
Dietary Intakes of Traditional Foods for Dene/Métis in the Dehcho and Sahtú Regions of the Northwest Territories


Abstract
:1. Introduction
2. Materials and Methods
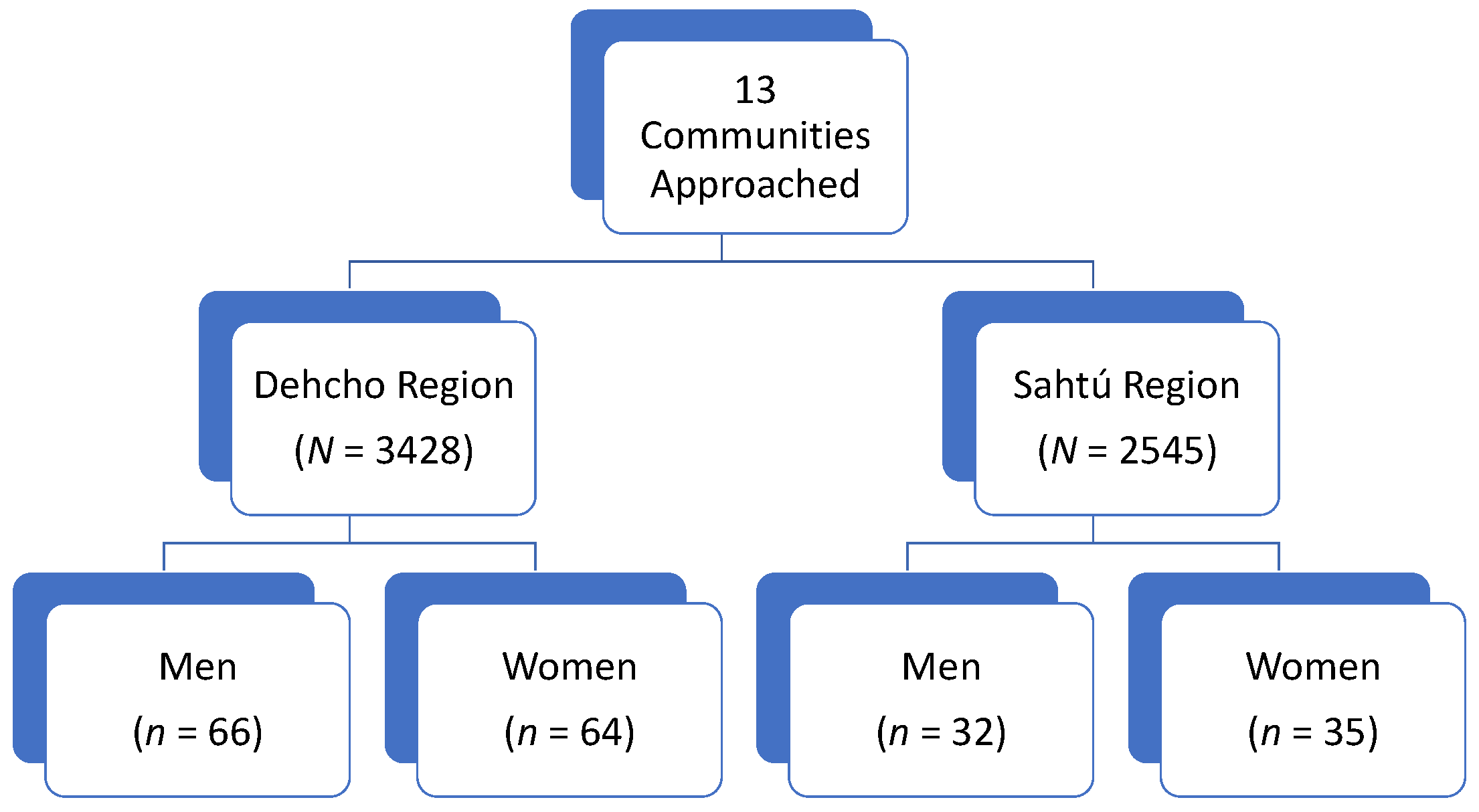
2.1. Recruitment
2.2. 24-h Dietary Recall
2.3. Analysis
2.4. Research and Ethics Licenses
3. Results
3.1. Nutrient Intake of Traditional Food
3.2. Traditional Food Consumption over Time
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Batal, M.; Chan, H.M.; Fediuk, K.; Ing, A.; Berti, P.; Sadik, T.; Johnson-Down, L. Importance of the traditional food systems for First Nations adults living on reserves in Canada. Can. J. Public Health 2021, 112, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Batal, M.; Gray-Donald, K.; Kuhnlein, H.V.; Receveur, O. Estimation of traditional food intake in indigenous communities in Denendeh and the Yukon. Int. J. Circumpolar Health 2005, 64, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Lambden, J.; Receveur, O.; Marshall, J.; Kuhnlein, H.V. Traditional and market food access in Arctic Canada is affected by economic factors. Int. J. Circumpolar Health 2006, 65, 331–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halseth, R. The Nutritional Health of the First Nations and Metis of the Northwest Territories: A Review of Current Knowledge and Gaps; National Collaborating Centre for Aboriginal Health: Prince George, BC, Canada, 2015. [Google Scholar]
- Council of Canadian Academies. Aboriginal Food Security in Northern Canada: An Assessment of the State of Knowledge; The Expert Panel on the State of Knowledge of Food Security in Northern Canada, Council of Canadian Academies: Ottawa, ON, Canada, 2014. [Google Scholar]
- Kuhnlein, H.V. Dietary Change and Traditional Food Systems of Indigenous Peoples. Annu. Rev. Nutr. 1996, 16, 417–442. [Google Scholar] [CrossRef] [PubMed]
- Kuhnlein, H.V.; Receveur, O. Local cultural animal food contributes high levels of nutrients for Arctic Canadian indigenous adults and children. J. Nutr. 2007, 137, 1110–1114. [Google Scholar] [CrossRef]
- Skinner, K.; Hanning, R.M.; Desjardins, E.; Tsuji, L.J.S. Giving voice to food insecurity in a remote indigenous community in subarctic Ontario, Canada: Traditional ways, ways to cope, ways forward. BMC Public Health 2013, 13, 427. [Google Scholar] [CrossRef] [Green Version]
