
Implementation of the Code of Marketing of Breast-Milk Substitutes in Vietnam: Marketing Practices by the Industry and Perceptions of Caregivers and Health Workers

 ,
,  , ,
, ,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants, Sampling, and Data Collection
2.4. Variables
2.5. Data Management and Analysis
3. Results
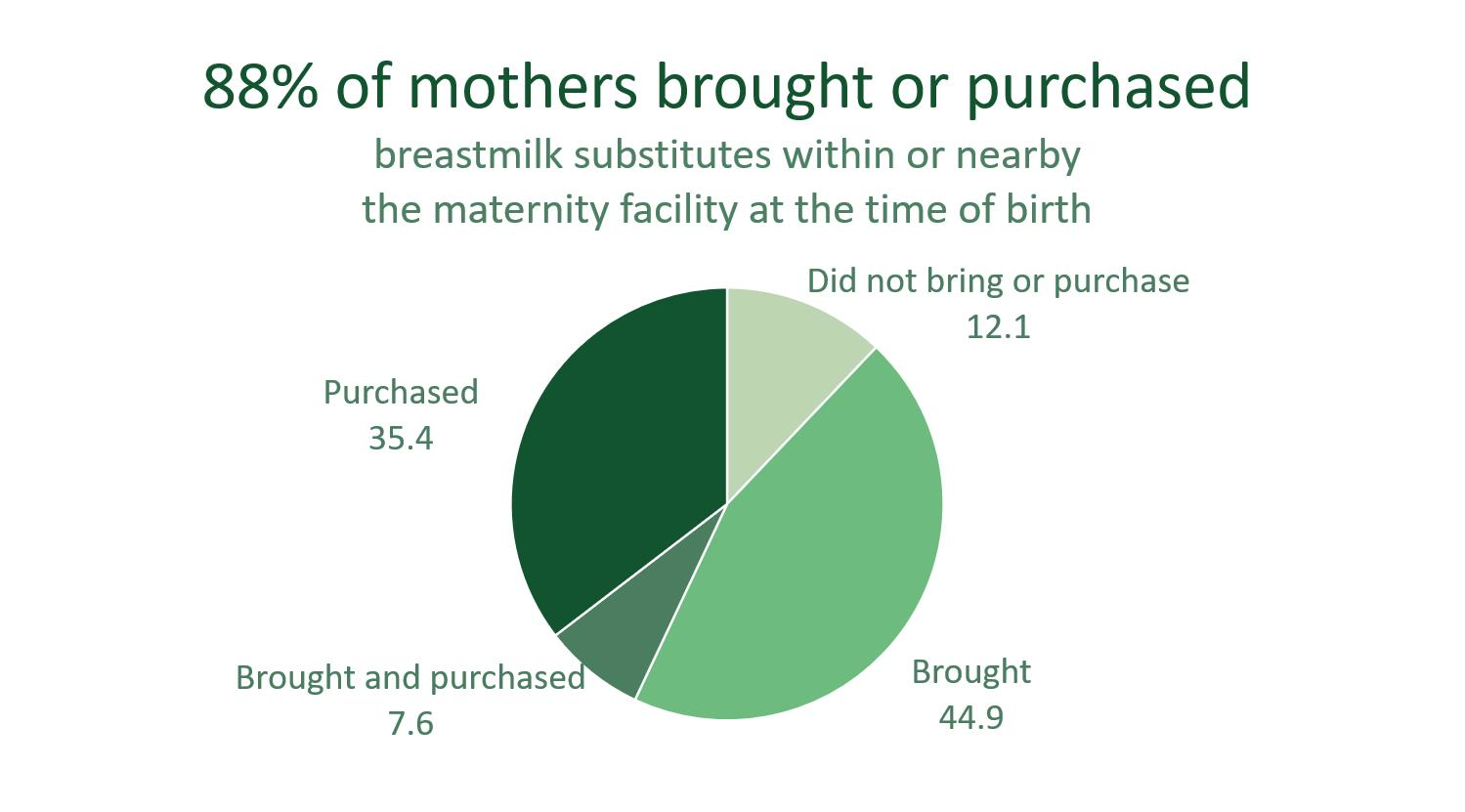
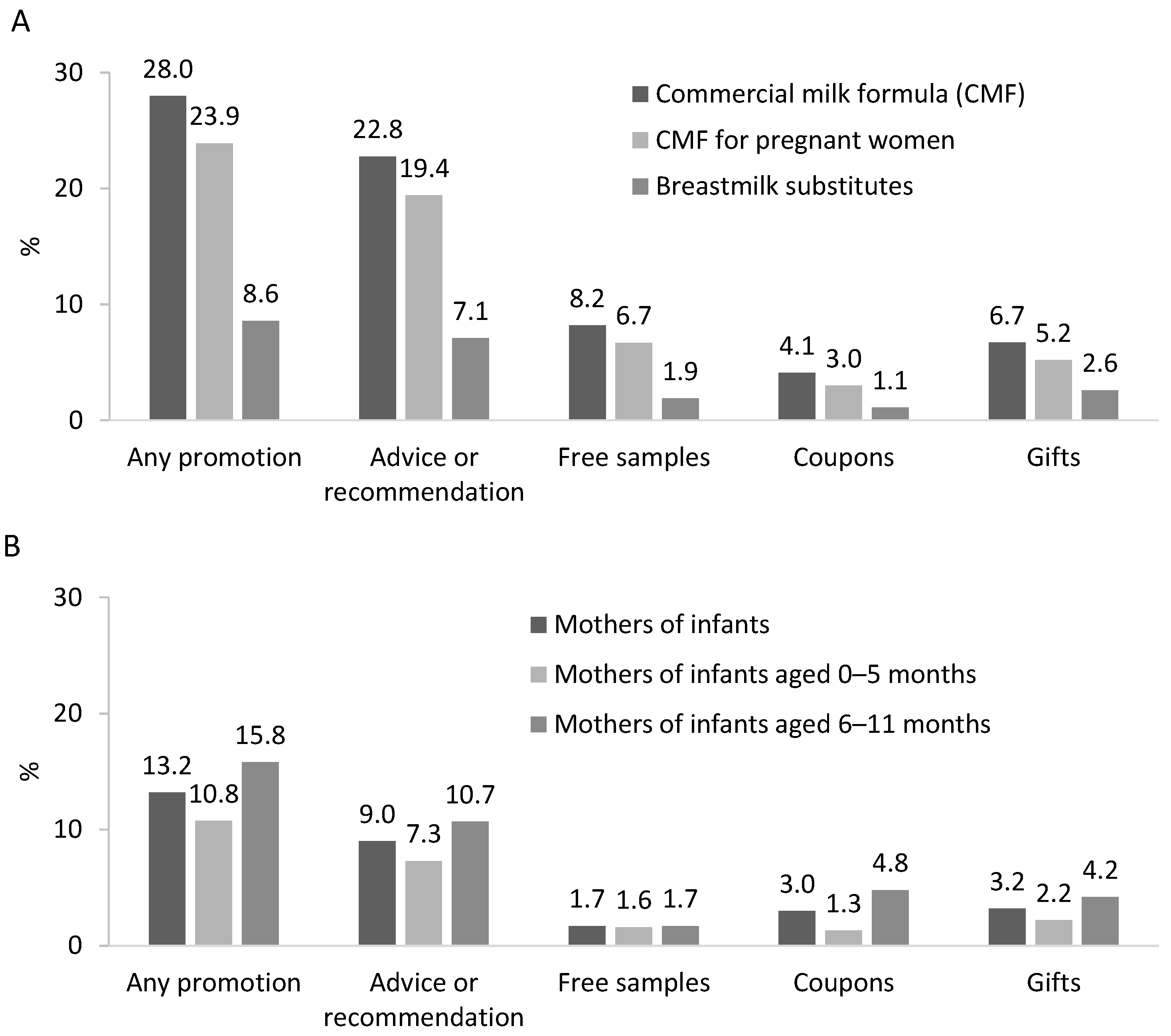
3.1. Women Are Exposed to Promotion of Commercial Milk Formula through Multiple Channels and from Pregnancy
When I went for my antenatal visit, peers instructed me about powdered milk for pregnant mothers. When approaching the due date, they recommended that I buy a can [of formula milk] to be ready in case I might not have breastmilk in the first day.Mother of 8-month-old child, HCMC.
My family bought formula milk from the pharmacist’s shop at the gate of the hospital. The doctor advised us to buy formula milk for the child as she cried a lot and I seemed not to have breastmilk in the first 2 days.Mother in postpartum period in a public hospital, Binh Duong.
3.2. Health Workers Do Not Commonly Promote BMS at Health Facilities
The hospital’s policy prohibits formula milk companies from entering the hospital and promoting sales. If any [BMS] company wants to access the hospital facility, they must first contact the hospital’s Department of Administration and Planning. We review all aspects before granting such permission. In general, we do not permit the sale and advertisement of formula milk.Health manager, Bac Ninh.
I bought formula at the hospital. The doctor asked me if my breastmilk had come out, then instructed me where to go and buy formula milk.Mother of 11-month-old child, Bac Ninh.
I was hospitalized in the service department and the doctor came to counsel me about breastfeeding and how to choose formula milk for bottle feeding.Mother of 5-month-old child, Binh Duong.
[Our approach entails] introducing the formula to women via the advice of health workers, and these health workers are given a high commission. Families are more likely to trust and buy the brand [if it is promoted by a health worker]. Each health worker is assigned one brand. This way, I can identify the number of sales by each health worker.Mother of 2-month-old child, Bac Ninh.
I saw one former staff of the hospital; she visited the hospital with a laptop and talked with mothers in the wards. When I asked her what she did, she said she would not have a salary if she did not meet mothers and talk about formula milk, so I hesitated to ask her to leave. It is sensitive, you know.Health staff, Bac Ninh.
