Efficacy of a New Low-Protein Multimedia Diet App for PKU

 , , ,
, , ,
Abstract
:1. Introduction
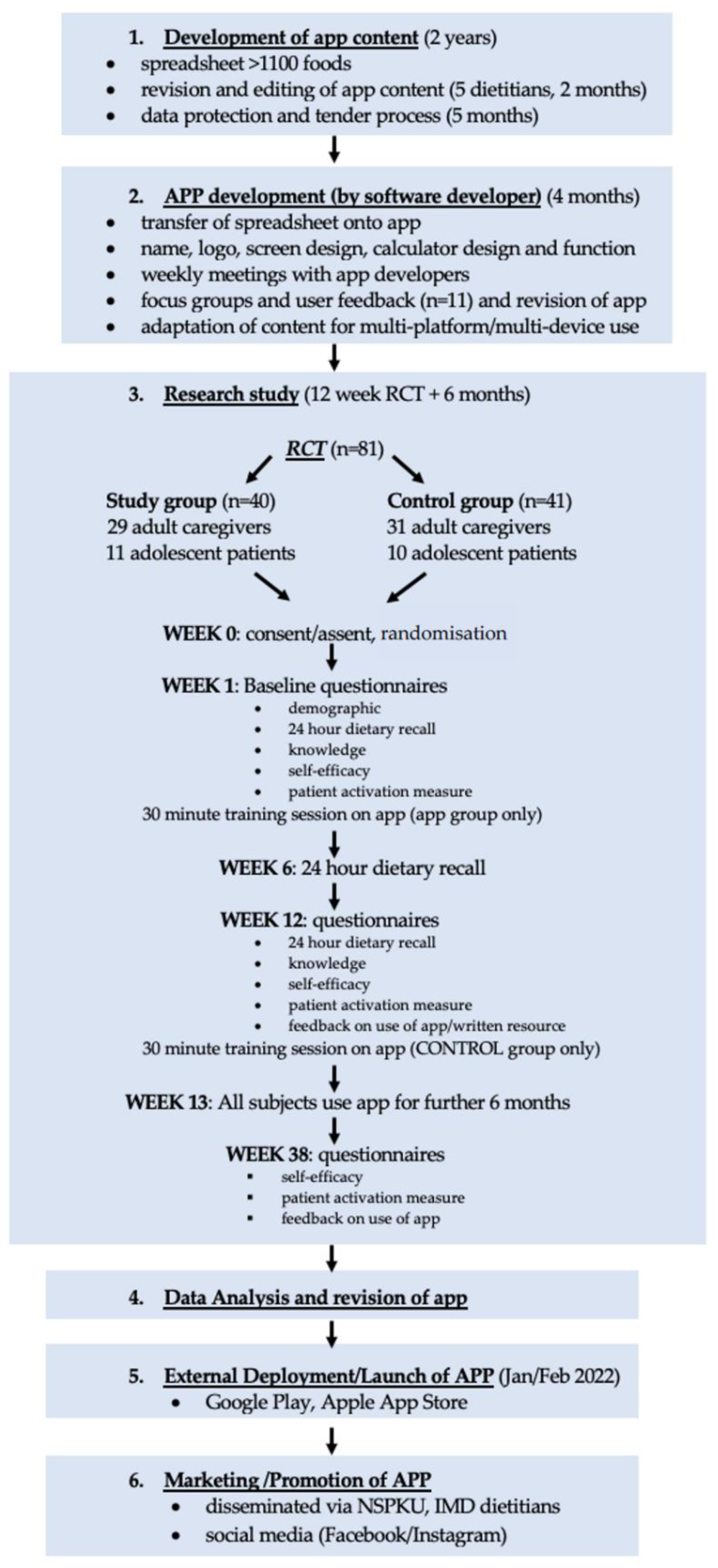
2. Materials and Methods
2.1. App Development
2.1.1. App Content
- a general description of the food such as appearance and origins;
- suitability for inclusion in a low-protein diet (based on British Inherited Metabolic Disease Group (BIMDG) UK dietetic consensus statements [18,19], including colour coding (green: low-protein exchange-free foods; orange: exchange foods that contain protein/Phe and so should be calculated as part of the daily allowance; red: high-protein foods that are best avoided);
- menu ideas and food serving suggestions;
- exchange-free (low-protein) recipes;
- food preparation;
- food storage recommendations;
- food availability information, including details of home delivery companies that supply low-protein prescription items.
