
Vitamin D Status Presents Different Relationships with Severity in Metabolic-Associated Fatty Liver Disease Patients with or without Hepatitis B Infection

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Clinical and Laboratory Parameters
2.3. Radiology Assessments
2.4. Histopathological Evaluation
2.5. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Factors Associated with VitD Deficiency
3.3. Correlation between VitD and Severity of Metabolic, Steatosis and Liver Injuries
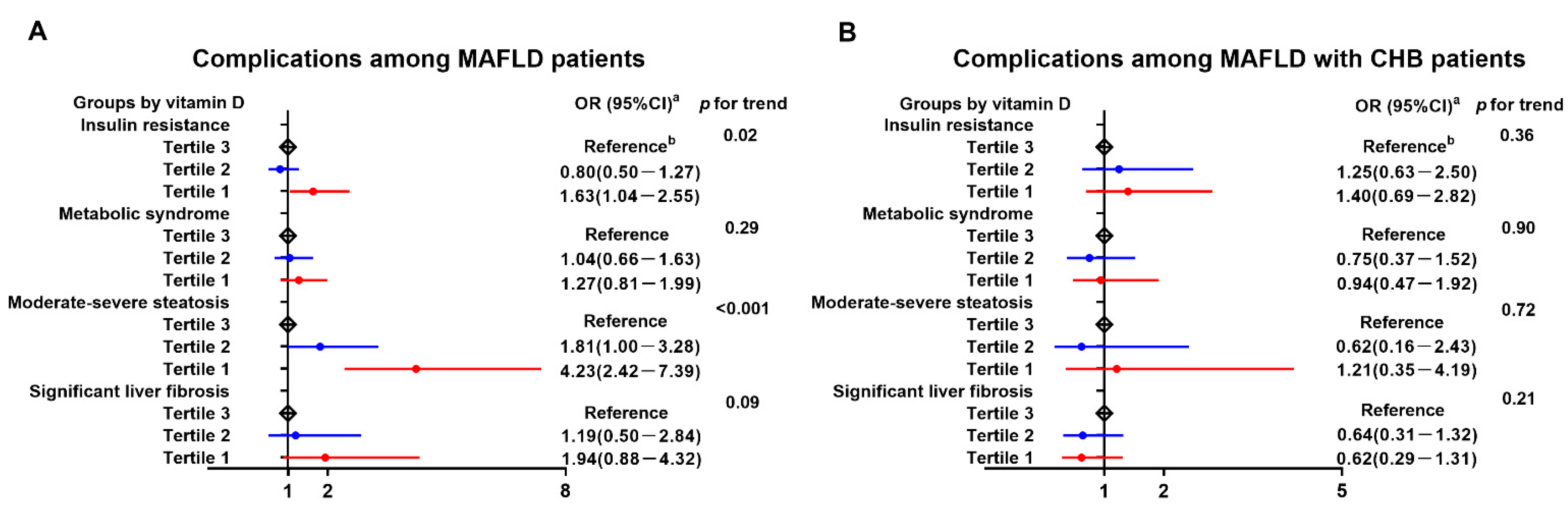
3.4. Dose-Dependent Relationship of Serum VitD Levels with Disease Severity among Different Groups
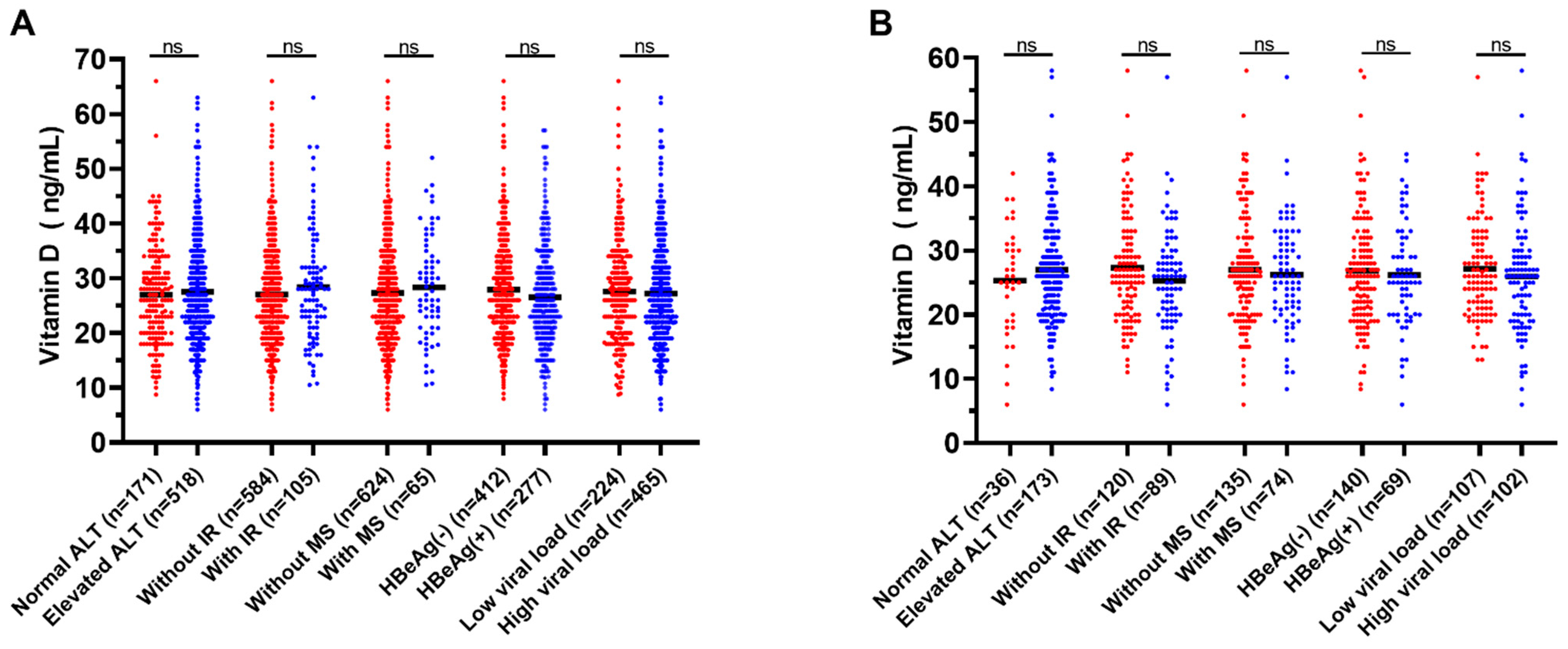
3.5. Serum VitD Levels and Different Infection Statuses of CHB Patients with or without MAFLD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the global burden of chronic liver diseases from 2012 to 2017: The Growing Impact of NAFLD. Hepatology 2020, 72, 1605–1616. [Google Scholar] [CrossRef] [PubMed]
- Ayada, I.; van Kleef, L.A.; Alferink, L.J.M.; Li, P.; de Knegt, R.J.; Pan, Q. Systematically comparing epidemiological and clinical features of MAFLD and NAFLD by meta-analysis: Focusing on the non-overlap groups. Liver Int. 2022, 42, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar] [CrossRef]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and extraskeletal actions of vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymczak-Pajor, I.; Drzewoski, J.; Śliwińska, A. The molecular mechanisms by which vitamin D prevents insulin resistance and associated disorders. Int. J. Mol. Sci. 2020, 21, 6644. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, W.; Jiang, W.; Li, C.; Guo, J.; Xun, Y. Low vitamin D levels are associated with high viral loads in patients with chronic hepatitis B: A systematic review and meta-analysis. BMC Gastroenterol. 2019, 19, 84. [Google Scholar] [CrossRef] [Green Version]
- Elangovan, H.; Chahal, S.; Gunton, J.E. Vitamin D in liver disease: Current evidence and potential directions. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 907–916. [Google Scholar] [CrossRef]
- Liu, T.; Xu, L.; Chen, F.; Zhou, Y. Association of serum vitamin D level and nonalcoholic fatty liver disease: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 140–147. [Google Scholar] [CrossRef]
- Guo, X.; Wang, C.; Yang, T.; Li, S.; Li, K.; Li, D. Vitamin D and non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Food Funct. 2020, 11, 7389–7399. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Chan, H.Y.; Tse, C.H.; Chim, A.M.; Lo, A.O.; Wong, V.W. Adverse effects of vitamin D deficiency on outcomes of patients with chronic hepatitis B. Clin. Gastroenterol. Hepatol. 2015, 13, 783–790.e1. [Google Scholar] [CrossRef] [PubMed]
- EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398.