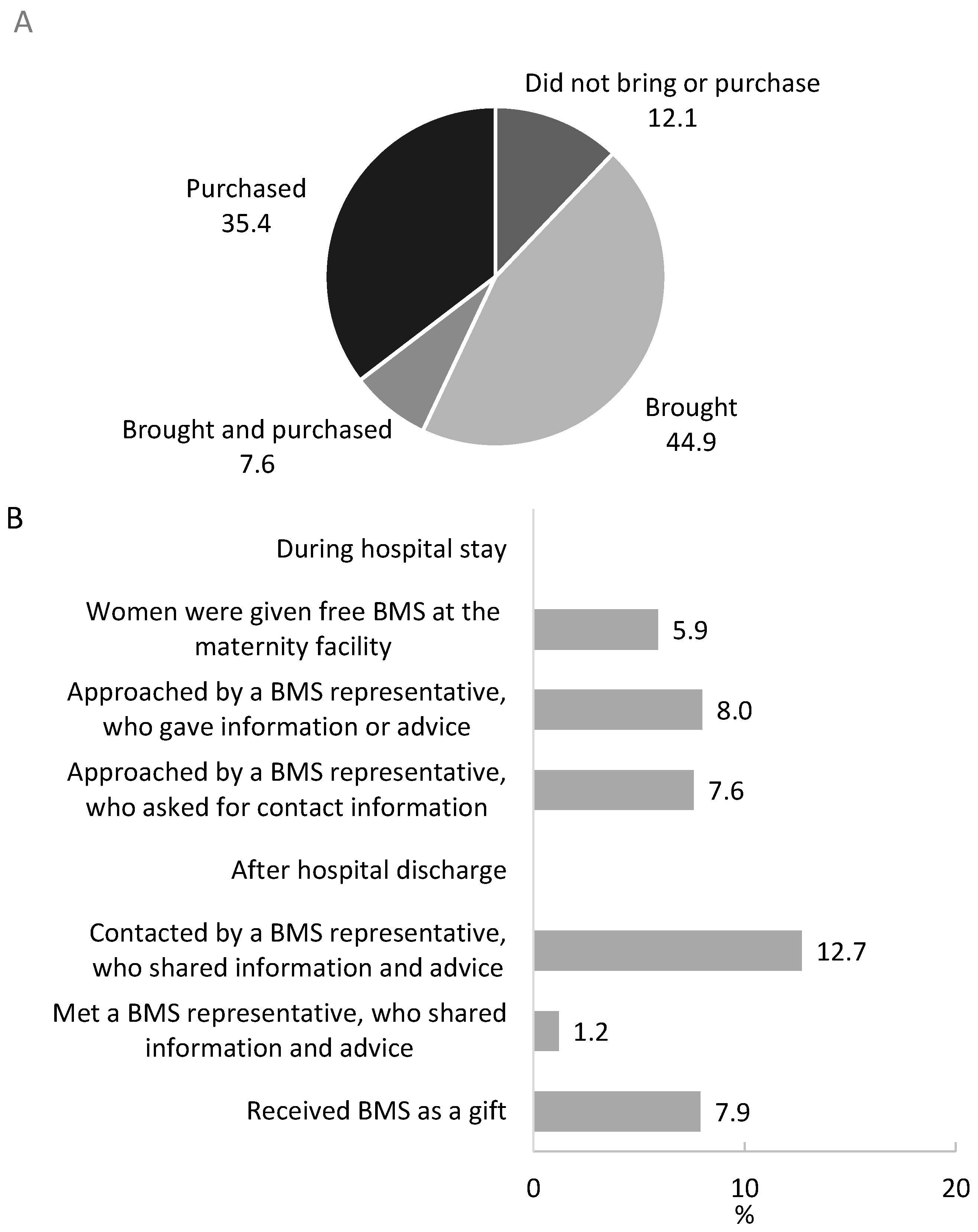
3.3. BMS Industry Representatives Promote Products within Health Facilities
When we were waiting for our antenatal care visit because they [BMS industry representatives] sat near the doctor, I thought they were health workers. There were two rooms. The room inside was the doctor’s room for antenatal examination. The room outside was for height and weight measurement, blood pressure measurement and health record filling. They sat in the room outside. They did not wear the hospital uniform but the milk company uniform.Mother of 8-month-old child, HCMC.
While I was waiting for the antenatal care visit, a staff in uniform of a milk company approached me and asked for permission to sit down and talk to me. She asked my gestation week, number of children I had, whether I used any formula milk for pregnant mother, and my intentions related to feeding my child with breastmilk or formula milk. Then she asked for my permission to take a photo of my health record and scan the bar code on the record and asked for my phone number, and then made friends with me on Zalo [a social media platform]. Several days after, she called my phone while I was at home to inform me about a promotional campaign for milk for pregnant mothers and newborn formula and shared images of toys from the promotion, which I could get if I bought a large number of cans.Mother of 9-month-old child, HCMC.
