Identification, Prevention and Treatment of Iron Deficiency during the First 1000 Days

Abstract
:1. Introduction
2. Iron Metabolism and Requirements
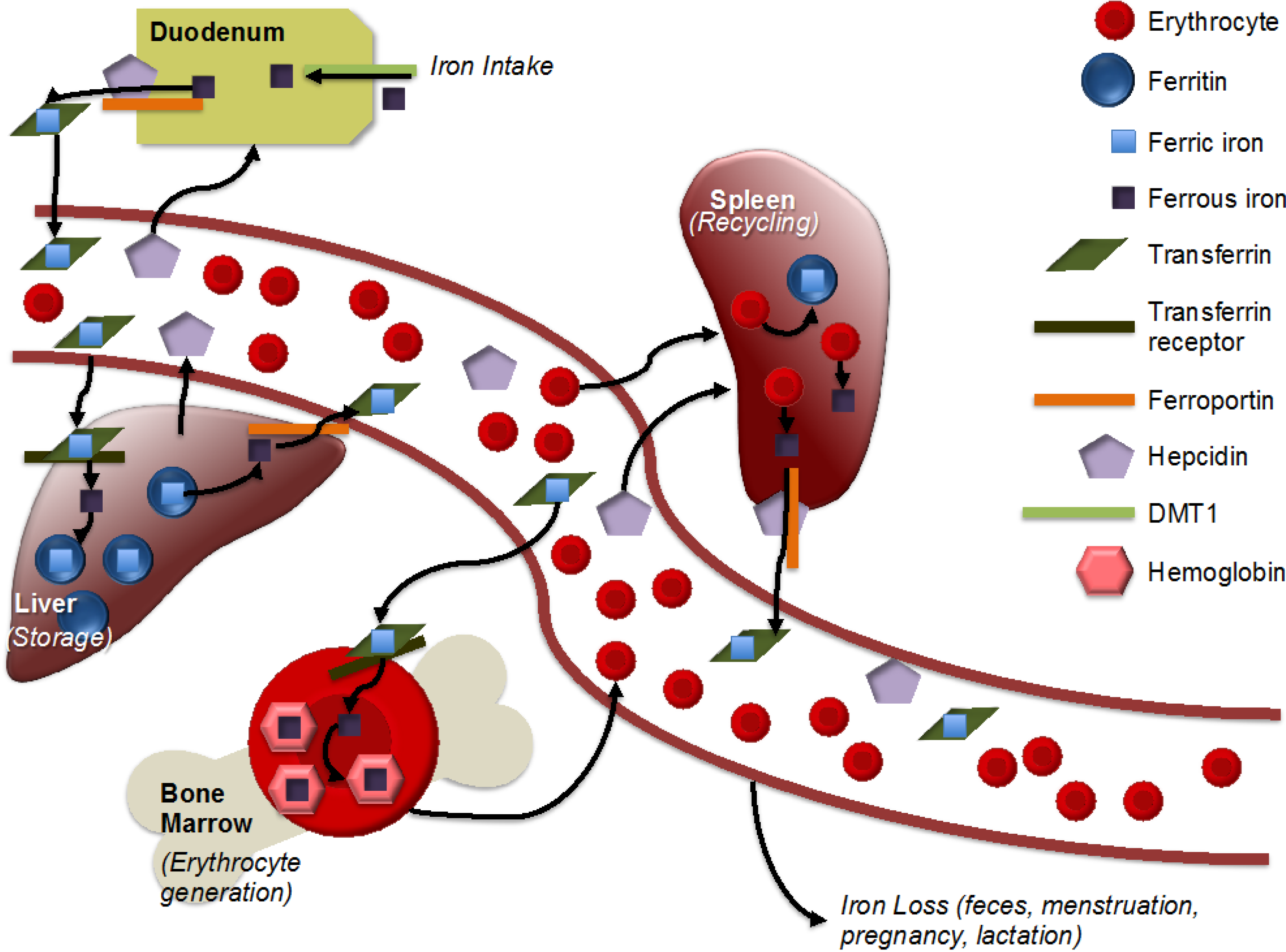
2.1. Iron Metabolism

2.2. Requirements in Pregnant and Lactating Women
2.3. Requirements in Infants of Zero to 24 Months of Age
3. Epidemiology of Iron Deficiency
3.1. Pregnant and Lactating Women
3.2. Infants of Zero to 24 Months of Age
4. Risk Factors for Iron Deficiency
4.1. Pregnant and Lactating Women
4.2. Infants of Zero to 24 Months of Age
4.2.1. Pre- and Peri-Natal Risk Factors
4.2.2. Postnatal Risk Factors
5. Consequences of Iron Deficiency
5.1. Pregnant and Lactating Women
5.2. Infants Zero to 24 Months
6. Screening and Measurement of Iron Deficiency
6.1. Commonly Used Indicators

{kind=link}
| Biomarker | Advantages | Limitations | Normal Range/Cut-offs |
|---|---|---|---|
| Hemoglobin (Hb) |
|
|
|
| Hematocrit (Hct) |
|
|
|
| Red blood cell indices (mean cell volume (MCV), red cell distribution width (RDW)) |
|
|
|
| Serum or plasma iron |
|
|
|
| Serum ferritin (SF) |
|
|
|
| Transferrin saturation (Tfs) |
|
|
|
| Transferrin receptor (TfR) |
|
|
|
| TfR:SF ratio |
|
|
|
| Total iron binding capacity (TIBC) |
|
|
|
| Zinc protoporphyrin (ZPP) |
|
|
|
| Hepcidin (Hep) |
|
|
|
| Reticulocyte hemoglobin (CHr) |
|
|
|
| Stainable bone marrow |
|
|
|
6.2. Impact of Inflammation on Indicators of Iron Status
7. Interventions
7.1. Pregnant and Lactating Women
7.2. Infants Zero–24 Months of Age
8. Research Needs
9. Conclusions and Recommendations
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Victora, C.G.; de Onis, M.; Hallal, P.C.; Blossner, M.; Shrimpton, R. Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics 2010, 125, e473–e480. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [PubMed]
- Berglund, S.; Domellof, M. Meeting iron needs for infants and children. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; O’Brien, K.O. Pregnancy and iron homeostasis: An update. Nutr. Rev. 2013, 71, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Martorell, R.; Zongrone, A. Intergenerational influences on child growth and under nutrition. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 302–314. [Google Scholar]
- Radlowski, E.C.; Johnson, R.W. Perinatal iron deficiency and neurocognitive development. Front. Human Neurosci. 2013, 7, 585. [Google Scholar] [CrossRef]
- Miller, J.L. Iron deficiency anemia: A common and curable disease. Cold Spring Harbor Perspect. Med. 2013, 3, a011866. [Google Scholar] [CrossRef]
- Andrews, N.C. Forging a field: The golden age of iron biology. Blood 2008, 112, 219–230. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, E.L.; Iwasaki, K.; Tsuji, Y. Intracellular iron transport and storage: From molecular mechanisms to health implications. Antioxid. Redox Signal. 2008, 10, 997–1030. [Google Scholar] [CrossRef] [PubMed]
