Consumers’ Exposure to Nutrition and Health Claims on Pre-Packed Foods: Use of Sales Weighting for Assessing the Food Supply in Slovenia



Abstract
:
1. Introduction

{kind=link}
{kind=link}
| Reference to the NHCR | Claim Type | Definition | Examples of Wordings |
|---|---|---|---|
| Art. 8 | Nutrition claims | Claims referring to particular beneficial nutritional properties of the food | High in vitamin D |
| Art. 13 | Function claims (FC) | Claims referring to (a) the role of a nutrient or other substance in growth, development and the functions of the body; (b) psychological and behavioral functions; or (c) slimming or weight-control or a reduction in the sense of hunger or an increase in the sense of satiety or to the reduction of the available energy from the diet | Vitamin D contributes to the maintenance of normal bones. |
| Art. 14(1)a | Reduction of disease risk claim (RDRC) | Claims that state, suggest or imply that the consumption of a food (constituent/category) significantly reduces a risk factor in the development of a human disease | Vitamin D helps to reduce the risk of falling associated with postural instability and muscle weakness. Falling is a risk factor for bone fractures among men and women 60 years of age and older. |
| Art. 14(1)b | Children's development and health claims (CDHC) | No specific definition in the regulation | Vitamin D is needed for normal growth and development of bone in children. |
| Art. 10(3) Art. 1(3) | General non-specific health claim | References to general, non-specific benefits of the nutrient or food for overall good health or health-related well-being. Such claims can also include trademarks and brand names. | Bone health support |
2. Experimental Section
2.1. Collection of Data

| Food Category | N | Nutrition Claim(s) | Health Claim (s) | Nutrition and/or Health Claim (s) | Health Symbol | Nutrition Declaration | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | ||
| Milk | 53 | 53% | 68% | 11% | 3% | 53% | 68% | 2% | 1% | 94% | 97% |
| Yoghurt and fermented milk drinks | 294 | 65% | 64% | 51% | 46% | 66% | 65% | 14% | 20% | 94% | 98% |
| Butter and spreads | 196 | 51% | 49% | 18% | 26% | 56% | 60% | 0% | 0% | 79% | 71% |
| Cheese | 335 | 21% | 30% | 2% | 10% | 21% | 30% | 1% | 8% | 45% | 72% |
| Other dairy products | 138 | 20% | 10% | 4% | 2% | 20% | 10% | 0% | 0% | 70% | 63% |
| Whole eggs | 42 | 19% | 1% | 5% | 1% | 24% | 2% | 0% | 0% | 14% | 6% |
| Frozen fruit & vegetables | 111 | 4% | 1% | 1% | 0% | 4% | 1% | 0% | 0% | 90% | 90% |
| Frozen ready meals | 239 | 10% | 6% | 2% | 1% | 11% | 6% | 0% | 0% | 89% | 95% |
| Breakfast cereals | 276 | 79% | 83% | 31% | 19% | 80% | 84% | 5% | 7% | 96% | 97% |
| Breads and similar products | 297 | 47% | 10% | 8% | 3% | 47% | 10% | 2% | 1% | 59% | 26% |
| Fine bakery wares (biscuits) | 323 | 26% | 22% | 5% | 2% | 26% | 22% | 0% | 0% | 53% | 51% |