When I got my antenatal visit at the hospital … the Friso wholesale staff contacted me and advised about formula milk for child 0 to 1 year old. After my child was born, they shipped free samples of formula to my home.Mother of 5-month-old child, Binh Duong.
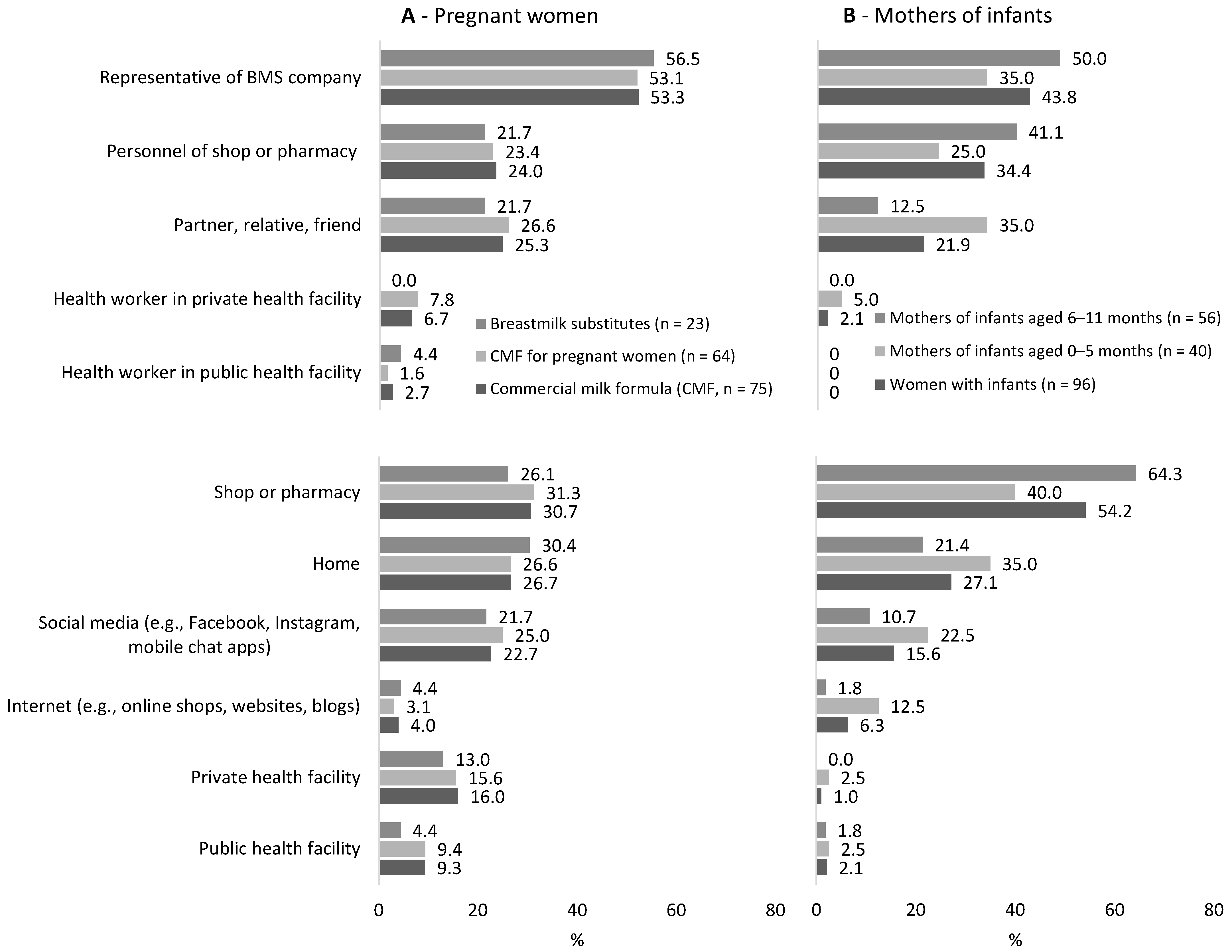
3.4. BMS Industry Promote Products on Mass and Social Media
Milk companies will invest in a province based on the expenditure of the population. Binh Duong is on top of the revenue list for Vinamilk company, so they invested their advertisement budget to our province... In the last 10 years, all well-known formula companies have advertised their products here such as Abbott, Mead Johnson, Friesland Campina, Nestlé, Nam Yang... formula milk advertisement accounted for 60–70% of milk related revenue…According to our statistics, formula milk accounted for over 50% of our total revenue from advertisement in general (80 billion VND annually at least).Key informant, Binh Duong.
I scrolled through Facebook and saw an advisement about free samples of powdered milk for pregnant mothers. I registered and got free samples from Enfa and Friso during my first pregnancy. With this pregnancy, I logged into the community groups on Facebook and heard peers advising about Japan’s powdered milk for pregnant mothers which nurture the fetus but not make the mother fat. Therefore, I looked for and bought it.Mother of 4-month-old child, Bac Ninh.
