
Personalised Nutritional Recommendations Based on Individual Post-Prandial Glycaemic Responses Improve Glycaemic Metrics and PROMs in Patients with Type 2 Diabetes: A Real-World Assessment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Study Design
2.3. Statistical Analysis of Baseline Participant Characteristics
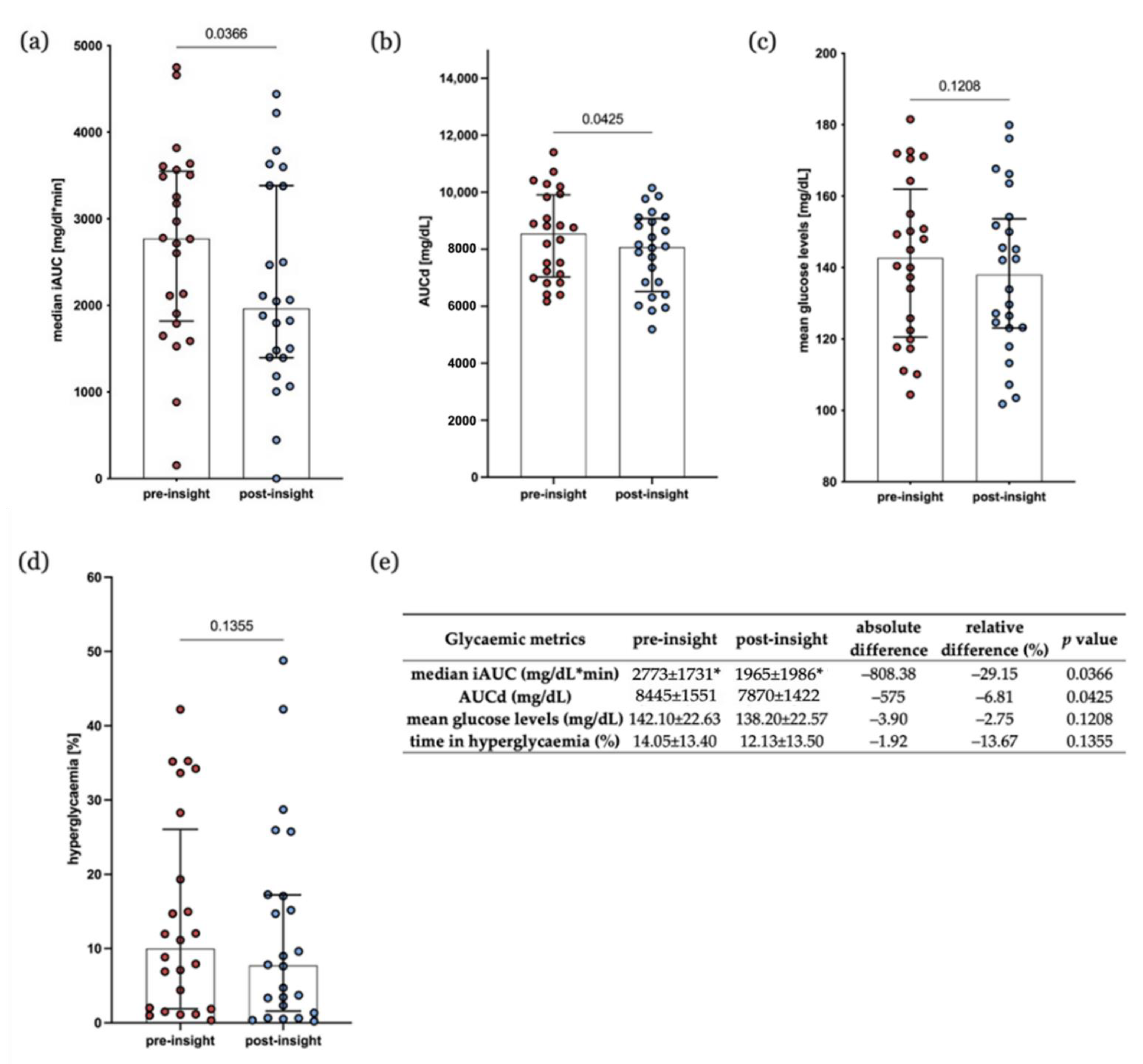
2.4. Statistical Analysis of Glycaemic Metrics
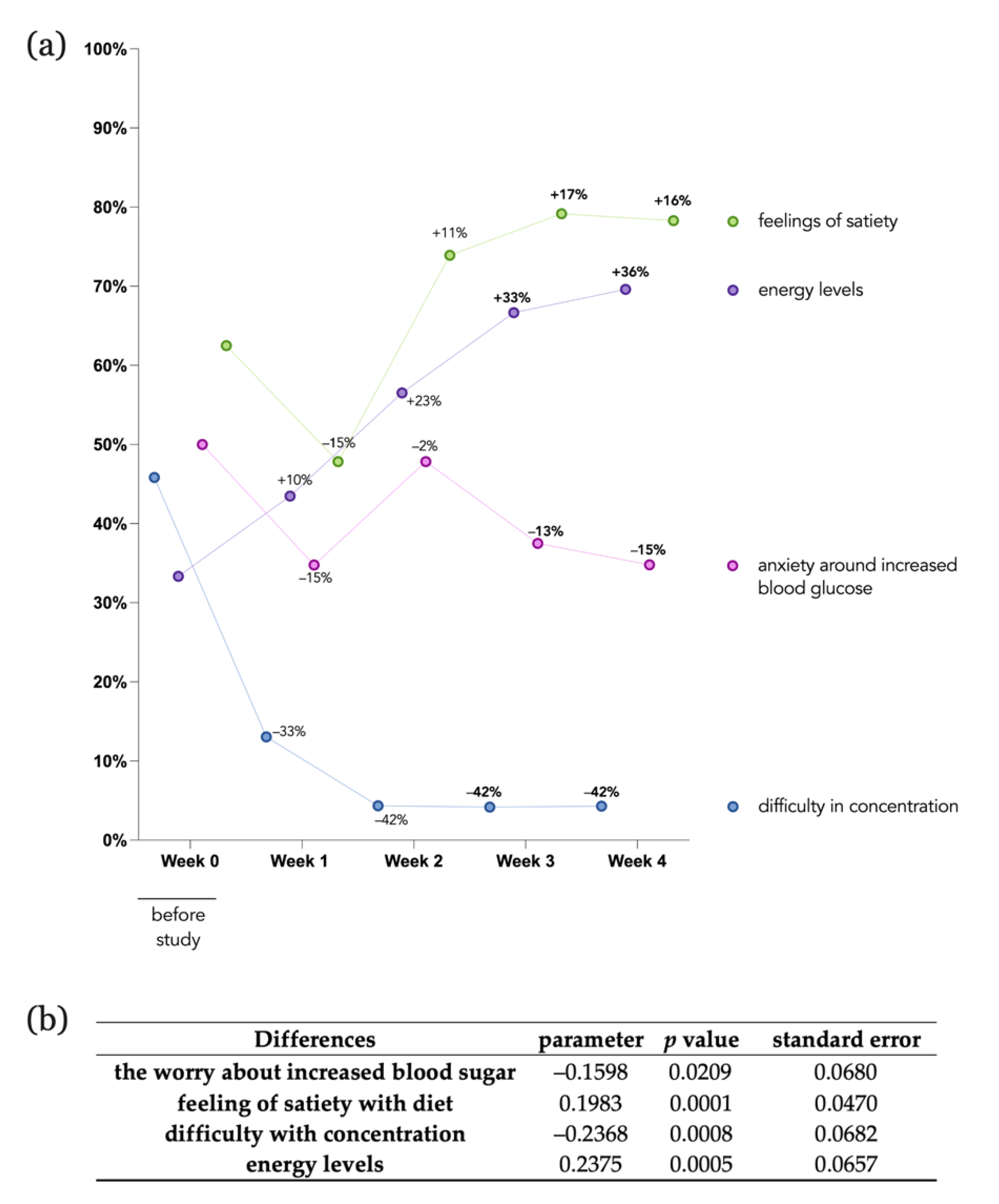
2.5. Statistical Analysis of Patient-Reported Outcome Measures (PROMs)
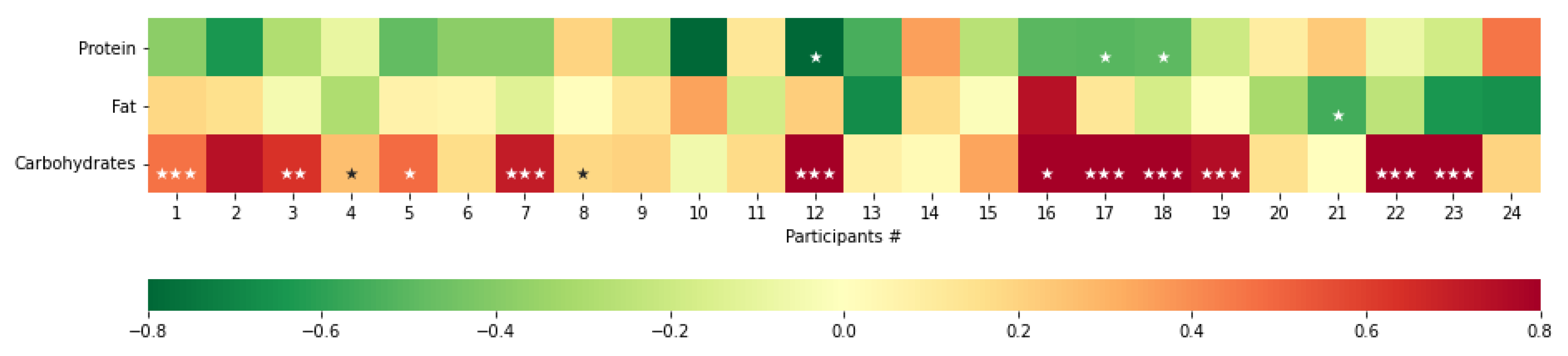
2.6. Multivariate Regression Analysis of Macronutrients
2.7. User Research Analysis
3. Results
3.1. Baseline Participant Characteristics
3.2. Individual Differences
3.3. Glycaemic Metrics
3.4. Participant-Reported Outcome Measures
3.5. User Research
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ali, M.K.; Pearson-Stuttard, J.; Selvin, E.; Gregg, E.W. Interpreting global trends in type 2 diabetes complications and mortality. Diabetologia 2022, 65, 3–13. [Google Scholar] [CrossRef]
- Unnikrishnan, R.; Pradeepa, R.; Joshi, S.R.; Mohan, V. Type 2 Diabetes: Demystifying the Global Epidemic. Diabetes 2017, 66, 1432–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, S.; Gastaldelli, A.; Yki-Järvinen, H.; Scherer, P.E. Why does obesity cause diabetes? Cell Metab. 2022, 34, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Hackett, R.A.; Moore, C.; Steptoe, A.; Lassale, C. Health behaviour changes after type 2 diabetes diagnosis: Findings from the English Longitudinal Study of Ageing. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef]
- Savarese, M.; Sapienza, M.; Acquati, G.M.; Nurchis, M.C.; Riccardi, M.T.; Mastrilli, V.; D’Elia, R.; Graps, E.A.; Graffigna, G.; Damiani, G. Educational Interventions for Promoting Food Literacy and Patient Engagement in Preventing Complications of Type 2 Diabetes: A Systematic Review. J. Pers. Med. 2021, 11, 795. [Google Scholar] [CrossRef]
- Berry, S.E.; Valdes, A.M.; Drew, D.A.; Asnicar, F.; Mazidi, M.; Wolf, J.; Capdevila, J.; Hadjigeorgiou, G.; Davies, R.; Al Khatib, H.; et al. Human postprandial responses to food and potential for precision nutrition. Nat. Med. 2020, 26, 964–973. [Google Scholar] [CrossRef]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [Green Version]