| Pasta & rice | 436 | 27% | 11% | 11% | 13% | 31% | 23% | 3% | 1% | 86% | 80% |
| Fruit juice & smoothies | 240 | 95% | 99% | 15% | 14% | 95% | 99% | 0% | 0% | 95% | 100% |
| Soft drinks and water | 459 | 63% | 41% | 9% | 10% | 63% | 42% | 0% | 0% | 83% | 62% |
| Teas | 362 | 21% | 33% | 19% | 5% | 31% | 34% | 0% | 0% | 13% | 18% |
| Peas, beans & lentils | 97 | 10% | 2% | 6% | 2% | 11% | 3% | 4% | 2% | 56% | 60% |
| Processed meats | 429 | 15% | 8% | 7% | 4% | 17% | 11% | 3% | 3% | 45% | 62% |
| Processed seafood | 237 | 25% | 35% | 3% | 1% | 26% | 35% | 0% | 0% | 49% | 70% |
| Ready meals – full meal | 96 | 19% | 10% | 0% | 0% | 19% | 10% | 0% | 0% | 89% | 84% |
| Ready meals – other | 133 | 6% | 3% | 2% | 1% | 6% | 3% | 0% | 0% | 59% | 64% |
| Vegetable fats and oils | 194 | 33% | 12% | 20% | 6% | 38% | 14% | 10% | 4% | 56% | 22% |
| Milk imitates | 35 | 94% | 98% | 6% | 13% | 94% | 98% | 0% | 0% | 100% | 100% |
| Yoghurt imitates | 27 | 81% | 82% | 63% | 72% | 81% | 82% | 0% | 0% | 100% | 100% |
| Chewing gum | 55 | 0% | 0% | 9% | 3% | 9% | 3% | 0% | 0% | 71% | 80% |
| TOTAL | 5104 | 37% | 13% | 39% | 2% | 67% | |||||
| TOTAL (excluding eggs and chewing gums) | 5007 | 37% | 45% | 13% | 11% | 39% | 46% | 2% | 2% | 67% | 72% |
| Food Category | Energy | Protein | Sugar | Fat | Fiber | Sodium/Salt | Mineral (s) | Vitamin (s) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | SCE | SWE | |
| Milk | 2% | 1% | 2% | 1% | 47% | 65% | 6% | 3% | ||||||||
| Yoghurt and fermented milk drinks | 0% | 1% | 3% | 2% | 3% | 1% | 23% | 33% | 3% | 6% | 13% | 9% | 8% | 8% | ||
| Butter and spreads | 1% | 0% | 18% | 9% | 5% | 0% | 1% | 0% | 3% | 1% | 21% | 44% | ||||
| Cheese | 0% | 0% | 6% | 24% | 0% | 0% | 12% | 11% | 3% | 3% | ||||||
| Other dairy products | 1% | 0% | 1% | 1% | 2% | 1% | 15% | 7% | 8% | 5% | ||||||
| Whole eggs | 7% | 0% | 10% | 0% | ||||||||||||
| Frozen fruit and vegetables | 1% | 0% | 3% | 1% | 1% | 0% | ||||||||||
| Frozen ready meals | 4% | 1% | 1% | 0% | 3% | 1% | 2% | 0% | 2% | 0% | ||||||
| Breakfast cereals | 15% | 5% | 8% | 3% | 38% | 32% | 8% | 1% | 37% | 43% | 47% | 66% | ||||
| Breads and similar products | 0% | 0% | 1% | 0% | 5% | 1% | 33% | 7% | 1% | 0% | 4% | 2% | 1% | 1% | ||
| Fine bakery wares (biscuits) | 0% | 0% | 1% | 1% | 3% | 1% | 14% | 11% | 2% | 0% | 6% | 14% | 3% | 1% | ||
| Pasta & rice | 4% | 0% | 10% | 3% | 7% | 6% | 3% | 4% | ||||||||
| Fruit juice and smoothies | 0% | 0% | 38% | 34% | 1% | 0% | 0% | 0% | 0% | 0% | 8% | 13% | 29% | 23% | ||
| Soft drinks and water | 20% | 15% | 4% | 1% | 2% | 0% | 3% | 5% | 9% | 11% | 23% | 10% | ||||
| Teas | 0% | 0% | 1% | 0% | 4% | 8% | ||||||||||
| Peas, beans, and lentils | 2% | 0% | 7% | 2% | 5% | 0% | 5% | 0% | ||||||||
| Processed meats | 1% | 0% | 4% | 4% | 1% | 0% | 0% | 0% | 0% | 0% | ||||||
