
Clinical Impact of Nutritional Status and Sarcopenia in Pediatric Patients with Bone and Soft Tissue Sarcomas: A Pilot Retrospective Study (SarcoPed)

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Endpoints
- -
- To describe the clinical characteristics, nutritional status (defined by the BMI and the PNI), and the presence of sarcopenia (defined by the measurement of tPMA detected by axial CT images of the L4–L5 vertebrae) at diagnosis and after 12 months of chemotherapy in pediatric patients with bone and soft tissue sarcomas.
- -
- To evaluate the association between clinical characteristics, nutritional status, and the presence of sarcopenia (at diagnosis) with overall survival (OS);
- -
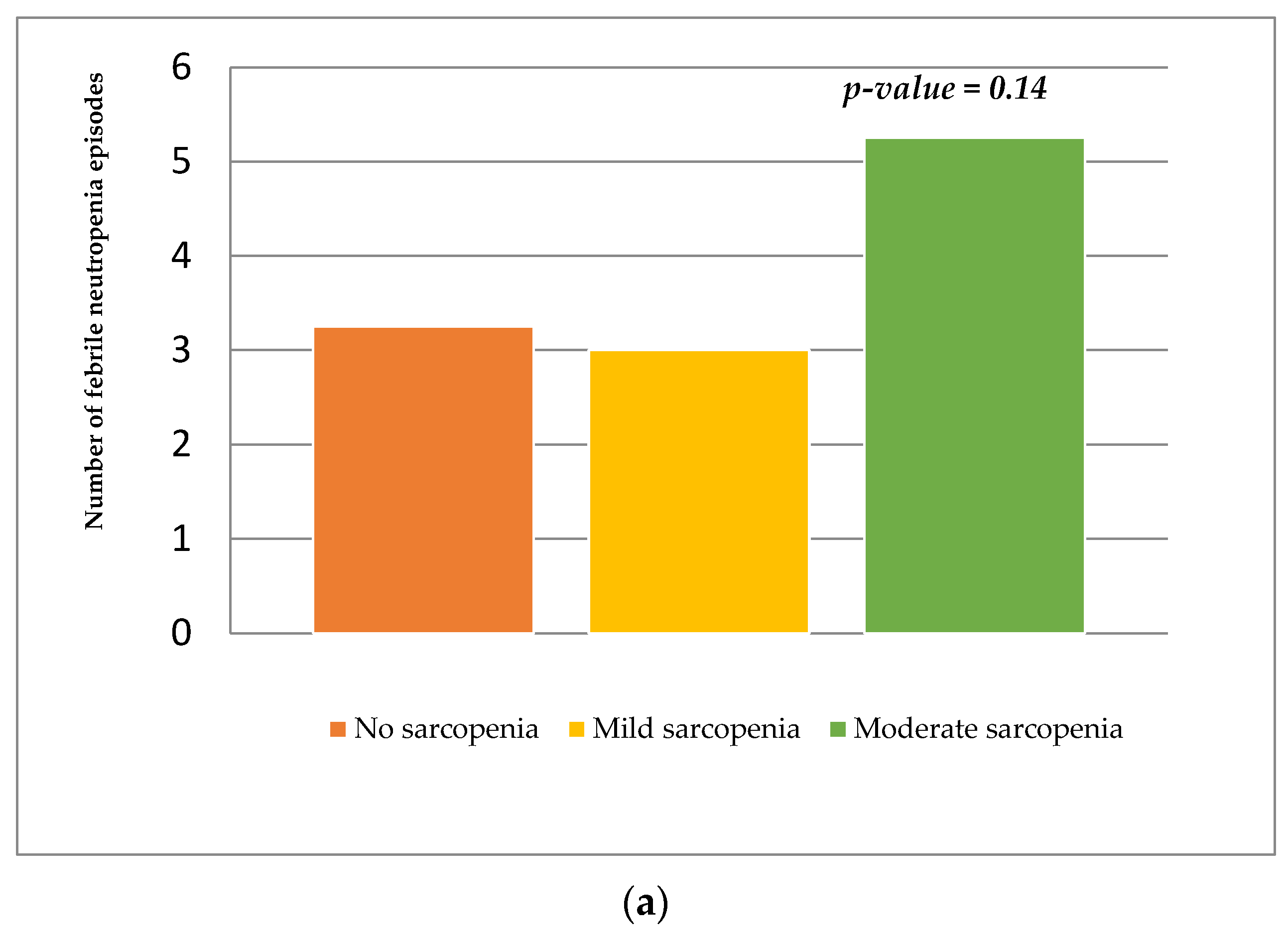
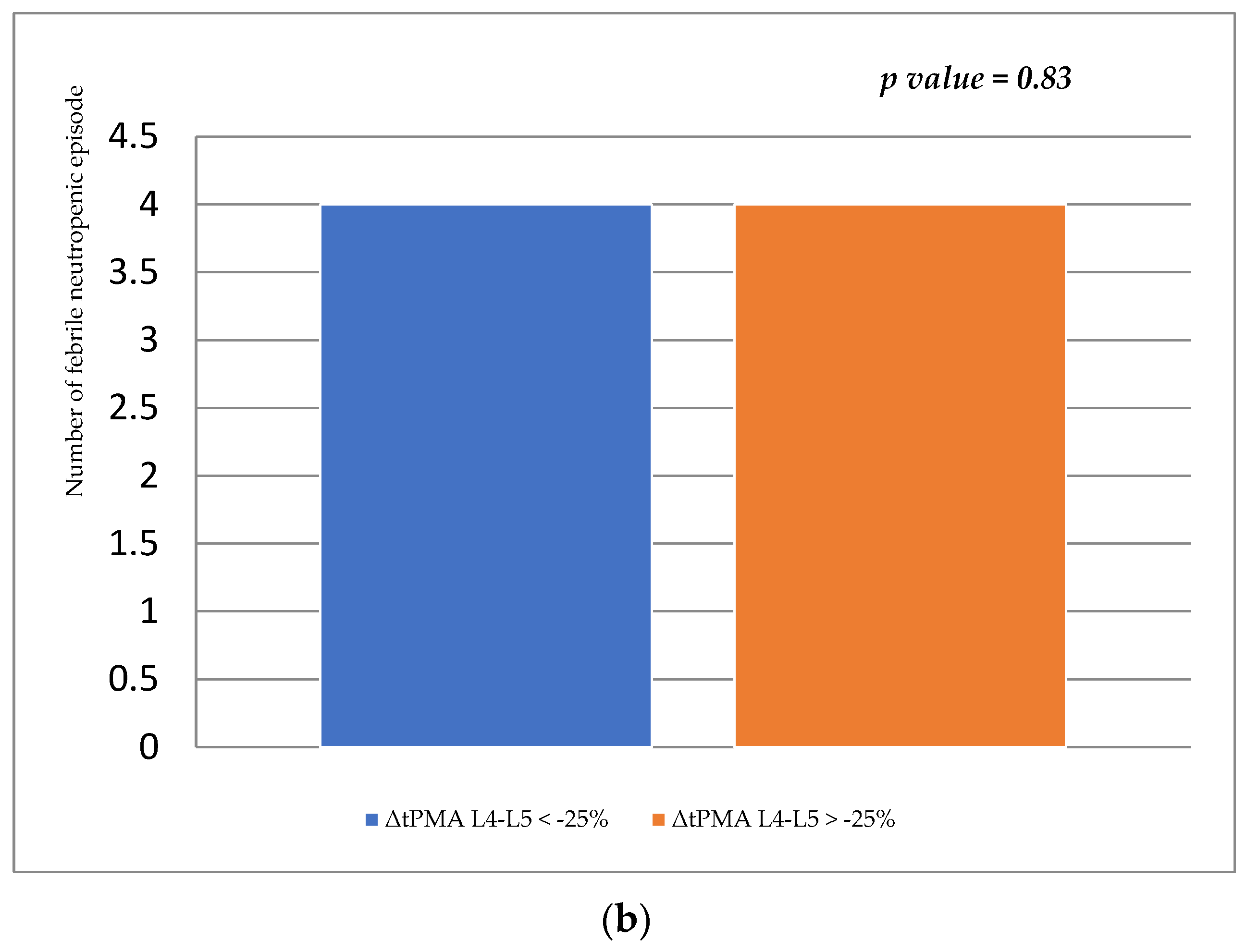
- To evaluate the association between the presence of sarcopenia (at diagnosis) with any infectious complications due to treatment (defined as the number of hospitalizations for febrile neutropenia in the 12 months of observation).