- Gray, I.D.; Kross, A.R.; Renfrew, M.E.; Wood, P. Precision Medicine in Lifestyle Medicine: The Way of the Future? Am. J. Lifestyle Med. 2019, 14, 169–186. [Google Scholar] [CrossRef]
- Sebire, S.J.; Toumpakari, Z.; Turner, K.M.; Cooper, A.R.; Page, A.S.; Malpass, A.; Andrews, R.C. I’ve made this my lifestyle now: A prospective qualitative study of motivation for lifestyle change among people with newly diagnosed type two diabetes mellitus. BMC Public Health 2018, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Vigersky, R.A.; Fonda, S.J.; Chellappa, M.; Walker, M.S.; Ehrhardt, N.M. Short- and long-term effects of real-time continuous glucose monitoring in patients with type 2 diabetes. Diabetes Care 2012, 35, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Cox, D.J.; Banton, T.; Moncrief, M.; Conaway, M.; Diamond, A.; McCall, A.L. Minimizing Glucose Excursions (GEM) With Continuous Glucose Monitoring in Type 2 Diabetes: A Randomized Clinical Trial. J. Endocr. Soc. 2020, 4, bvaa118. [Google Scholar] [CrossRef]
- Porter, M.; Fonda, S.; Swigert, T.; Ehrhardt, N. Real-Time Continuous Glucose Monitoring to Support Self-Care: Results from a Pilot Study of Patients with Type 2 Diabetes. J. Diabetes Sci. Technol. 2022, 16, 578–580. [Google Scholar] [CrossRef]
- Maurizi, A.R.; Pozzilli, P. Do we need continuous glucose monitoring in type 2 diabetes? Diabetes Metab. Res. Rev. 2013. [Google Scholar] [CrossRef]
- Ehrhardt, N.; al Zaghal, E. Behavior Modification in Prediabetes and Diabetes: Potential Use of Real-Time Continuous Glucose Monitoring. J. Diabetes Sci. Technol. 2019, 13, 271–275. [Google Scholar] [CrossRef]
- Engler, S.; Fields, S.; Leach, W.; van Loon, M. Real-Time Continuous Glucose Monitoring as a Behavioral Intervention Tool for T2D: A Systematic Review. J. Technol. Behav. Sci. 2022, 1–12. [Google Scholar] [CrossRef]
- Taylor, P.J.; Thompson, C.H.; Luscombe-Marsh, N.D.; Wycherley, T.P.; Wittert, G.; Brinkworth, G.D. Efficacy of Real-Time Continuous Glucose Monitoring to Improve Effects of a Prescriptive Lifestyle Intervention in Type 2 Diabetes: A Pilot Study. Diabetes Ther. 2019, 10, 509–522. [Google Scholar] [CrossRef] [Green Version]
