
Night Vision and Carotenoids (NVC): A Randomized Placebo Controlled Clinical Trial on Effects of Carotenoid Supplementation on Night Vision in Older Adults


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
2.2. Instrumentation
3. Statistical Analysis
4. Results
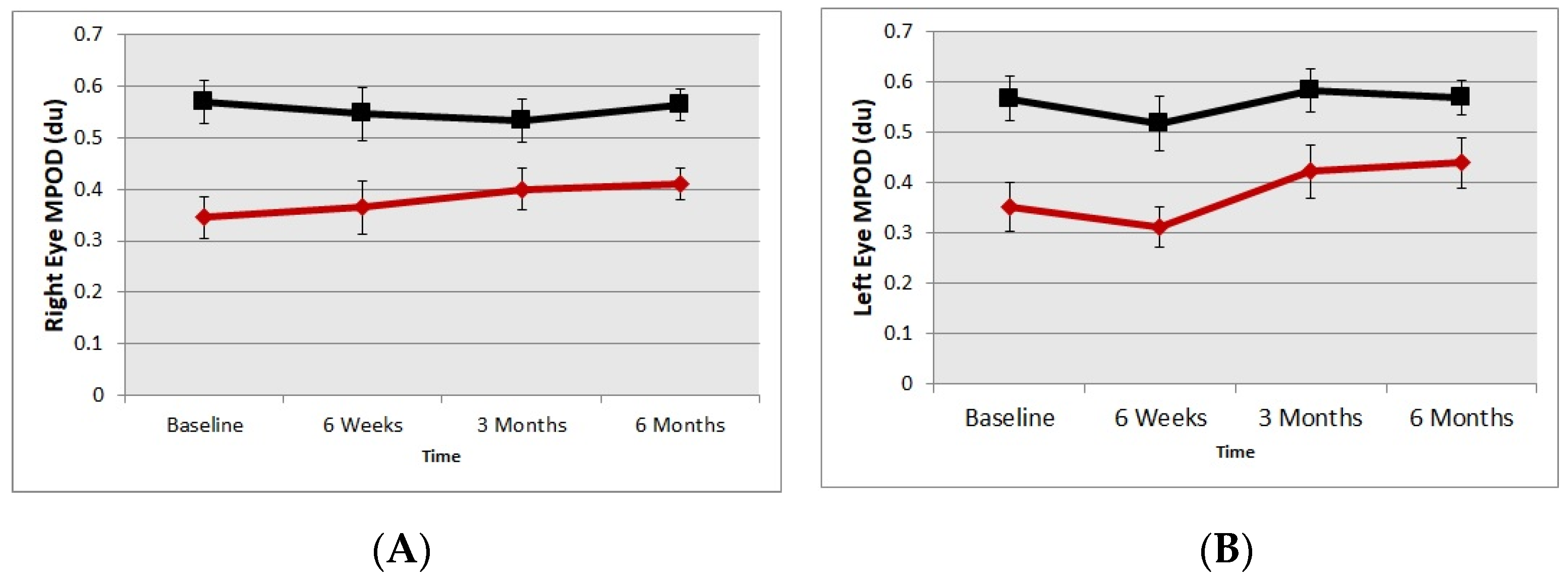
4.1. Macular Pigment Optical Density
4.2. Glare & Contrast Improvement
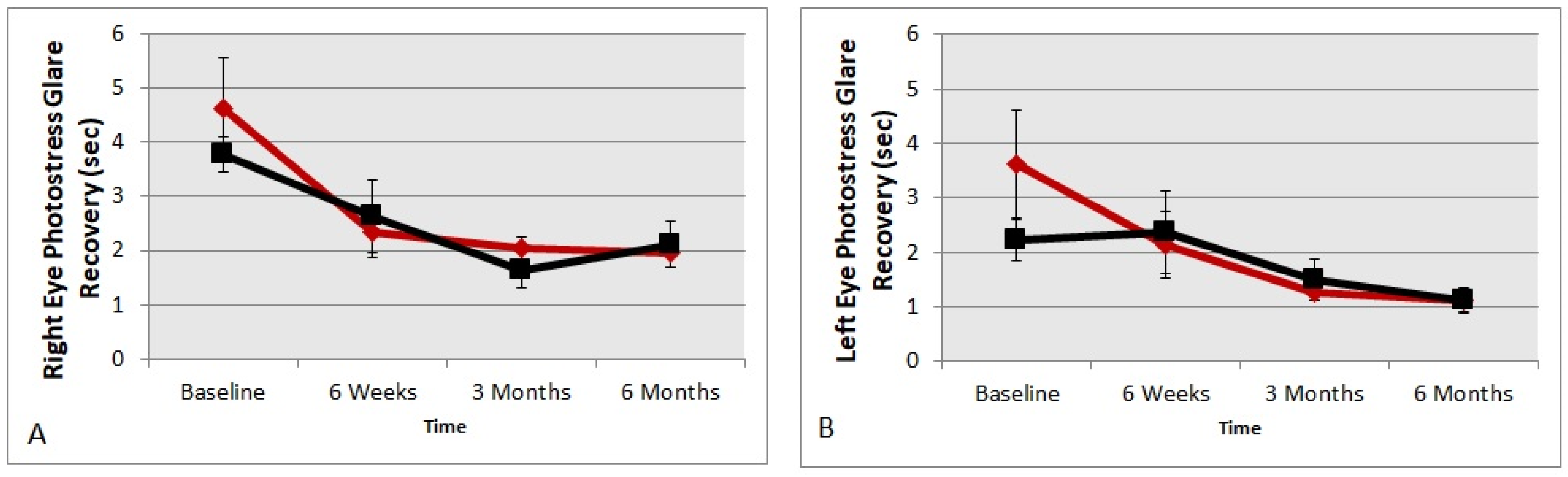
4.3. Glare Recovery Improvement
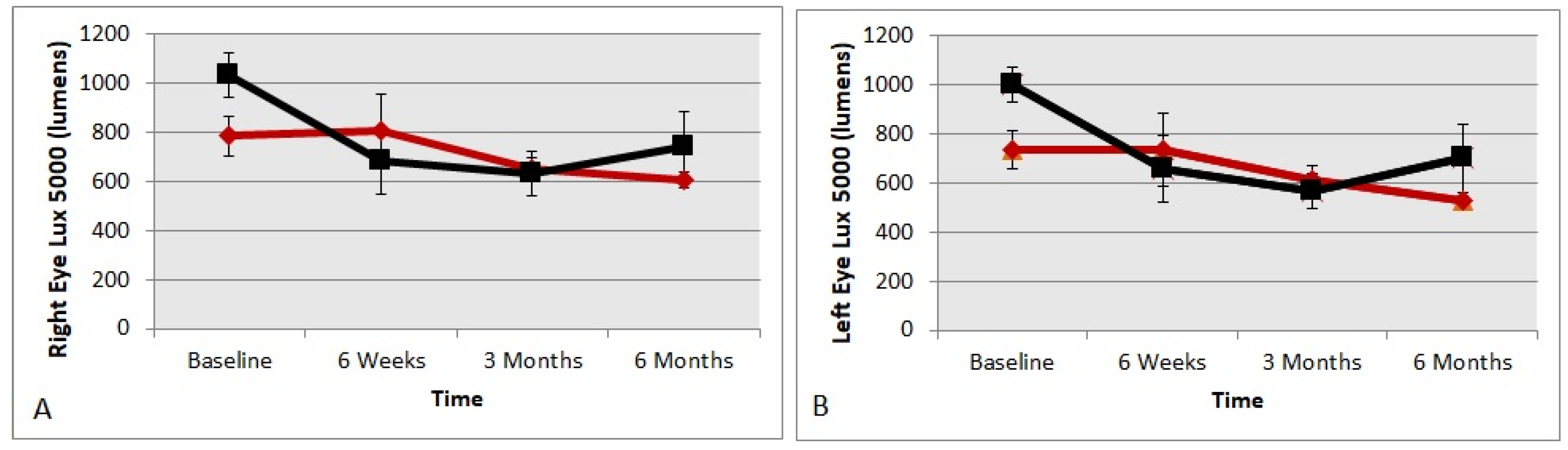
4.4. Preferred Luminance in Lumens
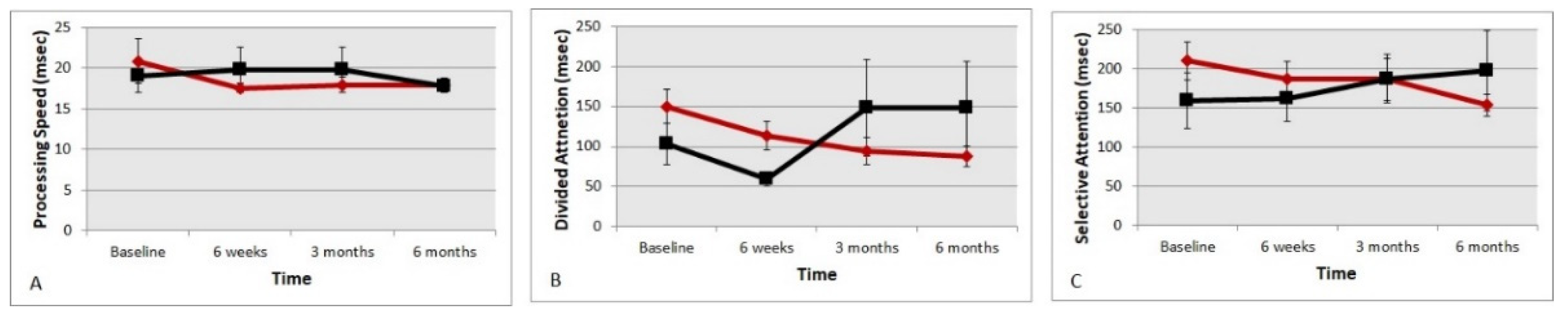
4.5. Useful Field of (UFOV) Reaction Times
4.6. Low Contrast Snellen Visual Acuity Letters