- all special low-protein prescription items;
- plant foods (e.g., fruits and vegetables, whether fresh, frozen, canned, or dried);
- cheese, yogurt, cream, and alternatives (e.g., regular, low-protein, or vegan cheeses, yoghurts, cream);
- savoury foods/meat alternatives (e.g., low-protein or plant burgers, sausages, soups, legumes, plant-based meat alternatives);
- flours, pasta, and cereals (e.g., breads, bread products, and pastries, including gluten-free varieties);
- fats, oils, sauces, dips, and spices (e.g., butter, margarine, oils, gravy, ketchup, dressings, marinades);
- cakes, biscuits, and desserts (e.g., plant and milk-based ice-cream, custards, jellies, puddings);
- drinks (e.g., fizzy drinks, squash, juices, smoothies, milk, plant milks, hot chocolate, milkshake powders);
- baking ingredients (e.g., sugar, baking powder, cake decorations, colourings, flavourings);
- sweet spreads, sweets, and syrups (e.g., chocolate, sweets, chewing gum, jams, honey, chocolate spread);
- snack foods (e.g., crisps, crackers, ice lollies);
- food label ingredients (e.g., food additives).
2.1.2. App Design
2.2. Randomised Controlled Trial
2.2.1. Subjects
2.2.2. Randomisation
2.2.3. App Group
2.2.4. Control Group
2.2.5. Demographic Questionnaire
2.2.6. Knowledge Questionnaire
2.2.7. Self-Efficacy Questionnaire
2.2.8. Patient Activation Measure
2.2.9. Feedback Questionnaire
2.2.10. Natural Protein Intake
2.2.11. Metabolic Control
2.3. Six Month Follow Up
2.4. Statistics
2.5. Ethical Approval
3. Results
3.1. Subjects
3.2. Baseline Use of Apps and Sources of Dietary Information
3.3. Frequency of Using the ‘PKU Bite’® App at Twelve Weeks and Six Months Follow Up
3.4. Frequency of Seeking Dietary Assistance at Baseline, Twelve Weeks, and Six Months
3.4.1. Between Group Differences
3.4.2. Within Group Changes
3.5. Self Confidence in Managing PKU
3.6. Knowledge and Interpretation of Low-Protein Labelling
3.7. Accuracy of Calculating Daily Natural Protein Intake
3.8. Metabolic Control
3.9. Participant Feedback
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, A.; van Wegberg, A.M.J.; Ahring, K.; Beblo, S.; Belanger-Quintana, A.; Burlina, A.; Campistol, J.; Coskun, T.; Feillet, F.; Gizewska, M.; et al. Pku Dietary Handbook to Accompany Pku Guidelines. Orphanet. J. Rare Dis. 2020, 15, 171. [Google Scholar] [CrossRef] [PubMed]
- European Parliament. Regulation (Eu) No 1169/2011 of the European Parliament and the Council of the European Union of 25 October 2011 on the Setting of Tolerances for Nutrient Values Declared on a Label. Off. J. Eur. Union. L. 2011, 304, 18–63. [Google Scholar]
- Imogen, H.; Pinto, A.; Evans, S.; Daly, A.; Ashmore, C.; Ford, S.; Buckley, S.; MacDonald, A. The Challenges and Dilemmas of Interpreting Protein Labelling of Prepackaged Foods Encountered by the Pku Community. Nutrients 2022, 14, 1355. [Google Scholar] [CrossRef]
- Kraleva, D.; Evans, S.; Pinto, A.; Daly, A.; Ashmore, C.; Pointon-Bell, K.; Rocha, J.C.; MacDonald, A. Protein Labelling Accuracy for Uk Patients with Pku Following a Low Protein Diet. Nutrients 2020, 12, 3440. [Google Scholar] [CrossRef] [PubMed]
- Newbould, E.; Pinto, A.; Evans, S.; Ford, S.; O’Driscoll, M.; Ashmore, C.; Daly, A.; MacDonald, A. Accidental Consumption of Aspartame in Phenylketonuria: Patient Experiences. Nutrients 2021, 13, 707. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Yilmaz, O.; Pinto, A.; Daly, A.; MacDonald, A. Low Protein Mobile and Web-Based Diet Applications: What’s out There? JIEMS 2017, 5, 74. [Google Scholar]
- Jaffar, A.; Sidik, S.M.; Foo, C.N.; Muhammad, N.A.; Manaf, R.A.; Suhaili, N. Preliminary Effectiveness of Mhealth App-Based Pelvic Floor Muscle Training among Pregnant Women to Improve Their Exercise Adherence: A Pilot Randomised Control Trial. Int. J. Environ. Res. Public Health 2022, 19, 2332. [Google Scholar] [CrossRef]
