
Effects of Caloric Restriction and Rope-Skipping Exercise on Cardiometabolic Health: A Pilot Randomized Controlled Trial in Young Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Randomization
2.3. Intervention
2.3.1. Dietary Intervention
2.3.2. Exercise Intervention
2.4. Data Collection
2.4.1. Anthropometry
2.4.2. Cardiopulmonary Exercise Testing
2.4.3. Laboratory Tests
2.4.4. Dietary Records
2.4.5. Exercise Records
2.5. Quality Control
2.5.1. Randomization
2.5.2. Participant Compliance
2.6. Statistical Analyses
3. Results
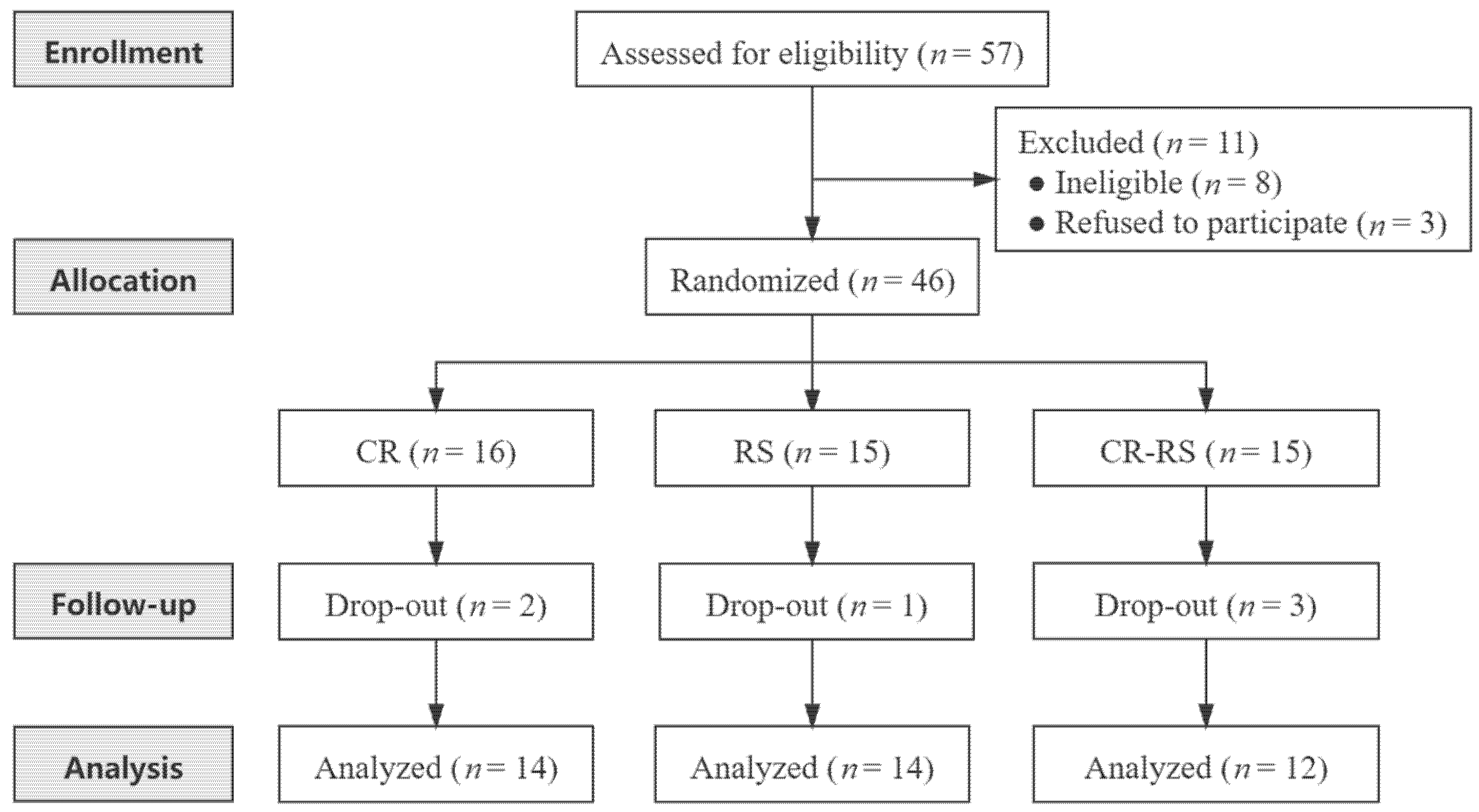
3.1. Study Overview and Participant Characteristics
3.2. Effect of Caloric Restriction and Exercise on Body Weight and Composition
3.3. Effect of Caloric Restriction and Exercise on Metabolic Risk Markers
3.4. Effect of Caloric Restriction and Exercise on Inflammatory Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Connor, E.A.; Evans, C.V.; Rushkin, M.C.; Redmond, N.; Lin, J.S. Behavioral Counseling to Promote a Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults With Cardiovascular Risk Factors: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 324, 2076–2094. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.A.; Winkel, M.; Ali, M.K.; Narayan, K.M.; Mehta, N.K. Cardiovascular mortality associated with 5 leading risk factors: National and state preventable fractions estimated from survey data. Ann. Intern. Med. 2015, 163, 245–253. [Google Scholar] [CrossRef]
- Li, N.; Guenancia, C.; Rigal, E.; Hachet, O.; Chollet, P.; Desmoulins, L.; Leloup, C.; Rochette, L.; Vergely, C. Short-term moderate diet restriction in adulthood can reverse oxidative, cardiovascular and metabolic alterations induced by postnatal overfeeding in mice. Sci. Rep. 2016, 6, 30817. [Google Scholar] [CrossRef]
- Cevikelli-Yakut, Z.A.; Ozcelik, R.; Cevik, O.; Sener, T.E.; Sener, G. Exercise and caloric restriction improve cardiovascular and erectile function in rats with metabolic syndrome. Int. J. Impot. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- La Russa, D.; Marrone, A.; Mandala, M.; Macirella, R.; Pellegrino, D. Antioxidant/Anti-Inflammatory Effects of Caloric Restriction in an Aged and Obese Rat Model: The Role of Adiponectin. Biomedicines 2020, 8, 532. [Google Scholar] [CrossRef]
- Mattison, J.A.; Colman, R.J.; Beasley, T.M.; Allison, D.B.; Kemnitz, J.W.; Roth, G.S.; Ingram, D.K.; Weindruch, R.; de Cabo, R.; Anderson, R.M. Caloric restriction improves health and survival of rhesus monkeys. Nat. Commun. 2017, 8, 14063. [Google Scholar] [CrossRef]
- Colman, R.J.; Beasley, T.M.; Kemnitz, J.W.; Johnson, S.C.; Weindruch, R.; Anderson, R.M. Caloric restriction reduces age-related and all-cause mortality in rhesus monkeys. Nat. Commun. 2014, 5, 3557. [Google Scholar] [CrossRef]
- Most, J.; Tosti, V.; Redman, L.M.; Fontana, L. Calorie restriction in humans: An update. Ageing Res. Rev. 2017, 39, 36–45. [Google Scholar] [CrossRef]