- Noreen, W.; Johnson-Down, L.; Jean-Claude, M.; Lucas, M.; Robinson, E.; Batal, M. Factors associated with the intake of traditional foods in the Eeyou Istchee (Cree) of northern Quebec include age, speaking the Cree language and food sovereignty indicators. Int. J. Circumpolar Health 2018, 77, 1536251. [Google Scholar] [CrossRef] [Green Version]
- Hopping, B.N.; Erber, E.; Mead-Morse, E.; Sheehy, T.; Roache, C.; Sharma, S. Socioeconomic indicators and frequency of traditional food, junk food, and fruit and vegetable consumption amongst Inuit adults in the Canadian Arctic. J. Hum. Nutr. Diet. 2010, 23, 51–58. [Google Scholar] [CrossRef]
- Hopping, B.N.; Mead-Morse, E.; Erber, E.; Sheehy, C.; Roache, C.; Sharma, S. Dietary adequacy of Inuit in the Canadian Arctic. J. Hum. Nutr. Diet. 2010, 23, 27–34. [Google Scholar] [CrossRef]
- Batal, M.; Johnson-Down, L.; Moubarac, J.-C.; Ing, A.; Fediuk, K.; Sadik, T.; Chan, L.; Willows, N. Sociodemographic associations of the dietary proportion of ultra-processed foods in First Nations peoples in the Canadian provinces of British Columbia, Manitoba, Alberta and Ontario. Int. J. Food Sci. Nutr. 2018, 69, 753–761. [Google Scholar] [CrossRef]
- Batal, M.; Johnson-Down, L.; Moubarac, J.-C.; Ing, A.; Fediuk, K.; Sadik, T.; Tikhonov, C.; Chan, L.; Willows, N. Quantifying associations of the dietary share of ultra-processed foods with overall diet quality in First Nations peoples in the Canadian provinces of British Columbia, Alberta, Manitoba and Ontario. Public Health Nutr. 2018, 21, 103–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egeland, G.M.; Johnson-Down, L.; Cao, Z.R.; Sheikh, N.; Weiler, H. Food Insecurity and Nutrition Transition Combine to Affect Nutrient Intakes in Canadian Arctic Communities. J. Nutr. 2011, 141, 1746–1753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M. Nutritional Patterns and Transitions. Popul. Dev. Rev. 1993, 19, 138–157. [Google Scholar] [CrossRef]
- Wilk, P.; Maltby, A.; Cooke, M. Residential schools and the effects on Indigenous health and well-being in Canada—A scoping review. Public Health Rev. 2017, 38, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, A.; Levkoe, C.Z.; Andree, P.; Blay-Palmer, A.; Boulet, A.; Brockington, M.; Ferguson, R.; Galloway, T.; Martin, D.; Martorell, H.; et al. Cultivating Food Sovereignty and Sustainable Food Systems in the North: A Review and Recommendations; Food Secure Canada: Montreal, QC, Canada, 2019; p. 16. [Google Scholar]
- Receveur, O.; Boulay, M.; Kuhnlein, H.V. Decreasing traditional food use affects diet quality for adult Dene/Metis in 16 communities of the Canadian Northwest Territories. J. Nutr. 1997, 127, 2179–2186. [Google Scholar] [CrossRef]
