A Priori and a Posteriori Dietary Patterns during Pregnancy and Gestational Weight Gain: The Generation R Study

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
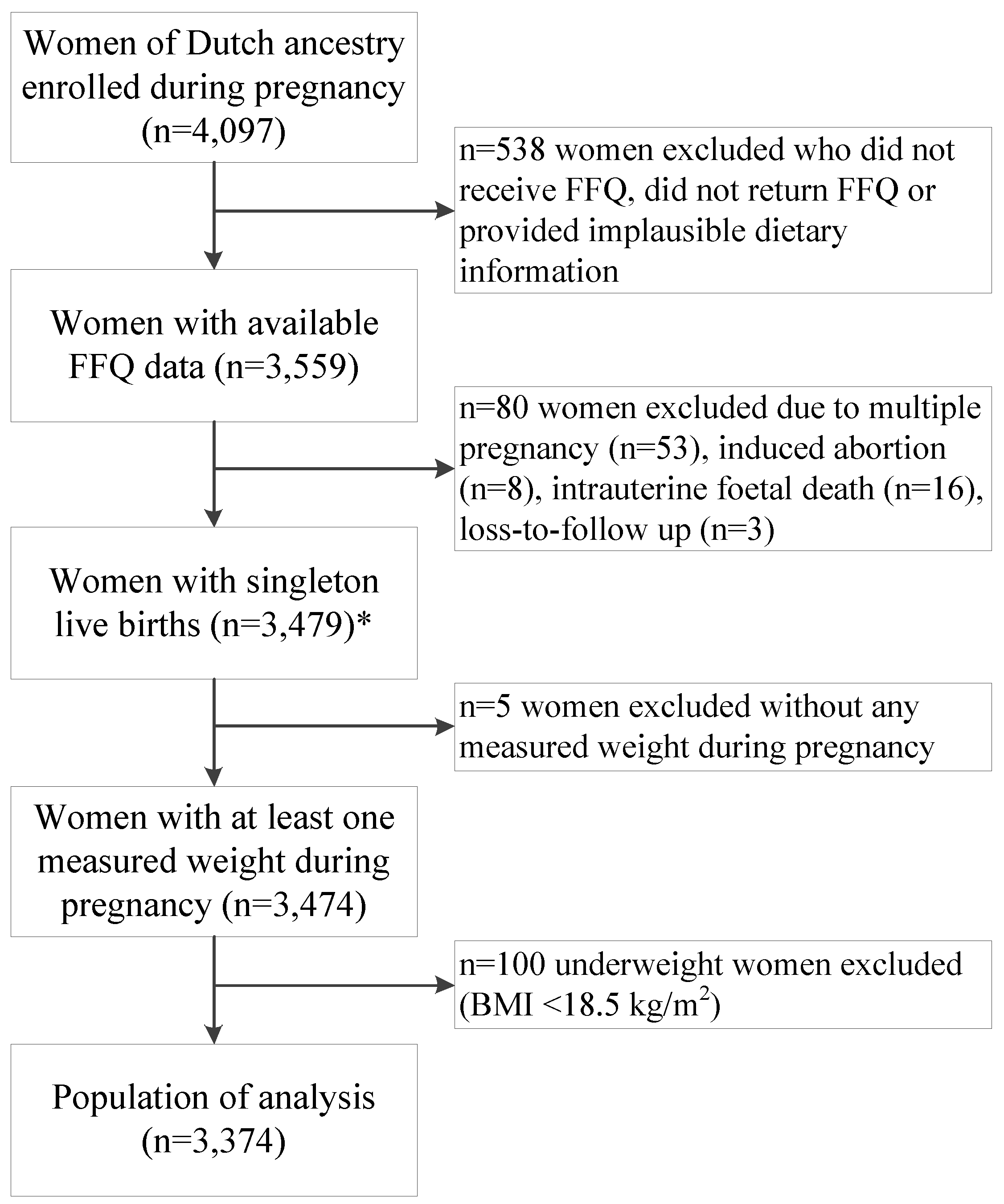
2.2. Population of Analysis

2.3. Dietary Assessment
2.3.1. A Posteriori-Derived Dietary Patterns

{kind=link}
| Food Group | “Vegetable, Oil and Fish” Dietary Pattern | “Nuts, High-Fiber Cereals and Soy” Dietary Pattern | “Margarine, Sugar and Snacks” Dietary Pattern |
|---|---|---|---|
| Potatoes and other tubers | 0.05 | −0.53 | 0.21 |
| Vegetables | 0.78 * | 0.17 | −0.03 |
| Fruits | 0.13 | 0.37 | 0.02 |
| Dairy products—high fat | 0.26 | −0.26 | 0.29 |
| Dairy products—low fat | −0.15 | 0.29 | 0.16 |
| Cereals—high fiber | 0.24 | 0.43 * | 0.36 |
| Cereals—low fiber | 0.23 | −0.16 | 0.25 |
| Meat and meat products | 0.08 | −0.54 | 0.33 |
| Fish and shellfish | 0.45 * | 0.24 | −0.11 |
| Eggs and egg products | 0.27 | 0.05 | 0.19 |
| Vegetable oils | 0.74 * | 0.08 | −0.12 |
| Margarine and butter | −0.06 | −0.03 | 0.61 * |
| Sugar and confectionary and cakes | −0.11 | 0.13 | 0.56 * |
| Snacks | 0.05 | 0.08 | 0.40 * |
| Coffee and tea | 0.28 | 0.34 | 0.10 |
| Sugar-containing beverages | −0.14 | −0.28 | 0.29 |
| Light soft drinks | 0.13 | 0.28 | 0.02 |
| Alcoholic beverages | 0.35 | −0.00 | −0.04 |
| Condiments and sauces | 0.05 | −0.09 | 0.39 |
| Soups and bouillon | 0.19 | −0.02 | 0.15 |
| Nuts, seeds and olives | 0.03 | 0.64 * | 0.30 |
| Soy products | 0.01 | 0.39 * | −0.10 |
| Legumes | 0.44 | −0.02 | 0.07 |
2.3.2. A Priori-Defined Dietary Pattern
2.4. Maternal Weight Gain
2.4.1. Gestational Weight Gain during Different Phases in Pregnancy
2.4.2. Adequacy of Gestational Weight Gain
2.5. Covariates
2.6. Statistical Analyses
Sensitivity Analyses
3. Results
3.1. Study Population
| Subject Characteristics | Normal Weight Women (n = 2544) | Overweight Women (n = 830) |
|---|---|---|
| Age (years) | 31.6 ± 4.3 | 31.0 ± 4.4 |
| Educational level, n (%) | ||
| Low and midlow | 307 (12.1) | 201 (24.2) |
| Midhigh | 1283 (50.4) | 436 (52.5) |
| High | 954 (37.5) | 193 (23.3) |
| Household income, n (%) | ||
| <2200 Euro/month | 620 (24.4) | 266 (32.1) |
| ≥2200 Euro/month | 1924 (75.6) | 564 (67.9) |
| Parity, n (%) | ||
| 0 | 1554 (61.1) | 465 (56.0) |
| ≥1 | 990 (38.9) | 365 (44.0) |
| Pre-pregnancy BMI (kg/m2) | 21.6 (20.4–23.0) | 27.7 (26.0–30.5) |
| Smoking during pregnancy, n (%) | ||
| Never during pregnancy | 1911 (75.1) | 612 (73.7) |
| Until pregnancy was known | 233 (9.2) | 61 (7.3) |
| Continued throughout pregnancy | 400 (15.7) | 157 (19.0) |
| Alcohol consumption during pregnancy, n (%) | ||
| Never during pregnancy | 764 (30.0) | 359 (43.2) |
| Until pregnancy was known | 416 (16.4) | 138 (16.6) |
| Continued throughout pregnancy | 1364 (53.6) | 334 (40.2) |
| Stress during pregnancy (score 0–4) | 0.12 (0.06–0.24) | 0.13 (0.06–0.26) |
| Energy intake (kcal/day) | 2162 ± 507 | 2090 ± 514 |
| Dutch Healthy Diet Index (score 0–60) | 32 ± 8 | 30 ± 8 |