- Lefevre, M.; Redman, L.M.; Heilbronn, L.K.; Smith, J.V.; Martin, C.K.; Rood, J.C.; Greenway, F.L.; Williamson, D.A.; Smith, S.R.; Ravussin, E.; et al. Caloric restriction alone and with exercise improves CVD risk in healthy non-obese individuals. Atherosclerosis 2009, 203, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.S.; Covington, J.D.; Ravussin, E.; Redman, L.M.; Pennington, C.T. Little evidence of systemic and adipose tissue inflammation in overweight individuals(dagger). Front. Genet. 2012, 3, 58. [Google Scholar]
- Meydani, S.N.; Das, S.K.; Pieper, C.F.; Lewis, M.R.; Klein, S.; Dixit, V.D.; Gupta, A.K.; Villareal, D.T.; Bhapkar, M.; Huang, M.; et al. Long-term moderate calorie restriction inhibits inflammation without impairing cell-mediated immunity: A randomized controlled trial in non-obese humans. Aging 2016, 8, 1416–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Most, J.; Gilmore, L.A.; Smith, S.R.; Han, H.; Ravussin, E.; Redman, L.M. Significant improvement in cardiometabolic health in healthy nonobese individuals during caloric restriction-induced weight loss and weight loss maintenance. Am. J. Physiol. Endocrinol. Metab. 2018, 314, E396–E405. [Google Scholar] [CrossRef] [Green Version]
- Kraus, W.E.; Bhapkar, M.; Huffman, K.M.; Pieper, C.F.; Krupa Das, S.; Redman, L.M.; Villareal, D.T.; Rochon, J.; Roberts, S.B.; Ravussin, E.; et al. 2 years of calorie restriction and cardiometabolic risk (CALERIE): Exploratory outcomes of a multicentre, phase 2, randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 673–683. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 3), 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gronek, P.; Wielinski, D.; Cyganski, P.; Rynkiewicz, A.; Zajac, A.; Maszczyk, A.; Gronek, J.; Podstawski, R.; Czarny, W.; Balko, S.; et al. A Review of Exercise as Medicine in Cardiovascular Disease: Pathology and Mechanism. Aging Dis. 2020, 11, 327–340. [Google Scholar] [CrossRef] [Green Version]
- Wasenius, N.S.; Isomaa, B.A.; Ostman, B.; Soderstrom, J.; Forsen, B.; Lahti, K.; Hakaste, L.; Eriksson, J.G.; Groop, L.; Hansson, O.; et al. Low-cost exercise interventions improve long-term cardiometabolic health independently of a family history of type 2 diabetes: A randomized parallel group trial. BMJ Open Diabetes Res. Care 2020, 8, e001377. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.; Andersson, J.; Stahl, J.; Stomby, A.; Saleh, A.; Waling, M.; Ryberg, M.; Hauksson, J.; Svensson, M.; Johansson, B.; et al. Exercise Training Adds Cardiometabolic Benefits of a Paleolithic Diet in Type 2 Diabetes Mellitus. J. Am. Heart Assoc. 2019, 8, e010634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, K.D.; Pekas, E.J.; Scott, S.D.; Son, W.M.; Park, S.Y. The effects of a 12-week jump rope exercise program on abdominal adiposity, vasoactive substances, inflammation, and vascular function in adolescent girls with prehypertension. Eur. J. Appl. Physiol. 