- Lavikainen, P.; Mattila, E.; Absetz, P.; Harjumaa, M.; Lindstrom, J.; Jarvela-Reijonen, E.; Aittola, K.; Mannikko, R.; Tilles-Tirkkonen, T.; Lintu, N.; et al. Digitally Supported Lifestyle Intervention to Prevent Type 2 Diabetes through Healthy Habits: Secondary Analysis of Long-Term User Engagement Trajectories in a Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e31530. [Google Scholar] [CrossRef]
- Al-Arkee, S.; Mason, J.; Lane, D.A.; Fabritz, L.; Chua, W.; Haque, M.S.; Jalal, Z. Mobile Apps to Improve Medication Adherence in Cardiovascular Disease: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2021, 23, e24190. [Google Scholar] [CrossRef]
- van Beurden, S.B.; Smith, J.R.; Lawrence, N.S.; Abraham, C.; Greaves, C.J. Feasibility Randomized Controlled Trial of Impulsepal: Smartphone App-Based Weight Management Intervention to Reduce Impulsive Eating in Overweight Adults. JMIR Form. Res. 2019, 3, e11586. [Google Scholar] [CrossRef]
- Jimoh, F.; Lund, E.K.; Harvey, L.J.; Frost, C.; Lay, W.J.; A Roe, M.; Berry, R.; Finglas, P.M. Comparing Diet and Exercise Monitoring Using Smartphone App and Paper Diary: A Two-Phase Intervention Study. JMIR mHealth uHealth 2018, 6, e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, M.C.; Burley, V.J.; Cade, J.E. Weight Loss Associated with Different Patterns of Self-Monitoring Using the Mobile Phone App My Meal Mate. JMIR mHealth uHealth 2017, 5, e8. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Chen, M.; Yuan, J.; Sun, Y. A Smart Phone-Based Diabetes Management Application Improves Blood Glucose Control in Chinese People with Diabetes. Diabetes Res. Clin. Pract. 2016, 116, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Burley, V.J.; Cade, J.E. Handheld Electronic Technology for Weight Loss in Overweight/Obese Adults. Curr. Obes. Rep. 2014, 3, 307–315. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a Smartphone Application for Weight Loss Compared to Website and Paper Diary: Pilot Randomized Controlled Trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef]
- Burke, L.E.; Styn, M.A.; Sereika, S.M.; Conroy, M.B.; Ye, L.; Glanz, K.; Sevick, M.A.; Ewing, L.J. Using Mhealth Technology to Enhance Self-Monitoring for Weight Loss: A Randomized Trial. Am. J. Prev. Med. 2012, 43, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Klasnja, P.; Pratt, W. Healthcare in the Pocket: Mapping the Space of Mobile-Phone Health Interventions. J. Biomed. Inform. 2012, 45, 184–198. [Google Scholar] [CrossRef] [Green Version]
- Evans, S.; Ford, S.; Adam, S.; Adams, S.; Ash, J.; Ashmore, C.; Caine, G.; Carruthers, R.; Cawtherley, S.; Chahal, S.; et al. Development of National Consensus Statements on Food Labelling Interpretation and Protein Allocation in a Low Phenylalanine Diet for Pku. Orphanet. J. Rare Dis. 2019, 14, 2. [Google Scholar] [CrossRef]
- Evans, S.; Adam, S.; Adams, S.; Allen, H.; Ashmore, C.; Bailey, S.; Banks, J.; Churchill, H.; Cochrane, B.; Cook, J.; et al. Uniformity of Food Protein Interpretation Amongst Dietitians for Patients with Phenylketonuria (Pku): 2020 Uk National Consensus Statements. Nutrients 2020, 12, 2205. [Google Scholar] [CrossRef]
- Viau, K.S.; Jessica, J.L.; Murtaugh, M.A.; Gren, L.H.; Stanford, J.B.; Bilder, D.A. Phone-Based Motivational Interviewing to Increase Self-Efficacy in Individuals with Phenylketonuria. Mol. Genet. Metab. Rep. 2016, 6, 27–33. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Mahoney, E.R.; Stockard, J.; Tusler, M. Development and Testing of a Short Form of the Patient Activation Measure. Health Serv. Res. 2005, 40, 1918–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gov.UK. What Qualification Levels Mean—England, Wales and Northern Ireland. Available online: https://www.gov.uk/what-different-qualification-levels-mean/list-of-qualification-levels (accessed on 19 April 2018).