| Fetal sex, n (%) | ||
| Male | 1287 (50.6) | 415 (50.0) |
| Female | 1257 (49.4) | 415 (50.0) |
| Gestational weight gain (kg) | 14.7 ± 7.3 | 12.9 ± 7.7 |
| Adequacy of gestational weight gain, n (%) | ||
| Inadequate | 370 (24.8) | 89 (20.9) |
| Adequate | 565 (37.9) | 67 (15.8) |
| Excessive | 557 (37.3) | 269 (63.3) |
3.2. Dietary Patterns and Gestational Weight Gain in Different Phases in Pregnancy
| Quartiles of the Dietary Patterns | Early-Pregnancy Weight Gain (g/Week) | |||
|---|---|---|---|---|
| Normal Weight Women (n = 1849) | Overweight Women (n = 576) | |||
| Model 1 | Model 2 | Model 1 | Model 2 | |
| “Vegetable, Oil And Fish” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −8 (−34; 17) | −3 (−28; 23) | 18 (−44; 80) | 29 (−34; 91) |
| Q3 | −14 (−40; 11) | −4 (−30; 22) | 59 (−3; 121) | 77 (14; 141) |
| Q4 (high) | 38 (12; 63) * | 43 (16; 69) * | 4 (−58; 66) | 31 (−37; 99) |
| Per SD | p < 0.01 * | p < 0.01 * | p = 0.63 | p = 0.24 |
| “Nuts, High-Fiber Cereals and Soy” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −10 (−36; 15) | 5 (−21; 30) | −19 (−81; 43) | −17 (−79; 45) |
| Q3 | −26 (−52; −1) | −4 (−31; 23) | −54 (−117; 10) | −44 (−109; 21) |
| Q4 (high) | −31 (−57; −6) | −10 (−37; 18) | −64 (−128; 1) | −52 (−120; 15) |
| Per SD | p < 0.01 * | p = 0.22 | p = 0.02 | p = 0.06 |
| “Margarine, Sugar and Snacks” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 3 (−22; 29) | 2 (−23; 27) | 33 (−28; 94) | 28 (−32; 88) |
| Q3 | 5 (−21; 30) | −1 (−26; 24) | 35 (−29; 98) | 41 (−22; 103) |
| Q4 (high) | 20 (−6; 46) | 13 (−12; 39) | 52 (−9; 114) | 45 (−17; 106) |
| Per SD | p = 0.11 | p = 0.36 | p = 0.20 | p = 0.24 |
| “Dutch Healthy Diet Index” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 0 (−25; 26) | −2 (−27; 23) | 4 (−58; 65) | 3 (−58; 64) |
| Q3 | 16 (−10; 42) | 7 (−19; 32) | 48 (−14; 110) | 38 (−23; 100) |
| Q4 (high) | 3 (−22; 29) | −14 (−40; 12) | 34 (−28; 96) | 11 (−54; 75) |
| Per SD | p = 0.86 | p = 0.17 | p = 0.32 | p = 0.86 |
| Quartiles of the Dietary Patterns | Mid-Pregnancy Weight Gain (g/Week) | |||
|---|---|---|---|---|
| Normal Weight Women (n = 2079) | Overweight Women (n = 669) | |||
| Model 1 | Model 2 | Model 1 | Model 2 | |
| “Vegetable, Oil and Fish” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −0 (−39; 38) | 6 (−33; 45) | 37 (−42; 115) | 17 (−64; 97) |
| Q3 | 2 (−36; 39) | 12 (−27; 51) | 21 (−59; 101) | 7 (−76; 90) |
| Q4 (high) | −13 (−52; 25) | −4 (−44; 36) | 23 (−56; 103) | −19 (−105; 68) |
| Per SD | p = 0.48 | p = 0.72 | p = 0.36 | p = 0.92 |
| “Nuts, High-Fiber Cereals and Soy” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 22 (−16; 60) | 25 (−14; 64) | 28 (−52; 107) | 8 (−73; 89) |
| Q3 | −7 (−46; 31) | −2 (−42; 39) | 47 (−33; 128) | 19 (−65; 102) |
| Q4 (high) | 25 (−13; 64) | 30 (−11; 70) | 62 (−19; 142) | 17 (−68; 103) |
| Per SD | p = 0.38 | p = 0.32 | p = 0.14 | p = 0.72 |
| “Margarine, Sugar and Snacks” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 31 (−7; 68) | 31 (−6; 69) | 25 (−53; 102) | 30 (−47; 107) |