2019, 119, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Son, W.M.; Headid Iii, R.J.; Pekas, E.J.; Noble, J.M.; Park, S.Y. The effects of a 12-week jump rope exercise program on body composition, insulin sensitivity, and academic self-efficacy in obese adolescent girls. J. Pediatr. Endocrinol. Metab. 2020, 33, 129–137. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caristia, S.; Vito, M.; Sarro, A.; Leone, A.; Pecere, A.; Zibetti, A.; Filigheddu, N.; Zeppegno, P.; Prodam, F.; Faggiano, F.; et al. Is Caloric Restriction Associated with Better Healthy Aging Outcomes? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 2290. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, A.A.; Beka, V.; Prado, C.M. The effect of caloric restriction on blood pressure and cardiovascular function: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 728–739. [Google Scholar] [CrossRef]
- Larson-Meyer, D.E.; Heilbronn, L.K.; Redman, L.M.; Newcomer, B.R.; Frisard, M.I.; Anton, S.; Smith, S.R.; Alfonso, A.; Ravussin, E. Effect of calorie restriction with or without exercise on insulin sensitivity, beta-cell function, fat cell size, and ectopic lipid in overweight subjects. Diabetes Care 2006, 29, 1337–1344. [Google Scholar] [CrossRef] [Green Version]
- Blumenthal, J.A.; Babyak, M.A.; Sherwood, A.; Craighead, L.; Lin, P.H.; Johnson, J.; Watkins, L.L.; Wang, J.T.; Kuhn, C.; Feinglos, M.; et al. Effects of the dietary approaches to stop hypertension diet alone and in combination with exercise and caloric restriction on insulin sensitivity and lipids. Hypertension 2010, 55, 1199–1205. [Google Scholar] [CrossRef] [Green Version]
- Zurlo, F.; Trevisan, C.; Vitturi, N.; Ravussin, E.; Salvo, C.; Carraro, S.; Siffi, M.; Iob, I.; Saller, A.; Previato, L.; et al. One-year caloric restriction and 12-week exercise training intervention in obese adults with type 2 diabetes: Emphasis on metabolic control and resting metabolic rate. J. Endocrinol. Investig. 2019, 42, 1497–1507. [Google Scholar] [CrossRef]
- Shaw, K.; Gennat, H.; O’Rourke, P.; Del Mar, C. Exercise for overweight or obesity. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagard, R.H.; Cornelissen, V.A. Effect of exercise on blood pressure control in hypertensive patients. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Buchowski, M.S.; Hongu, N.; Acra, S.; Wang, L.; Warolin, J.; Roberts, L.J., 2nd. Effect of modest caloric restriction on oxidative stress in women, a randomized trial. PLoS ONE 2012, 7, e47079. [Google Scholar] [CrossRef] [Green Version]
- Alberga, A.S.; Frappier, A.; Sigal, R.J.; Prud’homme, D.; Kenny, G.P. A review of randomized controlled trials of aerobic exercise training on fitness and cardiometabolic risk factors in obese adolescents. Phys. Sportsmed. 2013, 41, 44–57. [Google Scholar] [CrossRef]