- MacDonald, A.; van Rijn, M.; Feillet, F.; Lund, A.M.; Bernstein, L.; Bosch, A.M.; Gizewska, M.; van Spronsen, F.J. Adherence Issues in Inherited Metabolic Disorders Treated by Low Natural Protein Diets. Ann. Nutr. Metab. 2012, 61, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Feillet, F.; MacDonald, A.; Perron, D.H.; Burton, B. Outcomes Beyond Phenylalanine: An International Perspective. Mol. Genet. Metab. 2010, 99 (Suppl. S1), S79–S85. [Google Scholar] [CrossRef] [PubMed]
- Chau, M.M.; Burgermaster, M.; Mamykina, L. The Use of Social Media in Nutrition Interventions for Adolescents and Young Adults-a Systematic Review. Int. J. Med. Inform. 2018, 120, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Daly, A.; Hopkins, V.; Davies, P.; MacDonald, A. The Impact of Visual Media to Encourage Low Protein Cooking in Inherited Metabolic Disorders. J. Hum. Nutr. Diet. 2009, 22, 409–413. [Google Scholar] [CrossRef]
- Bernstein, L.E.; Helm, J.R.; Rocha, J.C.; Almeida, M.F.; Feillet, F.; Link, R.M.; Gizewska, M. Nutrition Education Tools Used in Phenylketonuria: Clinician, Parent and Patient Perspectives from Three International Surveys. J. Hum. Nutr. Diet. 2014, 27 (Suppl. S2), 4–11. [Google Scholar] [CrossRef]
- Durham-Shearer, S.J.; Judd, P.A.; Whelan, K.; Thomas, J.E. Knowledge, Compliance and Serum Phenylalanine Concentrations in Adolescents and Adults with Phenylketonuria and the Effect of a Patient-Focused Educational Resource. J. Hum. Nutr. Diet. 2008, 21, 474–485. [Google Scholar] [CrossRef]
- MacDonald, A.; Adam, S.; Ash, J.; Ashmore, C.; Caine, G.; Chan, H.; Clark, A.; Coates, E.; Cochrane, B.; Daly, A.; et al. Stricter and Differing Interpretation of Protein Food Labelling by Parents/Adults with Pku Than by Imd Dietitians. Ssiem 2016 Annual Symposium. J. Inherit. Metab. Dis. 2016, 39, 8. [Google Scholar]
- Wood, G.; Pinto, A.; Evans, S.; Daly, A.; Adams, S.; Costelloe, S.; Gribben, J.; Ellerton, C.; Emm, A.; Firman, S.; et al. Special Low Protein Foods Prescribed in England for Pku Patients: An Analysis of Prescribing Patterns and Cost. Nutrients 2021, 13, 3977. [Google Scholar] [CrossRef]
- Evans, S.; Ashmore, C.; Daly, A.; Jackson, R.; Pinto, A.; MacDonald, A. Validation of a Low-Protein Semi-Quantitative Food Frequency Questionnaire. Nutrients 2022, 14, 1595. [Google Scholar] [CrossRef]
- Department of Health and Social Care. Nhsx: New Joint Organisation for Digital, Data and Technology. 2019. Available online: https://www.gov.uk/government/news/nhsx-new-joint-organisation-for-digital-data-and-technology (accessed on 22 February 2022).
- NHSX. Digital Technology Assessment Criteria (Dtac). 2022. Available online: https://www.nhsx.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/ (accessed on 22 February 2022).