| Q3 | 15 (−23; 53) | 18 (−21; 56) | 8 (−71; 87) | 17 (−62; 96) |
| Q4 (high) | 16 (−22; 54) | 18 (−20; 57) | 14 (−64; 92) | 24 (−54; 103) |
| Per SD | p = 0.44 | p = 0.40 | p = 0.65 | p = 0.48 |
| “Dutch Healthy Diet Index” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −15 (−53; 23) | −14 (−52; 24) | −36 (−113; 41) | −31 (−109; 47) |
| Q3 | −0 (−38; 37) | −1 (−39; 36) | −23 (−101; 54) | −4 (−81; 74) |
| Q4 (high) | −7 (−46; 31) | −10 (−49; 30) | −9 (−89; 70) | 27 (−56; 109) |
| Per SD | p = 0.66 | p = 0.76 | p = 0.43 | p = 0.88 |
| Quartiles of the Dietary Patterns | Late-Pregnancy Weight Gain (g/week) | |||
|---|---|---|---|---|
| Normal Weight Women (n = 2384) | Overweight Women (n = 774) | |||
| Model 1 | Model 2 | Model 1 | Model 2 | |
| “Vegetable, Oil and Fish” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −3 (−32; 26) | 10 (−20; 39) | 21 (−35; 78) | 36 (−21; 93) |
| Q3 | −18 (−47; 10) | −4 (−33; 26) | −3 (−60; 55) | 21 (−38; 80) |
| Q4 (high) | −19 (−47; 10) | −0 (−31; 30) | −8 (−64; 49) | 24 (−38; 86) |
| Per SD | p = 0.09 | p = 0.54 | p = 0.42 | p = 0.82 |
| “Nuts, High-Fiber Cereals and Soy” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −2 (−30; 27) | 14 (−15; 44) | 4 (−54; 62) | 18 (−41; 77) |
| Q3 | −16 (−45; 12) | 8 (−22; 38) | −3 (−60; 55) | 15 (−45; 74) |
| Q4 (high) | −37 (−65; −8) | −13 (−43; 18) | 3 (−55; 61) | 21 (−41; 83) |
| Per SD | p < 0.01 * | p = 0.48 | p = 0.91 | p = 0.66 |
| “Margarine, Sugar and Snacks” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −21 (−49; 8) | −20 (−48; 8) | −8 (−65; 49) | −7 (−63; 50) |
| Q3 | −12 (−41; 16) | −12 (−40; 17) | 7 (−49; 64) | 17 (−40; 74) |
| Q4 (high) | −5 (−34; 24) | −6 (−35; 23) | 8 (−49; 65) | 10 (−48; 68) |
| Per SD | p = 0.86 | p = 0.76 | p = 0.64 | p = 0.66 |
| “Dutch Healthy Diet Index” Pattern | ||||
| Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | −14 (−43; 14) | −13 (−41;15) | 46 (−10; 102) | 51 (−5; 108) |
| Q3 | −2 (−31; 27) | −10 (−39; 18) | 23 (−34; 81) | 25 (−33; 82) |
| Q4 (high) | −3 (−31; 26) | −14 (−43; 15) | 33 (−24; 90) | 28 (−31; 88) |
| Per SD | p = 0.61 | p = 0.57 | p = 0.46 | p = 0.58 |
3.3. Dietary Patterns and Gestational Weight Gain Adequacy
| Quartiles of the Dietary Patterns | Inadequate GWG (n = 459) | Adequate GWG (n = 632) | Excessive GWG (n = 826) |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | ||
| “Vegetable, Oil and Fish” Pattern | |||
| Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.85 (0.60; 1.22) | Reference | 1.08 (0.79; 1.48) |
| Q3 | 0.86 (0.60; 1.23) | Reference | 1.05 (0.76; 1.46) |
| Q4 (high) | 0.84 (0.58; 1.22) | Reference | 1.06 (0.76; 1.48) |
| Per SD | p = 0.21 | p = 0.91 | |
| “Nuts, High-Fiber Cereals and Soy” Pattern | |||
| Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.77 (0.53; 1.13) | Reference | 1.16 (0.82; 1.62) |
| Q3 | 0.86 (0.59; 1.25) | Reference | 1.26 (0.89; 1.77) |
| Q4 (high) | 0.85 (0.58; 1.24) | Reference | 1.09 (0.77; 1.53) |
| Per SD | p = 0.76 | p = 0.46 | |