- Ben Ounis, O.; Elloumi, M.; Ben Chiekh, I.; Zbidi, A.; Amri, M.; Lac, G.; Tabka, Z. Effects of two-month physical-endurance and diet-restriction programmes on lipid profiles and insulin resistance in obese adolescent boys. Diabetes Metab. 2008, 34, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, F.B.; Ginsberg, H.N. Gerald M. Reaven, MD: Demonstration of the central role of insulin resistance in type 2 diabetes and cardiovascular disease. Diabetes Care 2014, 37, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Iaccarino, G.; Franco, D.; Sorriento, D.; Strisciuglio, T.; Barbato, E.; Morisco, C. Modulation of Insulin Sensitivity by Exercise Training: Implications for Cardiovascular Prevention. J. Cardiovasc. Transl. Res. 2021, 14, 256–270. [Google Scholar] [CrossRef]
- Gayoso-Diz, P.; Otero-Gonzalez, A.; Rodriguez-Alvarez, M.X.; Gude, F.; Garcia, F.; De Francisco, A.; Quintela, A.G. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: Effect of gender and age: EPIRCE cross-sectional study. BMC Endocr. Disord. 2013, 13, 47. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Shih, A.Z.; Woo, Y.C.; Fong, C.H.; Leung, O.Y.; Janus, E.; Cheung, B.M.; Lam, K.S. Optimal Cut-Offs of Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) to Identify Dysglycemia and Type 2 Diabetes Mellitus: A 15-Year Prospective Study in Chinese. PLoS ONE 2016, 11, e0163424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorling, J.L.; Martin, C.K.; Redman, L.M. Calorie restriction for enhanced longevity: The role of novel dietary strategies in the present obesogenic environment. Ageing Res. Rev. 2020, 64, 101038. [Google Scholar] [CrossRef]
- Imayama, I.; Ulrich, C.M.; Alfano, C.M.; Wang, C.; Xiao, L.; Wener, M.H.; Campbell, K.L.; Duggan, C.; Foster-Schubert, K.E.; Kong, A.; et al. Effects of a caloric restriction weight loss diet and exercise on inflammatory biomarkers in overweight/obese postmenopausal women: A randomized controlled trial. Cancer Res. 2012, 72, 2314–2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana, L.; Villareal, D.T.; Weiss, E.P.; Racette, S.B.; Steger-May, K.; Klein, S.; Holloszy, J.O.; Washington University School of Medicine, C.G. Calorie restriction or exercise: Effects on coronary heart disease risk factors. A randomized, controlled trial. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E197–E202. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (n = 40) | CR (n = 14) | RS (n = 14) | CR–RS (n = 12) | p Value |
|---|---|---|---|---|---|
| Age, years, mean (SD) | 19.4 (0.6) | 19.4 (0.6) | 19.3 (0.6) | 19.4 (0.7) | 0.840 |
| Sex | 0.938 | ||||
| Female | 25 (62.5) | 9 (64.3) | 9 (64.3) | 7 (58.3) | |
| Male | 15 (37.5) | 5 (35.7) | 5 (35.7) | 5 (41.7) | |
| Body weight status | 0.794 | ||||
| Normal | 17 (42.5) | 7 (50.0) | 5 (35.7) | 5 (41.7) | |
| Overweight and Obese | 23 (57.5) | 7 (50.0) | 9 (64.3) | 7 (58.3) | |
| Feeding patterns | 0.522 | ||||