{kind=link}
{kind=link}
| App Group | Control Group | |
|---|---|---|
| Number of child subjects (gender) | 11 (6 F, 5 M) | 10 (8 F, 2 M) |
| Median age of child subjects (years) (IQR) | 12.0 (10.5–13.0) | 12.7 (12.0–14.0) |
| Number of parent/carer subjects (gender) | 29 (18 mothers, 10 fathers, 1 grandmother) | 31 (24 mothers, 5 fathers, 2 grandmothers) |
| Median age of mothers (years) (IQR) | 36.5 (31.8–39.3) | 35.5 (31.3–41.0) |
| Median age of fathers (years) (IQR) | 39.0 (35.5–44.5) | 38.0 (30.0–44.0) |
| Mother’s highest educational qualification # median (IQR) | 3.0 (2.0–6.5) | 2.0 (2.0–3.0) |
| Father’s highest educational qualification # median (IQR) | 5.0 (2.0–6.0) | 4.0 (2.0–5.0) |
| Total number of children (including children of parent/carer participants) (gender) | 21 (10 F, 11 M) | 25 (15 F, 10 M) |
| Median age of all children (including children of parent/carer participants) (years) (IQR) | 10.0 (5.5–12.5) | 9.0 (2.5–12.0) |
| Ethnicity of all children | 19 White/European 1 Asian 1 mixed race | 20 White/European 4 Asian 1 mixed race |
| Parent/Carer | Child | |||||
|---|---|---|---|---|---|---|
| Number of Apps Used | App Group n = 29 Median (IQR) | Control Group n = 31 Median (IQR) | Total n = 60 Median (IQR) | App Group n = 11 Median (IQR) | Control Group n = 10 Median (IQR) | Total n = 21 Median (IQR) |
| Total no. apps used per participant | 40 (25–100) | 30 (13–61) | 36 (18–74) | 30 (7–79) | 30 (19–47) | 30 (10–60) |
| No. apps used/day per participant | 5.5 (3–15) | 4 (3–7) | 5 (3–10) | 4 (1–6) | 4.5 (4–6) | 4 (3–6) |
| No. apps used/week per participant | 11 (6–25) | 8 (6–14) | 10 (6–19) | 7 (3–12) | 7 (4–10) | 7 (4–10) |
| Sources of dietary information % of subjects (n) | ||||||
| Written info | 86 (25) | 81 (25) | 83 (50) | 36 (4) | 60 (6) | 48 (10) |
| Phone/email dietitian | 83 (24) | 71 (22) | 77 (46) | 55 (6) | 80 (8) | 67 (14) |
| Social media | 69 (20) | 61 (19) | 65 (39) | 18 (2) | 40 (4) | 29 (6) |
| Clinic/home visit dietitian | 55 (16) | 39 (12) | 47 (28) | 45 (5) | 30 (3) | 38 (8) |
| Ask others with PKU | 21 (6) | 23 (7) | 22 (13) | 9 (1) | 10 (1) | 10 (2) |
| Child’s parent(s) | N/A | N/A | N/A | 18 (2) | 30 (3) | 24 (5) |
| App Group 12 Weeks | App Group 6 Months | Control Group 6 Months | ||||
|---|---|---|---|---|---|---|
| Parent (n = 29) | Child (n = 11) | Parent (n = 29) | Child (n = 11) | Parent (n = 25) | Child (n = 7) | |
| Never | 5 (2 M, 3 F) | 3 (1 M, 2 F) | 6 (3 M, 3 F) | 3 (1 M, 2 F) | 5 (1 M, 4 F) | 4 (1 M, 3 F) |
| Rarely | 8 (4 M, 4 F) | 4 (1 M, 3 F) | 7 (1 M, 6 F) | 6 (3 M, 3 F) | 5 (1 M, 4 F) | 1 (1 F) |
| Once a week | 8 (2 M, 6 F) | 2 (1 M, 1 F) | 9 (5 M, 4 F) | 0 | 3 (2 M, 1 F) | 2 (2 F) |
| Two–six times per week | 4 (2 M, 2 F) | 1 (1 M) | 7 (1 M, 6 F) | 2 (1 M, 1 F) | 9 (1 M, 8 F) | 0 |
| Once a day | 3 (3 F) | 1 (1 M) | 0 | 0 | 1 (1 F) | 0 |
| >Once a day | 0 | 0 | 0 | 0 | 2 (2 F) | 0 |
| No response | 1 (1 F) | 0 | 0 | 0 | 0 | 0 |