- WHO. Assessing the iron status of populations: Including literature reviews. In Report of a Joint World Health Organization/Centers for Disease Control and Prevention Technical Consultation on the Assessment of Iron Status at the Population Level; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Escobar-Morreale, H.F. Iron metabolism and the polycystic ovary syndrome. Trends Endocrinol. Metab. 2012, 23, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Picciano, M.F. Pregnancy and lactation: Physiological adjustments, nutritional requirements and the role of dietary supplements. J. Nutr. 2003, 133, 1997S–2002S. [Google Scholar] [PubMed]
- Gambling, L.; Lang, C.; McArdle, H.J. Fetal regulation of iron transport during pregnancy. Am. J. Clin. Nutr. 2011, 94, 1903S–1907S. [Google Scholar] [CrossRef] [PubMed]
- Bothwell, T.H. Iron requirements in pregnancy and strategies to meet them. Am. J. Clin. Nutr. 2000, 72, 257S–264S. [Google Scholar] [PubMed]
- Beaton, G.H. Iron needs during pregnancy: Do we need to rethink our targets? Am. J. Clin. Nutr. 2000, 72, 265S–271S. [Google Scholar]
- Bender, D.A. Do we really know vitamin and mineral requirements for infants and children? J. R. Soc. Promot. Health 2003, 123, 154–158. [Google Scholar] [CrossRef]
- Siddappa, A.M.; Rao, R.; Long, J.D.; Widness, J.A.; Georgieff, M.K. The assessment of newborn iron stores at birth: A review of the literature and standards for ferritin concentrations. Neonatology 2007, 92, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Marin, G.H.; Mestorino, N.; Errecalde, J.; Huber, B.; Uriarte, A.; Orchuela, J. Personalised iron supply for prophylaxis and treatment of pregnant women as a way to ensure normal iron levels in their breast milk. J. Med. Life 2012, 5, 29–32. [Google Scholar] [PubMed]
- Nikniaz, L.; Mahdavi, R.; Gargari, B.P.; Gayem Magami, S.J.; Nikniaz, Z. Maternal body mass index, dietary intake and socioeconomic status: Differential effects on breast milk zinc, copper and iron content. Health Promot. Perspect. 2011, 1, 140–146. [Google Scholar] [PubMed]
- Silvestre, D.; Martinez-Costa, C.; Lagarda, M.J.; Brines, J.; Farre, R.; Clemente, G. Copper, iron, and zinc contents in human milk during the first three months of lactation: A longitudinal study. Biol. Trace Elem. Res. 2001, 80, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yamawaki, N.; Yamada, M.; Kan-no, T.; Kojima, T.; Kaneko, T.; Yonekubo, A. Macronutrient, mineral and trace element composition of breast milk from Japanese women. J. Trace Elem. Med. Biol. 2005, 19, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.D.; Greer, F.R. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age). Pediatrics 2010, 126, 1040–1050. [Google Scholar] [CrossRef] [PubMed]
- Saarinen, U.M.; Siimes, M.A.; Dallman, P.R. Iron absorption in infants: High bioavailability of breast milk iron as indicated by the extrinsic tag method of iron absorption and by the concentration of serum ferritin. J. Pediatr. 1977, 91, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.L.; O’Brien, K.O.; Abrams, S.A.; Zavaleta, N. Infant iron status affects iron absorption in Peruvian breastfed infants at 2 and 5 months of age. Am. J. Clin. Nutr. 2013, 98, 1475–1484. [Google Scholar] [PubMed]
- Lonnerdal, B.; Kelleher, S.L. Iron metabolism in infants and children. Food Nutr. Bull. 2007, 28, S491–S499. [Google Scholar] [PubMed]
