Vitamin B12 Deficiency in Relation to Functional Disabilities

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Biochemical Measurements
2.3. Functional Measures
2.3.1. Peripheral Neuropathy Assessment
2.3.2. Balance
2.3.3. Cognitive Functioning
2.3.4. Gait Speed
2.3.5. Disability Domains
2.3.6. Medical Conditions
2.3.7. Anthropometrics, Smoking, Alcohol, and Supplement Use
2.3.8. Statistics
3. Results
3.1. Demographic Characteristics of Study Population

{kind=link}
| Characteristics | Total Sample (n = 3105) | >Deficiency Definitions 1 | ||
|---|---|---|---|---|
| B12 Alone (<148 pmol/L) (n = 95) | B12 (<200 pmol/L) and Homocysteine (>20 μmol/L) (n = 40) | B12 (<258 pmol/L) or MMA (>0.21 μmol/L) (n = 1160) | ||
| Age (y) | 68.9 (0.4) 2 | 70.9 (1.1) | 76.6 (1.6) | 69.9 (0.5) |
| Female (%) | 56.7 (0.7) 3 | 58.1 (5.3) | 78.3 (8.0) | 54.7 (1.3) |
| NonHispanic White (%) | 81.5 (2.1) | 81.7 (6.2) | 87.1 (4.9) | 82.8 (2.1) |
| Smokers 4 (%) | 23.3 (1.3) | 31.4 (8.9) | NR | 26.2 (2.1) |
| Body Mass Index, BMI (kg/m2) | 27.1 (0.4) | 28.9 (1.0) | 28.9 (1.3) | 27.6 (0.5) |
| Peripheral artery disease 5 (%) | 6.2 (0.7) | 5.5 (3.0) | 24.7 (17.0) | 8.9 (1.5) |
| Coronary heart disease 6 (%) | 10.3 (0.8) | 11.1 (3.9) | 30.4 (7.5) | 10.3 (0.9) |
| Diabetes 7 (%) | 14.0 (1.4) | 6.7 (3.8) | 19.6 (8.5) | 16.7 (1.2) |
| B12 supplement use 8 (%) | 41.2 (1.7) | 24.9 (7.2) | 40.3 (8.1) | 29.6 (1.8) |
| Gait Time 9 (in seconds) | 7.7 (0.2) | 7.2 (0.4) | 8.6 (1.0) | 7.9 (0.2) |
| Hematocrit | 42.4 (0.2) | 42.6 (0.4) | 39.6 (0.9) | 42.1 (0.2) |
| Macrocytosis 10 (%) | 4.7 (0.5) | 5.5 (2.1) | 7.0 (4.1) | 5.6 (0.7) |
| Creatinine (μmol/L) | 81.1 (1.9) | 85.8 (4.6) | 118.4 (11.4) | 94.2 (3.1) |
