
Quality of Life and Psychological Disorders in Coeliac Disease: A Prospective Multicentre Study

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Population and Study Design
2.2. Procedures and Clinical Characteristics of Patients
2.3. Assessment of the Compliance with a Gluten-Free Diet
2.4. Self-Administered Quality of Life and Psychological Symptoms Questionnaires
2.5. Statistical Analysis
2.6. Ethical Considerations and Good Clinical Practice
3. Results
3.1. Sociodemographic and Clinical Characteristics at Diagnosis
3.2. Clinical and Biochemical Response and Compliance with a GFD
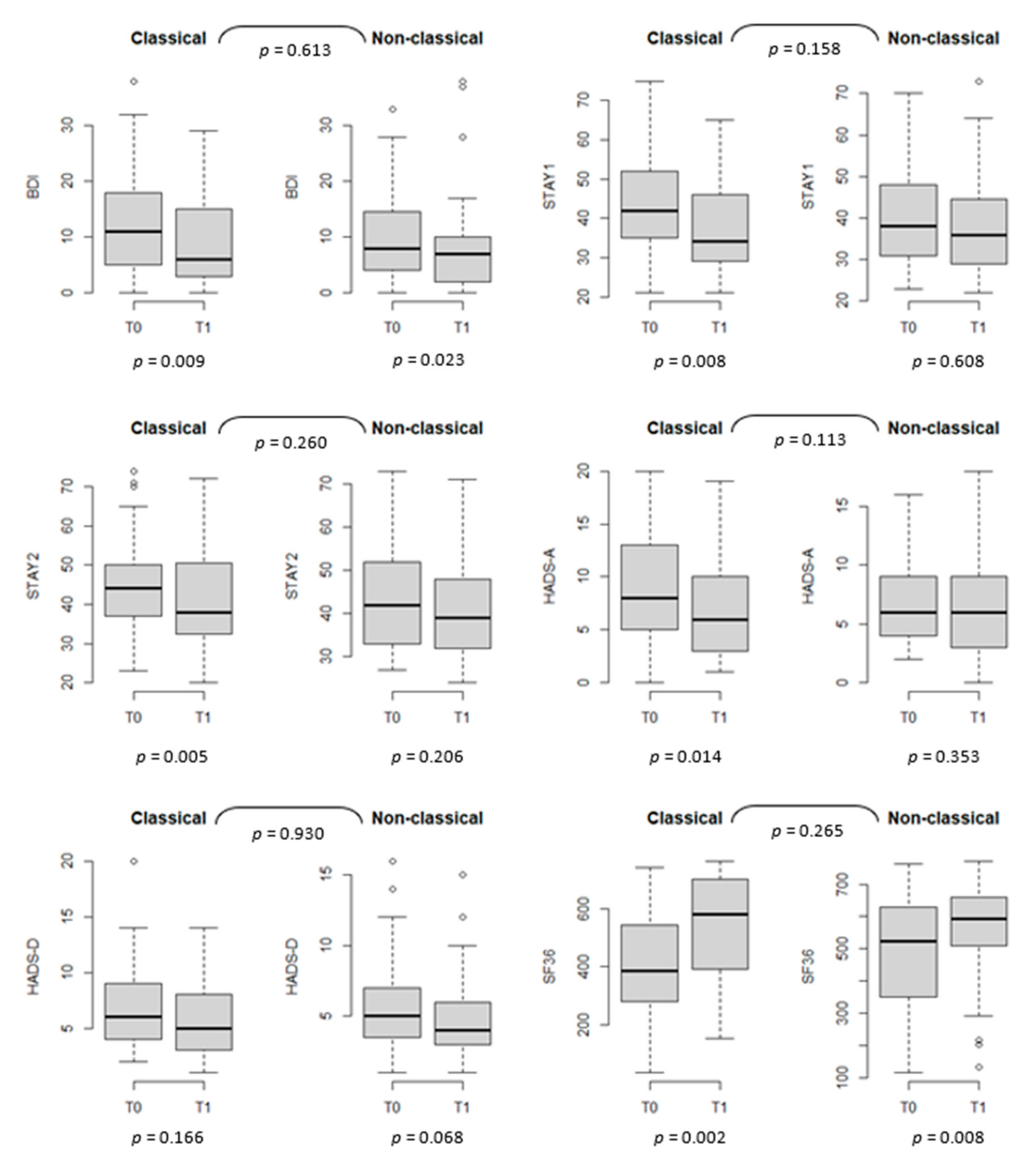
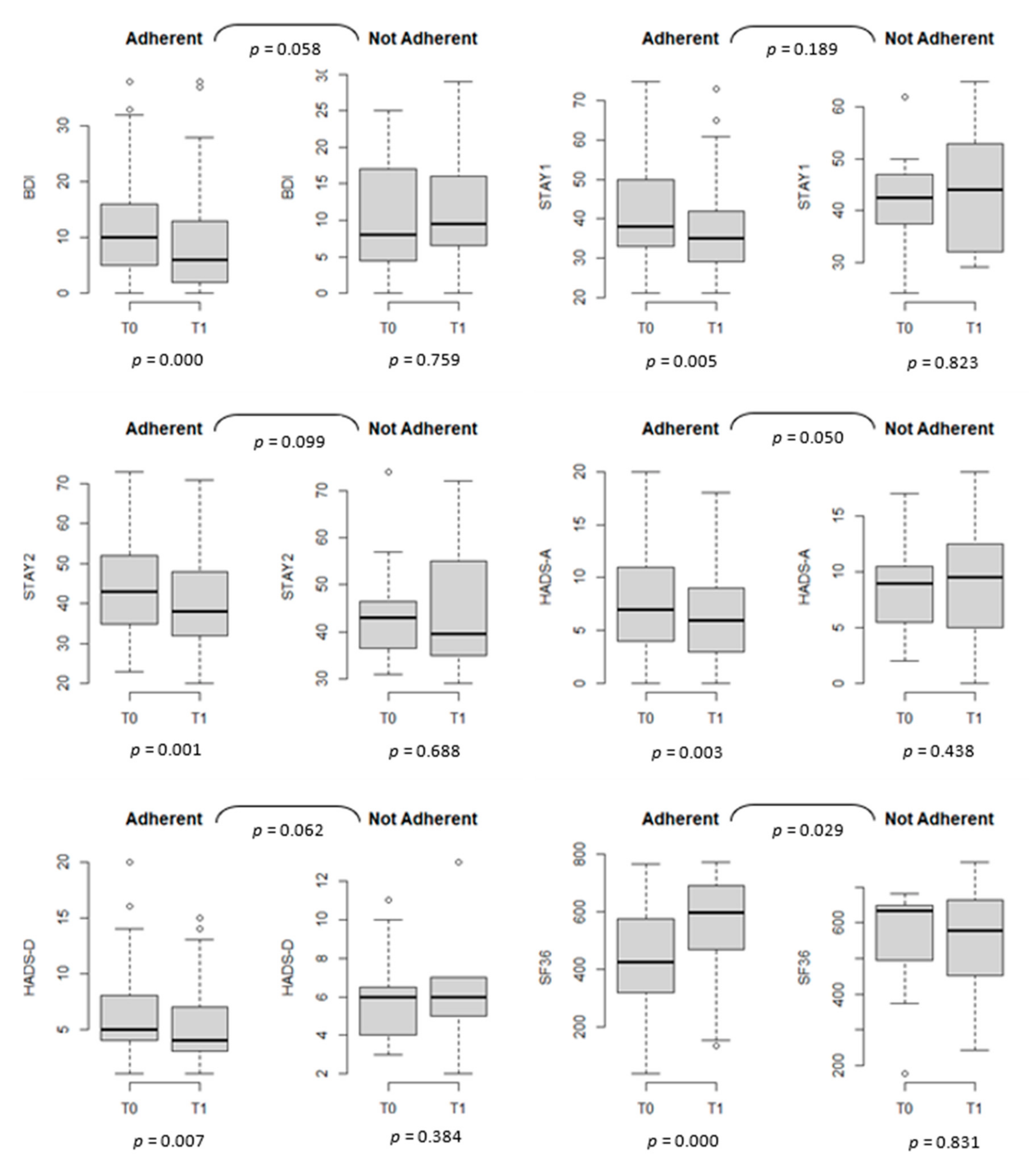
3.3. Psychological Aspects and QoL
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef]
- Zingone, F.; Swift, G.L.; Card, T.R.; Sanders, D.S.; Ludvigsson, J.F.; Bai, J.C. Psychological morbidity of celiac disease: A review of the literature. United Eur. Gastroenterol. J. 2015, 3, 136–145. [Google Scholar] [CrossRef]
- Nachman, F.; Maurino, E.; Vázquez, H.; Sfoggia, C.; Gonzalez, A.; Gonzalez, V.; del Campo, M.P.; Smecuol, E.; Niveloni, S.; Sugai, E. Quality of life in celiac disease patients: Prospective analysis on the importance of clinical severity at diagnosis and the impact of treatment. Dig. Liver Dis. 2009, 41, 15–25. [Google Scholar] [CrossRef]
- Mustalahti, K.; Lohiniemi, S.; Collin, P.; Vuolteenaho, N.; Laippala, P.; Maki, M. Gluten-free diet and quality of life in patients with screen-detected celiac disease. Eff. Clin. Pract. 2002, 5, 105–113. [Google Scholar]
- Johnston, S.D.; Rodgers, C.; Watson, R.G.P. Quality of life in screen-detected and typical coeliac disease and the effect of excluding dietary gluten. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1281. [Google Scholar] [CrossRef] [PubMed]
- Ukkola, A.; Mäki, M.; Kurppa, K.; Collin, P.; Huhtala, H.; Kekkonen, L.; Kaukinen, K. Diet improves perception of health and well-being in symptomatic, but not asymptomatic, patients with celiac disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2011, 9, 118–123.e111. [Google Scholar] [CrossRef]