- Zimmermann, M.B. Methods to assess iron and iodine status. Br. J. Nutr. 2008, 99 (Suppl. 3), S2–S9. [Google Scholar] [CrossRef]
- Cameron, B.M.; Neufeld, L.M. Estimating the prevalence of iron deficiency in the first two years of life: Technical and measurement issues. Nutr. Rev. 2011, 69 (Suppl. 1), S49–S56. [Google Scholar] [CrossRef]
- WHO. Iron deficiency anaemia: Assessment, prevention, and control. In A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; de Benoist, B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef] [PubMed]
- WHO. Worldwide Prevalence of Anaemia 1993–2005. WHO Global Database on Anaemia; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Qureshi, I.A.; Arlappa, N.; Qureshi, M.A. Prevalence of malaria and anemia among pregnant women residing in malaria-endemic forest villages in India. Int. J. Gynaecol. Obstetr. 2014, 127, 93. [Google Scholar] [CrossRef]
- Menon, K.C.; Ferguson, E.L.; Thomson, C.D.; Gray, A.R.; Zodpey, S.; Saraf, A.; Das, P.K.; Pandav, C.S.; Skeaff, S.A. Iron status of pregnant Indian women from an area of active iron supplementation. Nutrition 2014, 30, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Milman, N. Postpartum anemia I: Definition, prevalence, causes, and consequences. Ann. Hematol. 2011, 90, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.E.; Nelson, S.E.; Jeter, J.M. Iron supplementation of breastfed infants. Nutr. Rev. 2011, 69 (Suppl. 1), S71–S77. [Google Scholar]
- Thorisdottir, A.V.; Ramel, A.; Palsson, G.I.; Tomassson, H.; Thorsdottir, I. Iron status of one-year-olds and association with breast milk, cow’s milk or formula in late infancy. Eur. J. Nutr. 2013, 52, 1661–1668. [Google Scholar] [CrossRef] [PubMed]
- Dube, K.; Schwartz, J.; Mueller, M.J.; Kalhoff, H.; Kersting, M. Iron intake and iron status in breastfed infants during the first year of life. Clin. Nutr. 2010, 29, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Morales-Ruan Mdel, C.; Villalpando, S.; Garcia-Guerra, A.; Shamah-Levy, T.; Robledo-Perez, R.; Avila-Arcos, M.A.; Rivera, J.A. Iron, zinc, copper and magnesium nutritional status in Mexican children aged 1 to 11 years. Salud Publica de Mexico 2012, 54, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Sandjaja, S.; Budiman, B.; Harahap, H.; Ernawati, F.; Soekatri, M.; Widodo, Y.; Sumedi, E.; Rustan, E.; Sofia, G.; Syarief, S.N.; et al. Food consumption and nutritional and biochemical status of 0.5–12-year-old Indonesian children: The SEANUTS study. Br. J. Nutr. 2013, 110 (Suppl. 3), S11–S20. [Google Scholar]
- Sachdev, H.P.; Gera, T. Preventing childhood anemia in India: Iron supplementation and beyond. Eur. J. Clin. Nutr. 2013, 67, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Statcompiler: Building Tables with DHS Data. Available online: http://www.statcompiler.com/ (accessed on 24 September 2014).
- Milman, N. Iron in pregnancy: How do we secure an appropriate iron status in the mother and child? Ann. Nutr. Metab. 2011, 59, 50–54. [Google Scholar] [CrossRef]