| “Margarine, Sugar and Snacks” Pattern | |||
| Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.97 (0.69; 1.36) | Reference | 1.40 (1.04; 1.90) |
| Q3 | 0.93 (0.66; 1.32) | Reference | 1.37 (1.00; 1.87) |
| Q4 (high) | 0.98 (0.69; 1.40) | Reference | 1.45 (1.06; 1.99) |
| Per SD | p = 0.73 | p = 0.09 | |
| “Dutch Healthy Diet Index” Pattern | |||
| Q1 (low) | Reference | Reference | Reference |
| Q2 | 1.04 (0.74; 1.45) | Reference | 0.92 (0.69; 1.24) |
| Q3 | 0.84 (0.59; 1.20) | Reference | 0.95 (0.70; 1.27) |
| Q4 (high) | 1.32 (0.92; 1.90) | Reference | 1.11 (0.80; 1.53) |
| Per SD | p = 0.07 | p = 0.66 | |
3.4. Dietary Patterns and trajectories of Gestational Weight
3.5. Sensitivity Analyses
4. Discussion
4.1. Summary of Main Findings
4.2. Interpretation and Comparison with Other Studies
4.3. Strengths and Limitations
4.4. Conclusions and Implications
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Han, Z.; Lutsiv, O.; Mulla, S.; Rosen, A.; Beyene, J.; McDonald, S.D.; Synthesis, G.K. Low gestational weight gain and the risk of preterm birth and low birthweight: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2011, 90, 935–954. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Sharma, A.J.; Sappenfield, W.; Wilson, H.G.; Salihu, H.M. Association of maternal body mass index, excessive weight gain, and gestational diabetes mellitus with large-for-gestational-age births. Obstet. Gynecol. 2014, 123, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Clifton, R.G.; Roberts, J.M.; Myatt, L.; Hauth, J.C.; Spong, C.Y.; Varner, M.W.; Wapner, R.J.; Thorp, J.M., Jr.; Mercer, B.M.; et al. Pregnancy outcomes with weight gain above or below the 2009 Institute of Medicine guidelines. Obstet. Gynecol. 2013, 121, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, R.; Durmus, B.; Hofman, A.; Mackenbach, J.P.; Steegers, E.A.; Jaddoe, V.W. Risk factors and outcomes of maternal obesity and excessive weight gain during pregnancy. Obesity 2013, 21, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.M.; Gunderson, E.P.; Ferrara, A. Gestational weight gain and risk of gestational diabetes mellitus. Obstet. Gynecol. 2010, 115, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.C.; Best, K.E.; Pearce, M.S.; Waugh, J.; Robson, S.C.; Bell, R. Cardiovascular disease risk in women with pre-eclampsia: Systematic review and meta-analysis. Eur. J. Epidemiol. 2013, 28, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Streuling, I.; Beyerlein, A.; Rosenfeld, E.; Schukat, B.; von Kries, R. Weight gain and dietary intake during pregnancy in industrialized countries—A systematic review of observational studies. J. Perinat. Med. 2011, 39, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuebe, A.M.; Oken, E.; Gillman, M.W. Associations of diet and physical activity during pregnancy with risk for excessive gestational weight gain. Am. J. Obstet. Gynecol. 2009, 201. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, A.S.; Skuladottir, G.V.; Thorsdottir, I.; Hauksson, A.; Steingrimsdottir, L. Maternal diet in early and late pregnancy in relation to weight gain. Int. J. Obes. (Lond.) 2006, 30, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, A.P.B.; Benicio, M.H.D. Influence of dietary intake during gestation on postpartum weight retention. Rev. Saude Publica 2011, 45, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Pitkin, R.M. Nutritional support in obstetrics and gynecology. Clin. Obstet. Gynecol. 1976, 19, 489–513. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Preparation and Use of Food-Based Dietary Guidelines: Report of a Joint Fao/Who Consultation; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- Uusitalo, U.; Arkkola, T.; Ovaskainen, M.L.; Kronberg-Kippila, C.; Kenward, M.G.; Veijola, R.; Simell, O.; Knip, M.; Virtanen, S.M. Unhealthy dietary patterns are associated with weight gain during pregnancy among Finnish women. Public Health Nutr. 2009, 12, 2392–2399. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Bianchi, L.; Chung, H.; Weatherspoon, L.; Song, W.O. Is gestational weight gain associated with diet quality during pregnancy? Matern. Child Health J. 2014, 18, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in Project Viva: A US cohort. J Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Hillesund, E.R.; Bere, E.; Haugen, M.; Overby, N.C. Development of a new nordic diet score and its association with gestational weight gain and fetal growth—A study performed in the Norwegian mother and child cohort study (MoBa). Public Health Nutr. 2014, 17, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- Kruithof, C.J.; Kooijman, M.N.; van Duijn, C.M.; Franco, O.H.; de Jongste, J.C.; Klaver, C.C.; Mackenbach, J.P.; Moll, H.A.; Raat, H.; Rings, E.H.; et al. The generation R study: Biobank update 2015. Eur. J. Epidemiol. 2014, 29, 911–927. [Google Scholar] [CrossRef] [PubMed]
- Donders-Engelen, M.; van der Heijden, L. Maten, Gewichten en Codenummers 2003 (Measures, Weights and Code Numbers 2003); Wageningen UR, Vakgroep Humane Voeding Wageningen and TNO Voeding: Zeist, The Netherlands, 2003. [Google Scholar]
- Netherlands-Nutrition-Centre. Dutch Food Composition Database 2006; Nevo: Hague, The Netherlands, 2006. [Google Scholar]
- Klipstein-Grobusch, K.; den Breeijen, J.H.; Goldbohm, R.A.; Geleijnse, J.M.; Hofman, A.; Grobbee, D.E.; Witteman, J.C. Dietary assessment in the elderly: Validation of a semiquantitative food frequency questionnaire. Eur. J. Clin. Nutr. 1998, 52, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H. The varimax criterion for analytic rotation in factor analysis. Psychometrika 1958, 23, 187–200. [Google Scholar] [CrossRef]
- Van den Broek, M.; Leermakers, E.T.; Jaddoe, V.W.; Steegers, E.A.; Rivadeneira, F.; Raat, H.; Hofman, A.; Franco, O.H.; Kiefte-de Jong, J.C. Maternal dietary patterns during pregnancy and body composition of the child at age 6 y: The generation R study. Am. J. Clin. Nutr. 2015, 102, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, I. Principal component analysis. In International Encyclopedia of Statistical Science; Springer: Berlin/Heidelberg, Germany, 2011; pp. 1094–1096. Available online: http://0-dx-doi-org.brum.beds.ac.uk/10.1007/978-3-642-04898-2_455 (accessed on 16 July 2015).