| Ferritin (μg/L) | 111.0 (10.0) | 116.0 (17.3) | 95.1 (24.1) | 146.9 (7.8) |
| Folate (nmol/L) | 42.9 (1.9) | 35.5 (3.0) | 40.0 (8.4) | 39.8 (1.3) |
| B12 (pmol/L) | 276.6 (12.0) | 149.9 (20.7) | 179.7 (61.9) | 260.5 (8.5) |
| Homocysteine (μmol/L) | 15.1 (2.4) | 19.9 (4.8) | 37.6 (6.6) | 12.4 (0.5) |
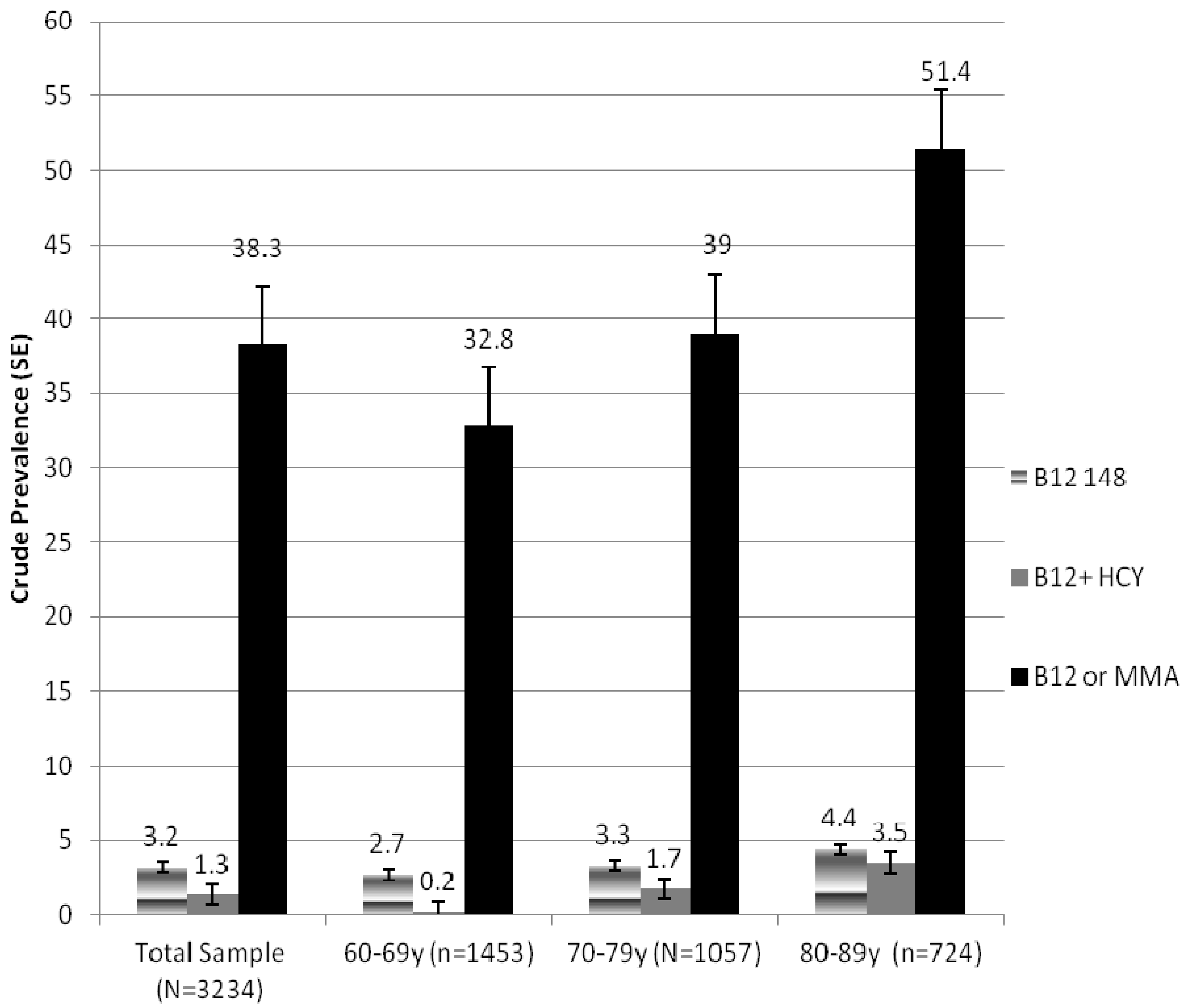
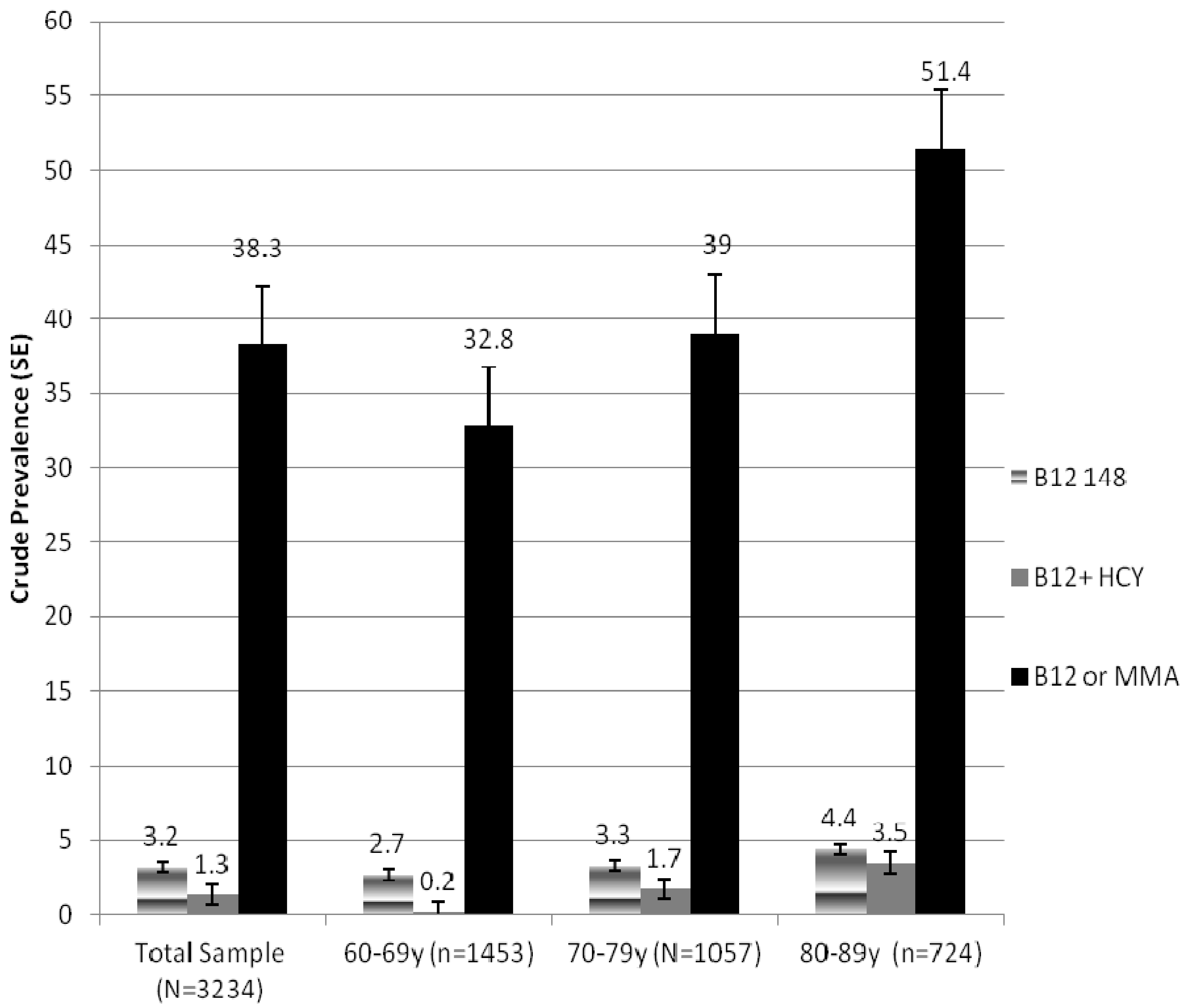
3.2. Prevalence of B12 Deficiency
3.3. Functional Measures and Reported Disabilities Associated with B12 Deficiency
| Characteristic | B12 Alone (<148 pmol/L) | B12 (<200 pmol/L) and Homocysteine (>20 μmol/L) | B12 (<258 pmol/L) or MMA (>0.21 μmol/L) |
|---|---|---|---|
| Odds Ratio; (95% Confidence Intervals); p Value | |||
| Peripheral Neuropathy1 | |||
| Exam % insensate | 0.67; (0.25, 1.78); 0.36 2 | 9.70; (2.24,42.07); 0.004 | 1.44; (1.03, 2.02); 0.03 |
| Balance3 | |||
| % fail | 2.08; (0.58, 7.44); 0.25 | 1.82; (0.20, 16.39); 0.58 | 0.97; (0.57, 1.64); 0.90 |
| Disability4 | |||
| Total | 1.80; (1.03, 3.14); 0.04 | 19.61; (6.22, 61.86); 0.0001 | 1.60; (1.09, 2.34); 0.02 |
| Activities of Daily Living (ADL) | 0.83; (0.12, 5.77); 0.84 | 2.20; (0.30, 15.88); 0.42 | 1.57; (0.78, 3.19); 0.98 |
| Instrumental Activities of Daily Living (IADL) | 1.52; (0.46, 5.02); 0.48 | 2.05; (0.28, 15.20); 0.47 | 1.36; (0.89, 2.08); 0.15 |
| Lower extremity mobility (LEM) | 1.53; (0.65, 3.57); 0.32 | 7.58; (1.22, 50.30); 0.03 | 1.44; (0.99, 2.20); 0.06 |
| Leisure and social activities (LSA) | 1.35; (0.04, 4.06); 0.58 | 4.04; (0.38, 42.61); 0.24 | 1.63; (1.06, 2.51); 0.03 |
| Cognitive Impairment5 | |||
| Digit Symbol Substitution Test (DSST) | 3.62; (1.45, 9.04); 0.01 | 0.84; (0.03,23.38); 0.91 | 1.58; (1.01, 2.47); 0.04 |
