
Relationship between 25 Hydroxyvitamin D, Overweight/Obesity Status, Pro-Inflammatory and Oxidative Stress Markers in Patients with Type 2 Diabetes: A Simplified Empirical Path Model


 , , and
, , and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Patients
2.2. Anthropometric and Laboratory Assessment
2.3. Statistical Analysis
3. Results
3.1. General Characteristics Measured in Overweight/Obese Patients with T2DM
3.2. Association between Serum Levels of 25(OH)D and Overweight/Degree of Obesity, Metabolic, Pro-Inflammatory and Oxidative Stress Biomarkers in Patients with T2DM
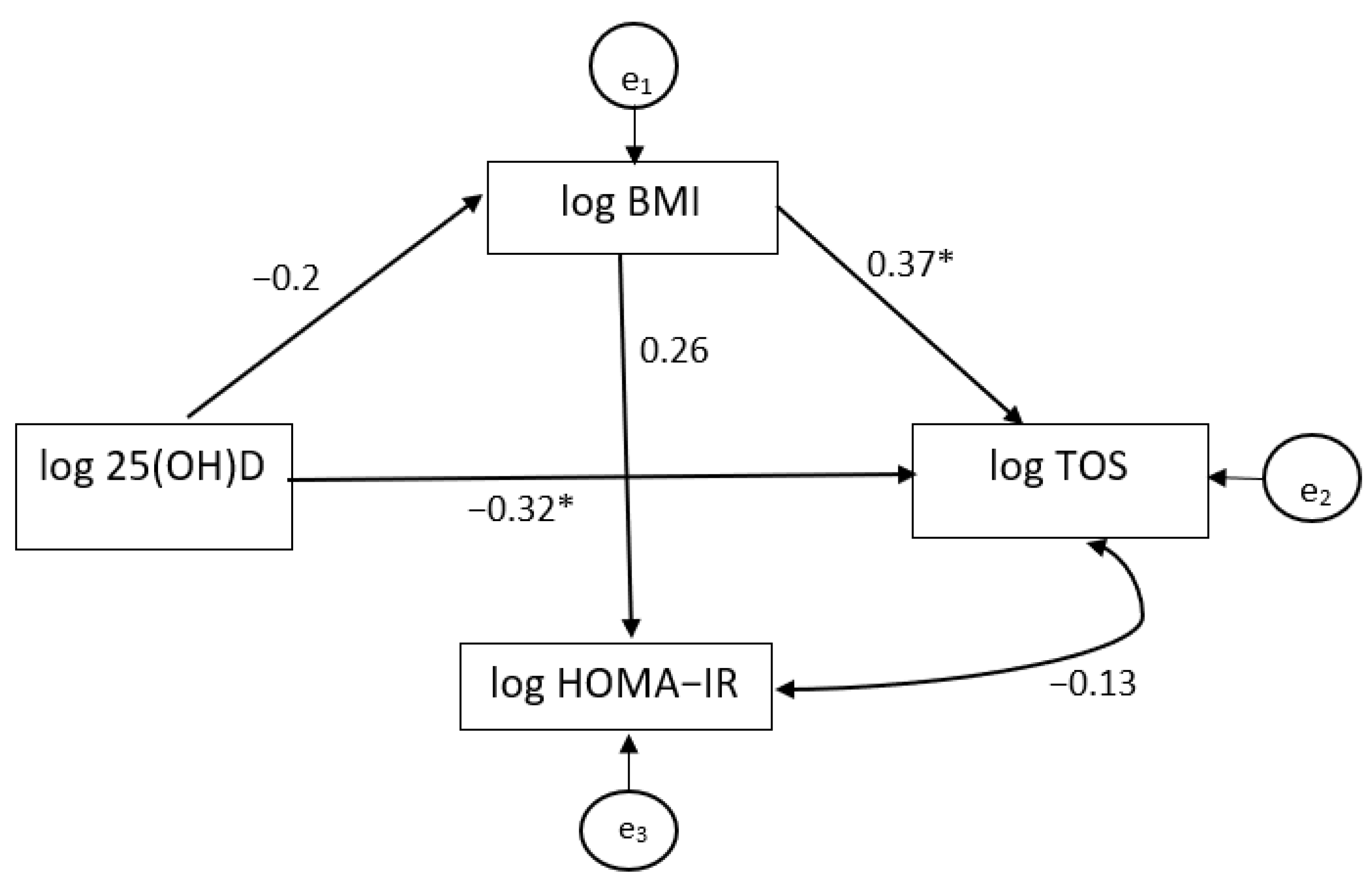
3.3. Path Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Migliaccio, S.; Di Nisio, A.; Mele, C.; Scappaticcio, L.; Savastano, S.; Colao, A. Obesity Programs of nutrition, Education, Research and Assessment (OPERA) Group. Obesity and hypovitaminosis D: Causality or casualty? Int. J. Obes. Suppl. 2019, 9, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Wimalawansa, S.J. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. J. Steroid Biochem. Mol. Biol. 2018, 175, 177–189. [Google Scholar] [CrossRef]
- Vimaleswaran, K.S.; Berry, D.J.; Lu, C.; Tikkanen, E.; Pilz, S.; Hiraki, L.T.; Cooper, J.D.; Dastani, Z.; Li, R.; Houston, D.K.; et al. Causal relationship between obesity and vitamin D status: Bi-directional Mendelian randomization analysis of multiple cohorts. PLoS Med. 2013, 10, e1001383. [Google Scholar] [CrossRef]
- Rontoyanni, V.G.; Avila, J.C.; Kaul, S.; Wong, R.; Veeranki, S.P. Association between obesity and serum 25(OH)D concentrations in older Mexican adults. Nutrients 2017, 9, 97. [Google Scholar] [CrossRef] [Green Version]
- Marquina, C.; Mousa, A.; Scragg, R.; de Courten, B. Vitamin D and cardiometabolic disorders: A review of current evidence, genetic determinants and pathomechanisms. Obes. Rev. 2019, 20, 262–277. [Google Scholar] [CrossRef] [PubMed]
- Al-Khalidi, B.; Kimball, S.M.; Rotondi, M.A.; Ardern, C.I. Standardized serum 25 hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in U.S. adults: A cross-sectional analysis of NHANES, 2001–2010. Nutr. J. 2017, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Caprio, M.; Infante, M.; Calanchini, M.; Mammi, C.; Fabbri, A. Vitamin D: Not just the bone. Evidence for beneficial pleiotropic extraskeletal effects. Eat. Weight Disord. 2017, 22, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Dix, C.F.; Barcley, J.L.; Wright, O.R.L. The role of vitamin D in adipogenesis. Nutr. Rev. 2018, 76, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Kjalarsdottir, L.; Tersey, S.A.; Vishwanath, M.; Chuang, J.C.; Posner, B.A.; Mirmira, R.G.; Repa, J.J. 1,25-Dihydroxyvitamin D3 enhances glucose-stimulated insulin secretion in mouse and human islets: A role for transcriptional regulation of voltage-gated calcium channels by the vitamin D receptor. J. Steroid Biochem. Mol. Biol. 2019, 185, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhangi, M.A.; Mesgari-Abbasi, M.; Hajiluian, G.; Nameni, G.; Shahabi, P. Adipose tissue inflammation and oxidative stress: The ameliorative effects of vitamin D. Inflammation 2017, 40, 1688–1697. [Google Scholar] [CrossRef]