I think many mothers feed their children with formula milk due to pressure from the child’s grandparents and family members, not from the will of mothers. You will see a common situation in this province where grandparents told mothers “why is your child so tiny / small, why don’t you feed him/her with formula to grow better?”Mother of 6-month-old child, Bac Ninh.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walters, D.D.; Phan, L.T.H.; Mathisen, R. The cost of not breastfeeding: Global results from a new tool. Health Policy Plan. 2019, 34, 407–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguayo, V.M.; Morris, S.S. Introduction: Food systems for children and adolescents. Glob. Food Secur. 2020, 27, 100435. [Google Scholar] [CrossRef]
- UNICEF. Breastfeeding: A Mother’s Gift, for Every Child; UNICEF: New York, NY, USA, 2018. [Google Scholar]
- Tran, H.T.; Nguyen, T.T.; Mathisen, R. The use of human donor milk. BMJ 2020, 371, m4243. [Google Scholar] [CrossRef]
- Development Initiatives. Global Nutrition Report 2020: Action on Equity to End Malnutrition; Development Initiatives: Bristol, UK, 2020. [Google Scholar]
- WHO; UNICEF; IBFAN. Marketing of Breast-Milk Substitutes: National Implementation of the International Code. Status Report 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Piwoz, E.G.; Huffman, S.L. The Impact of Marketing of Breast-Milk Substitutes on WHO-Recommended Breastfeeding Practices. Food Nutr. Bull. 2015, 36, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Robinson, H.; Buccini, G.; Curry, L.; Perez-Escamilla, R. The World Health Organization Code and exclusive breastfeeding in China, India, and Vietnam. Matern. Child Nutr. 2019, 15, e12685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFadden, A.; Mason, F.; Baker, J.; Begin, F.; Dykes, F.; Grummer-Strawn, L.; Kenney-Muir, N.; Whitford, H.; Zehner, E.; Renfrew, M.J. Spotlight on infant formula: Coordinated global action needed. Lancet 2016, 387, 413–415. [Google Scholar] [CrossRef]
- WHO. International Code of Marketing of Breast-Milk Substitutes; WHO Code; World Health Organization: Geneva, Switzerland, 1981. [Google Scholar]
- WHO; UNICEF; IBFAN. Marketing of Breast-Milk Substitutes: National Implementation of the International Code. Status Report 2018; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Nguyen, P.H.; Menon, P.; Ruel, M.; Hajeebhoy, N. A situational review of infant and young child feeding practices and interventions in Viet Nam. Asia Pac. J. Clin. Nutr. 2011, 20, 359–374. [Google Scholar]
- Nguyen, T.T.; Darnell, A.; Weissman, A.; Cashin, J.; Withers, M.; Mathisen, R.; Lapping, K.; Mastro, T.D.; Frongillo, E.A. National nutrition strategies that focus on maternal, infant, and young child nutrition in Southeast Asia do not consistently align with regional and international recommendations. Matern. Child Nutr. 2020, 16 (Suppl. S2), e12937. [Google Scholar] [CrossRef]
- Vietnam National Assembly. Law on Advertising In 16/2012/QH13; Vietnam National Assembly: Ha Noi, Vietnam, 2012.
- Vietnam Government. Decree 100/2014/NĐ-CP on the Trading in and Use of Nutritious Products for Infants, Feeding Bottles and Teats; Vietnam Government: Ha Noi, Vietnam, 2014.
- UNICEF. Bottleneck Analysis of Breast-Milk Substitutes Code Monitoring and Enforcement Systems in Vietnam, Philippines, Indonesia and Cambodia; UNICEF East Asia and Pacific Region: Bangkok, Thailand, 2020. [Google Scholar]
- Baker, P.; Russ, K.; Kang, M.; Santos, T.M.; Neves, P.A.R.; Smith, J.; Kingston, G.; Mialon, M.; Lawrence, M.; Wood, B.; et al. Globalization, first-foods systems transformations and corporate power: A synthesis of literature and data on the market and political practices of the transnational baby food industry. Glob. Health 2021, 17, 58. [Google Scholar] [CrossRef]
- Pereira, C.; Ford, R.; Feeley, A.B.; Sweet, L.; Badham, J.; Zehner, E. Cross-sectional survey shows that follow-up formula and growing-up milks are labelled similarly to infant formula in four low and middle income countries. Matern. Child Nutr. 2016, 12 (Suppl. S2), 91–105. [Google Scholar] [CrossRef]
- WHO; UNICEF. WHO/UNICEF Information Note: Cross-Promotion of Infant Formula and Toddler Milks; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Berry, N.J.; Jones, S.C.; Iverson, D. Circumventing the WHO Code? An observational study. Arch. Dis. Child. 2012, 97, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, N.J.; Jones, S.; Iverson, D. It’s all formula to me: Women’s understandings of toddler milk ads. Breastfeed. Rev. Prof. Publ. Nurs. Mothers’ Assoc. Aust. 2010, 18, 21–30. [Google Scholar]
- Hastings, G.; Angus, K.; Eadie, D.; Hunt, K. Selling second best: How infant formula marketing works. Glob. Health 2020, 16, 77. [Google Scholar] [CrossRef]
- Vietnam Ministry of Health. National Guideline on Nutrition for Pregnant Women and Lactating Mothers In 776/QĐ-BYT; Vietnam Ministry of Health: Ha Noi, Vietnam, 2017.