4. Discussion
Strength and Limitations
5. Conclusions and Implications
Conflicts of Interest
References
- Institute of Medicine. Vitamin B12. In Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academy Press: Washington, DC, USA, 1998; pp. 306–356. [Google Scholar]
- Clarke, R.; Evans, J.G.; Schneede, J.; Nexo, E.; Bates, C.; Fletcher, A.; Prentice, A.; Johnston, C.; Ueland, P.M.; Refsum, H.; et al. Vitamin B12 and folate deficiency in later life. Age Ageing 2004, 33, 34–41. [Google Scholar] [CrossRef]
- Herbert, V. The 1986 Herman Award Lecture. Nutrition science as a continually unfolding story, the folate and vitamin B12 paradigm. Am. J. Clin. Nutr. 1987, 46, 387–402. [Google Scholar]
- Bjorkegren, K.; Svardsudd, K. A population-based intervention study on elevated serum levels of methylmalonic acid and total homocysteine in elderly people, results after 36 months of follow-up. J. Intern. Med. 2004, 256, 446–452. [Google Scholar] [CrossRef]
- Lesihear, K.; Ferucci, L.; Lauretani, F.; Boudreau, R.M.; Studenski, S.A.; Rosano, C.; Abbate, R.; Gori, A.M.; Corsi, A.M.; DiIorio, A.; et al. Vitamin B12 and homocysteine levels and 6-year change in peripheral nerve function and neurological signs. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 537–543. [Google Scholar]
- Lewerin, C.; Matousek, M.; Steen, G.; Johansson, B.; Steen, B; Nilsson-Ehle, H. Significant correlations of plasma homocysteine and serum methylmalonic acid with movement and cognitive performance in elderly subjects but no improvement from short-term vitamin therapy, a placebo-controlled randomized study. Am. J. Clin. Nutr. 2005, 81, 1155–1162. [Google Scholar]