- Pajor, I.S.; Sliwinska, A. Analysis of association between vitamin D deficiency and insulin resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef] [Green Version]
- De Pergola, G.; Martino, T.; Zupo, R.; Caccavo, D.; Pecorella, C.; Paradiso, S.; Silvestris, F.; Triggiani, V. 25 Hydroxyvitamin D levels are negatively and independently associated with fat mass in a cohort of healthy overweight and obese subjects. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 838–844. [Google Scholar] [CrossRef]
- Kocot, J.; Dziemidok, P.; Kiełczykowska, M.; Kurzepa, J.; Szcześniak, G.; Musik, I. Is there any relationship between plasma 25-Hydroxyvitamin D₃, adipokine profiles and excessive body weight in type 2 diabetic patients? Int. J. Environ. Res. Public Health 2017, 15, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rafiq, S.; Jeppesen, P.B. Body mass index, vitamin D, and type 2 diabetes: A systematic review and meta-analysis. Nutrients 2018, 10, 1182. [Google Scholar] [CrossRef] [Green Version]
- Greco, E.A.; Lenzi, A.; Migliaccio, S. Role of Hypovitaminosis D in the pathogenesis of obesity-induced insulin resistance. Nutrients 2019, 11, 1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscogiuri, G.; Sorice, G.P.; Prioletta, A.; Policola, C.; Della Casa, S.; Pontecorvi, A.; Giaccari, A. 25-Hydroxyvitamin D concentration correlates with insulin sensitivity and BMI in obesity. Obesity 2010, 18, 1906–1910. [Google Scholar] [CrossRef]
- Clemente-Postigo, M.; Munoz-Garach, A.; Serrano, M.; Garrido-Sanchez, L.; Bernal-Lopez, M.R.; Fernandez-Garcıa, D.; Moreno-Santos, I.; Garriga, N.; Castellano-Castillo, D.; Camargo, A.; et al. Serum 25-hydroxyvitamin D and adipose tissue vitamin D receptor gene expression: Relationship with obesity and type 2 diabetes. J. Clin. Endocrinol. Metab. 2015, 100, E591–E595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manco, M.; Calvani, M.; Nanni, G.; Greco, A.V.; Iaconelli, A.; Gasbarrini, G.; Castagneto, M.; Mingrone, G. Low 25-hydroxyvitamin D does not affect insulin sensitivity in obesity after bariatric surgery. Obes. Res. 2005, 13, 1692–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Masri, M.; Romain, A.J.; Boegner, C.; Maimoun, L.; MarianoGoulart, D.; Attalin, V.; Leprieur, E.; Picandet, M.; Avignon, A.; Sultan, A. Vitamin D status is not related to insulin resistance in different phenotypes of moderate obesity. Appl. Physiol. Nutr. Metab. 2017, 42, 438–442. [Google Scholar] [CrossRef]