| Processed seafood | 1% | 0% | 2% | 0% | 1% | 0% | 5% | 15% | 5% | 14% | ||||||
| Ready meals—full meal | 1% | 1% | 1% | 0% | 6% | 7% | 2% | 3% | 2% | 0% | 2% | 0% | ||||
| Ready meals—other | 1% | 0% | 4% | 3% | ||||||||||||
| Vegetable fats and oils | 1% | 0% | 19% | 10% | ||||||||||||
| Milk imitates | 20% | 31% | 6% | 13% | 3% | 6% | 34% | 55% | 9% | 1% | ||||||
| Yoghurt imitates | 19% | 20% | 4% | 1% | 22% | 17% | 4% | 7% | 4% | 11% | 41% | 27% | 19% | 16% | ||
| Chewing gum | ||||||||||||||||
| TOTAL | 2% | 1% | 4% | 4% | 7% | 1% | 8% | 10% | ||||||||
| Health claim category | Health relationship (classification according to ICF/WHO body functions) | |||||||||||||||||
| Food category | N | General non-specific health claims | Function claims | Children's development and health | Reduction of disease risk claims | Mental functions (b1) | Cardiovascular system functions (b410-b429) | Haematological system functions (b430) | - Blood cholesterol levels (b4302) | Immunological system functions (b435) | Digestive system functions (b510-b539) | - Glycaemic response (b5152) | - Weight maintenancefunctions (b530) | Metabolic functions (b540-b559) | Bones (b720) & teeth functions (b5101) | Muscle functions (b730-b749) | Functions of the skin, hair, nails (b810-b869) | |
| Milk | 53 | 7.5% | 1.9% | 3.8% | 1.9% | 1.9% | 1.9% | 1.9% | 1.9% | 1.9% | ||||||||
| Yoghurt and fermented milk drinks | 294 | 35.4% | 24.1% | 1.0% | 0.3% | 1.0% | 1.0% | 7.1% | 12.2% | 2.7% | 2.4% | |||||||
| Butter and spreads | 196 | 13.8% | 4.6% | 0.5% | 1.0% | 2.0% | 2.0% | 2.0% | 0.5% | |||||||||
| Cheese | 335 | 0.9% | 0.9% | 0.6% | 0.9% | |||||||||||||
| Other dairy products | 138 | 3.6% | 3.6% | |||||||||||||||
| Whole eggs | 42 | 4.8% | 4.8% | |||||||||||||||
| Frozen fruit & vegetables | 111 | 0.9% | ||||||||||||||||
| Frozen ready meals | 239 | 2.1% | ||||||||||||||||
| Breakfast cereals | 276 | 10.1% | 19.6% | 1.1% | 0.4% | 5.8% | 2.5% | 2.9% | 2.5% | 2.5% | 7.2% | 3.3% | 7.2% | 1.1% | 2.5% | 0.7% | 0.4% | |
| Breads and similar products | 297 | 4.0% | 4.0% | 0.3% | 0.7% | 1.0% | 1.0% | 0.3% | 2.4% | 1.3% | 1.3% | 0.3% | 0.7% | 0.3% | ||||
| Fine bakery wares (biscuits) | 323 | 1.5% | 4.3% | 0.3% | 0.9% | 3.1% | 0.9% | 1.5% | 0.9% | 0.9% | ||||||||
| Pasta & rice | 436 | 0.9% | 8.0% | 0.2% | 0.2% | 0.2% | 0.2% | 5.0% | 4.1% | 3.0% | 0.2% | 0.2% | ||||||
| Fruit juice & smoothies | 240 | 6.3% | 9.2% | 0.4% | 1.7% | 1.3% | 3.3% | 1.3% | 1.3% | 0.4% | ||||||||
| Soft drinks and water | 459 | 3.7% | 7.6% | 2.4% | 1.7% | 2.6% | 1.1% | 2.4% | 1.7% | 2.0% | 0.7% | |||||||
| Teas | 362 | 3.0% | 17.1% | 3.9% | 1.1% | 9.1% | 6.4% | 1.4% | 0.3% | 0.8% | ||||||||
| Peas, beans & lentils | 97 | 1.0% | 1.0% | 1.0% | 1.0% | 1.0% | 1.0% | 1.0% | 1.0% | |||||||||
| Processed meats | 429 | 4.9% | 0.2% | 0.2% | 0.2% | |||||||||||||
| Processed seafood | 237 | 2.1% | 0.8% | 0.8% | ||||||||||||||