- Collings, R.; Harvey, L.J.; Hooper, L.; Hurst, R.; Brown, T.J.; Ansett, J.; King, M.; Fairweather-Tait, S.J. The absorption of iron from whole diets: A systematic review. Am. J. Clin. Nutr. 2013, 98, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.D.; Biggs, B.A.; Tran, T.; Casey, G.J.; Hanieh, S.; Simpson, J.A.; Dwyer, T.; Fisher, J. Psychological and social factors associated with late pregnancy iron deficiency anaemia in rural Viet Nam: A population-based prospective study. PLoS One 2013, 8, e78162. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Drakesmith, H.; Black, J.; Hipgrave, D.; Biggs, B.A. Control of iron deficiency anemia in low- and middle-income countries. Blood 2013, 121, 2607–2617. [Google Scholar] [CrossRef] [PubMed]
- Nikonorov, A.A.; Skalnaya, M.G.; Tinkov, A.A.; Skalny, A.V. Mutual interaction between iron homeostasis and obesity pathogenesis. J. Trace Elem. Med. Biol. 2014. [Google Scholar] [CrossRef]
- Hicks, P.D.; Zavaleta, N.; Chen, Z.; Abrams, S.A.; Lonnerdal, B. Iron deficiency, but not anemia, upregulates iron absorption in breast-fed Peruvian infants. J. Nutr. 2006, 136, 2435–2438. [Google Scholar] [PubMed]
- Ziegler, E.E.; Nelson, S.E.; Jeter, J.M. Iron stores of breastfed infants during the first year of life. Nutrients 2014, 6, 2023–2034. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O. Maternal iron status: Relation to fetal growth, length of gestation, and iron endowment of the neonate. Nutr. Rev. 2011, 69 (Suppl. 1), S23–S29. [Google Scholar] [CrossRef]
- Shao, J.; Lou, J.; Rao, R.; Georgieff, M.K.; Kaciroti, N.; Felt, B.T.; Zhao, Z.Y.; Lozoff, B. Maternal serum ferritin concentration is positively associated with newborn iron stores in women with low ferritin status in late pregnancy. J. Nutr. 2012, 142, 2004–2009. [Google Scholar] [CrossRef] [PubMed]
- Lanzkowsky, P. The influence of maternal iron-deficiency anaemia on the haemoglobin of the infant. Arch. Dis. Child. 1961, 36, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, H.; Akman, I.; Demirel, U.; Coskun, S.; Bilgen, H.; Ozek, E. Iron deficiency anemia in late-preterm infants. Turk. J. Pediatr. 2013, 55, 500–505. [Google Scholar] [PubMed]
- Hay, G.; Refsum, H.; Whitelaw, A.; Melbye, E.L.; Haug, E.; Borch-Iohnsen, B. Predictors of serum ferritin and serum soluble transferrin receptor in newborns and their associations with iron status during the first 2 years of life. Am. J. Clin. Nutr. 2007, 86, 64–73. [Google Scholar] [PubMed]
- Berglund, S.; Westrup, B.; Domellof, M. Iron supplements reduce the risk of iron deficiency anemia in marginally low birth weight infants. Pediatrics 2010, 126, e874–e883. [Google Scholar] [CrossRef] [PubMed]
- Haga, P. Plasma ferritin concentrations in preterm infants in cord blood and during the early anaemia of prematurity. Acta Paediatr. Scand. 1980, 69, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Lonnerdal, B.; Adu-Afarwuah, S.; Brown, K.H.; Chaparro, C.M.; Cohen, R.J.; Domellof, M.; Hernell, O.; Lartey, A.; Dewey, K.G. Prevalence and predictors of iron deficiency in fully breastfed infants at 6 mo of age: Comparison of data from 6 studies. Am. J. Clin. Nutr. 2009, 89, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Mamiro, P.S.; Kolsteren, P.; Roberfroid, D.; Tatala, S.; Opsomer, A.S.; Van Camp, J.H. Feeding practices and factors contributing to wasting, stunting, and iron-deficiency anaemia among 3–23-month old children in Kilosa district, rural Tanzania. J. Health Popul. Nutr. 2005, 23, 222–230. [Google Scholar]