- Taylor, P.J.; Thompson, C.H.; Brinkworth, G.D. Effectiveness and acceptability of continuous glucose monitoring for type 2 diabetes management: A narrative review. J. Diabetes Investig. 2018, 9, 713–725. [Google Scholar] [CrossRef]
- Ruijgrok, C.; Blaak, E.E.; Egli, L.; Dussort, P.; Vinoy, S. Reducing postprandial glucose in dietary intervention studies and the magnitude of the effect on diabetes-related risk factors: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 259. [Google Scholar] [CrossRef] [Green Version]
- Kröger, J.; Siegmund, T.; Schubert-Olesen, O.; Keuthage, W.; Lettmann, M.; Richert, K.; Pfeiffer, A.F. AGP and Nutrition—Analysing postprandial glucose courses with CGM. Diabetes Res. Clin. Pract. 2021, 174, 108738. [Google Scholar] [CrossRef]
- Neuberger, G.B. Measures of fatigue: The Fatigue Questionnaire, Fatigue Severity Scale, Multidimensional Assessment of Fatigue Scale, and Short Form-36 Vitality (Energy/Fatigue) Subscale of the Short Form Health Survey. Arthritis Care Res. 2003, 49, S175–S183. [Google Scholar] [CrossRef]
- Karalus, M.; Vickers, Z. Satiation and satiety sensations produced by eating oatmeal vs. oranges. A comparison of different scales. Appetite 2016, 99, 168–176. [Google Scholar] [CrossRef]
- Haugstvedt, A.; Hernar, I.; Strandberg, R.B.; Richards, D.A.; Nilsen, R.M.; Tell, G.S.; Graue, M. Use of patient-reported outcome measures (PROMs) in clinical diabetes consultations: Study protocol for the DiaPROM randomised controlled trial pilot study. BMJ Open 2019, 9, e024008. [Google Scholar] [CrossRef]
- Flick, U. The SAGE Handbook of Qualitative Data Analysis; SAGE Publications Inc.: Los Angeles, CA, USA, 2014. [Google Scholar] [CrossRef] [Green Version]
- Polonsky, W.H.; Fisher, L.; Earles, J.; Dudl, R.J.; Lees, J.; Mullan, J.; Jackson, R.A. Assessing Psychosocial Distress in DiabetesDevelopment of the Diabetes Distress Scale. Diabetes Care 2005, 28, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Freeman, J.; Lyons, L. The Use of Continuous Glucose Monitoring to Evaluate the Glycemic Response to Food. Diabetes Spectr. 2008, 21, 134–137. [Google Scholar] [CrossRef] [Green Version]