2.2. Study Design, Patients’ Characteristics, Ethical Approval, Inclusion, and Exclusion Criteria
2.3. Clinical Data and Nutritional Assessment
- -
- Demographic characteristics (age, sex, ethnicity);
- -
- Data related to the neoplastic disease (histology, primarily affected site, date of diagnosis, and presence of metastasis at diagnosis);
- -
- Type and duration of the treatment (chemotherapy protocol, radiotherapy, and high-dose chemotherapy with autologous transplantation);
- -
- Surgery during the 12 months of observation;
- -
- Five-year OS defined as the time from the day of diagnosis to death from any cause in five years after diagnosis;
- -
- Data on treatment-related infectious complications (febrile neutropenia that required hospitalization and intravenous antibiotic therapy) in the 12 months of observation.
2.4. Sample Size and Statistical Analysis
3. Results
3.1. Clinical Characteristics, Nutritional Status, Sarcopenia at Diagnosis and 12 Months
3.2. Association between Clinical Characteristics, Nutritional Status, Sarcopenia, and Overall Survival
3.3. Association between Sarcopenia and Infectious Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehta, N.M.; Corkins, M.R.; Lyman, B.; Malone, A.; Goday, P.S.; Carney, L.N.; Monczka, J.L.; Plogsted, S.W.; Schwenk, W.F. Defining pediatric malnutrition: A paradigm shift toward etiology-related definitions. JPEN J. Parenter. Enteral Nutr. 2013, 37, 460–481. [Google Scholar] [CrossRef] [Green Version]
- Beer, S.S.; Juarez, M.D.; Vega, M.W.; Canada, N.L. Pediatric malnutrition: Putting the new definition and standards into practice. Nutr. Clin. Pract. 2015, 30, 609–624. [Google Scholar] [CrossRef] [Green Version]
- Joosten, K.F.; Hulst, J.M. Prevalence of malnutrition in pediatric hospital patients. Curr. Opin. Pediatr. 2008, 20, 590–596. [Google Scholar] [CrossRef]
- Hartman, C.; Shamir, R.; Hecht, C.; Koletzko, B. Malnutrition screening tools for hospitalized children. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Axelson, I.; Colomb, V.; Goulet, O.; Koletzko, B.; Michaelsen, K.F.; Puntis, J.W.; Rigo, J.; Shamir, R.; Szajewska, H.; et al. ESPGHAN Committee on Nutrition; European Society for Paediatric Gastroenterology. The need for nutrition support teams in pediatric units: A commentary by the ESPGHAN committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.F.; Viana, K.D. Nutritional screening in hospitalized pediatric patients: A systematic review. J. Pediatr. 2016, 92, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Rinninella, E.; Ruggiero, A.; Maurizi, P.; Triarico, S.; Cintoni, M.; Mele, M.C. Clinical tools to assess nutritional risk and malnutrition in hospitalized children and adolescents. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2690–2701. [Google Scholar] [PubMed]
- Iniesta, R.R.; Paciarotti, I.; Brougham, M.F.; McKenzie, J.M.; Wilson, D.C. Effects of pediatric cancer and its treatment on nutritional status: A systematic review. Nutr. Rev. 2015, 73, 276–295. [Google Scholar] [CrossRef]
- Zimmermann, K.; Ammann, R.A.; Kuehni, C.E.; De Geest, S.; Cignacco, E. Malnutrition in pediatric patients with cancer at diagnosis and throughout therapy: A multicenter cohort study. Pediatr. Blood Cancer 2013, 60, 642–649. [Google Scholar] [CrossRef]