- Monterrosa, E.C.; Frongillo, E.A.; Vasquez-Garibay, E.M.; Romero-Velarde, E.; Casey, L.M.; Willows, N.D. Predominant breast-feeding from birth to six months is associated with fewer gastrointestinal infections and increased risk for iron deficiency among infants. J. Nutr. 2008, 138, 1499–1504. [Google Scholar] [PubMed]
- Powers, H.J. Vitamin requirements for term infants: Considerations for infant formulae. Nutr. Res. Rev. 1997, 10, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Baykan, A.; Yalcin, S.S.; Yurdakok, K. Does maternal iron supplementation during the lactation period affect iron status of exclusively breast-fed infants? Turk. J. Pediatr. 2006, 48, 301–307. [Google Scholar]
- Domellof, M.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Iron requirements of infants and toddlers. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Van de Lagemaat, M.; Amesz, E.M.; Schaafsma, A.; Lafeber, H.N. Iron deficiency and anemia in iron-fortified formula and human milk-fed preterm infants until 6 months post-term. Eur. J. Nutr. 2013, 53, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Maguire, J.L.; Salehi, L.; Birken, C.S.; Carsley, S.; Mamdani, M.; Thorpe, K.E.; Lebovic, G.; Khovratovich, M.; Parkin, P.C. Association between total duration of breastfeeding and iron deficiency. Pediatrics 2013, 131, e1530–e1537. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, D.H.; Lee, J.E.; Kwon, Y.S.; Jun, Y.H.; Hong, Y.J.; Kim, S.K. Is it possible to predict the iron status from an infant's diet history? Pediatr. Gastroenterol. Hepatol. Nutr. 2013, 16, 95–103. [Google Scholar] [CrossRef]
- Iwai, Y.; Takanashi, T.; Nakao, Y.; Mikawa, H. Iron status in low birth weight infants on breast and formula feeding. Eur. J. Pediatr. 1986, 145, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Kazal, L.A., Jr. Prevention of iron deficiency in infants and toddlers. Am. Family Phys. 2002, 66, 1217–1224. [Google Scholar]
- Dewey, K.G.; Mayers, D.R. Early child growth: How do nutrition and infection interact? Matern. Child Nutr. 2011, 7 (Suppl. 3), 129–142. [Google Scholar]
- Pita, G.M.; Jimenez, S.; Basabe, B.; Garcia, R.G.; Macias, C.; Selva, L.; Hernandez, C.; Cruz, M.; Herrera, R.; O’Farrill, R.; et al. Anemia in children under five years old in eastern Cuba, 2005–2011. MEDICC Rev. 2014, 16, 16–23. [Google Scholar] [PubMed]
- Schmeer, K.K. Family structure and child anemia in Mexico. Soc. Sci. Med. 2013, 95, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Zeng, L.; Brouwer, I.D.; Kok, F.J.; Yan, H. Effect of iron deficiency anemia in pregnancy on child mental development in rural China. Pediatrics 2013, 131, e755–e763. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.D.; Biggs, B.A.; Tran, T.; Simpson, J.A.; Hanieh, S.; Dwyer, T.; Fisher, J. Impact on infants’ cognitive development of antenatal exposure to iron deficiency disorder and common mental disorders. PLoS One 2013, 8, e74876. [Google Scholar] [CrossRef] [PubMed]