| Breastfeeding | 27 (73.0) | 9 (64.3) | 11 (84.6) | 7 (70.0) | |
| Not breastfeeding | 10 (27.0) | 5 (35.7) | 2 (15.4) | 3 (30.0) | |
| Mode of delivery | 0.133 | ||||
| Vaginal delivery | 24 (64.9) | 7 (50.0) | 8 (61.5) | 9 (90.0) | |
| Cesarean delivery | 13 (35.1) | 7 (50.0) | 5 (38.5) | 1 (10.0) | |
| Paternal educational level | 0.836 | ||||
| Senior high school or below | 15 (40.5) | 5 (35.7) | 5 (38.5) | 5 (50.0) | |
| Junior college or above | 22 (59.5) | 9 (64.3) | 8 (61.5) | 5 (50.0) | |
| Maternal educational level | 0.942 | ||||
| Senior high school or below | 20 (54.1) | 8 (57.1) | 7 (53.8) | 5 (50.0) | |
| Junior college or above | 17 (45.9) | 6 (42.9) | 6 (46.2) | 5 (50.0) | |
| Monthly household income | 0.068 | ||||
| <5000 RMB/person | 21 (56.8) | 8 (57.1) | 5 (38.5) | 8 (80.0) | |
| ≥5000 RMB/person | 12 (32.4) | 6 (42.9) | 4 (30.8) | 2 (20.0) | |
| Unknown | 4 (10.8) | 0 (0.0) | 4 (30.8) | 0 (0.0) | |
| Outdoor time | 0.790 | ||||
| <1 h/d | 16 (43.2) | 6 (42.9) | 6 (46.2) | 4 (40.0) | |
| 1~<2 h/d | 17 (45.9) | 6 (42.9) | 5 (38.5) | 6 (60.0) | |
| ≥2 h/d | 4 (10.8) | 2 (14.3) | 2 (15.4) | 0 (0.0) |
| Variables | CR (n = 14) | RS (n = 14) | CR–RS (n = 12) | Among-Group p |
|---|---|---|---|---|
| Weight, kg | ||||
| Baseline a | 70.1 (11.5) | 69.3 (11.5) | 67.8 (9.6) | 0.860 |
| 8 weeks a | 69.0 (11.5) | 68.7 (11.6) | 66.5 (8.4) | 0.809 |
| Change a | −1.1 (1.7) | −0.6 (2.5) | −1.3 (2.0) | 0.670 |
| 8-week-adjusted c | 68.1 (67.0, 69.1) | 68.6 (67.5, 69.6) | 67.8 (66.6, 68.9) | 0.600 |
| Within-group p d | 0.038 | 0.424 | 0.051 | |
| BMI | ||||
| Baseline a | 24.8 (2.5) | 24.4 (1.9) | 24.5 (2.4) | 0.914 |
| 8 weeks a | 24.4 (2.6) | 24.2 (2.3) | 24.1 (2.0) | 0.937 |
| Change a | −0.4 (0.6) | −0.2 (1.0) | −0.5 (0.7) | 0.721 |
| 8-week-adjusted c | 24.2 (23.8, 24.6) | 24.3 (23.9, 24.7) | 24.1 (23.7, 24.5) | 0.710 |
| Within-group p d | 0.046 | 0.434 | 0.049 | |
| PBF, % | ||||
| Baseline a | 31.3 (7.0) | 30.6 (7.7) | 31.6 (7.9) | 0.949 |
| 8 weeks a | 30.1 (7.5) | 29.8 (7.9) | 29.9 (8.3) | 0.995 |
| Change a | −1.2 (1.6) | −0.8 (2.0) | −1.7 (1.8) | 0.478 |
| 8-week-adjusted c | 29.9 (29.1, 30.8) | 30.3 (29.4, 31.2) | 29.4 (28.5, 30.4) | 0.402 |
| Within-group p d | 0.014 | 0.156 | 0.007 | |
| BFM, kg | ||||
| Baseline b | 20.4 (17.8, 25.6) | 20.5 (18.3, 23.0) | 20.9 (17.2, 22.5) | 0.969 |
| 8 weeks b | 19.8 (16.1, 24.7) | 19.4 (15.3, 23.1) | 19.6 (15.9, 22.0) | 0.975 |
| Change b | −1.1 (−2.2, −0.3) | −0.3 (−1.3, 0.2) | −1.1 (−2.5, −0.4) | 0.316 |
| 8-week-adjusted c | 19.5 (18.7, 20.4) | 19.9 (19.1, 20.9) | 19.2 (18.3, 20.1) | 0.497 |
| Within-group p d | 0.006 | 0.151 | 0.015 |
| Variables | CR (n = 14) | RS (n = 14) | CR–RS (n = 12) | Among-Group p |
|---|---|---|---|---|
| SBP, mmHg | ||||
| Baseline a | 113 (10) | 115 (8) | 116 (12) | 0.761 |
| 8 weeks a | 118 (11) | 116 (11) | 112 (12) | 0.461 |