| Ready meals - full meal | 96 | |||||||||||||||||
| Ready meals - other | 133 | 0.8% | 2.3% | 0.8% | 0.8% | 0.8% | 0.8% | 0.8% | ||||||||||
| Vegetable fats and oils | 194 | 5.2% | 7.7% | 1.5% | 1.0% | 5.7% | 0.5% | 0.5% | 2.1% | 1.5% | 0.5% | 0.5% | ||||||
| Milk imitates | 35 | 5.7% | ||||||||||||||||
| Yoghurt imitates | 27 | 55.6% | 7.4% | 7.4% | ||||||||||||||
| Chewing gum | 55 | 9.1% | 1.8% | 7.3% | ||||||||||||||
| TOTAL | 5104 | 5.6% | 7.0% | 0.1% | 0.2% | 1.0% | 0.6% | 0.5% | 0.4% | 1.8% | 2.8% | 0.8% | 1.4% | 0.4% | 0.7% | 0.2% | 0.2% | |
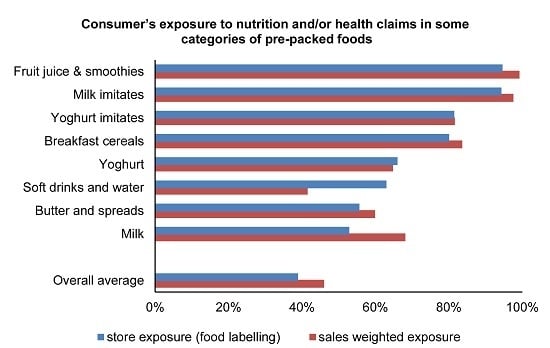
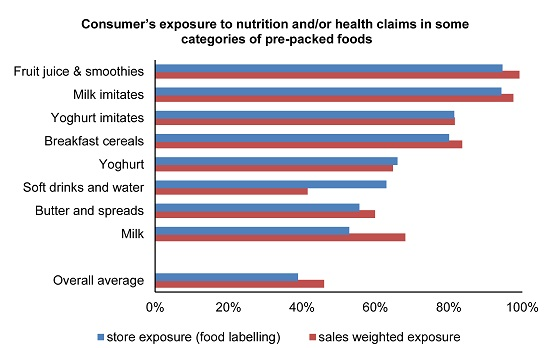
2.2. Consumers’ Exposure to Nutrition/Health Claims and Health Symbols on Pre-Packed Foods
2.3. Data Validation
2.4. Statistical Analyses
3. Results and Discussion
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pothoulaki, M.; Chryssochoidis, G. Health claims: Consumers’ matters. J. Funct. Foods 2009, 1, 222–228. [Google Scholar] [CrossRef]
- Nocella, G.; Kennedy, O. Food health claims: What consumers understand. Food Policy 2012, 37, 571–580. [Google Scholar] [CrossRef]
- Wills, J.M.; Storcksdieck genannt Bonsmann, S.; Kolka, M.; Grunert, K.G. European consumers and health claims: Attitudes, understanding and purchasing behaviour. Proc. Nutr. Soc. 2012, 71, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Van Wezemael, L.; Caputo, V.; Nayga, R.M.; Chryssochoidis, G.; Verbeke, W. European consumer preferences for beef with nutrition and health claims: A multi-country investigation using discrete choice experiments. Food Policy 2014, 44, 167–176. [Google Scholar] [CrossRef]
- Miklavec, K.; Pravst, I.; Grunert, K.G.; Klopčič, M.; Pohar, J. The influence of health claims and nutritional composition on consumers’ yoghurt preferences. Food Qual. Prefer. 2015, 43, 26–33. [Google Scholar] [CrossRef]
- Hoefkens, C.; Verbeke, W. Consumers’ Health-Related Motive Orientations and Reactions to Claims about Dietary Calcium. Nutrients 2013, 5, 82–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saarinen, N.M.; Tuominen, J.; Pylkkänen, L.; Santti, R. Assessment of Information to Substantiate a Health Claim on the Prevention of Prostate Cancer by Lignans. Nutrients 2010, 2, 99–115. [Google Scholar] [CrossRef] [PubMed]
- Hieke, S.; Kuljanic, N.; Wills, J.M.; Pravst, I.; Kaur, A.; Raats, M.M.; van Trijp, H.C.M.; Verbeke, W.; Grunert, K.G. The role of health-related claims and health-related symbols in consumer behaviour: Design and conceptual framework of the CLYMBOL project and initial results. Nutr. Bull. 2015, 40, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Union. Regulation (EC) No. 1924/2006 of the European Parliament and of the Council of 20 December 2006 on Nutrition and Health Claims Made on Foods. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32006R1924 (accessed on 2 October 2015).