- Boonchaya-anant, P.; Holick, M.F.; Apovian, C.M. Serum 25-hydroxyvitamin D levels and metabolic health status in extremely obese individuals. Obesity 2014, 22, 2539–2543. [Google Scholar] [CrossRef] [Green Version]
- ter Horst, K.W.; Versteeg, R.I.; Gilijamse, P.W.; Ackermans, M.T.; Heijboer, A.C.; Romijn, J.A.; la Fleur, S.E.; Trinko, R.; DiLeone, R.J.; Serlie, M.J. The vitamin D metabolites 25(OH)D and 1,25(OH)2D are not related to either glucose metabolism or insulin action in obese women. Diabetes Metab. 2016, 42, 416–423. [Google Scholar] [CrossRef]
- Wright, C.S.; Weinheimer-Haus, E.M.; Fleet, J.C.; Peacock, M.; Campbell, W.W. The Apparent Relation between Plasma 25-Hydroxyvitamin D and insulin resistance is largely attributable to central adiposity in overweight and obese adults. J. Nutr. 2015, 145, 2683–2689. [Google Scholar] [CrossRef] [Green Version]
- Bellia, A.; Garcovich, C.; D’Adamo, M.; Lombardo, M.; Tesauro, M.; Donadel, G.; Gentileschi, P.; Lauro, D.; Federici, M.; Lauro, R.; et al. Serum 25-hydroxyvitamin D levels are inversely associated with systemic inflammation in severe obese subjects. Intern. Emerg. Med. 2013, 8, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Vilarrasa, N.; Vendrell, J.; Maravall, J.; Elio, I.; Solano, E.; San Jose, P.; Garcia, I.; Virgili, N.; Soler, J.; Gomez, J.M. Is plasma 25(OH) D related to adipokines, inflammatory cytokines and insulin resistance in both a healthy and morbidly obese population? Endocrine 2010, 38, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.W.; Siu, P.M.; Pang, M.Y.; Woo, J.; Collins, A.R.; Benzie, I.F.F. Vitamin D deficiency, oxidative stress and antioxidant status: Only weak association seen in the absence of advanced age, obesity or pre-existing disease. Br. J. Nutr. 2017, 118, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionica, M.; Aburel, O.M.; Vaduva, A.; Petrus, A.; Rațiu, S.; Olariu, S.; Sturza, A.; Muntean, D.M. Vitamin D alleviates oxidative stress in adipose tissue and mesenteric vessels from obese patients with subclinical inflammation. Can. J. Physiol. Pharmacol. 2020, 98, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global consensus recommendations on prevention and management of nutritional rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]
- Miranda, K.; Espey, M.G.; Wink, D.A. A rapid, simple spectrophotometric method for simultaneous detection of nitrate and nitrite. Nitric Oxide Biol. Chem. 2001, 5, 62–71. [Google Scholar] [CrossRef]
- Cătoi, A.F.; Pârvu, A.; Galea, R.F.; Pop, I.D.; Muresan, A.; Cătoi, C. Nitric oxide, oxidant status and antioxidant response in morbidly obese patients: The impact of 1-year surgical weight loss. Obes. Surg. 2013, 13, 1858–1863. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, E. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar]
- Ozcan, E. A novel automated method to measure total antioxidant response against potent free radical reactions. Clin. Biochem. 2004, 37, 112–119. [Google Scholar]