- Kuhnlein, H.V.; Receveur, O.; Soueida, R.; Egeland, G.M. Arctic indigenous peoples experience the nutrition transition with changing dietary patterns and obesity. J. Nutr. 2004, 134, 1447–1453. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, M.; Berkes, F.; Forbes, B.; Kofinas, G.; Vlassova, T. Hunting, Herding, Fishing and Gathering: Indigenous Peoples and Renewable Resource Use in the Arctic. In Arctic Climate Impact Assessment; Cambridge University Press: Cambridge, UK, 2004; pp. 649–690. [Google Scholar]
- Johnson-Down, L.M.; Egeland, G.M. How is nutrition transition affecting dietary adequacy in Eeyouch (Cree) adults of Northern Quebec, Canada? Appl. Physiol. Nutr. Metab. 2013, 38, 300–305. [Google Scholar] [CrossRef] [Green Version]
- Gaudin, V.L.; Receveur, O.; Girard, F.; Potvin, L. Facilitators and Barriers to Traditional Food Consumption in the Cree Community of Mistissini, Northern Quebec. Ecol. Food Nutr. 2015, 54, 663–692. [Google Scholar] [CrossRef]
- Rosol, R.; Powell-Hellyer, S.; Chan, H.M. Impacts of decline harvest of country food on nutrient intake among Inuit in Arctic Canada: Impact of climate change and possible adaptation plan. Int. J. Circumpolar Health 2016, 75, 31127. [Google Scholar] [CrossRef]
- Pal, S.; Haman, F.; Robidoux, M.A. The Costs of Local Food Procurement in Two Northern Indigenous Communities in Canada. Food Foodways 2013, 21, 132–152. [Google Scholar] [CrossRef]
- Randazzo, M.L.; Robidoux, M.A. The costs of local food procurement in a Northern Canadian First Nation community: An affordable strategy to food security? J. Hunger. Environ. Nutr. 2018, 14, 662–682. [Google Scholar] [CrossRef]
- Laird, M.J.; Henao, J.J.A.; Reyes, E.S.; Stark, K.D.; Low, G.; Swanson, H.K.; Laird, B.D. Mercury and omega-3 fatty acid profiles in freshwater fish of the Dehcho Region, Northwest Territories: Informing risk benefit assessments. Sci. Total Environ. 2018, 637, 1508–1517. [Google Scholar] [CrossRef] [PubMed]
- Pontual, M.D.M.; Ayotte, P.; Little, M.; Furgal, C.; Boyd, A.D.; Muckle, G.; Avard, E.; Ricard, S.; Gauthier, M.-J.; Sidi, E.A.-L.; et al. Seasonal variations in exposure to methylmercury and its dietary sources among pregnant Inuit women in Nunavik, Canada. Sci. Total Environ. 2021, 755, 143196. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Geography; Parliament of Canada: Ottawa, ON, Canada, 2011; pp. 208–221.