- Nachman, F.; del Campo, M.P.; González, A.; Corzo, L.; Vázquez, H.; Sfoggia, C.; Smecuol, E.; Sánchez, M.I.P.; Niveloni, S.; Sugai, E. Long-term deterioration of quality of life in adult patients with celiac disease is associated with treatment noncompliance. Dig. Liver Dis. 2010, 42, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Barratt, S.M.; Leeds, J.S.; Sanders, D.S. Quality of Life in Coeliac Disease is Determined by Perceived Degree of Difficulty Adhering to a Gluten-Free Diet, not the Level of Dietary Adherence Ultimately Achieved. J. Gastrointestin. Liver Dis. 2011, 20, 241–245. [Google Scholar] [PubMed]
- Burger, J.P.W.; de Brouwer, B.; IntHout, J.; Wahab, P.J.; Tummers, M.; Drenth, J.P.H. Systematic review with meta-analysis: Dietary adherence influences normalization of health-related quality of life in coeliac disease. Clin. Nutr. 2017, 36, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Marsilio, I.; Canova, C.; D’Odorico, A.; Ghisa, M.; Zingone, L.; Lorenzon, G.; Savarino, E.V.; Zingone, F. Quality-of-Life Evaluation in Coeliac Patients on a Gluten-Free Diet. Nutrients 2020, 12, 2981. [Google Scholar] [CrossRef]
- Möller, S.P.; Hayes, B.; Wilding, H.; Apputhurai, P.; Tye-Din, J.A.; Knowles, S.R. Systematic review: Exploration of the impact of psychosocial factors on quality of life in adults living with coeliac disease. J. Psychosom. Res. 2021, 147, 110537. [Google Scholar] [CrossRef] [PubMed]
- Casellas, F.; Rodrigo, L.; Vivancos, J.L.; Riestra, S.; Pantiga, C.; Baudet, J.S.; Junquera, F.; Diví, V.P.; Abadia, C.; Papo, M.; et al. Factors that impact health-related quality of life in adults with celiac disease: A multicenter study. World J. Gastroenterol. 2008, 14, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Norström, F.; Lindholm, L.; Sandström, O.; Nordyke, K.; Ivarsson, A. Delay to celiac disease diagnosis and its implications for health-related quality of life. BMC Gastroenterol. 2011, 11, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usai, P.; Minerba, L.; Marini, B.; Cossu, R.; Spada, S.; Carpiniello, B.; Cuomo, R.; Boy, M. Case control study on health-related quality of life in adult coeliac disease. Dig. Liver Dis. 2002, 34, 547–552. [Google Scholar] [CrossRef]