- Loeffen, E.A.; Brinksma, A.; Miedema, K.G.; de Bock, G.H.; Tissing, W.J. Clinical implications of malnutrition in childhood cancer patients--infections and mortality. Support. Care Cancer 2015, 23, 143–150. [Google Scholar] [CrossRef]
- Joffe, L.; Schadler, K.L.; Shen, W.; Ladas, E.J. Body Composition in Pediatric Solid Tumors: State of the Science and Future Directions. J. Natl. Cancer Inst. Monogr. 2019, 54, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Triarico, S.; Rinninella, E.; Cintoni, M.; Capozza, M.A.; Mastrangelo, S.; Mele, M.C.; Ruggiero, A. Impact of malnutrition on survival and infections among pediatric patients with cancer: A retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1165–1175. [Google Scholar]
- Ikeya, T.; Shibutani, M.; Maeda, K.; Sugano, K.; Nagahara, H.; Ohtani, H.; Hirakawa, K. Maintenance of the nutritional prognostic index predicts survival in patients with unresectable metastatic colorectal cancer. J. Cancer Res. Clin. Oncol. 2015, 141, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Hofbauer, S.L.; Pantuck, A.J.; de Martino, M.; Lucca, I.; Haitel, A.; Shariat, S.F.; Belldegrun, A.S.; Klatte, T. The preoperative prognostic nutritional index is an independent predictor of survival in patients with renal cell carcinoma. Urol. Oncol. 2015, 33, 68.e1–68.e7. [Google Scholar] [CrossRef]
- Miao, J.; Xiao, W.; Wang, L.; Han, F.; Wu, H.; Deng, X.; Guo, X.; Zhao, C. The value of the Prognostic Nutritional Index (PNI) in predicting outcomes and guiding the treatment strategy of nasopharyngeal carcinoma (NPC) patients receiving intensity-modulated radiotherapy (IMRT) with or without chemotherapy. J. Cancer Res. Clin. Oncol. 2017, 143, 1263–1273. [Google Scholar] [CrossRef]
- Zhang, H.; Shang, X.; Ren, P.; Gong, L.; Ahmed, A.; Ma, Z.; Wu, X.; Xiao, X.; Jiang, H.; Tang, P.; et al. The predictive value of a preoperative systemic immune-inflammation index and prognostic nutritional index in patients with esophageal squamous cell carcinoma. J. Cell Physiol. 2019, 234, 1794–1802. [Google Scholar] [CrossRef]
- Ooi, P.H.; Thompson-Hodgetts, S.; Pritchard-Wiart, L.; Gilmour, S.M.; Mager, D.R. Pediatric Sarcopenia: A Paradigm in the Overall Definition of Malnutrition in Children? JPEN J. Parenter. Enteral Nutr. 2020, 44, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Salini, S.; Sisto, A.; Picca, A.; et al. Sarcopenia: An Overview on Current Definitions, Diagnosis and Treatment. Curr. Protein Pept. Sci. 2018, 19, 633–638. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.; Narici, M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marhold, M.; Topakian, T.; Unseld, M. Sarcopenia in cancer—a focus on elderly cancer patients. memo-Mag. Eur. Med. Oncol. 2021, 14, 20–23. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; Macdonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Lai, H.J. Classification of nutritional status in cystic fibrosis. Curr. Opin. Pulm. Med. 2006, 12, 422–427. [Google Scholar] [CrossRef]
