
Association between Intestinal Parasite Infections and Proxies for Body Composition: A Scoping Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.2.1. Study Inclusion Criteria
2.2.2. Study Exclusion Criteria
2.3. Quality Assessment of Included Studies
2.4. Data Extraction and Comparison
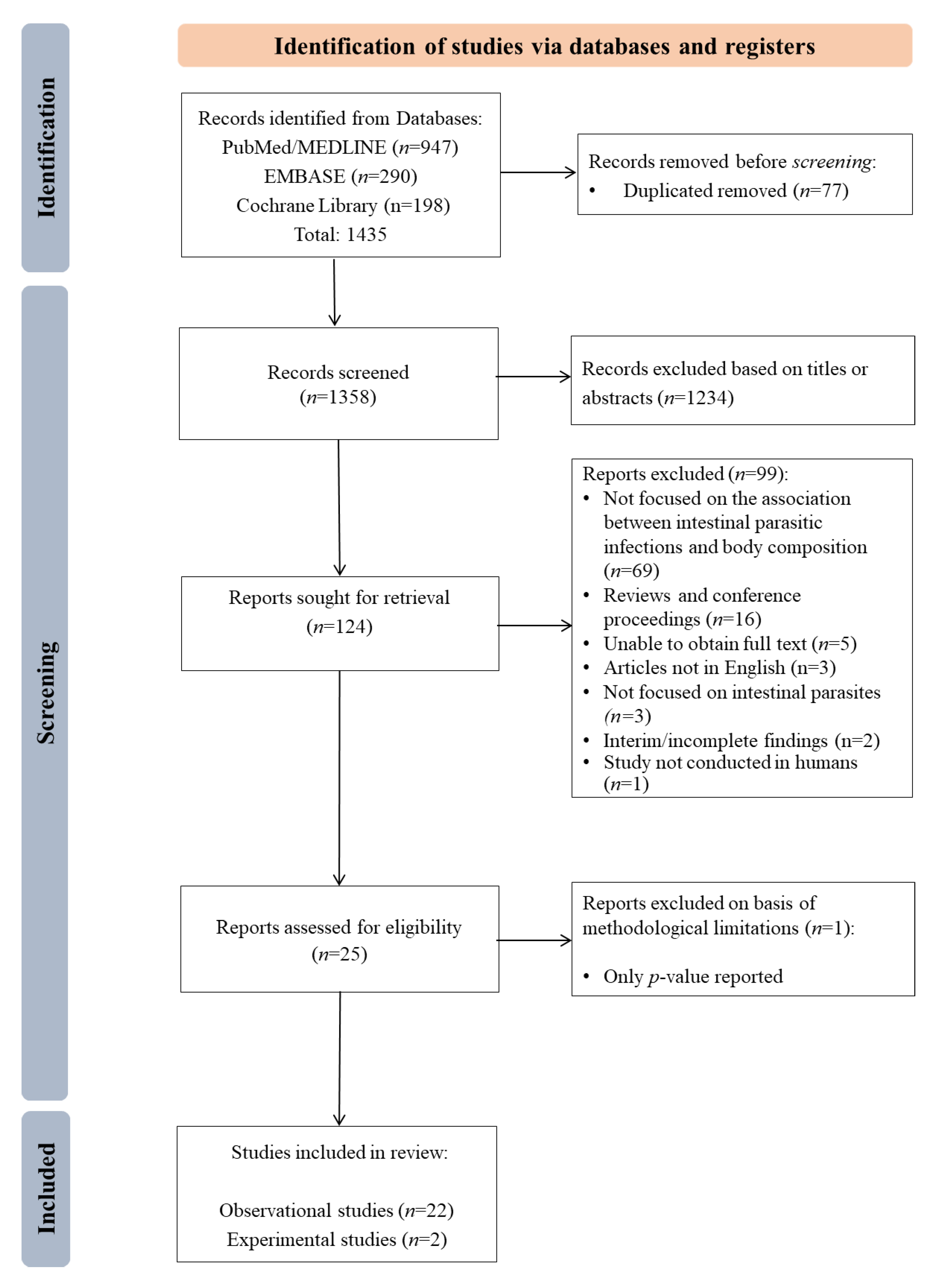
3. Results

{kind=link}
| Author, Year | Study Setting, Years | Study Design | No. of Participant | Age of the Participants | Intestinal Parasite Infections (IPI’s) Reported | Body Composition Reported | References |
|---|---|---|---|---|---|---|---|
| Amare et al., 2013 | Ethiopia, 2008 | Cross-Sectional | 405 | 12.09 ± 2.54 y | Ascaris, Hookworm, Trichuris, Strongyloides Giardia, Entamoeba spp. | BMI, BMIZ | [26] |
| Campos-Ponce et al., 2012 | Venezuela, 2010 | Cross-Sectional | 225 | 0–19 y, >19 y | Giardia, Geohelminths, IPI | BMI | [18] |
| Casapia et al., 2007 | Peru, 2005–2006 | Cross-Sectional | 252 | <5 y | Ascaris, Hookworm, Trichuris | WHZ | [27] |
| Chu et al., 2013 | Taiwan, 2010 | Cross-Sectional | 11,080 | 7–14 y | Pinworm | BMI | [28] |
| Geltman et al., 2001 | USA, 1995–1998 | Cross-Sectional | 1825 | <18 y | IPI | WHZ, BMI | [29] |
| Gerber et al., 2018 | South Africa, 2015 | Cross-Sectional | 801 | 8–12 y | Ascaris, Trichuris | BMI, Body fat | [30] |
| Jardim-Botelho et al., 2008 | Brazil, 2004 | Cross-Sectional | 1113 | 0–18, >18 y | Ascaris, Hookworm, Trichuris, Strongyloides | Triceps SF, WHZ, BMI, BMI/AGE, MUAC | [31] |
| Kurscheid et al., 2020 | Indonesia, 2015 | Cross-Sectional | 998 | 2–12 y | Ascaris, Hookworm, Trichuris | BMI | [32] |
| Lander et al., 2015 | Brazil, 2010 | Cross-Sectional | 376 | 3–6 y | Helminths | WHZ, BMI, BMIZ | [33] |
| Li et al., 2015 | China, 2012 | Cross-Sectional | 369 | 50–70 y | Hookworm, Ascaris, Protozoa, Helminths | BMI | [34] |
| Orden et al., 2014 | Argentina, 2009–2011 | Cross-Sectional | 708 | 3–11 y | Giardia, Ascaris, Trichuris | BMI, Triceps, Subscapular SF, BMIZ | [35] |
| Patel and Khandekar, 2006 | Oman, 2004–2005 | Cross-Sectional | 436 | 9–10 y | Entamoeba, Giardia, Ascaris, Trichuris, Hookworm, Strongyloides | BMI | [36] |