- Zingone, F.; Secchettin, E.; Marsilio, I.; Valiante, F.; Zorzetto, V.; Cataudella, G.; D’Odorico, A.; Canova, C. Clinical features and psychological impact of celiac disease at diagnosis. Dig. Liver Dis. 2021. [Google Scholar] [CrossRef]
- Biagi, F.; Andrealli, A.; Bianchi, P.I.; Marchese, A.; Klersy, C.; Corazza, G.R. A gluten-free diet score to evaluate dietary compliance in patients with coeliac disease. Br. J. Nutr. 2009, 102, 882–887. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Sica, C.; Ghisi, M. The Italian Versions of the Beck Anxiety Inventory and the Beck Depression Inventory-II: Psychometric Properties and Discriminant Power. In Leading-Edge Psychological Tests and Testing Research; Nova Science Publishers, 2007; pp. 27–50. Available online: https://psycnet.apa.org/record/2007-13441-002 (accessed on 10 September 2021).
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011, 63 (Suppl. S11), S467–S472. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory STAI (Form Y) (“Self-Evaluation Questionnaire”). 1983. [Google Scholar]
- Pedrabissi, L.; Santinello, M. Verifica Della Validità Dello STAI Forma Y [Verification of the Validity of the STAI, Form Y]. In Giunti Organizzazioni Speciali; Charles, S., Ed.; 1989; pp. 11–14. Available online: https://psycnet.apa.org/record/1991-73411-001 (accessed on 10 September 2021).
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Annunziata, M.A.; Muzzatti, B.; Altoè, G. Defining hospital anxiety and depression scale (HADS) structure by confirmatory factor analysis: A contribution to validation for oncological settings. Ann. Oncol. 2011, 22, 2330–2333. [Google Scholar] [CrossRef]
- Ware, J.E.; Keller, S.D.; Kosinski, M. SF-36 Physical and Mental Health Summary Scales: A User’s Manual; The Health Institute, New England Medical Center: Boston, MA, USA, 1994. [Google Scholar]
- Corvaglia, L.; Catamo, R.; Pepe, G.; Lazzari, R.; Corvaglia, E. Depression in adult untreated celiac subjects: Diagnosis by the pediatrician. Am. J. Gastroenterol. 1999, 94, 839–843. [Google Scholar] [CrossRef]