- Magnant, C. The Nutritional Market for Pregnant and Breastfeeding Women: What Opportunities Are There for Dairy Ingredients? Lactalis Ingredients: Bourgbarré, France. 2021. Available online: https://www.lactalisingredients.com/news/blog/the-nutritional-market-for-pregnant-and-breastfeeding-women-what-opportunities-are-there-for-dairy-ingredients/ (accessed on 15 June 2021).
- Nguyen, T.T.; Weissman, A.; Cashin, J.; Ha, T.T.; Zambrano, P.; Mathisen, R. Assessing the Effectiveness of Policies Relating to Breastfeeding Promotion, Protection, and Support in Southeast Asia: Protocol for a Mixed-method Study. JMIR Res. Protoc. 2020, 9, e21286. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. The State of the World’s Children 2019: Children, Food and Nutrition: Growing Well in a Changing World; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- General Statistics Office of Vietnam. Statistical Yearbook of Vietnam; General Statistics Office of Vietnam: Hanoi, Vietnam, 2019; Volume 2019.
- WHO; UNICEF. NetCode Toolkit. Monitoring the Marketing of Breast-Milk Substitutes: Protocol for Periodic Assessments; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- UNICEF; WHO. Compendium of Case Studies of the Baby-Friendly Hospital Initiative; UNICEF: New York, NY, USA, 2017. [Google Scholar]
- Hernandez-Cordero, S.; Lozada-Tequeanes, A.L.; Shamah-Levy, T.; Lutter, C.; Gonzalez de Cosio, T.; Saturno-Hernandez, P.; Rivera Dommarco, J.; Grummer-Strawn, L. Violations of the International Code of Marketing of Breast-milk Substitutes in Mexico. Matern. Child Nutr. 2019, 15, e12682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pries, A.M.; Huffman, S.L.; Mengkheang, K.; Kroeun, H.; Champeny, M.; Roberts, M.; Zehner, E. Pervasive promotion of breastmilk substitutes in Phnom Penh, Cambodia, and high usage by mothers for infant and young child feeding. Matern. Child Nutr. 2016, 12 (Suppl. S2), 38–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, K.D.; Eastham, C.A.; Kasehagen, L.J.; Sandoval, A.P. Marketing infant formula through hospitals: The impact of commercial hospital discharge packs on breastfeeding. Am. J. Public Health 2008, 98, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Vietnam Ministry of Health. National Hospital Standards and Accreditation. In 6858/QĐ-BYT; Vietnam Ministry of Health: Ha Noi, Vietnam, 2016. [Google Scholar]
- Vietnam Ministry of Health. Circular No. 38/2016/TT-BYT: Providing for Measures for Encouraging the Breastfeeding at Health Facilities; Vietnam Ministry of Health: Ha Noi, Vietnam, 2016.
- Vietnam Ministry of Health. Decision: On Approval of the Document “Centers of Excellence for Breastfeeding Assessment Criteria and Designation Mechanism”; Vietnam Ministry of Health: Ha Noi, Vietnam, 2019.
- Ching, C.; Zambrano, P.; Nguyen, T.T.; Tharaney, M.; Zafimanjaka, M.G.; Mathisen, R. Old Tricks, New Opportunities: How Companies Violate the International Code of Marketing of Breast-Milk Substitutes and Undermine Maternal and Child Health during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2381. [Google Scholar] [CrossRef]
- Pereira-Kotze, C.; Doherty, T.; Swart, E.C. Use of social media platforms by manufacturers to market breast-milk substitutes in South Africa. BMJ Glob. Health 2020, 5, e003574. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, L.; Kelly, B.; Yeatman, H.; Kariippanon, K. The Effects of Digital Marketing of Unhealthy Commodities on Young People: A Systematic Review. Nutrients 2018, 10, 148. [Google Scholar] [CrossRef] [Green Version]
- Vnetwork JSC. Vietnam Internet Statistics 2019. Available online: https://vnetwork.vn/en/news/cac-so-lieu-thong-ke-internet-viet-nam-2019 (accessed on 23 February 2020).
- Vnetwork JSC. Vietnam Internet Statistics 2020. Available online: https://vnetwork.vn/en/news/thong-ke-internet-viet-nam-2020 (accessed on 23 February 2020).
- Changing Markets Foundation. Milking It: How milk formula Companies Putting Profits before Science. 2017. Available online: https://changingmarkets.org/portfolio/milking-it/ (accessed on 15 June 2021).