- Ratelle, M.; Haig, L.; Laird, B.D.; Skinner, K. Game bird consumption in Dene communities of the Northwest Territories, Canada. Public Health Nutr. 2021, 24, 1229–1239. [Google Scholar] [CrossRef]
- Ratelle, M.; Skinner, K.; Laird, M.; Majowicz, S.; Brandow, D.; Packull-McCormick, S.; Bouchard, M.; Dieme, D.; Stark, K.D.; Henao, J.J.A.; et al. Implementation of human biomonitoring in the Dehcho region of the Northwest Territories, Canada (2016–2017). Arch. Public Health 2018, 76, 73. [Google Scholar] [CrossRef] [Green Version]
- Ratelle, M.; Laird, M.; Majowicz, S.; Skinner, K.; Swanson, H.; Laird, B. Design of a human biomonitoring community-based project in the Northwest Territories Mackenzie Valley, Canada, to investigate the links between nutrition, contaminants and country foods. Int. J. Circumpolar Health 2018, 77, 1510714. [Google Scholar] [CrossRef] [Green Version]
- Centre for Indigenous Peoples Nutrition and Environment. Variance in Food Use in Dene/Metis Communities; McGill University: McGill, QC, Canada, 1996. [Google Scholar]
- First Nations Information Governance Centre. The First Nations Principles of OCAP®. Available online: https://fnigc.ca/ocap-training/ (accessed on 22 November 2021).
- NWT Bureau of Statistics. 2018 Summary of NWT Community Statistics; Government of the Northwest Territories: Yellowknife, NT, Canada, 2018.
- Ratelle, M.; Skinner, K.; Packull-McCormick, S.; Laird, B. Food frequency questionnaire assessing traditional food consumption in Dene/Métis communities, Northwest Territories, Canada. Int. J. Circumpolar Health 2020, 79, 1760071. [Google Scholar] [CrossRef]
- Brandow, D. Country Food Consumption Notices: Assessing Awareness and Preferences of Health and Risk Communication Messages in the Sahtú Region of the Northwest Territories. Master’s Thesis, University Of Waterloo, Waterloo, ON, Canada, 2018. [Google Scholar]
- Skinner, K.; Ratelle, M.; Brandow, D.; Packull-Mccormick, S.; Laird, B. Results Report: Health Messages Survey. Contaminant Biomonitoring in the Northwest Territories Mackenzie Valley: Investigating the Links Between Contaminant Exposure, Nutritional Status, and Country Food Use; University Of Waterloo: Waterloo, ON, Canada, 2019. [Google Scholar]
- Hanning, R.M.; Royall, D.; Toews, J.E.; Blashill, L.; Wegener, J.; Driezen, P. Web-based food behaviour questionnaire: Validation with grades six to eight students. Can. J. Diet. Pract. Res. 2009, 70, 172–178. [Google Scholar] [CrossRef]
- McCargar, L.; Hanning, R.M.; Jessup, L.; Lambraki, I.; MacDonald, C.; Minaker, L. A web-based approach to assessment of food intake and behaviour of school children and adolescents. Can. J. Diet. Pract. Res. 2003, 64, S110. [Google Scholar]