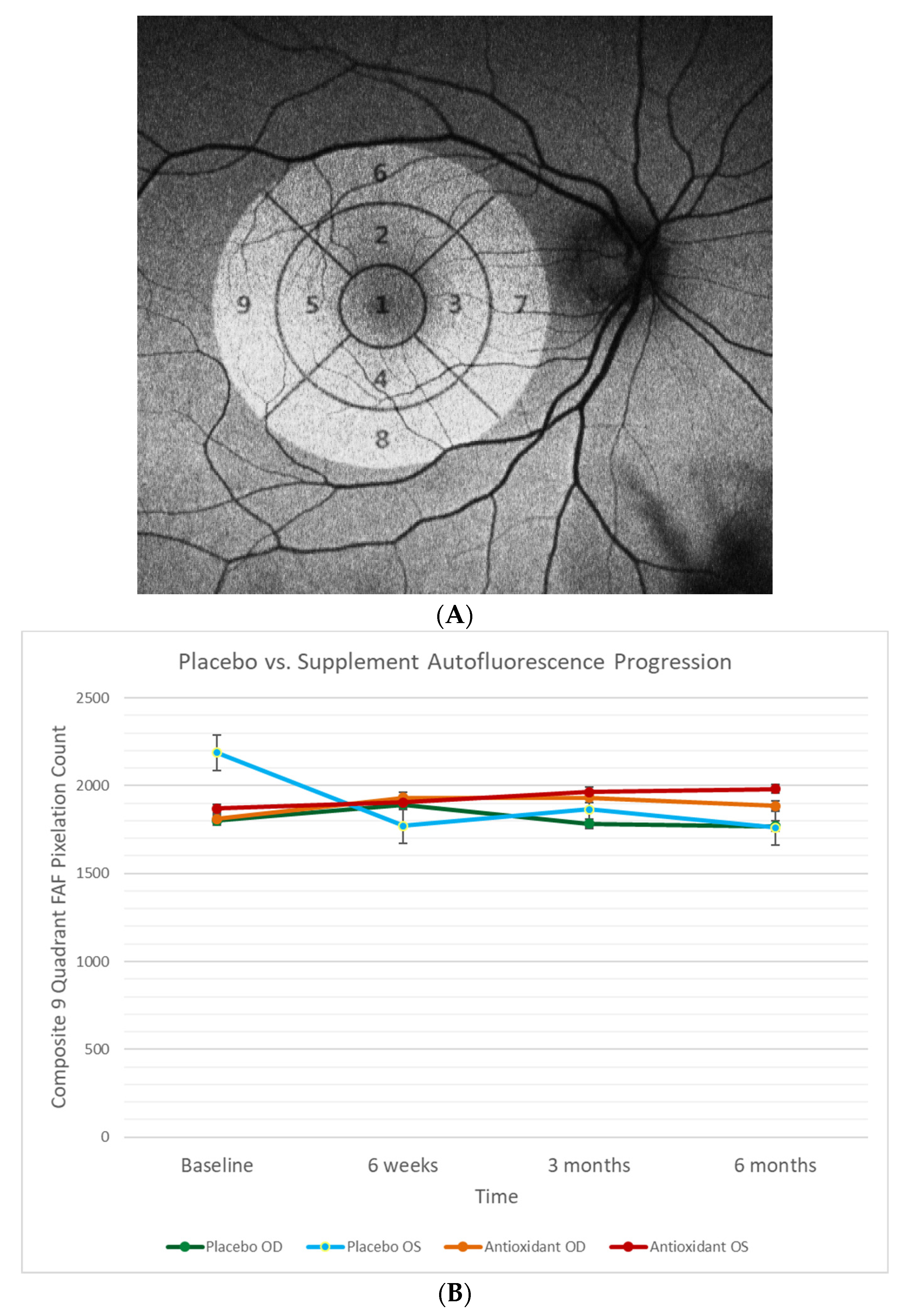
4.7. Retinal Fundus Auto-Fluorescence
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Ingredients | Amount per Serving |
|---|---|
| Zeaxanthin | 14 mg |
| Lutein | 7 mg |
| Vitamin A | 2500 IU |
| Vitamin C | 60 mg |
| Vitamin D | 1000 IU |
| Vitamin E | 60 IU |
| Vitamin B6 | 2 mg |
| Folic Acid | 400 mcg |
| Vitamin B12 | 6 mcg |
| Zinc | 15 mg |
| Selenium | 70 mcg |
| Manganese | 2 mg |
| Fish Oil | 150 mg |
| Coenzyme Q10 | 15 mg |
| Bilberry | 15 mg |
| Berry Anthocyanin Extract | 15 mg |
| Alpha Lipoic Acid | 10 mg |
| Mixed Tocopherols | 6 mg |

References