- Kim, S.; Koh, H. Nutritional aspect of pediatric inflammatory bowel disease: Its clinical importance. Korean J. Pediatr. 2015, 58, 363–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho do Nascimento, P.R.; Poitras, S.; Bilodeau, M. How do we define and measure sarcopenia? Protocol for a systematic review. Syst. Rev. 2018, 7, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abd Aziz, N.A.S.; Teng, N.; Abdul Hamid, M.R.; Ismail, N.H. Assessing the nutritional status of hospitalized elderly. Clin. Interv. Aging 2017, 12, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- Orsso, C.E.; Tibaes, J.R.B.; Oliveira, C.L.P.; Rubin, D.A.; Field, C.J.; Heymsfield, S.B.; Prado, C.M.; Haqq, A.M. Low muscle mass and strength in pediatric patients: Why should we care? Clin. Nutr. 2019, 38, 2002–2015. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Fielding, R.; Visser, M.; van Loon, L.J.; Rolland, Y.; Orwoll, E.; Reid, K.; Boonen, S.; Dere, W.; Epstein, S.; et al. Tools in the assessment of sarcopenia. Calcif. Tissue Int. 2013, 93, 201–210. [Google Scholar] [CrossRef]
- Anjanappa, M.; Corden, M.; Green, A.; Roberts, D.; Hoskin, P.; McWilliam, A.; Choudhury, A. Sarcopenia in cancer: Risking more than muscle loss. Tech. Innov. Patient Support Radiat. Oncol. 2020, 16, 50–57. [Google Scholar] [CrossRef]
- Amini, B.; Boyle, S.P.; Boutin, R.D.; Lenchik, L. Approaches to assessment of muscle mass and myosteatosis on computed tomography (CT): A systematic review. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1671–1678. [Google Scholar] [CrossRef] [PubMed]
- Moisey, L.L.; Mourtzakis, M.; Cotton, B.A.; Premji, T.; Heyland, D.K.; Wade, C.E.; Bulger, E.; Kozar, R.A. Nutrition and Rehabilitation Investigators Consortium (NUTRIC). Skeletal muscle predicts ventilator-free days, ICU-free days, and mortality in elderly ICU patients. Crit. Care 2013, 17, R206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akahoshi, T.; Yasuda, M.; Momii, K.; Kubota, K.; Shono, Y.; Kaku, N.; Tokuda, K.; Nagata, T.; Yoshizumi, T.; Shirabe, K. Sarcopenia is a predictive factor for prolonged intensive care unit stays in high-energy blunt trauma patients. Acute Med. Surg. 2016, 3, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Yeh, D.D.; Ortiz-Reyes, L.A.; Quraishi, S.A.; Chokengarmwong, N.; Avery, L.; Kaafarani, H.M.A.; Lee, J.; Fagenholz, P.; Chang, Y.; DeMoya, M.; et al. Early nutritional inadequacy is associated with psoas muscle deterioration and worse clinical outcomes in critically ill surgical patients. J. Crit. Care 2018, 45, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Giusto, M.; Lattanzi, B.; Albanese, C.; Galtieri, A.; Farcomeni, A.; Giannelli, V.; Lucidi, C.; Di Martino, M.; Catalano, C.; Merli, M. Sarcopenia in liver cirrhosis: The role of computed tomography scan for the assessment of muscle mass compared with dual-energy X-ray absorptiometry and anthropometry. Eur. J. Gastroenterol. Hepatol. 2015, 27, 328–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Vugt, J.L.A.; Levolger, S.; de Bruin, R.W.F.; van Rosmalen, J.; Metselaar, H.J.; Ijzermans, J.N.M. Systematic review and meta-analysis of the impact of computed tomography-assessed skeletal muscle mass on outcome in patients awaiting or undergoing liver transplantation. Am. J. Transplant. 2016, 16, 2277–2292. [Google Scholar] [CrossRef]
- Lurz, E.; Patel, H.; Lebovic, G.; Quammie, C.; Woolfson, J.P.; Perez, M.; Ricciuto, A.; Wales, P.W.; Kamath, B.M.; Chavhan, G.B.; et al. Paediatric reference values for total psoas muscle area. J. Cachexia Sarcopenia Muscle 2020, 11, 405–414. [Google Scholar] [CrossRef]