- Hanning, R.M.; Woodruff, S.J.; Lambraki, I.; Jessup, L.; Driezen, P.; Murphy, C.C. Nutrient intakes and food consumption patterns among Ontario students in grades six, seven and eight. Can. J. Public Health 2007, 98, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Storey, K.E.; Forbes, L.E.; Fraser, S.N.; Spence, J.C.; Plotnikoff, R.C.; Raine, K.D.; Hanning, R.M.; Mccargar, L.J. Diet quality, nutrition and physical activity among adolescents: The Web-SPAN (Web-Survey of Physical Activity and Nutrition) project. Public Health Nutr. 2009, 12, 2009–2017. [Google Scholar] [CrossRef] [Green Version]
- Vance, V.A.; Woodruff, S.J.; McCargar, L.J.; Husted, J.; Hanning, R.M. Self-reported dietary energy intake of normal weight, overweight and obese adolescents. Public Health Nutr. 2009, 12, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Woodruff, S.J.; Hanning, R.M.; McGoldrick, K.; Brown, K.S. Healthy eating index-C is positively associated with family dinner frequency among students in grades 6–8 from Southern Ontario, Canada. Eur. J. Clin. Nutr. 2010, 64, 454–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodruff, S.J.; Hanning, R.M.; Mcgoldrick, K. The Influence of Physical and Social Contexts of Eating on Lunch-Time Food Intake Among Southern Ontario, Canada, Middle School Students. J. Sch. Health 2010, 80, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, S.J.; Hanning, R.M. Effect of Meal Environment On Diet Quality Rating. Artic. Can. J. Diet. Pract. Res. 2009, 70, 118–124. [Google Scholar] [CrossRef]
- Gates, A.; Hanning, R.M.; Gates, M.; Skinner, K.; Martin, I.D.; Tsuji, L.J.S. Vegetable and Fruit Intakes of On-Reserve First Nations Schoolchildren Compared to Canadian Averages and Current Recommendations. Int. J. Environ. Res. Public Health 2012, 9, 1379–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, K.; Hanning, R.M.; Sutherland, C.; Edwards-Wheesk, R.; Tsuji, L.J.S. Using a SWOT analysis to inform healthy eating and physical activity strategies for a remote first nations community in Canada. Am. J. Health Promot. 2012, 26, e159–e171. [Google Scholar] [CrossRef] [PubMed]
- Skinner, K.; Hanning, R.M.; Metatawabin, J.; Martin, I.D.; Tsuji, L.J.S. Impact of a school snack program on the dietary intake of grade six to ten first nation students living in a remote community in Northern Ontario, Canada. Rural Remote Health 2012, 12, 2122. [Google Scholar] [CrossRef] [PubMed]
- Wein, E.E.; Freeman, M.M. Frequency of Traditional Food Use by Three Yukon First Nations Living in Four Communities. Arctic 1995, 48, 161–171. [Google Scholar] [CrossRef]
- Health Canada. Eating Well with Canada’s Food Guide; Health Canada: Toronto, ON, Canada, 2007.
- Health Canada. Canadian Nutrient File (CNF); Health Canada: Toronto, ON, Canada, 2021.
- Health Canada. Eating Well with First Nations, Inuit and Métis; Health Canada: Toronto, ON, Canada, 2007.