- Harma, M.; Harma, M.; Erel, O. Increased oxidative stress in patients with hydatidiform mole. Swiss Med. Wkly. 2003, 133, 563–566. [Google Scholar]
- Mattheus, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Kline, R.B. Methodology in the social sciences. In Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Muscogiuri, G.; Altieri, B.; Annweiler, C.; Balercia, G.; Pal, H.B.; Boucher, B.J.; Cannel, J.J.; Forest, C.; Grubler, M.R.; Kotsa, K.; et al. Vitamin D and chronic diseases: The current state of the art. Arch. Toxicol. 2016, 91, 97–101. [Google Scholar] [CrossRef]
- Cashman, K.D. Vitamin D deficiency: Defining, prevalence, causes, and strategies of addressing. Calcif. Tissue Int. 2020, 106, 14–29. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Earthman, C.P.; Beckman, L.M.; Masodkar, K.; Sibley, S.D. The link between obesity and low 25-hydroxyvitamin D concentrations: Considerations and implications. Int. J. Obes. 2012, 36, 387–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira-Santos, M.; Costa, P.R.; Assis, A.M.; Santos, C.A.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and metaanalysis. Ober. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Annunziata, G.; Laudisio, D.; de Alteriis, G.; Tenore, G.C.; Colao, A.; Savastano, S. A new light on vitamin D in obesity: A novel association with Trimethylamine-N-Oxide (TMAO). Nutrients 2019, 11, 1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigna, L.; Cassinelli, L.; Tirelli, A.S.; Felicetta, I.; Napolitano, F.; Tomaino, L.; Mutti, M.; Barberi, C.E.; Riboldi, L. 25(OH)D levels in relation to gender, overweight, insulin resistance, and inflammation in a cross-sectional cohort of Northern Italian workers: Evidence in support of preventive health care programs. J. Am. Coll. Nutr. 2017, 36, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Arunabh, S.; Pollack, S.; Yeh, J.; Aloia, J.F. Body fat content and 25- hydroxyvitamin D levels in healthy women. J. Clin. Endocrinol. Metab. 2003, 88, 157–161. [Google Scholar] [CrossRef]
- Mousa, A.; Naderpoor, N.; de Courten, M.P.J.; Scragg, R.; de Courten, B. 25-Hydroxyvitamin D is associated with adiposity and cardiometabolic risk factors in a predominantly vitamin D-deficient and overweight/obese but otherwise healthy cohort. J. Steroid Biochem. Mol. Biol. 2017, 173, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Piantanida, E.; Gallo, D.; Veronesi, G.; Dozio, E.; Trotti, E.; Lai, A.; Ippolito, S.; Sabatino, J.; Tanda, M.L.; Toniolo, A.; et al. Cardiometabolic healthy and unhealthy obesity: Does vitamin D play a role? Endocr. Connect. 2017, 6, 943–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savastano, S.; Barrea, L.; Savanelli, M.C.; Nappi, F.; Di Somma, C.; Orio, F.; Colao, A. Low vitamin D status and obesity: Role of nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 215–225. [Google Scholar] [CrossRef]