| Change a | 5 (9) | 1 (10) | −4 (7) | 0.065 |
| 8-week-adjusted c | 119 (115, 123) | 116 (111, 120) | 111 (106, 116) | 0.058 |
| Within-group p d | 0.075 | 0.695 | 0.090 | |
| DBP, mmHg | ||||
| Baseline a | 75 (9) | 73 (5) | 75 (8) | 0.702 |
| 8 weeks a | 74 (7) | 75 (7) | 73 (10) | 0.696 |
| Change a | 0 (7) | 2 (6) | −3 (7) | 0.180 |
| 8-week-adjusted c | 74 (71, 77) | 76 (73, 79) | 72 (68, 75) | 0.208 |
| Within-group p d | 0.810 | 0.214 | 0.208 | |
| TG, mmol/L | ||||
| Baseline b | 0.87 (0.63, 1.29) | 0.84 (0.71, 1.05) | 0.83 (0.67, 1.11) | 0.993 |
| 8 weeks b | 0.94 (0.72, 1.21) | 0.83 (0.72, 1.26) | 0.97 (0.78, 1.24) | 0.496 |
| Change b | 0.08 (−0.08, 0.15) | −0.08 (−0.19, 0.17) | 0.11 (−0.12, 0.60) | 0.480 |
| 8-week-adjusted c | 0.97 (0.84, 1.12) | 0.90 (0.78, 1.04) | 1.11 (0.95, 1.30) | 0.130 |
| Within-group p d | 0.504 | 0.985 | 0.102 | |
| TC, mmol/L | ||||
| Baseline a | 4.52 (0.70) | 4.39 (0.73) | 4.70 (0.85) | 0.581 |
| 8 weeks a | 4.30 (0.58) | 4.42 (0.89) | 4.42 (0.54) | 0.879 |
| Change a | −0.22 (0.58) | 0.03 (0.65) | −0.29 (0.51) | 0.358 |
| 8-week-adjusted c | 4.31 (4.05, 4.57) | 4.50 (4.24, 4.76) | 4.31 (4.02, 4.59) | 0.492 |
| Within-group p d | 0.188 | 0.872 | 0.080 | |
| HDL-C, mmol/L | ||||
| Baseline a | 1.40 (0.41) | 1.46 (0.31) | 1.49 (0.29) | 0.798 |
| 8 weeks a | 1.39 (0.30) | 1.52 (0.28) | 1.44 (0.28) | 0.504 |
| Change a | −0.01 (0.20) | 0.06 (0.15) | −0.06 (0.16) | 0.239 |
| 8-week-adjusted c | 1.42 (1.35, 1.50) | 1.51 (1.44, 1.59) | 1.41 (1.33, 1.49) | 0.114 |
| Within-group p d | 0.796 | 0.158 | 0.268 | |
| LDL-C, mmol/L | ||||
| Baseline a | 2.79 (0.61) | 2.67 (0.64) | 2.98 (0.79) | 0.505 |
| 8 weeks a | 2.56 (0.46) | 2.66 (0.83) | 2.58 (0.62) | 0.911 |
| Change a | −0.23 (0.51) | 0.00 (0.63) | −0.40 (0.37) | 0.172 |
| 8-week-adjusted c | 2.57 (2.33, 2.81) | 2.75 (2.51, 2.99) | 2.46 (2.20, 2.72) | 0.267 |
| Within-group p d | 0.119 | 0.980 | 0.004 | |
| FPG, mmol/L | ||||
| Baseline a | 4.21 (0.58) | 4.22 (0.30) | 3.93 (0.38) | 0.193 |
| 8 weeks a | 4.27 (0.50) | 4.21 (0.36) | 3.95 (0.42) | 0.159 |
| Change a | 0.06 (0.32) | 0.00 (0.43) | 0.02 (0.43) | 0.915 |
| 8-week-adjusted c | 4.22 (4.04, 4.40) | 4.16 (3.98, 4.34) | 4.06 (3.87, 4.26) | 0.520 |
| Within-group p d | 0.496 | 0.981 | 0.881 | |
| Insulin, mIU/L | ||||
| Baseline b | 10.59 (7.21, 14.42) | 10.13 (8.00, 13.89) | 7.93 (5.20, 11.44) | 0.260 |
| 8 weeks b | 10.20 (7.73, 15.67) | 11.36 (6.72, 14.04) | 9.79 (6.94, 13.05) | 0.630 |
| Change b | 1.03 (−0.54, 2.75) | −1.04 (−3.77, 0.82) | −0.67 (−1.84, 2.24) | 0.330 |
| 8-week-adjusted c | 13.07 (10.66, 15.48) | 11.01 (8.60, 13.42) | 10.18 (7.57, 12.78) | 0.251 |
| Within-group p d | 0.255 | 0.563 | 0.669 | |
| HOMA-IR | ||||
| Baseline b | 1.89 (1.32, 2.91) | 1.96 (1.48, 2.62) | 1.38 (0.90, 2.02) | 0.159 |
| 8 weeks b | 1.95 (1.26, 3.03) | 2.06 (1.25, 2.80) | 1.64 (1.13, 2.22) | 0.491 |