- Berkey, C.S.; Rockett, H.R.H.; Field, A.E.; Gillman, M.W.; Frazier, A.L.; Camargo, C.A., Jr.; Colditz, G.A. Activity, dietary intake, and weight changes in a longitudinal study of preadolescent and adolescent boys and girls. Pediatrics 2000, 105, e56. [Google Scholar] [CrossRef] [Green Version]
- Kuhnlein, H.V.; Barthet, V.; Farren, A.; Falahi, E.; Leggee, D.; Receveur, O.; Berti, P. Vitamins A, D, and E in Canadian Arctic traditional food and adult diets. J. Food Compos. Anal. 2006, 19, 495–506. [Google Scholar] [CrossRef]
- Batal, M.; Chan, H.M.; Ing, A.; Fediuk, K.; Berti, P.; Sadik, T.; Johnson-Down, L. Nutrient adequacy and nutrient sources of adults among ninety-two First Nations communities across Canada. Can. J. Public Health 2021, 112, 29–40. [Google Scholar] [CrossRef]
- Morton, V.; Manore, A.; Ciampa, N.; Glass-Kaastra, S.; Hurst, M.; Mullen, A.; Cutler, J. Country food consumption in Yukon, Northwest Territories and Nunavut, Foodbook study 2014–2015. Can. Commun. Dis. Rep. 2021, 47, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Willows, N.D. Determinants of Healthy Eating in Aboriginal Peoples in Canada The Current State of Knowledge and Research Gaps. Can. J. Public Health 2005, 96, S32–S41. [Google Scholar]
- Phillipps, B.; Ratelle, M.; Skinner, K.; Laird, B.D.; Andrew, L.; Yakeleya, J.; Jensen, K.; Simmons, D. Food Security and Resiliency in the Face of Climate Change: From Assessment to Improvement in the Sahtú Region. In Food Security Survey Results; Sahtú Renewable Resources Board: Tulita, NT, Canada; University of Waterloo: Waterloo, ON, Canada, 2020. [Google Scholar]
- Tarasuk, V.; Mitchell, A. Household Food Insecurity in Canada, 2017–2018; Research to identify policy options to reduce food insecurity (PROOF): Toronto, ON, Canada, 2020. [Google Scholar]
- Dehcho First Nations. Dehcho Regional Investment Plan; Dehcho First Nations: Fort Simpson, NT, Canada, 2009. [Google Scholar]
- Social Justice Fund Breakfast for Learning Northwest Territories. Available online: http://psac-sjf.org/breakfast-learning-northwest-territories (accessed on 1 April 2021).
- Food First Foundation Programs. Available online: http://www.unw.ca/social-justice-and-community-partnerships (accessed on 1 April 2021).
- Ford, J.D.; Lardeau, M.-P.; Blackett, H.; Chatwood, S.; Kurszewski, D. Community food program use in Inuvik, Northwest Territories. BMC Public Health 2013, 13, 970. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.C.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Gates, A.; Skinner, K.; Gates, M. The diets of school-aged Aboriginal youths in Canada: A systematic review of the literature. J. Hum. Nutr. Diet. 2015, 28, 246–261. [Google Scholar] [CrossRef]
- Hoover, E. Cultural and health implications of fish advisories in a native American community. Ecol. Process. 2013, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Resnicow, K.; Odom, E.; Wang, T.; Dudley, W.N.; Mitchell, D.; Vaughan, R.; Jackson, A.; Baranowski, T. Validation of Three Food Frequency Questionnaires and 24-Hour Recalls with Serum Carotenoid Levels in a Sample of African-American Adults. Am. J. Epidemiol. 2000, 152, 1072–1080. [Google Scholar] [CrossRef]