- Evatt, M.L.; Terry, P.D.; Ziegler, T.R.; Oakley, G.P. Association between vitamin B12-containing supplement consumption and prevalence of biochemically defined B12 deficiency in adults in NHANES III (Third National Health and Nutrition Examination Survey). Public Health Nutr. 2009, 13, 25–31. [Google Scholar]
- Morris, M.S.; Jacques, P.F.; Rosenberg, I.H.; Selhub, J. Folate and vitamin B-12 status in relation to anemia, macrocytosis and cognitive impairment in older Americans in the age of folic acid fortification. Am. J. Clin. Nutr. 2007, 85, 193–200. [Google Scholar]
- Johnson, M.A.; Hausman, D.B.; Davey, A.; Poon, L.W.; Allen, R.H.; Stabler, S.P. Vitamin B12 deficiency in African Americans and white octogenarians and centenarians in Georgia. J. Nutr. Health Aging 2010, 14, 339–345. [Google Scholar] [CrossRef]
- Pennypacker, L.C.; Allen, R.H.; Kelly, J.P.; Matthews, L.M.; Grigsby, J.; Kaye, K.; Lindenbaum, J.; Stabler, S.P. High prevalence of cobalamin deficiency in elderly outpatients. J. Am. Geriatr. Soc. 1992, 40, 1197–1204. [Google Scholar]
- Stabler, S.P.; Allen, R.H.; Savage, D.G.; Lindenbaum, J. Clinical spectrum and diagnosis of cobalamin deficiency. Blood 1990, 76, 871–881. [Google Scholar]
- Hin, H.; Clarke, R.; Sherliker, P.; Atoyebi, W.; Emmens, K.; Birks, J.; Schneede, J.; Ueland, P.M.; Nexo, E.; Scott, J.; et al. Clinical relevance of low serum vitamin B12 concentrations in older people, the Banbury B12 study. Age Ageing 2006, 36, 416–422. [Google Scholar]
- NHANES. Centers for Disease Control and Prevention, National Health and Nutrition Examination Survey 2001–2002. Available online: http://wwwn.cdc.gov/nchs/nhanes/search/datapage.aspx?Component=Examination&CycleBeginYear=2001 (accessed on 18 March 2010).
