CBGS-BF). Nutrients 2021, 13, 2879. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082879
Olga L, Petry CJ, van Diepen JA, Prentice PM, Hughes IA, Vervoort J, Boekhorst J, Chichlowski M, Gross G, Dunger DB, et al. Extensive Study of Breast Milk and Infant Growth: Protocol of the Cambridge Baby Growth and Breastfeeding Study (CBGS-BF). Nutrients. 2021; 13(8):2879. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082879
Chicago/Turabian StyleOlga, Laurentya, Clive J. Petry, Janna A. van Diepen, Philippa M. Prentice, Ieuan A. Hughes, Jacques Vervoort, Jos Boekhorst, Maciej Chichlowski, Gabriele Gross, David B. Dunger, and et al. 2021. "Extensive Study of Breast Milk and Infant Growth: Protocol of the Cambridge Baby Growth and Breastfeeding Study (CBGS-BF)" Nutrients 13, no. 8: 2879. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082879