| Rivero et al., 2018 | Argentina, 2017 | Cross-Sectional | 303 | <15 y | Helminths (Enterobius, Hookworms, Strongyloides, Hymenolepis, Ascaris), Protozoans (Giardia, Entamoeba, Blastocystis, Chilomastix, Endolimax, Cryptosporidium, Iodamoeba) | BMIZ | [37] |
| Quihui-Cota et al., 2015 | Mexico, 2008–2009 | Cross-Sectional | 405 | 6–13 y | Cryptosporidium | BMI/AGE | [38] |
| Sanchez et al., 2013 | Honduras, 2011 | Cross-Sectional | 320 | 7–14 y | Ascaris, Hookworm, Trichuris, STH | BMI/AGE | [39] |
| Sayasone et al., 2015 | Lao PDR, 2007 | Cross-Sectional | 1313 | 6 mo–12 y | Ascaris, Hookworm, Trichuris | BMI/AGE, WHZ | [40] |
| Stephenson et al., 1989 | Kenya, 1986 | Randomized controlled trial | 150 | 6–16 y | Ascaris, Hookworm, Trichuris | WH, Triceps, subscapular SF | [41] |
| Verhagen et al., 2013 | Venezuela, 2010–2011 | Cross-Sectional | 390 | 4–6 y | Ascaris, Trichuris, Hookworm, Giardia, Strongyloides, Helminths | BMI/AGE, WHZ | [42] |
| Wiria et al., 2013a | Indonesia, 2008–2010 | Randomized controlled trial | 4004 | >2 y (at semi-urban areas) and 5–15 y (at rural areas) | Helminths, Ascaris, Hookworm, Trichuris, Strongyloides, Ancylostoma | BMI | [43] |
| Wiria et al., 2013b | Indonesia, 2009 | Cross-Sectional | 675 | 18–80 y | Ascaris, Trichuris, Strongyloides, Ancylostoma | BMI | [44] |
| Zavala et al., 2016 | Mexico, 2013 | Cross-Sectional | 296 | 6–10 y | Ascaris, Balantidium coli, Hookworm, Giardia, E. coli, E. histolytica, E. nana, | BMI/AGE, Body Composition (Body Fat) | [19] |
| Zavala et al., 2019 | Mexico, 2000, 2006 and 2012 | Ecological | 1–5 y (8927), 6–10 y (16,347) and 11–19 y (13,992) | 1–19 y | Ascaris, Protozoa | BMI/AGE | [38] |
| Zhou et al., 2007 | China, 2001–2005 | Longitudinal | 274 | 10–12 y | Ascaris, Trichuris | BMI, BMI/AGE | [34] |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO|Soil-Transmitted Helminthiases. Available online: http://www.who.int/gho/neglected_diseases/soil_transmitted_helminthiases/en/ (accessed on 16 December 2020).