| Parent/Carer Baseline | Parent/Carer 12 Weeks | Parent/Carer 6 Months | Child Baseline | Child 12 Weeks | Child 6 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| App Group n = 29 | Control Group n = 31 | App Group n = 29 | Control Group n = 31 | App Group n = 29 | Control Group n = 25 | App Group n = 11 | Control Group n = 10 | App Group n = 11 | Control Group n = 10 | App Group n = 11 | Control Group n = 7 | |
| Phone/text/ email dietitian % (n) | 45 (13) | 42 ** (13) | 38 (11) | 45 (14) | 45 (13) | 28 ** (8) | 9 (1) | 50 (5) | 0 (0) | 30 (3) | 18 (2) | 43 (3) |
| p-value | 0.90 | 0.41 | 0.10 | 0.05 | 0.01 | 0.11 | ||||||
| Social media e.g., Facebook/Twitter % (n) | 72 *,# (21) | 65 ++ (20) | 41 * (12) | 55 (17) | 52 # (15) | 40 ++ (10) | 18 (2) | 60 (6) | 27 (3) | 10 (1) | 18 (2) | 14 (1) |
| p-value | 0.54 | 0.30 | 0.22 | 0.45 | 0.48 | 0.99 | ||||||
| Written information % (n) | 34 (10) | 71 § (22) | 38 (11) | 52 (16) | 28 (8) | 52 § (13) | 0 (0) | 50 (5) | 9 (1) | 0 (0) | 9 (1) | 14 (1) |
| p-value | 0.004 | 0.22 | 0.09 | 0.06 | 0.03 | 0.23 | ||||||
| Baseline Median (IQR) | 12 Weeks Median (IQR) | 6 Months Median (IQR) | p-Value * (Baseline vs. 6 Months) | |
|---|---|---|---|---|
| Self-efficacy questionnaire (1 = not confident, 10 = confident) | ||||
| App group parent | 8.85 (8.6–9.1) | 8.70 (8.4–9.1) | 9.00 (8.7–9.2) | 0.38 |
| Control group parent | 8.20 (7.9–8.5) | 8.65 (8.2–8.9) | 9.20 (9.1–9.3) | 0.02 |
| p-value * | 0.02 | 0.70 | 0.11 | |
| App group child | 7.95 (7.7–8.5) | 7.60 (6.8–8.4) | 8.20 (7.9–8.5) | 0.16 |
| Control group child | 6.35 (5.6–7.8) | 7.05 (6.4–7.5) | 6.65 (5.6–7.8) | 0.37 |
| p-value * | 0.02 | 0.17 | 0.01 | |
| App users (parents/carers from app and control groups, who used app ≥weekly) | 9.00 (8.3–9.5) | NA | 9.10 (8.3–9.8) | 0.08 |
| App nonusers (parents/carers from app and control groups, who rarely/never used app) | 8.60 (7.7–9.8) | NA | 9.45 (8.4–10.0) | 0.10 |
| p-value * | 0.75 | 0.51 | ||
| Patient activation measure (1 = strongly disagree, 4= strongly agree) | ||||
| App group parent | 3.60 (3.4–3.8) | 3.60 (3.5–3.8) | 3.70 (3.5–3.8) | 0.02 |
| Control group parent | 3.60 (3.4–3.7) | 3.60 (3.4–3.7) | 3.70 (3.6–3.8) | 0.009 |
| p-value * | 0.93 | 0.39 | 0.42 | |
| App group child | 3.30 (3.1–3.3) | 3.10 (3.0–3.2) | 3.20 (3.2–3.4) | 0.35 |
| Control group child | 3.10 (3.0–3.3) | 3.20 (2.9–3.3) | 2.90 (2.7–3.1) | 0.01 |
| p-value * | 0.11 | 0.87 | <0.0001 | |
| App users (parents/carers from app and control groups, who used app ≥weekly at 6 months) | 3.50 (3.3–3.8) | NA | 3.80 (3.5–4.0) | 0.03 |
| App nonusers (parents/carers from app and control groups, who rarely/never used app at 6 months) | 3.70 (3.2–3.9) | NA | 3.50 (3.2–4.0) | 0.48 |
| p-value * | 0.76 | 0.24 | ||
| Baseline Mean% (SD) | 12 Weeks Mean% (SD) | |
|---|---|---|
| App group parent | 65.4 (18.0) | 66.7 (15.9) |
| Control group parent | 61.4 (14.8) | 60.2 (17.3) |
| App group child | 52.1 (22.1) | 49.3 (15.3) |
| Control group child | 48.1 (13.7) | 47.7 (14.3) |
| App users (parents/carers from app group, who used app ≥weekly at 12 weeks) | 64.9 (18.3) | 69.0 (14.1) |
| App nonusers (parents/carers from app group, who rarely/never used app at 12 weeks) | 66.0 (18.4) | 63.9 (18.0) |
| Baseline Mean (SD) | 6 Weeks Mean (SD) | 12 Weeks Mean (SD) | p Value (Baseline vs. 12 Weeks) | ||