- Delahanty, L.M.; Pan, Q.; Jablonski, K.A.; Aroda, V.R.; Watson, K.E.; Bray, G.A.; Kahn, S.E.; Florez, J.C.; Perreault, L.; Franks, P.W.; et al. Effects of weight loss, weight cycling, and weight loss maintenance on diabetes incidence and change in cardiometabolic traits in the Diabetes Prevention Program. Diabetes Care 2014, 37, 2738–2745. [Google Scholar] [CrossRef] [Green Version]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar]
- Diabetes Prevention Program Research Group. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet 2009, 374, 1677–1686. [Google Scholar] [CrossRef] [Green Version]
- Chong, S.; Ding, D.; Byun, R.; Comino, E.; Bauman, A.; Jalaludin, B. Lifestyle changes after a diagnosis of type 2 diabetes. Diabetes Spectr. 2017, 30, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Reckinger, R.; Régnier, F. Diet and public health campaigns: Implementation and appropriation of nutritional recommendations in France and Luxembourg. Appetite 2017, 112, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Monterrosa, E.C.; Frongillo, E.A.; Drewnowski, A.; de Pee, S.; Vandevijvere, S. Sociocultural Influences on Food Choices and Implications for Sustainable Healthy Diets. Food Nutr. Bull. 2020, 41, 59S–73S. [Google Scholar] [CrossRef] [PubMed]
- Bickett, A.; Tapp, H. Anxiety and diabetes: Innovative approaches to management in primary care. Exp. Biol. Med. 2016, 241, 1724–1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.J.; Grigsby, A.B.; Freedland, K.E.; De Groot, M.; McGill, J.B.; Clouse, R.E.; Lustman, P.J. Anxiety and poor glycemic control: A meta-analytic review of the literature. Int. J. Psychiatry Med. 2002, 32, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Andersen, N.S.; Haugaard, L.H.; Pedersen, S.B.; Pedersen, M.S.; Bygholm, A. Digital Support for Self-Management in Children with Diabetes: Understanding Their Needs and Developing a Design Concept. Stud. Health Technol. Inform. 2020, 270, 951–955. [Google Scholar]
- Jandoo, T. WHO guidance for digital health: What it means for researchers. Digit. Health 2020, 6, 2055207619898984. [Google Scholar] [CrossRef]
- Fu, H.; McMahon, S.K.; Gross, C.R.; Adam, T.J.; Wyman, J.F. Usability and clinical efficacy of diabetes mobile applications for adults with type 2 diabetes: A systematic review. Diabetes Res. Clin. Pract. 2017, 131, 70–81. [Google Scholar] [CrossRef]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark Insights 2016, 11, 95–104. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Diagnosis of type 2 diabetes | Pregnancy or breastfeeding |