- World Health Organization (WHO). Preventive Chemotherapy to Control Soil-Transmitted Helminth Infections in at-Risk Population Groups Guideline; World Health Organization: Geneva, Switzerland, 2017; ISBN 978 92 4 155011 6. [Google Scholar]
- Fact Sheets—Malnutrition. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 16 December 2020).
- Barker, D.J.P.; Eriksson, J.G.; Forsén, T.; Osmond, C. Fetal Origins of Adult Disease: Strength of Effects and Biological Basis. Int. J. Epidemiol. 2002, 31, 1235–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, J.G.; Kajantie, E.; Thornburg, K.L.; Osmond, C.; Barker, D.J.P. Mother’s Body Size and Placental Size Predict Coronary Heart Disease in Men. Eur. Heart J. 2011, 32, 2297–2303. [Google Scholar] [CrossRef] [PubMed]
- Forsén, T.; Eriksson, J.; Tuomilehto, J.; Reunanen, A.; Osmond, C.; Barker, D. The Fetal and Childhood Growth of Persons Who Develop Type 2 Diabetes. Ann. Intern. Med. 2000, 133, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Stanner, S.A.; Yudkin, J.S. Fetal Programming and the Leningrad Siege Study. Twin Res. 2001, 4, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Sawaya, A.L.; Sesso, R.; Florêncio, T.M.; Fernandes, M.T.; Martins, P.A. Association between Chronic Undernutrition and Hypertension. Matern. Child. Nutr. 2005, 1, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.J.; Martins, P.A.; Roberts, S.B.; Sawaya, A.L. Body Fat Distribution in Stunted Compared with Normal-Height Children from the Shantytowns of São Paulo, Brazil. Nutrition 2007, 23, 640–646. [Google Scholar] [CrossRef]
- Adair, L.S.; Martorell, R.; Stein, A.D.; Hallal, P.C.; Sachdev, H.S.; Prabhakaran, D.; Wills, A.K.; Norris, S.A.; Dahly, D.L.; Lee, N.R.; et al. Size at Birth, Weight Gain in Infancy and Childhood, and Adult Blood Pressure in 5 Low- and Middle-Income-Country Cohorts: When Does Weight Gain Matter? Am. J. Clin. Nutr. 2009, 89, 1383–1392. [Google Scholar] [CrossRef] [Green Version]
- Adair, L.S.; Fall, C.H.D.; Osmond, C.; Stein, A.D.; Martorell, R.; Ramirez-Zea, M.; Sachdev, H.S.; Dahly, D.L.; Bas, I.; Norris, S.A.; et al. Associations of Linear Growth and Relative Weight Gain during Early Life with Adult Health and Human Capital in Countries of Low and Middle Income: Findings from Five Birth Cohort Studies. Lancet 2013, 382, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal and Child Undernutrition Study Group Maternal and Child Undernutrition: Consequences for Adult Health and Human Capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [Green Version]
- Martins, P.A.; Hoffman, D.J.; Fernandes, M.T.B.; Nascimento, C.R.; Roberts, S.B.; Sesso, R.; Sawaya, A.L. Stunted Children Gain Less Lean Body Mass and More Fat Mass than Their Non-Stunted Counterparts: A Prospective Study. Br. J. Nutr. 2004, 92, 819–825. [Google Scholar] [CrossRef]
- Papier, K.; Williams, G.M.; Luceres-Catubig, R.; Ahmed, F.; Olveda, R.M.; McManus, D.P.; Chy, D.; Chau, T.N.P.; Gray, D.J.; Ross, A.G.P. Childhood Malnutrition and Parasitic Helminth Interactions. Clin. Infect. Dis. 2014, 59, 234–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radhakrishna, K.V.; Kulkarni, B.; Balakrishna, N.; Rajkumar, H.; Omkar, C.; Shatrugna, V. Composition of Weight Gain during Nutrition Rehabilitation of Severely under Nourished Children in a Hospital Based Study from India. Asia Pac. J. Clin. Nutr. 2010, 19, 8–13. [Google Scholar] [PubMed]
- Rajoo, Y.; Ambu, S.; Lim, Y.A.L.; Rajoo, K.; Tey, S.C.; Lu, C.W.; Ngui, R. Neglected Intestinal Parasites, Malnutrition and Associated Key Factors: A Population Based Cross-Sectional Study among Indigenous Communities in Sarawak, Malaysia. PLoS ONE 2017, 12, e0170174. [Google Scholar] [CrossRef]
- Stephenson, L.S. Helminth Parasites, a Major Factor in Malnutrition. World Health Forum 1994, 15, 169–172. [Google Scholar]
- Campos Ponce, M.; Incani, R.N.; Pinelli, E.; Ten Kulve, N.; Ramak, R.; Polman, K.; Doak, C.M. Are Intestinal Parasites Fuelling the Rise in Dual Burden Households in Venezuela? Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 119–123. [Google Scholar] [CrossRef]
- Zavala, G.A.; García, O.P.; Campos-Ponce, M.; Ronquillo, D.; Caamaño, M.C.; Doak, C.M.; Rosado, J.L. Children with Moderate-High Infection with Entamoeba Coli Have Higher Percentage of Body and Abdominal Fat than Non-Infected Children. Pediatr. Obes. 2016, 11, 443–449. [Google Scholar] [CrossRef]
- Global Nutrition Transition and the Pandemic of Obesity in Developing Countries—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/22221213/ (accessed on 16 December 2020).
- Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults during 1980–2013: A Systematic Analysis for the Global Burden of Disease Study 2013—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/24880830/ (accessed on 16 December 2020).
- Wojcicki, J.M. The Double Burden Household in Sub-Saharan Africa: Maternal Overweight and Obesity and Childhood Undernutrition from the Year 2000: Results from World Health Organization Data (WHO) and Demographic Health Surveys (DHS). BMC Public Health 2014, 14, 1124. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Site Home Page|Joanna Briggs Institute. Available online: https://jbi.global/ (accessed on 23 September 2021).
- Amare, B.; Ali, J.; Moges, B.; Yismaw, G.; Belyhun, Y.; Gebretsadik, S.; Woldeyohannes, D.; Tafess, K.; Abate, E.; Endris, M.; et al. Nutritional Status, Intestinal Parasite Infection and Allergy among School Children in Northwest Ethiopia. BMC Pediatr. 2013, 13, 7. [Google Scholar] [CrossRef] [Green Version]
- Casapía, M.; Joseph, S.A.; Núñez, C.; Rahme, E.; Gyorkos, T.W. Parasite and Maternal Risk Factors for Malnutrition in Preschool-Age Children in Belen, Peru Using the New WHO Child Growth Standards. Br. J. Nutr. 2007, 98, 1259–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, C.-H.; Wang, J.-H.; Jan, R.-H.; Huang, C.-H.; Cheng, C.-F. Association between Health Examination Items and Body Mass Index among School Children in Hualien, Taiwan. BMC Public Health 2013, 13, 975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geltman, P.L.; Radin, M.; Zhang, Z.; Cochran, J.; Meyers, A.F. Growth Status and Related Medical Conditions among Refugee Children in Massachusetts, 1995-1998. Am. J. Public Health 2001, 91, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Müller, I.; Walter, C.; du Randt, R.; Adams, L.; Gall, S.; Joubert, N.; Nqweniso, S.; Smith, D.; Steinmann, P.; et al. Physical Activity and Dual Disease Burden among South African Primary Schoolchildren from Disadvantaged Neighbourhoods. Prev. Med. 2018, 112, 104–110. [Google Scholar] [CrossRef]
- Jardim-Botelho, A.; Brooker, S.; Geiger, S.M.; Fleming, F.; Souza Lopes, A.C.; Diemert, D.J.; Corrêa-Oliveira, R.; Bethony, J.M. Age Patterns in Undernutrition and Helminth Infection in a Rural Area of Brazil: Associations with Ascariasis and Hookworm. Trop. Med. Int. Health 2008, 13, 458–467. [Google Scholar] [CrossRef] [Green Version]
- Kurscheid, J.; Laksono, B.; Park, M.J.; Clements, A.C.A.; Sadler, R.; McCarthy, J.S.; Nery, S.V.; Soares-Magalhaes, R.; Halton, K.; Hadisaputro, S.; et al. Epidemiology of Soil-Transmitted Helminth Infections in Semarang, Central Java, Indonesia. PLoS Negl. Trop. Dis. 2020, 14, e0008907. [Google Scholar] [CrossRef]
- Lander, R.L.; Williams, S.M.; Costa-Ribeiro, H.; Mattos, A.P.; Barreto, D.L.; Houghton, L.A.; Bailey, K.B.; Lander, A.G.; Gibson, R.S. Understanding the Complex Determinants of Height and Adiposity in Disadvantaged Daycare Preschoolers in Salvador, NE Brazil through Structural Equation Modelling. BMC Public Health 2015, 15, 1086. [Google Scholar] [CrossRef] [Green Version]
- Li, X.-X.; Chen, J.-X.; Wang, L.-X.; Tian, L.-G.; Zhang, Y.-P.; Dong, S.-P.; Hu, X.-G.; Liu, J.; Wang, F.-F.; Wang, Y.; et al. Prevalence and Risk Factors of Intestinal Protozoan and Helminth Infections among Pulmonary Tuberculosis Patients without HIV Infection in a Rural County in P. R. China. Acta Trop. 2015, 149, 19–26. [Google Scholar] [CrossRef]