- Roberto, C.A.; Pomeranz, J.L.; Fisher, J.O. The need for public policies to promote healthier food consumption: A comment on Wansink and Chandon. J. Consum. Psychol. 2014, 24, 438–445. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Region and Demographic | Energy (kcal) | Carbohydrate (% Energy) | Protein (% Energy) | Fat (% Energy) | Saturated Fat (g) | Energy from TF (% Total Energy) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| With TF | ±SD | W/O TF | ±SD | With TF | ±SD | W/O TF | ±SD | With TF | ±SD | W/O TF | ±SD | With TF | ±SD | W/O TF | ±SD | With TF | ±SD | W/O TF | ±SD | With TF | ±SD | W/O TF | ±SD | |
| All Adults | 2144 | 913 | 1959 | 822 | 39 | 9 | 44 | 11 | 25 | 8 | 17 | 6 | 37 | 8 | 40 | 9 | 33 | 18 | 33 | 17 | 17 | 9 | NA | NA |
| All Children | 2190 | 962 | 1655 | 738 | 50 | 11 | 51 | 13 | 21 | 6 | 15 | 5 | 31 | 11 | 34 | 10 | 29 | 17 | 24 | 16 | 13 | 5 | NA | NA |
| Dehcho Adults | 2080 | 801 | 1872 | 874 | 40 | 9 | 44 | 12 | 26 | 9 | 16 | 6 | 36 | 7 | 41 | 9 | 29 | 14 | 33 | 19 | 18 | 9 | NA | NA |
| Dehcho Children | 2417 | 727 | 1710 | 883 | 48 | 8 | 50 | 14 | 21 | 6 | 16 | 5 | 33 | 9 | 35 | 11 | 32 | 15 | 25 | 17 | 12 | 6 | NA | NA |
| Sahtú Adults | 2235 | 1064 | 2162 | 656 | 39 | 10 | 45 | 10 | 24 | 5 | 19 | 4 | 37 | 8 | 36 | 9 | 38 | 21 | 32 | 14 | 16 | 8 | NA | NA |
| Sahtú Children | NA | NA | 1572 | 459 | NA | NA | 53 | 11 | NA | NA | 13 | 4 | NA | NA | 34 | 8 | NA | NA | 23 | 16 | NA | NA | NA | NA |
| All Regions | Dehcho | Sahtú | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Men | Women | Total | Men | Women | Total | Men | Women | |
| % Average Energy from TF | 5.1 | 5.1 | 5.2 | 5.0 | 4.5 | 5.5 | 5.4 | 6.3 | 4.5 |
| Age (years) | |||||||||
| 6–17 | 2.5 | 1.3 | 3.6 | 3.2 | 2.1 | 4.3 | 1.1 | 0.0 | 2.3 |
| 18–50 | 4.6 | 5.7 | 3.5 | 4.1 | 3.8 | 4.4 | 5.7 | 2.3 | 1.7 |
| 51+ | 7.4 | 6.4 | 8.4 | 7.7 | 7.3 | 8.2 | 6.8 | 5.1 | 8.8 |
| Refusal | 9.8 | ||||||||
| Adults | Children | |||||
|---|---|---|---|---|---|---|
| Region | Total | % with TF | % without TF | Total | % with TF | % without TF |
| All (n = 197) | 153 | 35 | 65 | 44 | 20 | 80 |
| Dehcho | 101 | 31 | 69 | 29 | 28 | 72 |
| Sahtú | 52 | 42 | 58 | 15 | 7 a | 93 |
| Nutrients (Average) | CINE (1994) a n = 1007 | Mackenzie Valley Project (2016–2018) n = 153 | ||||||
|---|---|---|---|---|---|---|---|---|
| With TF | ±SD | Without TF | ±SD | With TF n = 54 | ±SD | Without TF n = 99 | ±SD | |
| Energy (kcal) | 2261 | 39 | 2085 | 55 | 2144 | 913 | 1959 | 822 |
| Carbohydrate (% energy) | 35 | 1 | 47 | 1 | 39 | 9 | 44 | 11 |
| Protein (% energy) | 31 | 1 | 20 | 1 | 25 | 8 | 17 | 6 |
| Fat (% energy) | 34 | 1 | 39 | 1 | 37 | 8 | 40 | 9 |
| Saturated Fat (g) | 12 | 1 | 14 | 1 | 33 | 18 | 33 | 17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramirez Prieto, M.; Ratelle, M.; Laird, B.D.; Skinner, K. Dietary Intakes of Traditional Foods for Dene/Métis in the Dehcho and Sahtú Regions of the Northwest Territories. Nutrients 2022, 14, 378. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020378
Ramirez Prieto M, Ratelle M, Laird BD, Skinner K. Dietary Intakes of Traditional Foods for Dene/Métis in the Dehcho and Sahtú Regions of the Northwest Territories. Nutrients. 2022; 14(2):378. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020378
Chicago/Turabian StyleRamirez Prieto, Maria, Mylène Ratelle, Brian Douglas Laird, and Kelly Skinner. 2022. "Dietary Intakes of Traditional Foods for Dene/Métis in the Dehcho and Sahtú Regions of the Northwest Territories" Nutrients 14, no. 2: 378. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020378