- Vinje, K.H.; Phan, L.T.H.; Nguyen, T.T.; Henjum, S.; Ribe, L.O.; Mathisen, R. Media audit reveals inappropriate promotion of products under the scope of the International Code of Marketing of Breast-milk Substitutes in South-East Asia. Public Health Nutr. 2017, 20, 1333–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahams, S.W. Milk and social media: Online communities and the International Code of Marketing of Breast-milk Substitutes. J. Hum. Lact. 2012, 28, 400–406. [Google Scholar] [CrossRef]
- Furneaux, R. The Baby Brands Turning Indonesian Instagram into Free Formula Ads. Bur. Investig. Journal. 2020. Available online: https://www.thebureauinvestigates.com/stories/2020-07-30/the-baby-brands-turning-indonesian-instagram-into-free-formula-milk-ads (accessed on 15 June 2021).
- Linh, A. Stop Irrelevant ads on Google and Facebook. Available online: https://laodong.vn/kinh-te/ngan-chan-quang-cao-doc-hai-tren-google-facebook-831763.ldo (accessed on 21 May 2020).
- Bharadwaj, R. AI for Social Media Censorship—How It Works at Facebook, YouTube, and Twitter; Emerj: Boston, MA, USA, 2019. [Google Scholar]
- UN General Assembly. General Comment No. 25 (2021) on Children’s Rights in Relation to the Digitial Environment; UN: Geneva, Switzerland, 2021. [Google Scholar]
- Donnelly, A.; Snowden, H.M.; Renfrew, M.J.; Woolridge, M.W. Commercial hospital discharge packs for breastfeeding women. Cochrane Database Syst. Rev. 2000. [Google Scholar] [CrossRef]
- Sobel, H.L.; Iellamo, A.; Raya, R.R.; Padilla, A.A.; Olive, J.M.; Nyunt, U.S. Is unimpeded marketing for breast milk substitutes responsible for the decline in breastfeeding in the Philippines? An exploratory survey and focus group analysis. Soc. Sci. Med. 2011, 73, 1445–1448. [Google Scholar] [CrossRef]
- Tuan, N.T.; Nguyen, P.H.; Hajeebhoy, N.; Frongillo, E.A. Gaps between breastfeeding awareness and practices in Vietnamese mothers result from inadequate support in health facilities and social norms. J. Nutr. 2014, 144, 1811–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Nguyen, T.T.; Duan, Y.; Mathisen, R.; Yang, Z. Advice to use infant formula and free samples are common in both urban and rural areas in China: A cross-sectional survey. Public Health Nutr. 2021, 24, 1977–1988. [Google Scholar] [CrossRef] [PubMed]
- Zehner, E.; Champeny, M.; Huffman, S.L. Marketing and infant and young child feeding in rapidly evolving food environments. Matern. Child Nutr. 2019, 15 (Suppl. S4), e12810. [Google Scholar] [CrossRef] [PubMed]
- Pries, A.; Huffman, S.; Champeny, M. Assessment of Promotion of Foods Consumed by Infants and Young Children in Nepal: Assessment and Research on Child Feeding (ARCH); Helen Keller International: Washington, DC, USA, 2014. [Google Scholar]
- Li, Z.; Mannava, P.; Murray, J.C.S.; Sobel, H.L.; Jatobatu, A.; Calibo, A.; Tsevelmaa, B.; Saysanasongkham, B.; Ogaoga, D.; Waramin, E.J.; et al. Association between early essential newborn care and breastfeeding outcomes in eight countries in Asia and the Pacific: A cross-sectional observational-study. BMJ Glob. Health 2020, 5, e002581. [Google Scholar] [CrossRef]
- Perez-Escamilla, R.; Martinez, J.L.; Segura-Perez, S. Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: A systematic review. Matern. Child Nutr. 2016, 12, 402–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morseth, M.S.; Nguyen, T.T.; Skui, M.; Terragni, L.; Ngo, Q.V.; Vu, H.T.T.; Mathisen, R.; Henjum, S. Health staff experiences with the implementation of early essential newborn care guidelines in Da Nang municipality and Quang Nam province in Viet Nam. BMC Health Serv. Res. 2020, 20, 585. [Google Scholar] [CrossRef]
- Bich, T.H.; Hoa, D.T.; Ha, N.T.; Vui, L.T.; Nghia, D.T.; Malqvist, M. Father’s involvement and its effect on early breastfeeding practices in Viet Nam. Matern. Child Nutr. 2016, 12, 768–777. [Google Scholar] [CrossRef]
- Bohren, M.A.; Hofmeyr, G.J.; Sakala, C.; Fukuzawa, R.K.; Cuthbert, A. Continuous support for women during childbirth. Cochrane Database Syst. Rev. 2017, 7, CD003766. [Google Scholar] [CrossRef] [PubMed]