- Zingone, F.; Siniscalchi, M.; Capone, P.; Tortora, R.; Andreozzi, P.; Capone, E.; Ciacci, C. The quality of sleep in patients with coeliac disease. Aliment. Pharmacol. Ther. 2010, 32, 1031–1036. [Google Scholar] [CrossRef] [Green Version]
- Siniscalchi, M.; Iovino, P.; Tortora, R.; Forestiero, S.; Somma, A.; Capuano, L.; Franzese, M.; Sabbatini, F.; Ciacci, C. Fatigue in adult coeliac disease. Aliment. Pharmacol. Ther. 2005, 22, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Addolorato, G. Anxiety but not depression decreases in coeliac patients after one-year gluten-free diet: A longitudinal study. Scand. J. Gastroenterol. 2001, 36, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Addolorato, G.; De Lorenzi, G.; Abenavoli, L.; Leggio, L.; Capristo, E.; Gasbarrini, G. Psychological support counselling improves gluten-free diet compliance in coeliac patients with affective disorders. Aliment. Pharmacol. Ther. 2004, 20, 777–782. [Google Scholar] [CrossRef]
- Häuser, W.; Janke, K.H.; Klump, B.; Gregor, M.; Hinz, A. Anxiety and depression in adult patients with celiac disease on a gluten-free diet. World J. Gastroenterol. 2010, 16, 2780. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, M.; Zingone, F.; Savarino, E.V.; D’Odorico, A.; Ciacci, C. COVID-19 pandemic perception in adults with celiac disease: An impulse to implement the use of telemedicine. Dig. Liver Dis. 2020, 52, 1071–1075. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | N° Patients Included at T1 (n = 93) | N° Patients Included at T2 (n = 55) |
|---|---|---|
| n (%) | n (%) | |
| Sex | ||
| Females | 76 (81.72) | 47 (85.45) |
| Males | 17 (18.28) | 8 (14.55) |
| Civil Status | ||
| Not married | 50 (54.35) | 26 (48.15) |
| Married | 39 (42.39) | 27 (50.0) |
| Divorced | 2 (2.17) | 0 (0) |
| Widowed | 1 (1.09) | 1 (1.85) |
| Education | ||
| Degree/PhD | 27 (29.35) | 17 (31.5) |
| Upper secondary education | 51 (55.43) | 30 (55.6) |
| Lower secondary education | 13 (14.13) | 7 (12.9) |
| Primary education | 1 (1.09) | 0 (0) |
| Type of employment | ||
| Employee | 57 (61.96) | 35 (64.8) |
| Self-employed | 8 (8.7) | 5 (9.3) |
| Housewife | 9 (9.78) | 6 (11.1) |
| Unemployed | 4 (4.35) | 2 (3.7) |
| Retired | 2 (2.17) | 2 (3.7) |
| Student | 12 (13.04) | 4 (7.4) |
| Smoking habit | ||