| Age ≥ 18 years | Treated with insulin, sulphonylureas, glinides |
| Own and are able to operate a smartphone | Unable to consent to involvement in research |
| Episodes of symptomatic hypoglycaemia in the last 3 months |
| Demographics | Count n = 24 | Descriptive Statistics n = 24 |
|---|---|---|
| Age | ||
| <30 to 40 | 3 (12.50%) | |
| 41 to 50 | 7 (29.17%) | |
| 51 to 60 | 7 (29.17%) | |
| 61 to 70 | 5 (20.83%) | |
| 71 to 80 | 2 (8.33%) | |
| Mean ± SD | 54 ± 11.18 years | |
| Maximum | 74 years | |
| Minimum | 27 years | |
| Gender | ||
| Female | 18 (75.00%) | |
| Male | 6 (25.00%) | |
| HbA1c | ||
| <6.5% | 2 (8.33%) | |
| 6.5% to 6.9% | 6 (25.00%) | |
| 7% to 7.9% | 6 (25.00%) | |
| 8% to 8.9% | 5 (20.83%) | |
| 9% to 10% | 3 (12.50%) | |
| >10% | 2 (8.33%) | |
| Mean ± SD | 7.92 ± 1.77% | |
| Maximum | 13.40% | |
| Minimum | 5.30% | |
| Weight | ||
| Mean ± SD | 95.78 ± 17.61 kg | |
| Maximum | 125.40 kg | |
| Minimum | 61 kg | |
| BMI 1 (kg/m2) | ||
| Mean ± SD | 31.87 ± 6.27 kg/m2 | |
| Maximum | 44.43 kg/m2 | |
| Minimum | 21.36 kg/m2 | |
| Median | 31.59 kg/m2 | |
| Year of diagnosis | ||
| <2000 | 1 (4.17%) | |
| 2000 to 2009 | 3 (12.50%) | |
| 2010 to 2019 | 12 (50.00%) | |
| >2020 | 8 (33.33%) | |
| Mean ± SD | 2015 ± 8 years | |
| Maximum | 2021 | |
| Minimum | 1986 | |
| Age at diagnosis | ||
| <31 | 3 (12.50%) | |
| 31 to 40 | 1 (4.17%) | |
| 41 to 50 | 11 (45.83%) | |
| 51 to 60 | 6 (25.00%) | |
| 61 to 70 | 3 (12.50%) | |
| Mean ± SD | 47 ± 11.81 years | |
| Maximum | 68 years | |
| Minimum | 17 years | |
| Antidiabetes medication | ||
| No | 3 (11.54%) | |
| Yes | 21 (88.46%) | |
| 1 type of AM | 9 (37.50%) | |
| >1 type of AM | 12 (50.00%) | |
| metformin | 19 (79.17%) | |
| GLP-1-agonist 1 | 4 (16.67%) | |
| SGLT-2-inhibitor 1 | 6 (25.00%) | |
| DPP-4 1 | 7 (29.17%) | |
| Alpha-glucosidase inhibitors | 1 (4.17%) | |
| Other conditions | ||
| No | 9 (37.50%) | |
| Yes | 15 (62.50%) | |
| Hypertension | 8 (33.33%) | |
| Autoimmune disease | 3 (12.50%) | |
| Other illness 1 | 9 (37.50%) |
| Major Baseline Characteristics | Regression Coefficient (Beta) | Standard Error of the Estimate | p Value |
|---|---|---|---|
| Pre-insight median iAUC | |||