- Ding, C.; Parameswaran, V.; Blizzard, L.; Burgess, J.; Jones, G. Not a simple fat-soluble vitamin: Changes in serum 25-(OH)D levels are predicted by adiposity and adipocytokines in older adults. J. Intern. Med. 2010, 268, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Wamberg, L.; Kampmann, U.; Stodkilde-Jorgensen, H.; Rejnmark, L.; Pedersen, S.B.; Richelsen, B. Effects of vitamin D supplementation on body fat accumulation, inflammation, and metabolic risk factors in obese adults with low vitamin D levels- results from a randomized trial. Eur. J. Intern. Med. 2013, 24, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-hydroxyvitamin D, diabetes, and ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care 2004, 27, 2813–2818. [Google Scholar] [CrossRef] [Green Version]
- Lips, P.; Eekhoff, M.; van Schoor, N.; Oosterwerff, M.; de Jongh, R.; Krul-Poel, Y.; Simsek, S. Vitamin D and type 2 diabetes. J. Steroid Biochem. Mol. Biol. 2017, 173, 280–285. [Google Scholar] [CrossRef]
- Bellan, M.; Guzzaloni, G.; Rinaldi, M.; Merlotti, E.; Ferrari, C.; Tagliaferri, A.; Pirisi, M.; Aimaretti, G.; Scacchi, M.; Marzullo, P. Altered glucose metabolism rather than naive type 2 diabetes mellitus (T2DM) is related to vitamin D status in severe obesity. Cardiovasc. Diabetol. 2014, 13, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondia-Pons, I.; Ryan, L.; Martinez, J.A. Oxidative stress and inflammation interactions in human obesity. J. Physiol. Biochem. 2012, 68, 701–711. [Google Scholar] [CrossRef]
- Catoi, A.F.; Pârvu, A.E.; Andreicut, A.D.; Mironiuc, A.; Craciun, C.; Catoi, C.; Pop, I.D. Metabolically healthy versus unhealthy morbidly obese: Chronic inflammation, nitro-oxidative stress, and insulin resistance. Nutrients 2018, 10, 1199. [Google Scholar] [CrossRef] [Green Version]
- Wimalawansa, S.J. Vitamin D deficiency: Effects on oxidative stress, epigenetics, gene regulation, and aging. Biology 2019, 8, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landrier, J.F.; Karkeni, E.; Marcotorchino, J.; Bonnet, L.; Tourniaire, F. Vitamin D modulates adipose tissue biology: Possible consequences for obesity? Proc. Nutr. Soc. 2016, 75, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbossa, S.G.; Folli, F. Vitamin D, sub-inflammation and insulin resistance. A window on a potential role for the interaction between bone and glucose metabolism. Rev. Endocr. Metab. Disord. 2017, 18, 243–258. [Google Scholar] [CrossRef]
- Nguyen, V.T.; Li, X.; Elli, E.F.; Ayloo, S.M.; Castellanos, K.J.; Fantuzzi, G.; Freels, S.; Braunschweig, C.L. Vitamin D, inflammation, and relations to insulin resistance in premenopausal women with morbid obesity. Obesity 2015, 23, 1591–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krivošíková, Z.; Gajdoš, M.; Šebeková, K. Vitamin D levels decline with rising number of cardiometabolic risk factors in healthy adults: Association with adipokines, inflammation, oxidative stress and advanced glycation markers. PLoS ONE 2015, 10, e0131753. [Google Scholar] [CrossRef]