|---|---|---|---|---|---|
| App group Parent/carer n = 29 | % of incorrectly calculated food items * | 20.6 (20.9) | 15.5 (18.0) | 15.5 (18.9) | 0.18 |
| No. of subjects correctly calculating all protein intake | 11 | 9 | 19 | ||
| Control group Parent/carer n = 31 | % of incorrectly calculated food items * | 21.4 (27.4) | 24.4 (22.5) | 11.5 (19.5) | 0.32 |
| No. of subjects correctly calculating all protein intake | 14 | 7 | 10 | ||
| p value (% incorrect app group vs. control group) | 0.73 | 0.12 | 0.72 | ||
| App group Child n = 11 | % of incorrectly calculated food items * | 28.2 (32.5) | 15.9 (20.5) | 11.5 (18.2) | 0.09 |
| No. of subjects correctly calculating all protein intake | 3 | 3 | 4 | ||
| Control group Child n = 10 | % of incorrectly calculated food items * | 31.6 (32.8) | 40.8 (36.6) | 34.3 (39.4) | 0.88 |
| No. of subjects correctly calculating all protein intake | 2 | 0 | 1 | ||
| p value (% incorrect app group vs. control group) | 0.61 | 0.09 | 0.18 | ||
| App users (parents/carers from app group, who used app ≥weekly at 12 weeks) n = 16 | % of incorrectly calculated food items * | 18.2 (21.3) | 14.2 (19.2) | 16.6 (21.5) | 0.97 |
| No. of subjects correctly calculating all protein intake | 6 | 5 | 12 | ||
| App non-users (parents/carers from app group, who rarely/never used app at 12 weeks) n = 13 | % of incorrectly calculated food items * | 23.7 (29.9) | 17.0 (17.0) | 14.3 (16.3) | 0.13 |
| No. of subjects correctly calculating all protein intake | 5 | 4 | 7 | ||
| p value (% incorrect app users vs. non users) | 0.54 | 0.61 | 0.89 | ||
| Baseline Median (IQR) | 12 Weeks Median (IQR) | 6 Months Median (IQR) | p Value (Baseline vs. 12 Weeks) | p Value (Baseline vs. 6 Months) | |
|---|---|---|---|---|---|
| App group children * | 288 (222–376) | 260 (207–397) | 315 (232–428) | 0.58 | 0.25 |
| Control group children * | 287 (174–338) | 221 (198–403) | 246 (199–347) | 0.59 | 0.10 |
| p value | 0.50 | 0.52 | 0.22 |
| App Group 12 Weeks | App Group 6 Months | Control Group 6 Months | ||||
|---|---|---|---|---|---|---|
| Parent % (n = 29) | Child % (n = 11) | Parent % (n = 29) | Child % (n = 11) | Parent % (n = 25) | Child % (n = 7) | |
| Able to look up the number of exchanges in a food | 52 (15) | 55 (6) | 48 (14) | 55 (6) | 44 (11) | 29 (2) |
| Able to look up protein/Phe content of a food | 48 (14) | 27 (3) | 62 (18) | 36 (4) | 52 (13) | 43 (3) |
| Able to get advice on suitability of foods | 41 (12) | 0 | 52 (15) | 18 (2) | 52 (13) | 0 |
| Quick and easy to access diet information immediately when needed | 28 (8) | 27 (3) | 41 (12) | 27 (3) | 44 (11) | 0 |
| Able to calculate daily exchanges | 17 (5) | 9 (1) | 28 (8) | 27 (3) | 28 (7) | 0 |
| Able to look up guidelines/rules about certain foods | 24 (7) | 0 | 28 (8) | 18 (2) | 20 (5) | 0 |
| Able to get advice on how to use foods/ingredients in a low-protein diet | 17 (5) | 9 (1) | 31 (9) | 18 (2) | 8 (2) | 14 (1) |
| Able to get advice on how to cook/prepare a food | 14 (4) | 18 (2) | 21 (6) | 18 (2) | 8 (2) | 14 (1) |
| Do not need to contact the dietitian as often | 14 (4) | 0 | 14 (4) | 18 (2) | 16 (4) | 0 |