- Eslam, M.; Sarin, S.K.; Wong, V.W.; Fan, J.; Kawaguchi, T.; Ahn, S.H.; Zheng, M.; Shiha, G.; Yilmaz, Y.; Gani, R.; et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol. Int. 2020, 14, 889–919. [Google Scholar] [CrossRef]
- Park, S.; Buranakitjaroen, P.; Chen, C.; Chia, Y.C.; Divinagracia, R.; Hoshide, S.; Shin, J.; Siddique, S.; Sison, J.; Soenarta, A.A.; et al. Expert panel consensus recommendations for home blood pressure monitoring in Asia: The Hope Asia Network. J. Hum. Hypertens. 2018, 32, 249–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed] [Green Version]
- Prati, D.; Taioli, E.; Zanella, A.; Della Torre, E.; Butelli, S.; Del Vecchio, E.; Vianello, L.; Zanuso, F.; Mozzi, F.; Milani, S.; et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann. Intern. Med. 2002, 137, 1–10. [Google Scholar] [CrossRef]
- Shao, C.; Ye, J.; Li, F.; Lin, Y.; Wu, T.; Wang, W.; Feng, S.; Zhong, B. Early predictors of cardiovascular disease risk in nonalcoholic fatty liver disease: Non-obese versus obese patients. Dig. Dis. Sci. 2020, 65, 1850–1860. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Ballestri, S.; Lonardo, A.; Romagnoli, D.; Carulli, L.; Losi, L.; Day, C.P.; Loria, P. Ultrasonographic fatty liver indicator, a novel score which rules out NASH and is correlated with metabolic parameters in NAFLD. Liver Int. 2012, 32, 1242–1252. [Google Scholar] [CrossRef]
- Dong, Z.; Luo, Y.; Zhang, Z.; Cai, H.; Li, Y.; Chan, T.; Wu, L.; Li, Z.; Feng, S. MR quantification of total liver fat in patients with impaired glucose tolerance and healthy subjects. PLoS ONE 2014, 9, e111283. [Google Scholar] [CrossRef] [Green Version]
- Gu, J.; Liu, S.; Du, S.; Zhang, Q.; Xiao, J.; Dong, Q.; Xin, Y. Diagnostic value of MRI-PDFF for hepatic steatosis in patients with non-alcoholic fatty liver disease: A meta-analysis. Eur. Radiol. 2019, 29, 3564–3573. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Huang, Y.; Sun, Y.; Shao, C.; Zhang, S.; Wang, W.; Zhong, B. Dynamic monitoring with shear wave elastography predicts outcomes of chronic hepatitis B patients with decompensated cirrhosis. Ann. Transl. Med. 2021, 9, 1613. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, L.; Pan, S.; Wu, X.; Yin, X. No significant association between vitamin D and nonalcoholic fatty liver disease in a Chinese population. Dig. Dis. Sci. 2013, 58, 2376–2382. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Rotundo, L.; Kothari, N.; Kim, S.H.; Pyrsopoulos, N. Vitamin D is associated with severity and mortality of non-alcoholic fatty liver disease: A US population-based study. J. Clin. Transl. Hepatol. 2017, 5, 185–192. [Google Scholar] [CrossRef]
- Barchetta, I.; Angelico, F.; Del Ben, M.; Baroni, M.G.; Pozzilli, P.; Morini, S.; Cavallo, M.G. Strong association between non- alcoholic fatty liver disease (NAFLD) and low 25(OH) vitamin D levels in an adult population with normal serum liver enzymes. BMC Med. 2011, 9, 85. [Google Scholar] [CrossRef]