- Iacobellis, G. Local and systemic effects of the multifaceted epicardial adipose tissue depot. Nat. Rev. Endocrinol. 2015, 11, 363–371. [Google Scholar] [CrossRef]
- Conte, C.; Esposito, A.; De Lorenzo, R.; Di Filippo, L.; Palmisano, A.; Vignale, D.; Leone, R.; Nicoletti, V.; Ruggeri, A.; Gallone, G.; et al. Epicardial adipose tissue characteristics, obesity and clinical outcomes in COVID-19: A post-hoc analysis of a prospective cohort study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2156–2164. [Google Scholar] [CrossRef]
- Sun, X.; Zemel, M.B. 1α,25-Dihydroxyvitamin D3 Modulation of adipocyte reactive oxygen species production. Obesity 2007, 15, 1944–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codoñer-Franch, P.; Tavárez-Alonso, S.; Simó-Jordá, R.; Laporta-Martín, P.; Carratalá-Calvo, A.; Alonso-Iglesias, E. Vitamin D status is linked to biomarkers of oxidative stress, inflammation, and endothelial activation in obese children. J. Pediatr. 2012, 161, 848–854. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overweight/Obesity Status | |||||
|---|---|---|---|---|---|
| Overweight (n1 = 7) | Class I Obesity (n2 = 10) | Class II Obesity (n3 = 15) | Class III/Morbid Obesity (n4 = 15) | p-Value | |
| Age (years) (a) | 57.86 ± 2.04 | 57.80 ± 4.13 | 57.00 ± 9.09 | 55.80 ± 7.97 | 0.888 |
| BMI (kg/m2) (b) | 28.66 (27.06–28.99) | 32.31 (31.24–33.46) | 35.94 (35.56–36.62) | 44.70 (42.43–45.86) | <0.0001 *** |
| Blood glucose (mg/dL) (c) | 133.77 ± 1.19 | 127.01 ± 1.15 | 128.87 ± 1.19 | 134.53 ± 1.21 | 0.827 |
| Insulin (μIU/mL) (c) | 10.14 ± 2.10 | 20.23 ± 2.21 | 19.96 ± 1.59 | 19.34 ± 1.93 | 0.110 |
| HOMA-IR (c) | 3.35 ± 1.97 | 6.35 ± 2.39 | 6.35 ± 1.63 | 6.42 ± 2.21 | 0.195 |
| Total cholesterol (mg/dL) (c) | 148.56 ± 1.33 | 186.60 ± 1.26 | 175.02 ± 1.29 | 174.83 ± 1.37 | 0.411 |
| Tryglicerides (mg/dL) (c) | 115.57 ± 1.52 | 120.19 ± 1.51 | 121.92 ± 1.73 | 142.78 ± 1.36 | 0.637 |
| IL-6 (pg/mL) (a) | 25.00 ± 21.41 | 14.58 ± 8.77 | 21.04 ± 15.49 | 16.26 ± 8.98 | 0.468 |
| NOx (μmol/L) (a) | 50.09 ± 24.96 | 64.78 ± 18.73 | 62.96 ± 20.96 | 65.57 ± 12.55 | 0.323 |
| TOS (μmol H2O2 equiv./L) (c) | 20.88 ± 1.31 | 27.31 ± 1.50 | 28.82 ± 1.31 | 35.97 ± 1.38 | 0.006 ** |
| TAR (mmol Trolox equiv./L) (a) | 1.094 ± 0.001 | 1.093 ± 0.002 | 1.094 ± 0.002 | 1.094 ± 0.001 | 0.758 |
| OSI (c) | 19.03 ± 1.31 | 23.58 ± 1.58 | 26.02 ± 1.32 | 29.24 ± 1.46 | 0.073 |
| Serum 25(OH)D (ng/mL) | <10 ng/mL (n1 = 28) | 10–20 ng/mL (n2 = 15) | ≥20 ng/mL (n3 = 4) | p-Value |
|---|---|---|---|---|
| BMI (kg/m2) GM (95% CI) | 37.90 (35.44–40.53) | 34.85 (31.90–38.07) | 30.59 (23.04–40.60) | 0.043 * |