| App Group 6 Months | Control Group 6 Months | Total 6 Months | Direct Quotes | |||
|---|---|---|---|---|---|---|
| Parent % (n = 29) | Child % (n = 11) | Parent % (n = 25) | Child % (n = 7) | Total % (n = 72) | ||
| App | 45 (13) | 27 (3) | 48 (12) | 43 (3) | 43 (31) | App preferred because it’s mobile and always with me (much easier than the sheets of paper). App is more discrete [mother of teenager] I think it will be really useful when she’s older [mother of toddler] |
| Dietitian (phone/email) | 38 (11) | 18 (2) | 52 (13) | 71 (5) | 43 (31) | I don’t think the app will ever be able to replace contacting our dietitian who has so much knowledge and experience but it’s definitely very handy and convenient when dietitian is unavailable or when you just want to double check things to be safe [mother] I would rather speak to someone re diet [mother] |
| Written/pictorial information | 28 (8) | 9 (1) | 28 (7) | 14 (1) | 24 (17) | I like the books when they arrive; they make me want to look at them and try new foods. It gives me ideas and my family always try to get me to eat different foods. I tend to stick to the same foods that I like. I don’t like change! [teenage girl] I just kept going back to using a calculator and looking in my written paper work for clarity on things, but probably would use the app more if away from home or on holiday [father of teenager] |
| Social media | 21 (6) | 9 (1) | 24 (6) | 0 | 18 (13) | Find that because I am used to using social media that is where I still tend to go back to first [mother of teenager] Currently the app does not list branded food items (like on Twitter/written information) so cannot replace those yet [mother] |
| Reading food labels | 3 (1) | 18 (2) | 0 | 0 | 4 (3) | It has helped but I have still used other ways of getting info [mother] Use a mixture of all [mother] |
| Others with PKU | 10 (3) | 0 | 8 (2) | 0 | 7 (5) | |
| Mum | 0 | 18 (2) | 4 (1) * | 14 (1) | 6 (4) | |
| NSPKU | 0 | 0 | 4 (1) | 0 | 4 (3) | |
| App Feedback | Responses | Examples of Direct Quotes |
|---|---|---|
| Positive feedback on existing functions:
| 5% (n = 4) 4% (n = 3) 2% (n = 2) |
|
Difficulties with app:
| 9% (n = 7) 11% (n = 9) 4% (n = 3) |
|
Reasons for not using the app:
| 2% (n = 2) 9% (n = 7) |
|
Ideas for additional functions:
| 11% (n = 9) 9% (n = 7) 7% (n = 6) 10% (n = 8) |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, S.; Ashmore, C.; Daly, A.; Dhadwar, P.; Syed, A.; Lecocq, O.; Jackson, R.; Pinto, A.; MacDonald, A. Efficacy of a New Low-Protein Multimedia Diet App for PKU. Nutrients 2022, 14, 2182. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112182
Evans S, Ashmore C, Daly A, Dhadwar P, Syed A, Lecocq O, Jackson R, Pinto A, MacDonald A. Efficacy of a New Low-Protein Multimedia Diet App for PKU. Nutrients. 2022; 14(11):2182. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112182
Chicago/Turabian StyleEvans, Sharon, Catherine Ashmore, Anne Daly, Perninder Dhadwar, Atif Syed, Olivia Lecocq, Richard Jackson, Alex Pinto, and Anita MacDonald. 2022. "Efficacy of a New Low-Protein Multimedia Diet App for PKU" Nutrients 14, no. 11: 2182. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112182