- Gregg, E.W.; Sorlie, P.; Paulose-Ram, R.; Gu, Q.; Eberhardt, M.S.; Wolz, M.; Burt, V.; Curtin, L.; Engelau, M.; Geiss, L. Prevalence of lower-extremity disease in the US adult population ≥ 40 years of age with and without diabetes, 1999–2000 National Health and Nutrition Examination survey. Diabetes Care 2004, 27, 1591–1597. [Google Scholar] [CrossRef]
- Wechler, D. Administration and Scoring Guide. In WAIS-III, Wechsler Adult Intelligence Scale, 3rd ed.; The Psychological, Corporation, Ed.; Harcourt Brace and Company: San Antonio, TX, USA, 1997. [Google Scholar]
- Kuo, H.K.; Leveille, S.G.; Yu, Y.-H.; Milberg, W.P. Cognitive function, habitual gait speed, and late-life disability in the National Health and Nutrition Examination Survey (NHANES) 1999–2002. Gerontology 2007, 53, 102–110. [Google Scholar] [CrossRef]
- Ostchega, Y.; Dillon, C.F.; Lindle, R.; Carroll, M.; Hurley, B.F. Isokinetic leg muscle strength in older Americans and its relationship to a standardized walk test. Data from the National Health and Nutrition Examination Survey 1999–2000. J. Am. Geriatr. Soc. 2004, 52, 977–982. [Google Scholar]
- Shinkai, S.; Watanabe, S.; Kumagai, S.; Fujiwara, Y.; Amano, H.; Yoshida, H.; Ishizaki, T.; Yukama, H.; Suzuki, T.; Shibata, H. Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing 2002, 29, 441–446. [Google Scholar]
- Nagi, S.Z. An epidemiology of disability among adults in the United States. Milbank Mem. Fund Q. Health Soc. 1976, 54, 439–467. [Google Scholar] [CrossRef]
- Healton, H.B.; Savage, D.G.; Brust, J.C.M.; Garrett, T.J.; Lindenbaum, J. Neurologic aspects of cobalamin deficiency. Medicine 1991, 70, 229–245. [Google Scholar]
- Martin, D.C.; Francis, J.; Protetch, J.; Huff, F.J. Time dependency of cognitive recovery with cobalamin replacement, report of a pilot study. J. Am. Geriatr. Soc. 1992, 40, 168–172. [Google Scholar]
- Lindenbaum, J.; Rosenberg, I.H.; Wilson, P.W.F.; Stabler, S.P.; Allen, R.H. Prevalence of cobalamin deficiency in the Framingham elderly population. Am. J. Clin. Nutr. 1994, 60, 2–11. [Google Scholar]
- Fabrigoule, C.; Letenneur, L.; Dartigues, J.F.; Zarrouk, M.; Commenges, D.; Barberger-Gateau, P. Social and leisure activities and risk of dementia, a prospective longitudinal study. J. Am. Geriatr. Soc. 1995, 43, 485–490. [Google Scholar]
- Matteini, A.M.; Walston, J.D.; Fallin, M.D.; Bandeed-Roche, K.; Kao, W.H.L.; Semba, R.D.; Allen, R.H.; Guralnik, J.; Fried, L.P.; Stabler, S.P. Markers of B-vitamin deficiency and frailty in older women. J. Nutr. Health Aging 2008, 12, 303–308. [Google Scholar] [CrossRef]
- Scarmeas, N.; Levy, G.; Tang, M.X.; Manly, J.; Stern, Y. Influence of leisure activity on the incidence of Alzheimer’s disease. Neurology 2001, 57, 2236–2242. [Google Scholar] [CrossRef]
- Tangney, C.C.; Tang, Y.; Evans, D.A.; Morris, M.C. Biochemical indicators of vitamin B12 and folate insufficiency and cognitive decline. Neurology 2009, 72, 361–367. [Google Scholar] [CrossRef]
- Sun, Y.; Lai, M.S.; Lu, C.J. Effectiveness of vitamin B12 on diabetic neuropathy, Systematic review of clinical controlled trials. Acta Neurol. Taiwan 2008, 14, 48–54. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Oberlin, B.S.; Tangney, C.C.; Gustashaw, K.A.R.; Rasmussen, H.E. Vitamin B12 Deficiency in Relation to Functional Disabilities. Nutrients 2013, 5, 4462-4475. https://0-doi-org.brum.beds.ac.uk/10.3390/nu5114462
Oberlin BS, Tangney CC, Gustashaw KAR, Rasmussen HE. Vitamin B12 Deficiency in Relation to Functional Disabilities. Nutrients. 2013; 5(11):4462-4475. https://0-doi-org.brum.beds.ac.uk/10.3390/nu5114462
Chicago/Turabian StyleOberlin, Breanna S., Christy C. Tangney, Kristin A. R. Gustashaw, and Heather E. Rasmussen. 2013. "Vitamin B12 Deficiency in Relation to Functional Disabilities" Nutrients 5, no. 11: 4462-4475. https://0-doi-org.brum.beds.ac.uk/10.3390/nu5114462