- Andysz, A.; Merecz, D. Visual abilities of older drivers—Review of driving simulator studies. Med. Pr. 2012, 63, 677–687. [Google Scholar]
- Prevalence of Impairments of Visual Function among European Drivers—Vision Impact Institute. Available online: https://www.visionimpactinstitute.org/research/prevalence-of-impairments-of-visual-function-among-european-drivers (accessed on 16 March 2021).
- Van Rijn, L.J.; Nischler, C.; Michael, R.; Heine, C.; Coeckelbergh, T.; Wilhelm, H.; Grabner, G.; Barraquer, R.I.; Van Den Berg, T.J.T.P. Prevalence of impairment of visual function in European drivers. Acta Ophthalmol. 2011, 89, 124–131. [Google Scholar] [CrossRef]
- Hessburg, P.C. Autonomous Vehicles, Drivers Fitness to Function and Naturalistic Driving Methods. In Proceedings of the 9th World Congress on Health and Modern Mobility, Detroit, MI, USA, 7–8 December 2002; Available online: www.henryford.com/TheEyeAndTheAuto (accessed on 16 March 2021).
- Wood, J.M.; Black, A.A.; Mallon, K.; Kwan, A.S.; Owsley, C. Effects of Age-Related Macular Degeneration on Driving Performance. Investig. Opthalmol. Vis. Sci. 2018, 59, 273. [Google Scholar] [CrossRef] [Green Version]
- NHTSA Report. Available online: https://one.nhtsa.gov/nhtsa/whatis/planning/2020Report/2020report.html (accessed on 27 March 2021).