| No | 75 (80.65) | 48 (87.3) |
| Yes | 10 (10.75) | 4 (7.2) |
| Ex smoker | 8 (8.6) | 3 (5.5) |
| Who suggested the diagnostic path to patients? | ||
| Patient/Family/Friends | 13 (13.98) | 5 (9.1) |
| General practitioner | 35 (37.63) | 26 (47.3) |
| Gastroenterologist | 13 (13.98) | 7 (12.7) |
| Other specialist physician | 32 (34.41) | 17 (30.9) |
| With family affected by CeD | ||
| No | 74 (79.57) | 46 (83.6) |
| Yes | 19 (20.43) | 9 (16.4) |
| Cohabitation with celiac patients | ||
| No | 85 (92.39) | 52 (96.3) |
| Yes | 7 (7.61) | 2 (3.7) |
| Age, years | ||
| mean (SD) | 37.33 (13.21) | 39.64 (13.73) |
| min-max | 16.36–78.32 | 19.44–78.32 |
| Median (Q1–Q3) | 34.88 (27.26–45.77) | 42.77 (27.53–51.13) |
| BMI | ||
| mean (SD) | 22.31 (3.49) | 22.79 (3.53) |
| min-max | 16.94–36.06 | 18.42–36.06 |
| Median (Q1–Q3) | 21.54 (20.01–24.1) | 22.06 (20.26–24.14) |
| Type of CeD * | ||
| Classical | 46 (49.46) | 26 (47.3) |
| Non classical | 47 (50.54) | 29 (52.7) |
| Non classical with anemia | 19 (40.4) | 9 (31.0) |
| T0 | T1 | p-Value * | |||||
|---|---|---|---|---|---|---|---|
| Min–Max | Median | 1st–3rd Qu. | Min–Max | Median | 1st–3rd Qu. | ||
| BDI | 0.0–38.0 | 9.0 | 5.0–16.5 | 0.0–38.0 | 6.0 | 2.0–13.5 | 0.001 |
| STAI 1 | 21.0–75.0 | 39.0 | 32.8–49.3 | 21.0–73.0 | 36.0 | 29.0–44.8 | 0.023 |
| STAI 2 | 23.0–74.0 | 43.0 | 34.8–51.3 | 20.0–72.0 | 39.0 | 32.0–49.0 | 0.004 |
| HADS-A | 0.0–20.0 | 7.0 | 4.0–11.0 | 0.0–19.0 | 6.0 | 3.0–10.0 | 0.019 |
| HADS-D | 1.0–20.0 | 6.0 | 4.0–8.0 | 1.0–15.0 | 4.0 | 3.0–7.0 | 0.024 |
| SF36 | 35.5–764.0 | 468.1 | 326.0–587.1 | 133.0–772.0 | 592.5 | 470.0–687.5 | 0.000 |
| T0 | T1 | T2 | p-Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min–Max | Median | 1st–3rd Qu. | Min–Max | Median | 1st–3rd Qu. | Min–Max | Median | 1st–3rd Qu. | ||
| BDI | 0.0–38.0 | 8.0 | 5.0–16.5 | 0.0–38.0 | 6.0 | 2.0–11.0 | 0.0–28.0 | 4.0 | 1.0–8.0 | 0.001 |
| STAI 1 | 21.0–72.0 | 38.0 | 31.0–50.5 | 21.0–65.0 | 34.0 | 28.0–41.8 | 20.0–60.0 | 32.0 | 28.0–39.0 | 0.063 |
| STAI 2 | 23.0–73.0 | 43.0 | 34.0–51.5 | 22.0–65.0 | 38.0 | 31.8–45.8 | 20.0–67.0 | 36.5 | 30.3–44.0 | 0.000 |
| HADS-A | 0.0–20.0 | 7.0 | 4.0–11.0 | 0.0–18.0 | 4.5 | 3.0–8.8 | 0.0–15.0 | 4.0 | 3.0–7.0 | 0.000 |