- Kordas, K. Iron, lead, and children’s behavior and cognition. Ann. Rev. Nutr. 2010, 30, 123–148. [Google Scholar] [CrossRef]
- Iron-Status Indicators. Available online: http://www.cdc.gov/nutritionreport/99-02/pdf/nr_ch3.pdf (accessed on 24 May 2014).
- Raiten, D.J.; Namaste, S.; Brabin, B.; Combs, G., Jr.; L’Abbe, M.R.; Wasantwisut, E.; Darnton-Hill, I. Executive summary—Biomarkers of nutrition for development: Building a consensus. Am. J. Clin. Nutr. 2011, 94, 633S–650S. [Google Scholar] [CrossRef] [PubMed]
- Thurnham, D.; McCabe, G. Influence of Infection and Inflammation on Biomarkers of Nutritional Status with an Emphasis on Vitamin A and Iron; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Aguilar, R.; Moraleda, C.; Quinto, L.; Renom, M.; Mussacate, L.; Macete, E.; Aguilar, J.L.; Alonso, P.L.; Menendez, C. Challenges in the diagnosis of iron deficiency in children exposed to high prevalence of infections. PLoS One 2012, 7, e50584. [Google Scholar] [CrossRef] [PubMed]
- Brugnara, C.; Schiller, B.; Moran, J. Reticulocyte hemoglobin equivalent (ret he) and assessment of iron-deficient states. Clin. Lab. Haematol. 2006, 28, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Looker, A.C.; Dallman, P.R.; Carroll, M.D.; Gunter, E.W.; Johnson, C.L. Prevalence of iron deficiency in the United States. J. Am. Med. Assoc. 1997, 277, 973–976. [Google Scholar] [CrossRef]
- Galesloot, T.E.; Vermeulen, S.H.; Geurts-Moespot, A.J.; Klaver, S.M.; Kroot, J.J.; van Tienoven, D.; Wetzels, J.F.; Kiemeney, L.A.; Sweep, F.C.; den Heijer, M.; et al. Serum hepcidin: Reference ranges and biochemical correlates in the general population. Blood 2011, 117, e218–e225. [Google Scholar] [CrossRef] [PubMed]
- Gyarmati, B.; Szabo, E.; Szalay, B.; Czuczy, N.; Toldi, G.; Cseh, A.; Vasarhelyi, B.; Takats, Z. Serum maternal hepcidin levels 3 days after delivery are higher compared to those measured at parturition. J. Obstetr. Gynaecol. Res. 2011, 37, 1620–1624. [Google Scholar] [CrossRef]
- Muller, K.F.; Lorenz, L.; Poets, C.F.; Westerman, M.; Franz, A.R. Hepcidin concentrations in serum and urine correlate with iron homeostasis in preterm infants. J. Pediatr. 2012, 160, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Rehu, M.; Punnonen, K.; Ostland, V.; Heinonen, S.; Westerman, M.; Pulkki, K.; Sankilampi, U. Maternal serum hepcidin is low at term and independent of cord blood iron status. Eur. J. Haematol. 2010, 85, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Schulze, K.J.; Christian, P.; Ruczinski, I.; Ray, A.L.; Nath, A.; Wu, L.S.; Semba, R.D. Hepcidin and iron status among pregnant women in Bangladesh. Asia Pac. J. Clin. Nutr. 2008, 17, 451–456. [Google Scholar] [PubMed]