- Pirgon, O.; Cekmez, F.; Bilgin, H.; Eren, E.; Dundar, B. Low 25-hydroxyvitamin D level is associated with insulin sensitivity in obese adolescents with non-alcoholic fatty liver disease. Obes. Res. Clin. Pract. 2013, 7, e275–e283. [Google Scholar] [CrossRef]
- Chen, L.; Chien, C.H.; Kuo, S.F.; Yu, C.Y.; Lin, C.L.; Chien, R.N. Low vitamin D level was associated with metabolic syndrome and high leptin level in subjects with nonalcoholic fatty liver disease: A community-based study. BMC Gastroenterol. 2019, 19, 126. [Google Scholar] [CrossRef]
- Lim, H.S.; Kim, T.H.; Lee, H.H.; Kim, S.K.; Lee, B.; Park, Y.H. Relationship between serum 25-hydroxyvitamin D concentration and risk of metabolic syndrome in patients with fatty liver. J. Bone Metab. 2017, 24, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Jaruvongvanich, V.; Ahuja, W.; Sanguankeo, A.; Wijarnpreecha, K.; Upala, S. Vitamin D and histologic severity of nonalcoholic fatty liver disease: A systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 618–622. [Google Scholar] [CrossRef]
- Arai, T.; Atsukawa, M.; Tsubota, A.; Koeda, M.; Yoshida, Y.; Okubo, T.; Nakagawa, A.; Itokawa, N.; Kondo, C.; Nakatsuka, K.; et al. Association of vitamin D levels and vitamin D-related gene polymorphisms with liver fibrosis in patients with biopsy-proven nonalcoholic fatty liver disease. Dig. Liver Dis. 2019, 51, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Kallman, J.B.; Bai, C.; Pawloski, L.; Gewa, C.; Arsalla, A.; Sabatella, M.E.; Younossi, Z.M. Nutritional assessments of patients with nonalcoholic fatty liver disease. Obes. Surg. 2010, 20, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.S.; Liu, W.; Chao, Y.; Lin, H.; Tseng, T.C.; Wang, C.; Chen, D.; Kao, J.H. Adipocytokines and liver fibrosis stages in patients with chronic hepatitis B virus infection. Hepatol. Int. 2015, 9, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, A.; Williams, J.S.; Forman, J.P. The independent association between 25-hydroxyvitamin D and adiponectin and its relation with BMI in two large cohorts: The NHS and the HPFS. Obesity 2012, 20, 186–191. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | HC (N = 360) | CHB (N = 689) | MAFLD (N = 529) | MAFLD with CHB (N = 209) |
|---|---|---|---|---|
| Age (years) | 45.3 ± 10.5 | 43.7 ± 11.4 | 44.3 ± 11.8 | 43.8 ± 10.5 |
| Male, n (%) | 249 (69.2%) | 472 (68.5%) | 388 (73.3%) | 157 (75.1%) |
| BMI (kg/m2) | 23.0 ± 3.1 | 22.1 ± 2.9 ** a | 26.9 ± 3.3 ** a ** b | 26.4 ± 3.3 ** a ** b |
| WC (cm) | 78.5 ± 4.3 | 78.2 ± 8.3 | 90.0 ± 7.4 ** a ** b | 89.2 ± 8.2 ** a ** b |
| WHR | 0.84 ± 0.03 | 0.84 ± 0.06 | 0.90 ± 0.04 ** a ** b | 0.89 ± 0.05 ** a ** b |