| HADS-D | 2.0–20.0 | 5.0 | 4.0–8.0 | 1.0–15.0 | 4.0 | 3.0–7.0 | 1.0–14.0 | 4.0 | 3.0–6.8 | 0.001 |
| SF36 | 35.5–764.0 | 418.8 | 294.8–560.5 | 133.0–772.0 | 608.2 | 472.8–696.5 | 227.8–791.0 | 612.8 | 480.7–704.2 | 0.000 |
| BDI | STAI 1 | STAI 2 | ||||||||
| Predictor | n (%) * | OR (CI 95%) | aOR (CI 95%) | n (%) * | OR (CI 95%) | aOR (CI 95%) | n (%) * | OR (CI 95%) | aOR (CI 95%) | |
| adherence to GFD | non adherent | 8/12 (67) | 3.57 (0.99; 12.93) | 4.05 (1.09; 14.99) | 7/12 (58) | 1.72 (0.50; 5.89) | 1.68 (0.48; 5.83) | 8/12 (67) | 3.57 (0.99; 12.93) | 3.89 (1.04; 14.47) |
| Adherent | 28/78 (36) | 35/78 (45) | 28/78 (36) | |||||||
| type of CeD | non classical CeD | 20/47 (43) | 1.05 (0.46; 2.40) | 0.94 (0.39; 2.26) | 25/47 (53) | 1.48 (0.65; 3.35) | 1.41 (0.61; 3.28) | 21/47 (45) | 1.26 (0.55; 2.87) | 1.08 (0.45; 2.60) |
| classical CeD | 19/46 (41) | 20/46 (43) | 18/46 (39) | |||||||
| Age | 35+ | 24/54 (44) | 1.28 (0.55; 2.96) | 1.18 (0.48; 2.87) | 27/54 (50) | 1.17 (0.51; 2.66) | 1.08 (0.46; 2.53) | 21/54 (39) | 0.74 (0.32; 1.71) | 0.64 (0.26; 1.54) |
| 16–34 | 15/39 (38) | 18/39 (46) | 18/39 (46) | |||||||
| Gender | M | 9/17 (53) | 1.73 (0.60; 4.97) | 2.28 (0.76; 6.83) | 8/17 (47) | 0.94 (0.33; 2.69) | 1.07 (0.36; 3.13) | 8/17 (47) | 1.29 (0.45; 3.71) | 1.57 (0.52; 4.71) |
| F | 30/76 (39) | 37/76 (49) | 31/76 (41) | |||||||
| HADS-A | HADS-D | SF36 | ||||||||
| Predictor | n (%) * | OR (CI 95%) | aOR (CI 95%) | n (%) * | OR (CI 95%) | aOR (CI 95%) | n (%) * | OR (CI 95%) | aOR (CI 95%) | |
| adherence to GFD | non adherent | 9/12 (75) | 4.31 (1.08; 17.18) | 4.14 (1.03; 16.75) | 9/12 (75) | 3.69 (0.93; 14.66) | 3.80 (0.94; 15.35) | 6/12 (50) | 2.54 (0.47; 8.75) | 2.87 (0.81; 10.17) |
| Adherent | 32/78 (41) | 35/78 (45) | 22/78 (28) | |||||||
| type of CeD | non classical CeD | 25/47 (53) | 1.61 (0.71; 3.67) | 1.58 (0.66; 3.67) | 22/47 (47) | 0.81 (0.36; 1.82) | 0.80 (0.34; 1.87) | 15/47 (32) | 1.07 (0.44; 2.58) | 0.90 (0.36; 2.26) |
| classical CeD | 19/46 (41) | 24/46 (52) | 14/46 (30) | |||||||
| Age | 35+ | 25/54 (53) | 1.55 (0.67; 3.56) | 1.46 (0.60; 3.52) | 28/54 (52) | 1.26 (0.55; 2.87) | 1.19 (0.50; 2.81) | 15/54 (28%) | 0.69 (0.28; 1.66) | 0.68 (0.27; 1.73) |