- Pravst, I. Risking public health by approving some health claims?—The case of phosphorus. Food Policy 2011, 36, 725–727. [Google Scholar] [CrossRef]
- Pravst, I. The evaluation of health claims in Europe: What have we learned? Agro Food Ind. HiTech 2010, 21, 4–6. [Google Scholar]
- Cappuccio, F.P.; Pravst, I. Health claims on foods: Promoting healthy food choices or high salt intake? Br. J. Nutr. 2011, 106, 1770–1771. [Google Scholar] [CrossRef] [PubMed]
- Sacco, J.E.; Sumanac, D.; Tarasuk, V. Front-of-package references to fiber on foods in Canadian supermarkets highlight the need for increased nutrition knowledge among consumers. J. Nutr. Educ. Behav. 2013, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Schermel, A.; Emrich, T.E.; Arcand, J.; Wong, C.L.; L’Abbe, M.R. Nutrition marketing on processed food packages in Canada: 2010 Food Label Information Program. Appl. Physiol. Nutr. Metab. 2013, 38, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Colby, S.E.; Johnson, L.; Scheett, A.; Hoverson, B. Nutrition marketing on food labels. J. Nutr. Educ. Behav. 2010, 42, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Brecher, S.J.; Bender, M.M.; Wilkening, V.L.; McCabe, N.M.; Anderson, E.M. Status of nutrition labeling, health claims, and nutrient content claims for processed foods: 1997 Food Label and Package Survey. J. Am. Diet. Assoc. 2000, 100, 1057–1062. [Google Scholar] [CrossRef]
- Hughes, C.; Wellard, L.; Lin, J.; Suen, K.L.; Chapman, K. Regulating health claims on food labels using nutrient profiling: What will the proposed standard mean in the Australian supermarket? Public Health Nutr. 2013, 16, 2154–2161. [Google Scholar] [CrossRef] [PubMed]
- Devi, A.; Eyles, H.; Rayner, M.; Ni Mhurchu, C.; Swinburn, B.; Lonsdale-Cooper, E.; Vandevijvere, S. Nutritional quality, labelling and promotion of breakfast cereals on the New Zealand market. Appetite 2014, 81, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.Z.; Woods, J.L.; Rickard, C.A.; Wong, C.K. Product variety in Australian snacks and drinks: How can the consumer make a healthy choice? Public Health Nutr. 2008, 11, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Yeatman, H.; Ridges, L.; Houston, A.; Rafferty, J.; Ridges, A.; Roesler, L.; Sobierajski, M.; Spratt, B. Nutrition function, health and related claims on packaged Australian food products—Prevalence and compliance with regulations. Asia Pac. J. Clin. Nutr. 2006, 15, 10–20. [Google Scholar] [PubMed]
- Williams, P.; Yeatman, H.; Zakrzewski, S.; Aboozaid, B.; Henshaw, S.; Ingram, K.; Rankine, A.; Walcott, S.; Ghani, F. Nutrition and related claims used on packaged Australian foods—Implications for regulation. Asia Pac. J. Clin. Nutr. 2003, 12, 138–150. [Google Scholar] [PubMed]
- Storcksdieck genannt Bonsmann, S.; Fernandez Celemin, L.; Larranaga, A.; Egger, S.; Wills, J.M.; Hodgkins, C.; Raats, M.M. Penetration of nutrition information on food labels across the EU-27 plus Turkey. Eur. J. Clin. Nutr. 2010, 64, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Lalor, F.; Kennedy, J.; Flynn, M.A.; Wall, P.G. A study of nutrition and health claims—A snapshot of what’s on the Irish market. Public Health Nutr. 2010, 13, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Kaur, A.; Scarborough, P.; Matthews, A.; Payne, S.; Mizdrak, A.; Rayner, M. How many foods in the UK carry health and nutrition claims, and are they healthier than those that do not? Public Health Nutr. 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Korosec, Z.; Pravst, I. Assessing the average sodium content of prepacked foods with nutrition declarations: The importance of sales data. Nutrients 2014, 6, 3501–3515. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, J.; Barron, J.; Gunn, J.; Yuan, K.; Perrine, C.; Cogswell, M. Iodized salt sales in the United States. Nutrients 2015, 7, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Rayner, M.; Wood, A.; Lawrence, M.; Ni Mhurchu, C.; Albert, J.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; Kumanyika, S.; et al. Monitoring the health-related labelling of foods and non-alcoholic beverages in retail settings. Obes. Rev. 2013, 14, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Dunford, E.; Neal, B.; Macgregor, G.; Czernichow, S.; Ni Mhurchu, C.; Food Monitoring, G. International collaborative project to compare and track the nutritional composition of fast foods. BMC Public Health 2012, 12. [Google Scholar] [CrossRef]
- European Food Safety Authority. The Food Classification and Description System FoodEx2. Available online: http://www.efsa.europa.eu/en/supporting/pub/215e.htm (accessed on 2 October 2015).