- Orden, A.B.; Apezteguía, M.C.; Ciarmela, M.L.; Molina, N.B.; Pezzani, B.C.; Rosa, D.; Minvielle, M.C. Nutritional Status in Parasitized and Nonparasitized Children from Two Districts of Buenos Aires, Argentina. Am. J. Hum. Biol. 2014, 26, 73–79. [Google Scholar] [CrossRef]
- Patel, P.K.; Khandekar, R. Intestinal Parasitic Infections among School Children of the Dhahira Region of Oman. Saudi. Med. J. 2006, 27, 627–632. [Google Scholar]
- Rivero, M.R.; De Angelo, C.; Nuñez, P.; Salas, M.; Liang, S. Intestinal Parasitism and Nutritional Status among Indigenous Children from the Argentinian Atlantic Forest: Determinants of Enteroparasites Infections in Minority Populations. Acta Trop. 2018, 187, 248–256. [Google Scholar] [CrossRef]
- Quihui-Cota, L.; Lugo-Flores, C.M.; Ponce-Martínez, J.A.; Morales-Figueroa, G.G. Cryptosporidiosis: A Neglected Infection and Its Association with Nutritional Status in Schoolchildren in Northwestern Mexico. J. Infect. Dev. Ctries. 2015, 9, 878–883. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, A.L.; Gabrie, J.A.; Usuanlele, M.-T.; Rueda, M.M.; Canales, M.; Gyorkos, T.W. Soil-Transmitted Helminth Infections and Nutritional Status in School-Age Children from Rural Communities in Honduras. PLoS Negl. Trop. Dis. 2013, 7, e2378. [Google Scholar] [CrossRef]
- Sayasone, S.; Utzinger, J.; Akkhavong, K.; Odermatt, P. Multiparasitism and Intensity of Helminth Infections in Relation to Symptoms and Nutritional Status among Children: A Cross-Sectional Study in Southern Lao People’s Democratic Republic. Acta Trop. 2015, 141, 322–331. [Google Scholar] [CrossRef]
- Stephenson, L.S.; Latham, M.C.; Kurz, K.M.; Kinoti, S.N.; Brigham, H. Treatment with a Single Dose of Albendazole Improves Growth of Kenyan Schoolchildren with Hookworm, Trichuris Trichiura, and Ascaris Lumbricoides Infections. Am. J. Trop. Med. Hyg. 1989, 41, 78–87. [Google Scholar] [CrossRef]
- Verhagen, L.M.; Incani, R.N.; Franco, C.R.; Ugarte, A.; Cadenas, Y.; Sierra Ruiz, C.I.; Hermans, P.W.M.; Hoek, D.; Campos Ponce, M.; de Waard, J.H.; et al. High Malnutrition Rate in Venezuelan Yanomami Compared to Warao Amerindians and Creoles: Significant Associations with Intestinal Parasites and Anemia. PLoS ONE 2013, 8, e77581. [Google Scholar] [CrossRef] [Green Version]
- Wiria, A.E.; Hamid, F.; Wammes, L.J.; Kaisar, M.M.M.; May, L.; Prasetyani, M.A.; Wahyuni, S.; Djuardi, Y.; Ariawan, I.; Wibowo, H.; et al. The Effect of Three-Monthly Albendazole Treatment on Malarial Parasitemia and Allergy: A Household-Based Cluster-Randomized, Double-Blind, Placebo-Controlled Trial. PLoS ONE 2013, 8, e57899. [Google Scholar] [CrossRef]
- Wiria, A.E.; Wammes, L.J.; Hamid, F.; Dekkers, O.M.; Prasetyani, M.A.; May, L.; Kaisar, M.M.M.; Verweij, J.J.; Tamsma, J.T.; Partono, F.; et al. Relationship between Carotid Intima Media Thickness and Helminth Infections on Flores Island, Indonesia. PLoS ONE 2013, 8, e54855. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Watanabe, C.; Ohtsuka, R. Impacts of Dietary Intake and Helminth Infection on Diversity in Growth among Schoolchildren in Rural South China: A Four-Year Longitudinal Study. Am. J. Hum. Biol. 2007, 19, 96–106. [Google Scholar] [CrossRef]