| Change b | 0.13 (−0.22, 0.43) | −0.13 (−0.64, 0.26) | −0.07 (−0.30, 0.39) | 0.412 |
| 8-week-adjusted c | 2.53 (2.01, 3.05) | 2.11 (1.59, 2.63) | 1.82 (1.26, 2.39) | 0.186 |
| Within-group p d | 0.273 | 0.690 | 0.623 | |
| HOMA-β | ||||
| Baseline a | 263.83 (188.64, 880.00) | 280.19 (220.00, 370.40) | 373.47 (266.07, 686.53) | 0.566 |
| 8 weeks a | 367.63 (187.96, 748.70) | 309.30 (236.87, 418.89) | 370.47 (249.18, 758.90) | 0.595 |
| Change a | 52.03 (−73.93, 120.15) | −35.85 (−59.52, 62.71) | −41.38 (−169.59, 66.11) | 0.690 |
| 8-week-adjusted c | 498.26 (293.20, 703.31) | 552.72 (349.09, 756.34) | 540.54 (324.13, 756.96) | 0.931 |
| Within-group p d | 0.889 | 0.959 | 0.842 | |
| UA, μmol/L | ||||
| Baseline a | 390 (124) | 390 (77) | 406 (86) | 0.904 |
| 8 weeks a | 377 (111) | 358 (54) | 375 (64) | 0.785 |
| Change a | −13 (53) | −33 (66) | −30 (90) | 0.727 |
| 8-week-adjusted c | 380 (351, 409) | 360 (332, 389) | 369 (338, 400) | 0.639 |
| Within-group p d | 0.376 | 0.086 | 0.268 |
| Variables | CR (n = 14) | RS (n = 14) | CR–RS (n = 12) | Among-Group p |
|---|---|---|---|---|
| hs-CRP, mg/L | ||||
| Baseline b | 1.1 (0.6, 2.2) | 0.5 (0.3, 1.1) | 0.5 (0.2, 1.5) | 0.203 |
| 8 weeks b | 1.2 (0.2, 1.7) | 0.5 (0.3, 0.6) | 0.35 (0.2, 1) | 0.360 |
| Change b | −0.1 (−0.3, 0.2) | 0.1 (−0.2, 0.2) | 0.0 (−0.2, 0.3) | 0.794 |
| 8-week-adjusted c | 0.6 (0.4, 1.0) | 0.6 (0.3, 0.9) | 0.6 (0.4, 1.1) | 0.928 |
| Within-group p d | 0.247 | 0.649 | 0.744 | |
| NO, μmol/L | ||||
| Baseline b | 675.40 (142.75, 1000.00) | 120.21 (74.44, 213.18) | 34.27 (23.22, 256.87) | 0.020 |
| 8 weeks b | 621.95 (516.87, 812.29) | 97.68 (69.45, 123.29) | 123.53 (37.29, 349.45) | 0.028 |
| Change b | 19.39 (0.00, 71.01) | 0.15 (−8.18, 17.30) | −0.97 (−24.76, 19.14) | 0.535 |
| 8-week-adjusted c | 178.67 (150.91, 211.54) | 138.68 (114.49, 167.99) | 141.71 (119.88, 167.52) | 0.099 |
| Within-group p d | 0.104 | 0.604 | 0.327 | |
| TNF-α, pg/mL | ||||
| Baseline a | 2.05 (0.51) | 2.04 (0.56) | 2.23 (0.67) | 0.664 |
| 8 weeks a | 2.22 (0.63) | 1.95 (0.48) | 2.05 (0.57) | 0.457 |
| Change a | 0.18 (0.68) | −0.09 (0.49) | −0.18 (0.48) | 0.260 |
| 8-week-adjusted c | 2.25 (2.00, 2.49) | 1.98 (1.72, 2.23) | 1.99 (1.71, 2.26) | 0.234 |
| Within-group p d | 0.350 | 0.501 | 0.241 | |
| IL-6, pg/mL | ||||
| Baseline a | 1.73 (0.95) | 1.72 (1.07) | 1.38 (0.32) | 0.547 |
| 8 weeks a | 1.70 (0.60) | 1.70 (1.02) | 1.32 (0.24) | 0.343 |
| Change a | −0.03 (0.92) | −0.02 (0.37) | −0.06 (0.26) | 0.988 |
| 8-week-adjusted c | 1.64 (1.39, 1.89) | 1.64 (1.38, 1.90) | 1.46 (1.18, 1.75) | 0.596 |
| Within-group p d | 0.913 | 0.849 | 0.487 | |
| IL-8, pg/mL | ||||
| Baseline a | 1.90 (0.54) | 2.25 (0.91) | 2.57 (1.42) | 0.245 |
| 8 weeks a | 1.68 (0.47) | 1.91 (0.51) | 1.85 (1.37) | 0.760 |
| Change a | −0.22 (0.69) | −0.34 (0.71) | −0.73 (0.65) | 0.183 |
| 8-week-adjusted c | 1.87 (1.58, 2.17) | 1.89 (1.59, 2.19) | 1.62 (1.29, 1.95) | 0.441 |