- Chew, E.Y.; Clemons, T.E.; Sangiovanni, J.P.; Danis, R.P.; Ferris, F.L.; Elman, M.J.; Antoszyk, A.N.; Ruby, A.J.; Orth, D.; Bressler, S.B.; et al. Secondary Analyses of the Effects of Lutein/Zeaxanthin on Age-Related Macular Degeneration Progression. JAMA Ophthalmol. 2014, 132, 142. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, M.E.; Carroll, Y.; Corridan, B.; Olmedilla, B.; Granado, F.; Blanco, I.; Berg, H.V.D.; Hininger, I.; Rousell, A.M.; Chopra, M.; et al. A European carotenoid database to assess carotenoid intakes and its use in a five-country comparative study. Br. J. Nutr. 2001, 85, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Richer, S.; Park, D.W.; Epstein, R.; Wrobel, J.S.; Thomas, C. Macular Re-pigmentation Enhances Driving Vision in Elderly Adult Males with Macular Degeneration. J. Clin. Exp. Ophthalmol. 2012, 3, 217. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.; Qiu, Q.-H.; Wu, X.-W.; Cai, Z.-Y.; Xu, S.; Liang, X.-Q. Lutein supplementation improves visual performance in Chinese drivers: 1-year randomized, double-blind, placebo-controlled study. Nutrition 2013, 29, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Arunkumar, R.; Calvo, C.M.; Conrady, C.D.; Bernstein, P.S. What do we know about the macular pigment in AMD: The past, the present, and the future. Eye 2018, 32, 992–1004. [Google Scholar] [CrossRef] [Green Version]
- Hammond, B.R.; Fletcher, L.M.; Elliott, J.G. Glare Disability, Photostress Recovery, and Chromatic Contrast: Relation to Macular Pigment and Serum Lutein and Zeaxanthin. Investig. Opthalmol. Vis. Sci. 2013, 54, 476. [Google Scholar] [CrossRef] [Green Version]
- Owsley, C.; Wood, J.M.; McGwin, G., Jr. A roadmap for interpreting the literature on vision and driving. Surv. Ophthalmol. 2015, 60, 250–262. [Google Scholar] [CrossRef] [Green Version]
- Stringham, J.M.; Garcia, P.V.; Smith, P.A.; McLin, L.N.; Foutch, B.K. Macular Pigment and Visual Performance in Glare: Benefits for Photostress Recovery, Disability Glare, and Visual Discomfort. Investig. Opthalmol. Vis. Sci. 2011, 52, 7406. [Google Scholar] [CrossRef] [Green Version]
- Oliver, W.; Renzi-Hammond, L.M.; Thorne, S.A.; Clementz, B.; Miller, L.S.; Hammond, B.R. Neural Activation During Visual Attention Differs in Individuals with High versus Low Macular Pigment Density. Mol. Nutr. Food Res. 2019, 63, 1801052. [Google Scholar] [CrossRef]
- Kaido, M.; Matsutani, T.; Negishi, K.; Dogru, M.; Tsubota, K. Aged Drivers May Experience Decreased Visual Function While Driving. Asia-Pac. J. Ophthalmol. 2013, 2, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.J.; Vishwanathan, R.; Johnson, M.A.; Hausman, D.B.; Davey, A.; Scott, T.M.; Green, R.C.; Miller, L.S.; Gearing, M.; Woodard, J.; et al. Relationship between Serum and Brain Carotenoids,α-Tocopherol, and Retinol Concentrations and Cognitive Performance in the Oldest Old from the Georgia Centenarian Study. J. Aging Res. 2013, 2013, 951786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishwanathan, R.; Schalch, W.; Johnson, E.J. Macular pigment carotenoids in the retina and occipital cortex are related in humans. Nutr. Neurosci. 2016, 19, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Feeney, J.; Finucane, C.; Savva, G.M.; Cronin, H.; Beatty, S.; Nolan, J.M.; Kenny, R.A. Low macular pigment optical density is associated with lower cognitive performance in a large, population-based sample of older adults. Neurobiol. Aging 2013, 34, 2449–2456. [Google Scholar] [CrossRef]
- Hoffmann, K.G.; Richer, S.P.; Wrobel, J.S.; Chen, E.; Podella, C.J. A Prospective Study of Neuro-Cognitive Enhancement with Carotenoids in Elderly Adult Males with Early Age Related Macular Degeneration. Ophthalmol. Res. Int. J. 2015, 4, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, P.S.; Delori, F.C.; Richer, S.; Van Kuijk, F.J.M.; Wenzel, A.J. The value of measurement of macular carotenoid pigment optical densities and distributions in age-related macular degeneration and other retinal disorders. Vis. Res. 2010, 50, 716–728. [Google Scholar] [CrossRef] [Green Version]