- Zavala, G.A.; Doak, C.M.; Portrait, F.; Seidell, J.C.; García, O.P.; Rosado, J.L.; Jarquín, T.; Polman, K.; Campos-Ponce, M. Are Intestinal Parasites Associated with Obesity in Mexican Children and Adolescents? Parasitol. Int. 2019, 71, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Wasilewska, J.; Kaczmarski, M.G.; Sawicka-Zukowska, M.; Tomaszewska, B.; Majewska, A.; Plewa, K.; Ołdak, E.; Debkowska, K. Analysis of Clinical Symptoms and Selected Hematological Indices in Hospitalized Children with Ascaris Lumbricoides Infection from the Northeastern Region of Poland. Wiad. Parazytol. 2011, 57, 43–51. [Google Scholar]
- Kinung’hi, S.M.; Mazigo, H.D.; Dunne, D.W.; Kepha, S.; Kaatano, G.; Kishamawe, C.; Ndokeji, S.; Angelo, T.; Nuwaha, F. Coinfection of Intestinal Schistosomiasis and Malaria and Association with Haemoglobin Levels and Nutritional Status in School Children in Mara Region, Northwestern Tanzania: A Cross-Sectional Exploratory Study. BMC Res. Notes 2017, 10, 583. [Google Scholar] [CrossRef]
- Grimes, J.E.T.; Tadesse, G.; Gardiner, I.A.; Yard, E.; Wuletaw, Y.; Templeton, M.R.; Harrison, W.E.; Drake, L.J. Sanitation, Hookworm, Anemia, Stunting, and Wasting in Primary School Children in Southern Ethiopia: Baseline Results from a Study in 30 Schools. PLoS Negl. Trop. Dis. 2017, 11, e0005948. [Google Scholar] [CrossRef] [Green Version]
- Welch, V.A.; Ghogomu, E.; Hossain, A.; Awasthi, S.; Bhutta, Z.A.; Cumberbatch, C.; Fletcher, R.; McGowan, J.; Krishnaratne, S.; Kristjansson, E.; et al. Mass Deworming to Improve Developmental Health and Wellbeing of Children in Low-Income and Middle-Income Countries: A Systematic Review and Network Meta-Analysis. Lancet Glob. Health 2017, 5, e40–e50. [Google Scholar] [CrossRef] [Green Version]
- Kadakia, R.; Josefson, J. The Relationship of Insulin-Like Growth Factor 2 to Fetal Growth and Adiposity. Horm. Res. Paediatr. 2016, 85, 75–82. [Google Scholar] [CrossRef]
- Sørensen, K.; Juul, A. BMI Percentile-for-Age Overestimates Adiposity in Early Compared with Late Maturing Pubertal Children. Eur. J. Endocrinol. 2015, 173, 227–235. [Google Scholar] [CrossRef] [Green Version]

| Database | Search Terms |
|---|---|
| MEDLINE | #1 ((((body fat) OR (BMI)) OR (body composition)) OR (overweight)) OR (obesity) |
| #2 ((((((((((((((((((parasitic infections) OR (parasites)) OR (helminth)) OR (intestinal parasite)) OR (protozoa)) OR (Entamoeba coli)) OR (Giardia)) OR (Entamoeba histolytica)) OR (Cryptosporidium)) OR (Ascaris)) OR (Trichuris)) OR (Ancylostoma)) OR (Necator)) OR (hookworm)) OR (whipworm)) OR (roundworm)) OR (pinworm)) OR (deworm)) OR (Strongyloides) | |
| #3 Humans | |
| #4 (combination)—((((((body fat) OR (BMI)) OR (body composition)) OR (overweight)) OR (obesity) AND (((((((((((((((((((parasitic infections) OR (parasites)) OR (helminth)) OR (intestinal parasite)) OR (protozoa)) OR (Entamoeba coli)) OR (Giardia)) OR (Entamoeba histolytica)) OR (Cryptosporidium)) OR (Ascaris)) OR (Trichuris)) OR (Ancylostoma)) OR (Necator)) OR (hookworm)) OR (whipworm)) OR (roundworm)) OR (pinworm)) OR (deworm)) OR (Strongyloides) AND (Humans) | |
| EMBASE | #1 ‘body fat’ OR ‘bmi’ OR ‘body composition’ OR overweight OR obesity |
| #2 ‘parasitic infections’ OR parasites OR helminth OR ‘intestinal parasite’ OR protozoa OR ‘Entamoeba coli’ OR Giardia OR ‘Entamoeba histolytica’ OR ‘Cryptosporidium’ OR ‘Ascaris’ OR ‘Trichuris’ OR ‘Ancylostoma’ OR ‘Necator’ OR ‘hookworm’ OR ‘whipworm’ OR ‘roundworm OR ‘pinworm’ OR ‘deworm’ OR ‘Strongyloides’ | |
| #3 humans | |