| HOMA-IR, GM (95% CI) | 5.73 (4.40–7.46) | 7.35 (4.91–10.99) | 2.56 (1.16–5.66) | 0.032 * |
| Total cholesterol (mg/dL), GM (95% CI) | 185.31 (168.23–204.13) | 160.44 (134.35–191.61) | 142.63 (132.48–153.57) | 0.087 |
| Tryglicerides (mg/dL), GM (95% CI) | 143.75 (125.87–164.17) | 112.50 (84.33–150.07) | 82.68 (63.61–107.46) | 0.019 * |
| IL-6 (pg/mL), ME (95% CI) | 18.06 (14.19–24.21) | 14.81 (5.96–18.18) | 8.64 (1.02–23.82) | 0.228 |
| NOx (μmol/L), AM (95% CI) | 65.60 (58.59–72.61) | 59.33 (47.74–70.91) | 49.90 (28.98–70.82) | 0.235 |
| TOS (μmol H2O2 equiv./L), GM (95% CI) | 32.33 (28.30–36.93) | 27.10 (22.62–32.48) | 18.54 (15.66–21.96) | 0.007 ** |
| TAR (mmol Trolox equiv./L), AM (95% CI) | 1.0932 (1.0909–1.0956) | 1.0936 (1.0925–1.0947) | 1.0936 (1.0931–1.0941) | 0.908 |
| OSI, GM (95% CI) | 28.49 (24.77–32.77) | 22.69 (19.09–26.97) | 16.14 (12.04–21.64) | 0.005 ** |
| Log 25(OH)D | Log BMI | Log TOS | Log HOMA-IR | |
|---|---|---|---|---|
| Log25(OH)D | 1 | |||
| logBMI | −0.23 (0.127) | 1 | ||
| logTOS | −0.41 (0.004) | 0.45 (0.0016) | 1 | |
| LogHOMA-IR | −0.02 (0.873) | 0.26 (0.078) | 0.00 (0.873) | 1 |
| Unstandardized Path Coefficient | SE | Z-Statistics | Percentile 95% CI | ||
|---|---|---|---|---|---|
| Direct effect | |||||
| log 25(OH)D → log BMI | −0.07 | 0.04 | −1.59 | 0.113 | (−0.15; 0.02) |
| log 25(OH)D → log TOS | −0.20 | 0.08 | −2.46 | 0.014 * | (−0.36; −0.03) |
| log BMI → log TOS | 0.75 | 0.27 | 2.76 | 0.006 * | (0.21; 1.29) |
| log BMI → log HOMA-IR | 1.05 | 0.56 | 1.87 | 0.061 | (−0.10; 2.14) |
| Indirect effect | |||||
| log 25(OH)D → log BMI → log TOS | −0.05 | 0.04 | −1.41 | 0.159 | (−0.13; 0.02) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cătoi, A.F.; Iancu, M.; Pârvu, A.E.; Cecan, A.D.; Bidian, C.; Chera, E.I.; Pop, I.D.; Macri, A.M. Relationship between 25 Hydroxyvitamin D, Overweight/Obesity Status, Pro-Inflammatory and Oxidative Stress Markers in Patients with Type 2 Diabetes: A Simplified Empirical Path Model. Nutrients 2021, 13, 2889. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082889
Cătoi AF, Iancu M, Pârvu AE, Cecan AD, Bidian C, Chera EI, Pop ID, Macri AM. Relationship between 25 Hydroxyvitamin D, Overweight/Obesity Status, Pro-Inflammatory and Oxidative Stress Markers in Patients with Type 2 Diabetes: A Simplified Empirical Path Model. Nutrients. 2021; 13(8):2889. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082889
Chicago/Turabian StyleCătoi, Adriana Florinela, Mihaela Iancu, Alina Elena Pârvu, Andra Diana Cecan, Cristina Bidian, Elisabeta Ioana Chera, Ioana Delia Pop, and Adrian Maximilian Macri. 2021. "Relationship between 25 Hydroxyvitamin D, Overweight/Obesity Status, Pro-Inflammatory and Oxidative Stress Markers in Patients with Type 2 Diabetes: A Simplified Empirical Path Model" Nutrients 13, no. 8: 2889. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082889