| Age | 5.566 | 0.836 | 0.836 |
| HbA1c | 118.845 | 0.437 | 0.437 |
| BMI | −17.832 | 0.697 | 0.697 |
| Other diseases | 68.698 | 0.903 | 0.903 |
| Post-insight median iAUC | |||
| Age | 1.822 | 0.950 | 0.950 |
| HbA1c | −36.546 | 0.824 | 0.824 |
| BMI | 6.180 | 0.901 | 0.901 |
| Other diseases | −174.313 | 0.775 | 0.775 |
| Absolute difference median iAUC | |||
| Age | −3.744 | 0.884 | 0.884 |
| HbA1c | −155.391 | 0.289 | 0.289 |
| BMI | 24.012 | 0.583 | 0.583 |
| Other diseases | −243.010 | 0.651 | 0.651 |
| Themes | User Quotes |
|---|---|
| The perceived impact of knowledge gained by CGM | |
| Altered meal planning behaviour | The bad meals, so to say, don’t make it on my grocery list. (U4) |
| Recycling of good ingredients for other meals | I looked at what was positive and then I also looked at which building blocks I could use or could use later and perhaps modify them a little and then make another meal out of it that would have the same positive effect. (U3) |
| Decreasing proportions of less ideal ingredients | Or take one tablespoon or two tablespoons less oatmeal. Well, you’ll still be full with the nuts you add and everything. But take a little less of it. And I found that really very, very pleasant to be able to observe over these four weeks that there had been a clear improvement. (U5) |
| Reduction in hidden sugars | But I eat much, much more consciously. I always try to include nuts and things like that, things that have value, and I really refrain from anything that basically also contains hidden sugars and things like that. I stick to that consistently. (U6) |
| Increased motivation | I was somehow relieved. I didn’t do everything wrong. Before I really thought I was doing everything wrong when it was so high. And yes, I’m highly motivated, totally motivated. (U2) |
| Acquiring knowledge of the individual reactions to different foods | |
| Meal analysis of meal components | But you suddenly notice it, or at least I do, much more consciously, because otherwise you don’t dissect and pick apart your meal like that. (U5) |
| Personalised meal analysis and recommendations | With so many programmes, I would say, or dietary change programmes, a lot of things are given to you and you have to integrate things that you might not like so much. They also include foods that you don’t use in your routine. And I actually found it very, very good that I got information about the value of my diet tailored to my meal plan, to my family’s daily routine. (U1) |