| Within-group p d | 0.248 | 0.110 | 0.004 | |
| MCP-1, pg/mL | ||||
| Baseline a | 54.50 (22.43) | 63.92 (27.51) | 67.91 (31.25) | 0.442 |
| 8 weeks a | 74.34 (38.43) | 80.17 (42.05) | 74.01 (46.07) | 0.917 |
| Change a | 19.84 (27.32) | 16.25 (37.06) | 6.10 (26.15) | 0.531 |
| 8-week-adjusted c | 81.90 (66.27, 97.53) | 77.71 (61.69, 93.73) | 67.30 (49.76, 84.84) | 0.471 |
| Within-group p d | 0.018 | 0.140 | 0.457 | |
| VEGF, pg/mL | ||||
| Baseline a | 24.79 (11.15) | 22.61 (11.35) | 22.89 (10.42) | 0.857 |
| 8 weeks a | 26.98 (13.84) | 21.59 (11.14) | 19.70 (10.87) | 0.300 |
| Change a | 2.19 (13.63) | −1.03 (13.79) | −3.19 (5.95) | 0.534 |
| 8-week-adjusted c | 26.31 (20.89, 31.73) | 22.04 (16.42, 27.65) | 20.01 (13.91, 26.11) | 0.292 |
| Within-group p d | 0.558 | 0.793 | 0.106 | |
| Leptin, ng/mL | ||||
| Baseline a | 12.44 (11.65) | 13.05 (8.70) | 12.46 (11.81) | 0.987 |
| 8 weeks a | 12.41 (11.56) | 11.94 (10.01) | 8.54 (5.53) | 0.571 |
| Change a | −0.02 (4.42) | −1.12 (5.86) | −3.93 (8.51) | 0.307 |
| 8-week-adjusted c | 12.57 (9.77, 15.38) | 11.65 (8.73, 14.56) | 8.68 (5.51, 11.84) | 0.179 |
| Within-group p d | 0.984 | 0.505 | 0.157 | |
| VCAM-1, ng/mL | ||||
| Baseline a | 383.15 (127.38) | 452.66 (143.90) | 451.60 (117.68) | 0.304 |
| 8 weeks a | 397.65 (116.18) | 450.39 (142.19) | 498.31 (120.50) | 0.156 |
| Change a | 14.50 (87.75) | −2.27 (85.41) | 46.71 (109.98) | 0.446 |
| 8-week-adjusted c | 428.73 (384.51, 472.96) | 431.91 (386.68, 477.15) | 480.59 (431.49, 529.68) | 0.240 |
| Within-group p d | 0.547 | 0.925 | 0.189 | |
| ICAM-1, ng/mL | ||||
| Baseline a | 142.29 (65.22) | 129.79 (79.11) | 125.95 (45.08) | 0.804 |
| 8 weeks a | 134.44 (57.58) | 123.94 (65.91) | 122.70 (33.64) | 0.836 |
| Change a | −7.85 (29.14) | −5.85 (18.86) | −3.25 (20.65) | 0.890 |
| 8-week-adjusted c | 127.34 (117.67, 137.00) | 126.69 (116.70, 136.68) | 128.48 (117.60, 139.36) | 0.972 |
| Within-group p d | 0.332 | 0.285 | 0.613 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, Z.; Ming, Y.; Wu, M.; Jing, J.; Xu, S.; Li, H.; Zhu, Y. Effects of Caloric Restriction and Rope-Skipping Exercise on Cardiometabolic Health: A Pilot Randomized Controlled Trial in Young Adults. Nutrients 2021, 13, 3222. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093222
Tang Z, Ming Y, Wu M, Jing J, Xu S, Li H, Zhu Y. Effects of Caloric Restriction and Rope-Skipping Exercise on Cardiometabolic Health: A Pilot Randomized Controlled Trial in Young Adults. Nutrients. 2021; 13(9):3222. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093222
Chicago/Turabian StyleTang, Zhaoxie, Yingan Ming, Miao Wu, Jiajia Jing, Suhua Xu, Hailin Li, and Yanna Zhu. 2021. "Effects of Caloric Restriction and Rope-Skipping Exercise on Cardiometabolic Health: A Pilot Randomized Controlled Trial in Young Adults" Nutrients 13, no. 9: 3222. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093222