- Morrell, G.R.; Ikizler, T.A.; Chen, X.; Heilbrun, M.E.; Wei, G.; Boucher, R.; Beddhu, S. Psoas Muscle Cross-sectional Area as a Measure of Whole-body Lean Muscle Mass in Maintenance Hemodialysis Patients. J. Ren. Nutr. 2016, 26, 258–264. [Google Scholar] [CrossRef] [Green Version]
- Triarico, S.; Rinninella, E.; Mele, M.C.; Cintoni, M.; Attinà, G.; Ruggiero, A. Prognostic impact of sarcopenia in children with cancer: A focus on the psoas muscle area (PMA) imaging in the clinical practice. Eur. J. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Rommersbach, N.; Wirth, R.; Lueg, G.; Klimek, C.; Schnatmann, M.; Liermann, D.; Janssen, G.; Müller, M.J.; Pourhassan, M. The impact of disease-related immobilization on thigh muscle mass and strength in older hospitalized patients. BMC Geriatr. 2020, 20, 500. [Google Scholar] [CrossRef]
- Joseph, C.; Kenny, A.M.; Taxel, P.; Lorenzo, J.A.; Duque, G.; Kuchel, G.A. Role of endocrine-immune dysregulation in osteoporosis, sarcopenia, frailty and fracture risk. Mol. Aspects Med. 2005, 26, 181–201. [Google Scholar] [CrossRef]
- Di Giorgio, A.; Rotolo, S.; Cintoni, M.; Rinninella, E.; Pulcini, G.; Schena, C.A.; Ferracci, F.; Grassi, F.; Raoul, P.; Moroni, R.; et al. The prognostic value of skeletal muscle index on clinical and survival outcomes after cytoreduction and HIPEC for peritoneal metastases from colorectal cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2021, in press. [Google Scholar] [CrossRef]
- Goedhart, L.M.; Gerbers, J.G.; Ploegmakers, J.J.; Jutte, P.C. Delay in Diagnosis and Its Effect on Clinical Outcome in High-grade Sarcoma of Bone: A Referral Oncological Centre Study. Orthop. Surg. 2016, 8, 122–128. [Google Scholar] [CrossRef]
- Chindapasirt, J. Sarcopenia in Cancer Patients. Asian Pac. J. Cancer Prev. 2015, 16, 8075–8077. [Google Scholar] [CrossRef] [Green Version]
- Rayar, M.; Webber, C.E.; Nayiager, T.; Sala, A.; Barr, R.D. Sarcopenia in children with acute lymphoblastic leukemia. J. Pediatr. Hematol. Oncol. 2013, 35, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.J.; White, M.; Davies, P.S. Body composition of children with cancer. Am. J. Clin. Nutr. 2010, 92, 55–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Margioris, A.N. Sarcopenic obesity. Hormones 2018, 17, 321–331. [Google Scholar] [CrossRef]
- Baracos, V.E.; Arribas, L. Sarcopenic obesity: Hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann. Oncol. 2018, 29 (Suppl. S2), ii1–ii9. [Google Scholar] [CrossRef]
- Ritz, A.; Kolorz, J.; Hubertus, J.; Ley-Zaporozhan, J.; von Schweinitz, D.; Koletzko, S.; Häberle, B.; Schmid, I.; Kappler, R.; Berger, M.; et al. Sarcopenia is a prognostic outcome marker in children with high-risk hepatoblastoma. Pediatr. Blood Cancer 2021, 68, e28862. [Google Scholar] [CrossRef] [PubMed]
- Kawakubo, N.; Kinoshita, Y.; Souzaki, R.; Koga, Y.; Oba, U.; Ohga, S.; Taguchi, T. The Influence of Sarcopenia on High-Risk Neuroblastoma. J. Surg. Res. 2019, 236, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Masetti, R.; Muratore, E.; Leardini, D.; Zama, D.; Turroni, S.; Brigidi, P.; Esposito, S.; Pession, A. Gut microbiome in pediatric acute leukemia: From predisposition to cure. Blood Adv. 2021, 5, 4619–4629. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Patients (%) or Median IQR |
|---|---|
| Age (months) | 125.6 (78.7; 181.5) |
| Sex (male) | 11 (52.4) |
| Histology | |
| Ewing sarcoma | 14 (66.6) |
| Rhabdomyosarcoma | 6 (28.6) |
| Desmoplastic tumor | 1 (4.8) |