- Davey, P.G.; Henderson, T.; Lem, D.W.; Weis, R.; Amonoo-Monney, S.; Evans, D.W. Visual Function and Macular Carotenoid Changes in Eyes with Retinal Drusen—An Open Label Randomized Controlled Trial to Compare a Micronized Lipid-Based Carotenoid Liquid Supplementation and AREDS-2 Formula. Nutrients 2020, 12, 3271. [Google Scholar] [CrossRef] [PubMed]
- Lem, D.W.; Davey, P.G.; Gierhart, D.L.; Rosen, R.B. A Systematic Review of Carotenoids in the Management of Age-Related Macular Degeneration. Antioxidants 2021, 10, 1255. [Google Scholar] [CrossRef]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. Carotenoids in the Management of Glaucoma: A Systematic Review of the Evidence. Nutrients 2021, 13, 1949. [Google Scholar] [CrossRef] [PubMed]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. A Systematic Review of Carotenoids in the Management of Diabetic Retinopathy. Nutrients 2021, 13, 2441. [Google Scholar] [CrossRef]
- Richer, S.; Stiles, W.; Statkute, L.; Pulido, J.; Frankowski, J.; Rudy, D.; Pei, K.; Tsipursky, M.; Nyland, J. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: The Veterans LAST study (Lutein Antioxidant Supplementation Trial). Optometry 2004, 75, 216–230. [Google Scholar] [CrossRef]
- Richer, S.P.; Stiles, W.; Graham-Hoffman, K.; Levin, M.; Ruskin, D.; Wrobel, J.; Park, D.-W.; Thomas, C. Randomized, double-blind, placebo-controlled study of zeaxanthin and visual function in patients with atrophic age-related macular degeneration. Optom. J. Am. Optom. Assoc. 2011, 82, 667–680.e666. [Google Scholar] [CrossRef] [PubMed]
- Owsley, C.; McGwin, G.; Scilley, K.; Kallies, K. Development of a Questionnaire to Assess Vision Problems under Low Luminance in Age-Related Maculopathy. Investig. Opthalmol. Vis. Sci. 2006, 47, 528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richer, S.; Robert, D.; Novil, S.; Dervishi, A.; Nassiri, S.; Davey, P.G. Predicting night vision difficulties during an eye examination. (Night Vision & Carotenoids RCT; Hines VA IRB 1052607-1, Baseline Data). Investig. Ophthalmol. Vis. Sci. 2019, 60, 1828. [Google Scholar]
- Jackson, G.R.; Scott, I.U.; Kim, I.K.; Quillen, D.A.; Iannaccone, A.; Edwards, J.G. Diagnostic Sensitivity and Specificity of Dark Adaptometry for Detection of Age-Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2014, 55, 1427. [Google Scholar] [CrossRef] [Green Version]
- Intelligent Refractor RT-6100. Available online: https://www.nidek-intl.com/product/ophthaloptom/refraction/ref_optometry/rt-6100.html (accessed on 16 March 2021).
- Smart System Standard. Available online: https://premierop.com/smart-system-standard/ (accessed on 16 March 2021).
- Davey, P.-G.; Alvarez, S.; Lee, J. Macular pigment optical density: Repeatability, intereye correlation, and effect of ocular dominance. Clin. Ophthalmol. 2016, 10, 1671–1678. [Google Scholar] [CrossRef] [Green Version]
- Van Der Veen, R.L.P.; Berendschot, T.T.J.M.; Hendrikse, F.; Carden, D.; Makridaki, M.; Murray, I.J. A new desktop instrument for measuring macular pigment optical density based on a novel technique for setting flicker thresholds. Ophthalmic Physiol. Opt. 2009, 29, 127–137. [Google Scholar] [CrossRef]
- Davey, P.G.; Rosen, R.B.; Gierhart, D.L. Macular Pigment Reflectometry: Developing Clinical Protocols, Comparison with Heterochromatic Flicker Photometry and Individual Carotenoid Levels. Nutrients 2021, 13, 2553. [Google Scholar] [CrossRef]
- Sanabria, J.C.; Bass, J.; Spors, F.; Gierhart, D.L.; Davey, P.G. Measurement of Carotenoids in Perifovea using the Macular Pigment Reflectometer. J. Vis. Exp. 2020, 155, e60429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, R.; Teussink, M.M.; Sloan, K.R.; Surya, J.; Raman, R. Evaluation of Macular Pigment Optical Density in Healthy Eyes Based on Dual-Wavelength Autofluorescence Imaging in South Indian Population. Transl. Vis. Sci. Technol. 2020, 9, 40. [Google Scholar] [CrossRef]
- Davey, P.G.; Lievens, C.; Amonoo-Monney, S. Differences in macular pigment optical density across four ethnicities: A comparative study. Ther. Adv. Ophthalmol. 2020, 12, 251584142092416. [Google Scholar] [CrossRef] [PubMed]
- Central Vision Analyzer. Available online: https://sinclairtechnologiesllc.com/project/real-world-functional-vision-analysis/cva/ (accessed on 16 March 2021).