- World Health Organization. ICF Browser. Available online: http://apps.who.int/classifications/icfbrowser/ (accessed on 2 October 2015).
- Davidović, D.B.; Tomić, D.V.; Paunović, K.Ž.; Vasiljević, N.D.; Jorga, J.B. Nutrition labelling of pre-packaged foods in Belgrade, Serbia: Current situation. Public Health Nutr. 2015, 18, 1969–1978. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.L.; Mummery, K.W. Characteristics of consumers using “better for you” front-of-pack food labelling schemes—An example from the Australian Heart Foundation Tick. Public Health Nutr. 2013, 16, 2265–2272. [Google Scholar] [CrossRef] [PubMed]
- Lahti-Koski, M.; Helakorpi, S.; Olli, M.; Vartiainen, E.; Puska, P. Awareness and use of the Heart Symbol by Finnish consumers. Public Health Nutr. 2012, 15, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Bend, D.; Dieren, J.V.; Marques, M.D.V.; Wezenbeek, N.; Kostareli, N.; Rodrigues, P.; Temme, E.; Westenbrink, S.; Verhagen, H. A simple visual model to compare existing front-of-pack nutrient profiling schemes. Eur. J. Nutr. Food Saf. 2014, 4, 429–534. [Google Scholar] [CrossRef]
- European Commission. EU Register of Nutrition and Health Claims Made on foods. Available online: http://ec.europa.eu/nuhclaims/ (accessed on 2 October 2015).
- Shimizu, T. Health Claims Regulation and Scientific Substantiation of Functional Foods and the International Comparison. In Clinical Aspects of Functional Foods and Nutraceuticals; Ghosh, D., Bagchi, D., Konishi, T., Eds.; CRC Press: Boca Raton, FL, USA, 2015; pp. 217–255. [Google Scholar]
- Lalor, F.; Wall, P.G. Health claims regulations: Comparison between USA, Japan and European Union. Br. Food J. 2011, 113, 298–313. [Google Scholar] [CrossRef]
- Berhaupt-Glickstein, A.; Nucci, M.L.; Hooker, N.H.; Hallman, W.K. The evolution of language complexity in qualified health claims. Food Policy 2014, 47, 62–70. [Google Scholar] [CrossRef]
- Van‘t Riet, J. Sales effects of product health information at points of purchase: A systematic review. Public Health Nutr. 2013, 16, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Debeljak, K.; Pravst, I.; Košmelj, K.; Kač, M. “Healthier” and “less heathy” classifications according to three nutrient profiling systems relative to nutrition and health claims on food labels. Acta Aliment. 2015, 44, 561–565. [Google Scholar] [CrossRef]
- Eržen, N.; Rayner, M.; Pravst, I. A comparative evaluation of the use of a food composition database and nutrition declarations for nutrient profiling. J. Food Nutr. Res. 2015, 54, 93–100. [Google Scholar] [CrossRef]
- Eržen, N.; Kač, M.; Pravst, I. Perceived healthfulness of dairy products and their imitations: Nutrition experts’ perspective. Agro Food Ind. HiTech 2014, 25, 24. [Google Scholar]
- Dunford, E.; Webster, J.; Metzler, A.B.; Czernichow, S.; Ni Mhurchu, C.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; Maulik, P.K.; et al. International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 19, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pravst, I.; Kušar, A. Consumers’ Exposure to Nutrition and Health Claims on Pre-Packed Foods: Use of Sales Weighting for Assessing the Food Supply in Slovenia. Nutrients 2015, 7, 9353-9368. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7115474
Pravst I, Kušar A. Consumers’ Exposure to Nutrition and Health Claims on Pre-Packed Foods: Use of Sales Weighting for Assessing the Food Supply in Slovenia. Nutrients. 2015; 7(11):9353-9368. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7115474
Chicago/Turabian StylePravst, Igor, and Anita Kušar. 2015. "Consumers’ Exposure to Nutrition and Health Claims on Pre-Packed Foods: Use of Sales Weighting for Assessing the Food Supply in Slovenia" Nutrients 7, no. 11: 9353-9368. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7115474