| Combination of CGM curve and meal logging | But I can also link that [CGM values] to the meal. That I can then see okay, I ate this and that and afterwards it rises and falls again in that specific period of time. This is also possible in the morning or at lunchtime with every meal, so that it is easier to follow up than if I were to take a blood sample. (U3) |
| Pain points and self-management barriers | |
| Weight reduction | If I want to lose weight, I also have to pay a bit of attention to how these macronutrients are and what influence they have. So in this case, not only for blood sugar, but also overall. (U3) |
| Lifestyle barriers | Testing the meals, that is actually something that I find very interesting. And actually, I would have liked to do all of them, but that is quite difficult for me in my everyday life. Because I can’t eat or drink anything else for two hours before and two hours after the meal. (U1) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungersboeck, M.; Tang, X.; Neeff, V.; Steele, D.; Grimm, P.; Fenech, M. Personalised Nutritional Recommendations Based on Individual Post-Prandial Glycaemic Responses Improve Glycaemic Metrics and PROMs in Patients with Type 2 Diabetes: A Real-World Assessment. Nutrients 2022, 14, 2123. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102123
Ungersboeck M, Tang X, Neeff V, Steele D, Grimm P, Fenech M. Personalised Nutritional Recommendations Based on Individual Post-Prandial Glycaemic Responses Improve Glycaemic Metrics and PROMs in Patients with Type 2 Diabetes: A Real-World Assessment. Nutrients. 2022; 14(10):2123. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102123
Chicago/Turabian StyleUngersboeck, Madlen, Xiaowen Tang, Vanessa Neeff, Dominic Steele, Pascal Grimm, and Matthew Fenech. 2022. "Personalised Nutritional Recommendations Based on Individual Post-Prandial Glycaemic Responses Improve Glycaemic Metrics and PROMs in Patients with Type 2 Diabetes: A Real-World Assessment" Nutrients 14, no. 10: 2123. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102123