| #4 (combination)—#1 AND #2 AND #3 | |
| Cochrane Library | #1 body fat |
| #2 BMI | |
| #3 body composition | |
| #4 overweight | |
| #5 obesity | |
| #6 (combination)—#1 OR #2 OR #3 OR #4 OR #5 | |
| #7 parasitic infections | |
| #8 parasites | |
| #9 helminth | |
| #10 intestinal parasite | |
| #11 protozoa | |
| #12 Entamoeba coli | |
| #13 Giardia | |
| #14 Entamoeba histolytica | |
| #15 Cryptosporidium | |
| #16 Ascaris | |
| #17 Trichuris | |
| #18 Ancylostoma | |
| #19 Necator | |
| #20 hookworm | |
| #21 whipworm | |
| #22 roundworm | |
| #23 pinworm | |
| #24 deworm | |
| #25 Strongyloides | |
| #26 (combination)—#7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 | |
| #27—Humans | |
| #28 (combination)—#6 AND #26 AND #27 |
| Author, Year | Study Setting, Year (s) | No. of Participants | Age of the Participants | Intestinal Parasite Infections (IPI’s) Reported | Body Composition Reported | Treatment | Follow Up | Major Outcome |
|---|---|---|---|---|---|---|---|---|
| Stephenson et al., 1989 | Kenya, 1986 | 150 | 6–16 y | Ascaris, Hookworm, Trichuris | WH, Triceps, Subscapular SF | Albendazole | 6 mo | i. The ALB group showed a larger increase in percentage of WH (4.3 percentage points) with a p-value < 0.0002; ii. The ALB group showed a larger increase in triceps SF (1.2 mm more) with a p-value < 0.0002; iii. The ALB group showed a larger increase in subscapular SF (1.2 mm more) with a p-value < 0.0002. |
| Wiria et al., 2013a | Indonesia, 2008–2010 | 4004 | 25.7 ± 18.7 y | Ascaris, Hookworm, Trichuris, Strongyloides, Ancylostoma | BMI | Albendazole | 9 mo, 21 mo | No significant change in BMI in children (9 mo follow-up: BMIZ: −0.04 (−0.17–0.09); 21 mo follow-up: BMIZ: −0.07 (−0.23–0.10)) or in adults (9 mo follow-up: BMI: −0.10 (−0.29–0.09); 21 mo follow-up: BMI: −0.15 (−0.29–0.10)) after Albendazole treatment. |
| Author, Year | Age Range | Body Composition | Intestinal Parasitic Infection | MD I vs. U | RR | OR | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Zavala et al., 2016 | 6–10 y | Body fat (%) | IPI | −0.3 | NR | NR | NR | 0.968 |
| 6–10 y | Abdominal fat (%) | IPI | −0.2 | NR | NR | NR | 0.919 | |
| 6–10 y | Body fat (kg) | IPI | 0.2 | NR | NR | NR | 0.873 | |
| 6–10 y | Abdominal fat (kg) | IPI | 0 | NR | NR | NR | 0.636 | |
| Jardim-Botelho et al., 2008 | <18 y | Low lean mass | Ascaris | NR | NR | 1.93 | 1.00–2.16 | 0.048 |
| <18 y | Low fat mass | Ascaris | NR | NR | 1.68 | 1.12–2.51 | 0.12 | |
| >18 y | Low fat mass | Ascaris | NR | NR | 1.87 | 1.07–3.28 | 0.029 | |
| >18 y | Low fat mass | Hookworm | NR | NR | 1.91 | 1.08–3.35 | 0.025 | |
| Gerber et al., 2018 | 8–12 y | Body composition | Ascaris | NR | 0.98 | NR | 0.92–1.04 | NR |
| 8–12 y | Body composition | Trichuris | NR | 0.93 | NR | 0.86–1.01 | NR | |
| 8–12 y | Body composition | Ascaris or Trichuris | NR | 0.93 | NR | 0.86–1.02 | NR |
| Author, Year | Age Range | Body Composition | Intestinal Parasite | MD I vs. U | OR | β | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Amare et al., 2013 | 12.09 ± 2.54 y | BMIZ (♀) | IPI | −0.36 c | NR | NR | NR | 0.3 |
| 12.09 ± 2.54 y | BMIZ (♂) | IPI | −0.19 c | NR | NR | NR | 0.143 | |
| Orden et al., 2014 | 3–11 y | BMIZ (Berisso) | IPI | −0.3 | NR | NR | NR | 0.138 |
| 3–11 y | BMIZ (Magdallena) | IPI | 0.00 | NR | NR | NR | 0.969 | |
| Sayasone et al., 2015 | 6 mo–12 y | <−2 BMIZ | 2 Helminths | NR | 1.40 | NR | 1.01–1.94 | NR |