| Hypertension 2, n (%) | 46 (12.8%) | 176 (25.6%) * a | 196 (37.1%) * a * b | 81 (38.8%) * a * b |
| Cold season 2, n (%) | 111 (30.8%) | 369 (53.6%) * a | 190 (35.9%) * b | 109 (52.2%) * a * c |
| VitD (ng/mL) | 29.0 ± 9.5 | 27.4 ± 9.5 * a | 24.4 ± 8.2 ** a ** b | 26.7 ± 8.5 * a * c |
| CHOL (mmol/L) | 5.0 ± 1.0 | 4.8 ± 1.0 * a | 5.6 ± 1.1 ** a ** b | 5.3 ± 1.1*a ** b * c |
| TG (mmol/L) | 1.0 (0.8, 1.4) | 0.9 (0.7, 1.2) ** a | 1.9 (1.4, 2.6) ** a ** b | 1.4 (1.0, 2.0) ** a ** b ** c |
| HDL-C (mmol/L) | 1.3 ± 0.3 | 1.3 ± 0.3 | 1.2 ± 0.3 ** a **b | 1.2 ± 0.3 ** a ** b |
| LDL-C (mmol/L) | 3.1 ± 0.7 | 3.0 ± 0.8 * a | 3.5 ± 0.8 **a ** b | 3.4 ± 0.9 * a ** b * c |
| FBG (mmol/L) | 4.7 (4.4, 5.1) | 4.8 (4.4, 5.2) | 5.1 (4.7, 5.7) ** a ** b | 4.9 (4.5, 5.5) ** a * b * c |
| HOMA-IR | 1.3 (1.0, 1.7) | 1.3 (0.9, 2.0) | 2.4 (1.6, 3.4) ** a ** b | 2.3 (1.5, 3.3) ** a ** b |
| UA (μmol/L) | 365 ± 94 | 344 ± 96 * a | 435 ± 103 ** a ** b | 404 ± 92 ** a ** b * c |
| ALT (U/L) | 18.0 (13.3, 24.0) | 45.0 (26.0, 86.5) ** a | 42.0 (25.0, 75.5) ** a | 49.0 (31.0, 80.5) ** a |
| AST (U/L) | 21.0 (18.0, 25.0) | 38.0 (26.0, 65.0) ** a | 29.0 (22.0, 43.8) ** a ** b | 34.0 (26.0, 49.0) ** a ** c |
| GGT (U/L) | 20.5 (15.0, 29.0) | 28.0 (19.0, 50.0) ** a | 42.0 (29.0, 73.0) ** a ** b | 36.5 (24.8, 69.3) ** a ** b |
| ALP (U/L) | 70.0 (61.0, 80.0) | 79.0 (66.0, 94.0) ** a | 76.0 (67.0, 89.0) ** a | 75.0 (65.0, 89.0) ** a |
| ALB (g/L) | 43.6 ± 3.3 | 43.4 ± 4.1 | 45.1 ± 3.0 ** a ** b | 44.6 ± 3.2 * a ** b |
| TB (μmol/L) | 12.9 (10.4, 16.7) | 14.9 (11.6, 20.4) ** a | 13.5 (10.8, 16.8) ** b | 13.9 (11.2, 17.9) |
| Hs-CRP (mg/L) | 0.7 (0.4, 1.1) | 0.6 (0.3, 1.0) * a | 1.4 (0.7, 3.0) **a ** b | 0.8 (0.4, 1.5) ** b ** c |
| Characteristics | HC (N = 360) | CHB (N = 689) | MAFLD (N = 529) | MAFLD with CHB (N = 209) | p |
|---|---|---|---|---|---|
| Non-alcoholic drinker 2 | 73 (20.3%) a | 139 (20.2%) a | 163 (30.8%) b | 70 (33.5%) b | <0.001 |
| Smoker 2 | 25 (6.8%) a | 103 (14.9%) b | 101 (19.1%) b | 37 (17.7%) b | <0.001 |
| Low education level 2 | 194 (54.0%) abc | 376 (54.6%) c | 225 (42.5%) b | 126 (60.3%) ac | <0.001 |
| Time outside between sunrise and sunset | <0.001 | ||||
| <1 h/day | 121 (33.6%) a | 271 (39.4%) ab | 228 (43.1%) b | 71 (34.0%) ab | |
| 1–2 h/day | 113 (31.4%) ab | 169 (24.5%) b | 183 (34.6%) a | 63 (30.1%) ab | |
| ≥2 h/day | 126 (35.0%) a | 249 (36.1%) a | 118 (22.3%) b | 75 (35.9%) a | |
| Sun protection | <0.001 | ||||
| Usually (≥50%) | 31 (8.6%) a | 153 (22.2%) b | 51 (9.6%) ac | 33 (15.9%) bc | |
| Sometimes (<50%) | 24 (6.7%) a | 143 (20.7%) b | 100 (18.9%) b | 28 (13.5%) b | |
| Never | 305 (84.7%) a | 393 (57.1%) b | 378 (71.5%) c | 147(70.5%) c | |
| Frequency of physical activity | <0.001 | ||||
| Never | 101 (28.1%) a | 256 (37.2%) b | 250 (47.3%) c | 109 (52.2%) c | |