- Young, M.F.; Griffin, I.; Pressman, E.; McIntyre, A.W.; Cooper, E.; McNanley, T.; Harris, Z.L.; Westerman, M.; O'Brien, K.O. Maternal hepcidin is associated with placental transfer of iron derived from dietary heme and nonheme sources. J. Nutr. 2012, 142, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Simavli, S.; Derbent, A.U.; Uysal, S.; Turhan, N.O. Hepcidin, iron status, and inflammation variables among healthy pregnant women in the Turkish population. J. Mater. Fetal Neonatal Med. 2014, 27, 75–79. [Google Scholar] [CrossRef]
- Ronnenberg, A.G.; Wood, R.J.; Wang, X.; Xing, H.; Chen, C.; Chen, D.; Guang, W.; Huang, A.; Wang, L.; Xu, X. Preconception hemoglobin and ferritin concentrations are associated with pregnancy outcome in a prospective cohort of Chinese women. J. Nutr. 2004, 134, 2586–2591. [Google Scholar] [PubMed]
- Akesson, A.; Bjellerup, P.; Berglund, M.; Bremme, K.; Vahter, M. Soluble transferrin receptor: Longitudinal assessment from pregnancy to postlactation. Obstetr. Gynecol. 2002, 99, 260–266. [Google Scholar] [CrossRef]
- Lorenz, L.; Peter, A.; Poets, C.F.; Franz, A.R. A review of cord blood concentrations of iron status parameters to define reference ranges for preterm infants. Neonatology 2013, 104, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Contreras, H.; Chim, N.; Credali, A.; Goulding, C.W. Heme uptake in bacterial pathogens. Curr. Opin. Chem. Biol. 2014, 19, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Raiten, D.J.; Ashour, F.A.S.; Ross, A.C.; Meydani, S.N.; Dawson, H.D.; Stephensen, C.B.; Brabin, B.J.; Ommen, B.V.; Suchdev, P.S.; Group, I.C. Inflammation and nutritional science for programs/policies and interpretation of research evidence (INSPIRE). J. Nutr. 2014, in press. [Google Scholar]
- Grant, F.K.; Suchdev, P.S.; Flores-Ayala, R.; Cole, C.R.; Ramakrishnan, U.; Ruth, L.J.; Martorell, R. Correcting for inflammation changes estimates of iron deficiency among rural Kenyan preschool children. J. Nutr. 2012, 142, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Kaestel, P.; Martinussen, T.; Aaby, P.; Michaelsen, K.F.; Friis, H. Serum retinol is associated with stage of pregnancy and the acute phase response in pregnant women in Guinea-Bissau. J. Nutr. 2012, 142, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Kuvibidila, S.; Vuvu, M. Unusual low plasma levels of zinc in non-pregnant Congolese women. Br. J. Nutr. 2009, 101, 1783–1786. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Intermittent Iron and Folic Acid Supplementation in Menstruating Women; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Nguyen, P.; Nava-Ocampo, A.; Levy, A.; O’Connor, D.L.; Einarson, T.R.; Taddio, A.; Koren, G. Effect of iron content on the tolerability of prenatal multivitamins in pregnancy. BMC Pregnancy Childbirth 2008, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Pena-Rosas, J.P.; De-Regil, L.M.; Dowswell, T.; Viteri, F.E. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2012, 12, CD004736. [Google Scholar] [PubMed]
- Bhutta, Z.A.; Imdad, A.; Ramakrishnan, U.; Martorell, R. Is it time to replace iron folate supplements in pregnancy with multiple micronutrients? Paediatr. Perinatal Epidemiol. 2012, 26 (Suppl. 1), S27–S35. [Google Scholar]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef] [PubMed]