| 16–34 | 19/39 (41) | 18/39 (46) | 14/39 (36%) | |||||||
| Gender | M | 7/17 (41) | 0.74 (0.25; 2.14) | 0.92 (0.30; 2.8) | 8/17 (47) | 0.89 (0.31; 2.55) | 1.05 (0.36; 3.09) | 7/17 (41) | 1.72 (0.58; 5.09) | 1.88 (0.61; 5.79) |
| F | 37/76 (49) | 38/76 (50) | 22/76 (29) | |||||||
| GI symptoms | EI symptoms | |||||||||
| Predictor | n (%) * | OR (CI 95%) | aOR (CI 95%) | n (%) * | OR (CI 95%) | aOR (CI 95%) | ||||
| adherence to GFD | non adherent | 4/12 (33) | 1.36 (0.37; 4.98) | 1.26 (0.32; 4.89) | 4/12 (33) | 2.29 (0.60; 8.66) | 2.31 (0.57; 9.46) | |||
| Adherent | 21/78 (27) | 14/78 (18) | ||||||||
| type of CeD | non classical CeD | 17/47 (36) | 2.70 (1.02; 7.08) | 2.68 (1.00; 7.14) | 12/47 (26) | 2.29 (0.78; 6.73) | 2.11 (0.69; 6.40) | |||
| classical CeD | 8/46 (17) | 6/46 (13) | ||||||||
| Age | 35+ | 12/54 (22) | 0.57 (0.23; 1.44) | 0.67 (0.26; 1.76) | 7/54 (13) | 0.38 (0.13; 1.09) | 0.43 (0.14; 1.28) | |||
| 16–34 | 13/39 (33) | 11/39 (28) | ||||||||
| Gender | M | 5/17 (29) | 1.17 (0.36; 3.73) | 1.06 (0.32; 3.53) | 4/17 (24) | 1.36 (0.39; 4.81) | 1.29 (0.34; 4.86) | |||
| F | 20/76 (26) | 14/76 (18) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canova, C.; Rosato, I.; Marsilio, I.; Valiante, F.; Zorzetto, V.; Cataudella, G.; D’Odorico, A.; Zingone, F. Quality of Life and Psychological Disorders in Coeliac Disease: A Prospective Multicentre Study. Nutrients 2021, 13, 3233. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093233
Canova C, Rosato I, Marsilio I, Valiante F, Zorzetto V, Cataudella G, D’Odorico A, Zingone F. Quality of Life and Psychological Disorders in Coeliac Disease: A Prospective Multicentre Study. Nutrients. 2021; 13(9):3233. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093233
Chicago/Turabian StyleCanova, Cristina, Isabella Rosato, Ilaria Marsilio, Flavio Valiante, Valerio Zorzetto, Giovanni Cataudella, Anna D’Odorico, and Fabiana Zingone. 2021. "Quality of Life and Psychological Disorders in Coeliac Disease: A Prospective Multicentre Study" Nutrients 13, no. 9: 3233. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093233