- Carlin, R.F.; Mathews, A.; Oden, R.; Moon, R.Y. The Influence of Social Networks and Norms on Breastfeeding in African American and Caucasian Mothers: A Qualitative Study. Breastfeed. Med. 2019, 14, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.H.; Frongillo, E.A.; Kim, S.S.; Zongrone, A.A.; Jilani, A.; Tran, L.M.; Sanghvi, T.; Menon, P. Information Diffusion and Social Norms Are Associated with Infant and Young Child Feeding Practices in Bangladesh. J. Nutr. 2019, 149, 2034–2045. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.H.; Kim, S.S.; Nguyen, T.T.; Hajeebhoy, N.; Tran, L.M.; Alayon, S.; Ruel, M.T.; Rawat, R.; Frongillo, E.A.; Menon, P. Exposure to mass media and interpersonal counseling has additive effects on exclusive breastfeeding and its psychosocial determinants among Vietnamese mothers. Matern. Child Nutr. 2016, 12, 713–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.T.; Alayon, S.; Jimerson, A.; Naugle, D.; Nguyen, P.H.; Hajeebhoy, N.; Baker, J.; Baume, C.; Frongillo, E.A. The Association of a Large-Scale Television Campaign With Exclusive Breastfeeding Prevalence in Vietnam. Am. J. Public Health 2017, 107, 312–318. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Hajeebhoy, N.; Li, J.; Do, C.T.; Mathisen, R.; Frongillo, E.A. Community support model on breastfeeding and complementary feeding practices in remote areas in Vietnam: Implementation, cost, and effectiveness. Int. J. Equity Health 2021, 20, 121. [Google Scholar] [CrossRef]
- WHO; UNICEF. WHO/UNICEF meeting on infant and young child feeding. J. Nurse Midwifery 1980, 25, 31–39. [Google Scholar] [CrossRef]
- Mansen, K.; Nguyen, T.T.; Nguyen, N.Q.; Do, C.T.; Tran, H.T.; Nguyen, N.T.; Mathisen, R.; Nguyen, V.D.; Ngo, Y.T.K.; Israel-Ballard, K. Strengthening Newborn Nutrition Through Establishment of the First Human Milk Bank in Vietnam. J. Hum. Lact. 2021, 37, 76–86. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pregnant Women (n = 268) | Mothers of Infants Aged 0–11 Months | |||
|---|---|---|---|---|
| Total (n = 726) | 0–5 Months (n = 372) | 6–11 Months (n = 354) | ||
| Ethnicity, majority Kinh | 93.3 | 95.3 | 95.4 | 95.2 |
| Age (Mean ± SD) | 29.3 ± 5.9 | 29.7 ± 5.5 | 29.5 ± 5.5 | 30.0 ± 5.5 |
| Marital status, Married | 99.2 | 98.9 | 98.7 | 99.2 |
| Living with husbands, partners | 96.3 | 97.0 | 96.2 | 97.7 |
| Highest level of education | ||||
| Never attended school | 1.9 | 1.9 | 1.6 | 2.3 |
| Primary school | 15.7 | 13.4 | 13.4 | 13.3 |
| Junior secondary school | 24.2 | 21.9 | 21.2 | 22.6 |
| Secondary school | 23.1 | 26.6 | 26.9 | 26.3 |
| Diploma | 16.8 | 17.9 | 19.1 | 16.7 |
| Bachelors or higher | 18.3 | 18.3 | 17.8 | 18.8 |
| Main occupations | ||||
| Farmer | 1.1 | 1.1 | 0.8 | 1.4 |
| Blue-collar | 18.3 | 30.2 | 32.0 | 28.3 |
| White-collar | 21.6 | 23.1 | 23.1 | 23.2 |
| Small trader, self-employed, small self-owned business, services | 34.0 | 27.3 | 24.5 | 30.2 |
| Unemployed, homemaker, student | 25.0 | 18.3 | 19.6 | 16.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.; Tran, H.T.T.; Cashin, J.; Nguyen, V.D.C.; Weissman, A.; Nguyen, T.T.; Kelly, B.; Mathisen, R. Implementation of the Code of Marketing of Breast-Milk Substitutes in Vietnam: Marketing Practices by the Industry and Perceptions of Caregivers and Health Workers. Nutrients 2021, 13, 2884. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082884
Nguyen TT, Tran HTT, Cashin J, Nguyen VDC, Weissman A, Nguyen TT, Kelly B, Mathisen R. Implementation of the Code of Marketing of Breast-Milk Substitutes in Vietnam: Marketing Practices by the Industry and Perceptions of Caregivers and Health Workers. Nutrients. 2021; 13(8):2884. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082884
Chicago/Turabian StyleNguyen, Tuan T., Ha T. T. Tran, Jennifer Cashin, Van D. C. Nguyen, Amy Weissman, Trang T. Nguyen, Bridget Kelly, and Roger Mathisen. 2021. "Implementation of the Code of Marketing of Breast-Milk Substitutes in Vietnam: Marketing Practices by the Industry and Perceptions of Caregivers and Health Workers" Nutrients 13, no. 8: 2884. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082884