| Primary localization | |
| Bone | 13 (61.9) |
| Soft tissue | 8 (38.1) |
| Presence of metastases at diagnosis | 9 (42.9) |
| BMI (kg/m2) | 17.4 (15; 19.6) |
| BMI (percentile) | 41.7 (0.9–86.2) |
| BMI Z-Score | −0.23 (−0.89; 0.85) |
| PNI | 48.1 (45.2; 53.2) |
| tPMA L4–L5 (mm2) | 13.21 (8.79; 19.38) |
| tPMA L4–L5 Z-Score | −1.01 (−1.71; −0.35) |
| Nonsarcopenic patients | 9 (42.8) |
| Sarcopenic patients | 12 (57.1) |
| Mild | 8 (38.1) |
| Moderate | 4 (19.1) |
| Severe | 0 (0) |
| Progressive disease | 13 (61.9) |
| Deaths | 11 (51.4) |
| Variables | Diagnosis (Median (25°; 75°) or Number of Patients (%)) | 12 Months (Median (25°; 75°) or Number of Patients (%)) | p Value |
|---|---|---|---|
| BMI (kg/m2) | 17.4 (15; 19.6) | 17.0 (13.6; 19.2) | 0.25 |
| BMI (percentile) | 41.7 (0.9–86.2) | 12.2 (3.9–72.9) | 0.28 |
| BMI Z-score | −0.23 (−0.89; 0.85) | −1.17 (−2.11; 0.48) | 0.01 |
| PNI | 48.1 (45.2; 53.2) | 39.6 (35.7; 45.6) | 0.001 |
| tPMA L4–L5 (mm2) | 13.2 (8.8; 19.4) | 11.5 (9.95; 18.48) | 0.31 |
| tPMA L4–L5 Z-score | −1.01 (−1.71; −0.35) | −1.46 (−2.57; −1.11) | 0.005 |
| Nonsarcopenic patients | 9 (42.8) | 5 (23.8) | 0.32 |
| Sarcopenic patients | |||
| Mild | 8 (38.1) | 8 (38.1) | 0.999 |
| Moderate | 4 (19.1) | 8 (38.1) | 0.29 |
| Severe | 0 (0) | 0 (0) | - |
| HR (95%CI) | p Value | |
|---|---|---|
| Absence of sarcopenia at diagnosis | 0.63 (0.18–2.15) | 0.461 |
| Mild sarcopenia at diagnosis | 0.8 (0.24–2.75) | 0.726 |
| Moderate sarcopenia at diagnosis | 3.19 (0.82–12.36) | 0.09 |
| Ewing sarcoma | 0.35 (0.1–1.15) | 0.08 |
| Rhabdomyosarcoma | 2.86 (0.86–9.4) | 0.08 |
| Presence of metastases at diagnosis | 6.07 (1.59–23) | 0.008 |
| High-dose chemotherapy | 0.39 (0.05–3.13) | 0.38 |
| Radiotherapy | 0.49 (0.06–3.83) | 0.49 |
| Absence of surgery | 0.17 (0–0.6) | 0.005 |
| BMI at diagnosis | 1.02 (0.96–1.07) | 0.52 |
| PNI at diagnosis | 1 (0.95–1.07) | 0.76 |
| tPMA L4–L5 Z-score at diagnosis | 1 (0.52–2) | 0.95 |
| ΔBMI | 1.01 (0.97–1.01) | 0.59 |
| ΔPNI | 0.966 (0–0.99) | 0.027 |
| ΔtPMA L4–L5 | 0.97 (0.94–1) | 0.122 |
| ΔtPMA L4–L5 > −25% | 4.14 (1.05–16.3) | 0.042 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.; Triarico, S.; Rinninella, E.; Natale, L.; Brizi, M.G.; Cintoni, M.; Raoul, P.; Maurizi, P.; Attinà, G.; Mastrangelo, S.; et al. Clinical Impact of Nutritional Status and Sarcopenia in Pediatric Patients with Bone and Soft Tissue Sarcomas: A Pilot Retrospective Study (SarcoPed). Nutrients 2022, 14, 383. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020383
Romano A, Triarico S, Rinninella E, Natale L, Brizi MG, Cintoni M, Raoul P, Maurizi P, Attinà G, Mastrangelo S, et al. Clinical Impact of Nutritional Status and Sarcopenia in Pediatric Patients with Bone and Soft Tissue Sarcomas: A Pilot Retrospective Study (SarcoPed). Nutrients. 2022; 14(2):383. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020383
Chicago/Turabian StyleRomano, Alberto, Silvia Triarico, Emanuele Rinninella, Luigi Natale, Maria Gabriella Brizi, Marco Cintoni, Pauline Raoul, Palma Maurizi, Giorgio Attinà, Stefano Mastrangelo, and et al. 2022. "Clinical Impact of Nutritional Status and Sarcopenia in Pediatric Patients with Bone and Soft Tissue Sarcomas: A Pilot Retrospective Study (SarcoPed)" Nutrients 14, no. 2: 383. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020383