| 1/week | 15 (4.2%) a | 57 (8.3%) a | 38 (7.2%) a | 17 (8.2%) a | |
| 2–4/week | 137 (38.1%) a | 241 (35.0%) a | 146 (27.6%) b | 50 (23.7%) b | |
| 5–6/week | 26 (7.2%) a | 82 (11.9%) a | 60 (11.3%) a | 25 (12.1%) a | |
| Every day | 81 (22.5%) a | 53 (7.7%) b | 35 (6.6%) b | 8 (3.9%) b | |
| Duration of physical activity | <0.001 | ||||
| Never | 101 (28.1%) a | 256 (37.2%) b | 250 (47.3%) c | 109 (52.2%) c | |
| <3 h/week | 92 (25.6%) a | 263 (38.2%) b | 165 (31.2%) ab | 61 (29.0%) ab | |
| ≥3 h/week | 167 (46.4%) a | 170 (24.7%) b | 114 (21.6%) b | 39 (18.8%) b | |
| Fatty Fish (≥1 x/week) | 100 (27.8%) a | 192 (27.9%) a | 154 (29.1%) a | 50 (23.7%) a | 0.53 |
| Liver (≥1 x/week) | 77 (21.4%) a | 94 (13.7%) b | 86 (16.3%) ab | 21 (10.1%) b | 0.001 |
| Margarine (≥1 x/week) | 29 (8.1%) a | 10 (1.5%) b | 7 (1.3%) b | 2 (1.0%) b | <0.001 |
| Eggs | <0.001 | ||||
| Never | 108 (30.0%) a | 196 (28.5%) a | 62 (11.7%) b | 65 (30.9%) a | |
| 1–6 units/week | 95 (26.4%) a | 372 (54.0%) b | 303 (57.3%) b | 102 (48.8%) b | |
| ≥7 units/week | 157 (43.6%) a | 121 (17.5%) b | 164 (31.0%) c | 42 (20.3%) b | |
| Milk | <0.001 | ||||
| Never | 184 (51.1%) a | 503 (73.0%) b | 326 (61.6%) c | 142 (68.1%) bc | |
| Sometimes (≥1 x/week) | 82 (22.8%) a | 121 (17.5%) a | 118 (22.3%) a | 43 (20.3%) a | |
| Every day | 94 (26.1%) a | 65 (9.5%) b | 85 (16.1%) c | 24 (11.6%) bc |
| Liver Fat Content 1 | ||||||
|---|---|---|---|---|---|---|
| MAFLD | MAFLD with CHB | |||||
| β | 95% CI | p | β | 95% CI | p | |
| Unadjusted | −0.352 | (−0.417, −0.287) | <0.001 | −0.016 | (−0.097, 0.064) | 0.69 |
| Model 1 2 | −0.276 | (−0.344, −0.209) | <0.001 | - | - | - |
| Model 2 3 | −0.280 | (−0.346, −0.214) | <0.001 | - | - | - |
| Model 3 4 | −0.353 | (−0.434, −0.272) | <0.001 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, L.; Ye, J.; Shao, C.; Lin, Y.; Sun, Y.; Feng, S.; Wang, W.; Zhong, B. Vitamin D Status Presents Different Relationships with Severity in Metabolic-Associated Fatty Liver Disease Patients with or without Hepatitis B Infection. Nutrients 2022, 14, 2114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102114
Luo L, Ye J, Shao C, Lin Y, Sun Y, Feng S, Wang W, Zhong B. Vitamin D Status Presents Different Relationships with Severity in Metabolic-Associated Fatty Liver Disease Patients with or without Hepatitis B Infection. Nutrients. 2022; 14(10):2114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102114
Chicago/Turabian StyleLuo, Ling, Junzhao Ye, Congxiang Shao, Yansong Lin, Yanhong Sun, Shiting Feng, Wei Wang, and Bihui Zhong. 2022. "Vitamin D Status Presents Different Relationships with Severity in Metabolic-Associated Fatty Liver Disease Patients with or without Hepatitis B Infection" Nutrients 14, no. 10: 2114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102114