| Sanchez et al., 2013 | 7–14 y | BMIZ | >3 Helminths | NR | 1.45 | NR | 1.03–2.04 | NR |
| Helminths | NR | NR | −0.06 | −0.31–0.19 | 0.622 | |||
| Verhagen et al., 2013 | 4–16 y | BMIZ or −WHZ 1 | Helminths | NR | NR | −0.24 | −0.46–−0.01 | NR |
| Quihui-Cota et al., 2015 | 6–13 y | BMIZ | Cryptosporidium | 0.05 c | NR | NR | NR | 0.68 |
| Zavala et al., 2016 | 6–10 y | BMIZ | IPI | 0.20 c | NR | NR | NR | 0.283 |
| Zavala et al., 2019 | 1–5 y | BMIZ | Ascaris | NR | NR | −0.32 | −0.33–−0.31 | <0.01 |
| 6–10 y | BMIZ | Ascaris | NR | NR | −0.21 | −0.22–0.19 | 0.01 | |
| 6–10 y | BMIZ | Protozoa | NR | NR | 0.61 | 0.59–0.63 | <0.01 | |
| 11–18 y | BMIZ | Protozoa | NR | NR | 0.85 | 0.83–0.88 | <0.01 | |
| Zhou et al., 2007 | 10–12 y | BMIZ | T. trichiura | NR | NR | −0.22 | NR | 0.001 |
| Patel and Khandekar, 2006 | 9–10 y | BMI | IPI | −0.46 | NR | NR | NR | >0.05 |
| Li et al., 2015 | 50–70 y | BMI (≤18 vs. >18) | Protozoa | NR | 3.3 | NR | 1.44–7.54 | NR |
| 50–70 y | BMI (≤18 vs. >18) | Helminths | NR | 3.32 | NR | 1.39–7.91 | NR | |
| Wiria et al., 2013b | 18–80 y | BMI | Helminths | −0.66 | NR | NR | −1.26–−0.06 | 0.031 |
| Gerber et al., 2018 | 8–12 y | BMI | Ascaris | NR | 0.91 7 | NR | 0.83–1.00 | NR |
| 8–12 y | BMI | Trichuris | NR | 0.89 7 | NR | 0.89–0.99 | NR | |
| Kurscheid et al., 2020 | 8–12 y 2–12 y | BMI BMI | Ascaris + Trichuris Ascaris and/or Trichuris and/or Hookworm | NR 0.1 c | 0.90 7 NR | NR NR | 0.82–0.99 NR | NR 0.79 |
| Casapia et al., 2007 | <5 y | WHZ < 0.2 SD | T. trichiuria | NR | 2.5 | NR | 1.06–5.93 | NR |
| <5 y | WHZ < 0.2 SD | Hookworm | NR | 6.67 | NR | 1.08–41.05 | NR | |
| <5 y | WHZ < 0.2 SD | A. lumbricoides | NR | 3.577 | NR | 1.79–7.09 | NR | |
| Campos-Ponce et al., 2012 | 0–19 y, >19 y | Overweight/obese 2 | IPI | NR | 1.47 | NR | 0.51–4.27 | 0.48 |
| Geltman et al., 2001 | <18 y | Overweight/obese 3 | IPI | NR | 0.5 | NR | 0.20–0.80 | NR |
| Rivero et al., 2018 | <15 y | Overweight/obese 4 | STH | NR | NR | 0.752 | NR | 0.33 |
| <15 y | Overweight/obese 4 | G. duodenalis | NR | −1.053 8 | NR | NR | 0.016 | |
| Chu et al., 2013 | 7–14 y | Overweight 5 | Pinworm | NR | 0.45 | NR | 0.28–0.71 | <0.01 |
| 7–14 y | Obese 6 | Pinworm | NR | 0.42 | NR | 0.26–0.70 | <0.01 | |
| Lander et al., 2015 | 3–6 y | BMIZ | Helminth | NR | NR | −0.004 9 | NR | <0.01 |
| Wasilewska et al., 2011 | 1–18 y | <1 BMIZ | Ascaris | NR | 0.98 | NR | 0.28–3.46 | 0.974 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cossa-Moiane, I.; Roucher, C.; Mac Quene, T.; Campos-Ponce, M.; de Deus, N.; Polman, K.; Doak, C. Association between Intestinal Parasite Infections and Proxies for Body Composition: A Scoping Review. Nutrients 2022, 14, 2229. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112229
Cossa-Moiane I, Roucher C, Mac Quene T, Campos-Ponce M, de Deus N, Polman K, Doak C. Association between Intestinal Parasite Infections and Proxies for Body Composition: A Scoping Review. Nutrients. 2022; 14(11):2229. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112229
Chicago/Turabian StyleCossa-Moiane, Idalécia, Clémentine Roucher, Tamlyn Mac Quene, Maiza Campos-Ponce, Nilsa de Deus, Katja Polman, and Colleen Doak. 2022. "Association between Intestinal Parasite Infections and Proxies for Body Composition: A Scoping Review" Nutrients 14, no. 11: 2229. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112229