- Van Lee, L.; Geelen, A.; van Huysduynen, E.J.; de Vries, J.H.; van’t Veer, P.; Feskens, E.J. The Dutch healthy diet index (DHD-index): An instrument to measure adherence to the Dutch guidelines for a healthy diet. Nutr. J. 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Health Council of the Netherlands. Guidelines for a Healthy Diet 2006; Health Council of the Netherlands: Hague, The Netherlands, 2006. [Google Scholar]
- Rasmussen, K.M.; Yaktine, A.L.; Editors Committee to Reexamine IOM Pregnancy Weight Guidelines; Institute of Medicine; National Research Council. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar]
- Van Rossem, L.; Oenema, A.; Steegers, E.A.; Moll, H.A.; Jaddoe, V.W.; Hofman, A.; Mackenbach, J.P.; Raat, H. Are starting and continuing breastfeeding related to educational background? The generation R study. Pediatrics 2009, 123, e1017–e1027. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Spencer, P.M. Brief Symptom Inventory: BSI; Pearson: Upper Saddle River, NJ, USA, 1993. [Google Scholar]
- Erler, N.S.; Rizopoulos, D.; van Rosmalen, J.; Jaddoe, V.W.; Franco, O.H.; Lesaffre, E.M. Dealing with missing covariates in epidemiologic studies. A comparison between multiple imputation and a full Bayesian approach. Stat. Med. 2015. submitted. [Google Scholar]
- Cook, R.D. Detection of influential observation in linear regression. Technometrics 1977, 19, 15–18. [Google Scholar] [CrossRef]
- Timmermans, S.; Steegers-Theunissen, R.P.; Vujkovic, M.; den Breeijen, H.; Russcher, H.; Lindemans, J.; Mackenbach, J.; Hofman, A.; Lesaffre, E.E.; Jaddoe, V.V.; et al. The mediterranean diet and fetal size parameters: The generation R study. Br. J. Nutr. 2012, 108, 1399–1409. [Google Scholar] [CrossRef] [PubMed]
- Coolman, M.; de Groot, C.J.; Jaddoe, V.W.; Hofman, A.; Raat, H.; Steegers, E.A. Medical record validation of maternally reported history of preeclampsia. J. Clin. Epidemiol. 2010, 63, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Plummer, M. JAGS: A Program for Analysis of Bayesian Graphical Models Using Gibbs Sampling. In Proceedings of the 3rd International Workshop on Distributed Statistical Computing, Wien, Austria, 20–22 March 2003; Technische Universit at Wien: Wien, Austria, 2003; p. 125. [Google Scholar]
- Carmichael, S.; Abrams, B.; Selvin, S. The pattern of maternal weight gain in women with good pregnancy outcomes. Am. J. Public Health 1997, 87, 1984–1988. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Clapp, J.F., 3rd; Seaward, B.L.; Sleamaker, R.H.; Hiser, J. Maternal physiologic adaptations to early human pregnancy. Am. J. Obstet. Gynecol. 1988, 159, 1456–1460. [Google Scholar] [CrossRef]