- Suchdev, P.S.; De-Regil, L.M.; Walleser, S.; Vist, G.; Peña-Rosas, J. Multiple Micronutrient Powders for Home (Point of Use) Fortification of Foods in Pregnant Women: A Systematic Review; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Suchdev, P.S.; Peña-Rosas, J.; De-Regil, L. Multiple micronutrient powders for home (point-of-use) fortification of foods in pregnant women (protocol). Cochrane Database Syst. Rev. 2014, 6, CD011158. [Google Scholar]
- Milman, N. Postpartum anemia ii: Prevention and treatment. Ann. Hematol. 2012, 91, 143–154. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Suchdev, P.S.; Vist, G.E.; Walleser, S.; Pena-Rosas, J.P. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Cochrane Database Syst. Rev. 2011, 9, CD008959. [Google Scholar] [PubMed]
- Zlotkin, S.H.; Schauer, C.; Christofides, A.; Sharieff, W.; Tondeur, M.C.; Hyder, S.M. Micronutrient sprinkles to control childhood anaemia. PLoS Med. 2005, 2, e1. [Google Scholar] [CrossRef] [PubMed]
- Sazawal, S.; Black, R.E.; Ramsan, M.; Chwaya, H.M.; Stoltzfus, R.J.; Dutta, A.; Dhingra, U.; Kabole, I.; Deb, S.; Othman, M.K.; et al. Effects of routine prophylactic supplementation with iron and folic acid on admission to hospital and mortality in preschool children in a high malaria transmission setting: Community-based, randomised, placebo-controlled trial. Lancet 2006, 367, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Ojukwu, J.U.; Okebe, J.U.; Yahav, D.; Paul, M. Oral iron supplementation for preventing or treating anaemia among children in malaria-endemic areas. Cochrane Database Syst. Rev. 2009, 3, CD006589. [Google Scholar] [PubMed]
- Suchdev, P.S.; Leeds, I.L.; McFarland, D.A.; Flores, R. Is it time to change guidelines for iron supplementation in malarial areas? J. Nutr. 2010, 140, 875–876. [Google Scholar] [CrossRef]
- Iannotti, L.L.; Tielsch, J.M.; Btlack, M.M.; Black, R.E. Iron supplementation in early childhood: Health benefits and risks. Am. J. Clin. Nutr. 2006, 84, 1261–1276. [Google Scholar] [PubMed]
- McDonald, S.J.; Middleton, P.; Dowswell, T.; Morris, P.S. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst. Rev. 2013, 7, CD004074. [Google Scholar] [PubMed]
- Beard, J. Iron deficiency alters brain development and functioning. J. Nutr. 2003, 133, 1468S–1472S. [Google Scholar] [PubMed]
- Ruel, M.T.; Alderman, H. Nutrition-sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? Lancet 2013, 382, 536–551. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burke, R.M.; Leon, J.S.; Suchdev, P.S. Identification, Prevention and Treatment of Iron Deficiency during the First 1000 Days. Nutrients 2014, 6, 4093-4114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu6104093
Burke RM, Leon JS, Suchdev PS. Identification, Prevention and Treatment of Iron Deficiency during the First 1000 Days. Nutrients. 2014; 6(10):4093-4114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu6104093
Chicago/Turabian StyleBurke, Rachel M., Juan S. Leon, and Parminder S. Suchdev. 2014. "Identification, Prevention and Treatment of Iron Deficiency during the First 1000 Days" Nutrients 6, no. 10: 4093-4114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu6104093