- Wittich, W.; St Amour, L.; Jarry, J.; Seiple, W. Test-retest Variability of a Standardized Low Vision Lighting Assessment. Optom. Vis. Sci. 2018, 95, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Newsome, D.A.; Negreiro, M. Reproducible measurement of macular light flash recovery time using a novel device can indicate the presence and worsening of macular diseases. Curr. Eye Res. 2009, 34, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Loughman, J.; Hewitt, C.; Judge, C.; Martin, L.; Moulds, C.; Davison, P.A. Clinical applicability of the Macular Degeneration Detection Device (MDD-2): A novel photostress recovery measurement device. Clin. Exp. Optom. 2013, 96, 272–277. [Google Scholar] [CrossRef] [Green Version]
- Brain Training That Works. Available online: https://www.brainhq.com/?v4=true&fr=y (accessed on 21 March 2021).
- Holz, F.G.; Schmitz-Valckenberg, S.; Spaide, R.F.; Bird, A.C. Atlas of Fundus Autofluorescence Imaging, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Xu, Q.; Li, Y.; Cheng, Y.; Qu, Y. Assessment of the effect of age on macular layer thickness in a healthy Chinese cohort using spectral-domain optical coherence tomography. BMC Ophthalmol. 2018, 18, 169. [Google Scholar] [CrossRef] [Green Version]
- Chous, A.P.; Richer, S.P.; Gerson, J.D.; Kowluru, R.A. The Diabetes Visual Function Supplement Study (DiVFuSS). Br. J. Ophthalmol. 2016, 100, 227–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loughman, J.; Loskutova, E.; Butler, J.S.; Siah, W.F.; O’Brien, C. Macular pigment response to lutein, zeaxanthin and meso-zeaxanthin supplementation in open angle glaucoma: A randomized controlled trial. Ophthalmol. Sci. 2021, 1, 100039. [Google Scholar] [CrossRef]
- Siah, W.F.; O’Brien, C.; Loughman, J.J. Macular pigment is associated with glare-affected visual function and central visual field loss in glaucoma. Br. J. Ophthalmol. 2018, 102, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Davey, P.G.; Roman, B.O.; Evans, D.W. Efficacy of Commercially Available Nutritional Supplements: Analysis of Serum Uptake, Macular Pigment Optical Density and Visual Functional Response. Nutrients 2020, 12, 1321. [Google Scholar] [CrossRef] [PubMed]
- Dukic Willstrand, T.; Broberg, T.; Selander, H. Driving Characteristics of Older Drivers and Their Relationship to the Useful Field of View Test. Gerontology 2017, 63, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.; Amoah, I.; Diep, T.; Jalili-Moghaddam, S. Determinants and Suitability of Carotenoid Reflection Score as a Measure of Carotenoid Status. Nutrients 2020, 12, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.R.; Sandberg, K.A.; Foutch, B.K. Macular pigment optical density and visual quality of life. J. Optom. 2021, 14, 92–99. [Google Scholar] [CrossRef]





| Placebo Group | Treatment Group | p-Value | |
|---|---|---|---|
| Mean (Standard Deviation) | |||
| Age | 65.7 (8.0) | 61.6 (11.63) | 0.027 |
| Body Mass Index | 26.3 (3.42) | 31.30 (6.54) | 0.06 |
| Percent Body Fat | 28.2 (4.56) | 33.5 (6.81) | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richer, S.; Novil, S.; Gullett, T.; Dervishi, A.; Nassiri, S.; Duong, C.; Davis, R.; Davey, P.G. Night Vision and Carotenoids (NVC): A Randomized Placebo Controlled Clinical Trial on Effects of Carotenoid Supplementation on Night Vision in Older Adults. Nutrients 2021, 13, 3191. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093191
Richer S, Novil S, Gullett T, Dervishi A, Nassiri S, Duong C, Davis R, Davey PG. Night Vision and Carotenoids (NVC): A Randomized Placebo Controlled Clinical Trial on Effects of Carotenoid Supplementation on Night Vision in Older Adults. Nutrients. 2021; 13(9):3191. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093191
Chicago/Turabian StyleRicher, Stuart, Steven Novil, Taylor Gullett, Avni Dervishi, Sherwin Nassiri, Co Duong, Robert Davis, and Pinakin Gunvant Davey. 2021. "Night Vision and Carotenoids (NVC): A Randomized Placebo Controlled Clinical Trial on Effects of Carotenoid Supplementation on Night Vision in Older Adults" Nutrients 13, no. 9: 3191. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093191