- Kopp-Hoolihan, L.E.; van Loan, M.D.; Wong, W.W.; King, J.C. Fat mass deposition during pregnancy using a four-component model. J. Appl. Physiol. 1999, 87, 196–202. [Google Scholar] [PubMed]
- Forsum, E.; Sadurskis, A.; Wager, J. Resting metabolic rate and body composition of healthy Swedish women during pregnancy. Am. J. Clin. Nutr. 1988, 47, 942–947. [Google Scholar] [PubMed]
- Freisling, H.; van Bakel, M.M.; Biessy, C.; May, A.M.; Byrnes, G.; Norat, T.; Rinaldi, S.; de Magistris, M.S.; Grioni, S.; Bueno-de-Mesquita, H.B.; et al. Dietary reporting errors on 24 h recalls and dietary questionnaires are associated with BMI across six European countries as evaluated with recovery biomarkers for protein and potassium intake. Br. J. Nutr. 2012, 107, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Ellis, K.J.; Wong, W.W.; Hopkinson, J.M.; Smith, E.O. Composition of gestational weight gain impacts maternal fat retention and infant birth weight. Am. J. Obstet. Gynecol. 2003, 189, 1423–1432. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Olson, C.M.; Strawderman, M.S. Modifiable behavioral factors in a biopsychosocial model predict inadequate and excessive gestational weight gain. J. Am. Diet. Assoc. 2003, 103, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Kipnis, V.; Subar, A.F.; Midthune, D.; Freedman, L.S.; Ballard-Barbash, R.; Troiano, R.P.; Bingham, S.; Schoeller, D.A.; Schatzkin, A.; Carroll, R.J. Structure of dietary measurement error: Results of the open biomarker study. Am. J. Epidemiol. 2003, 158, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s dietary patterns change little from before to during pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Rad, N.T.; Ritterath, C.; Siegmund, T.; Wascher, C.; Siebert, G.; Henrich, W.; Buhling, K.J. Longitudinal analysis of changes in energy intake and macronutrient composition during pregnancy and 6 weeks post-partum. Arch. Gynecol. Obstet. 2011, 283, 185–190. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tielemans, M.J.; Erler, N.S.; Leermakers, E.T.M.; Van den Broek, M.; Jaddoe, V.W.V.; Steegers, E.A.P.; Kiefte-de Jong, J.C.; Franco, O.H. A Priori and a Posteriori Dietary Patterns during Pregnancy and Gestational Weight Gain: The Generation R Study. Nutrients 2015, 7, 9383-9399. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7115476
Tielemans MJ, Erler NS, Leermakers ETM, Van den Broek M, Jaddoe VWV, Steegers EAP, Kiefte-de Jong JC, Franco OH. A Priori and a Posteriori Dietary Patterns during Pregnancy and Gestational Weight Gain: The Generation R Study. Nutrients. 2015; 7(11):9383-9399. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7115476
Chicago/Turabian StyleTielemans, Myrte J., Nicole S. Erler, Elisabeth T. M. Leermakers, Marion Van den Broek, Vincent W. V. Jaddoe, Eric A. P. Steegers, Jessica C. Kiefte-de Jong, and Oscar H. Franco. 2015. "A Priori and a Posteriori Dietary Patterns during Pregnancy and Gestational Weight Gain: The Generation R Study" Nutrients 7, no. 11: 9383-9399. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7115476