Nutritional Solutions to Reduce Risks of Negative Health Impacts of Air Pollution

 , ,
, ,
Abstract
:1. Introduction
2. Characteristics of Air Pollution
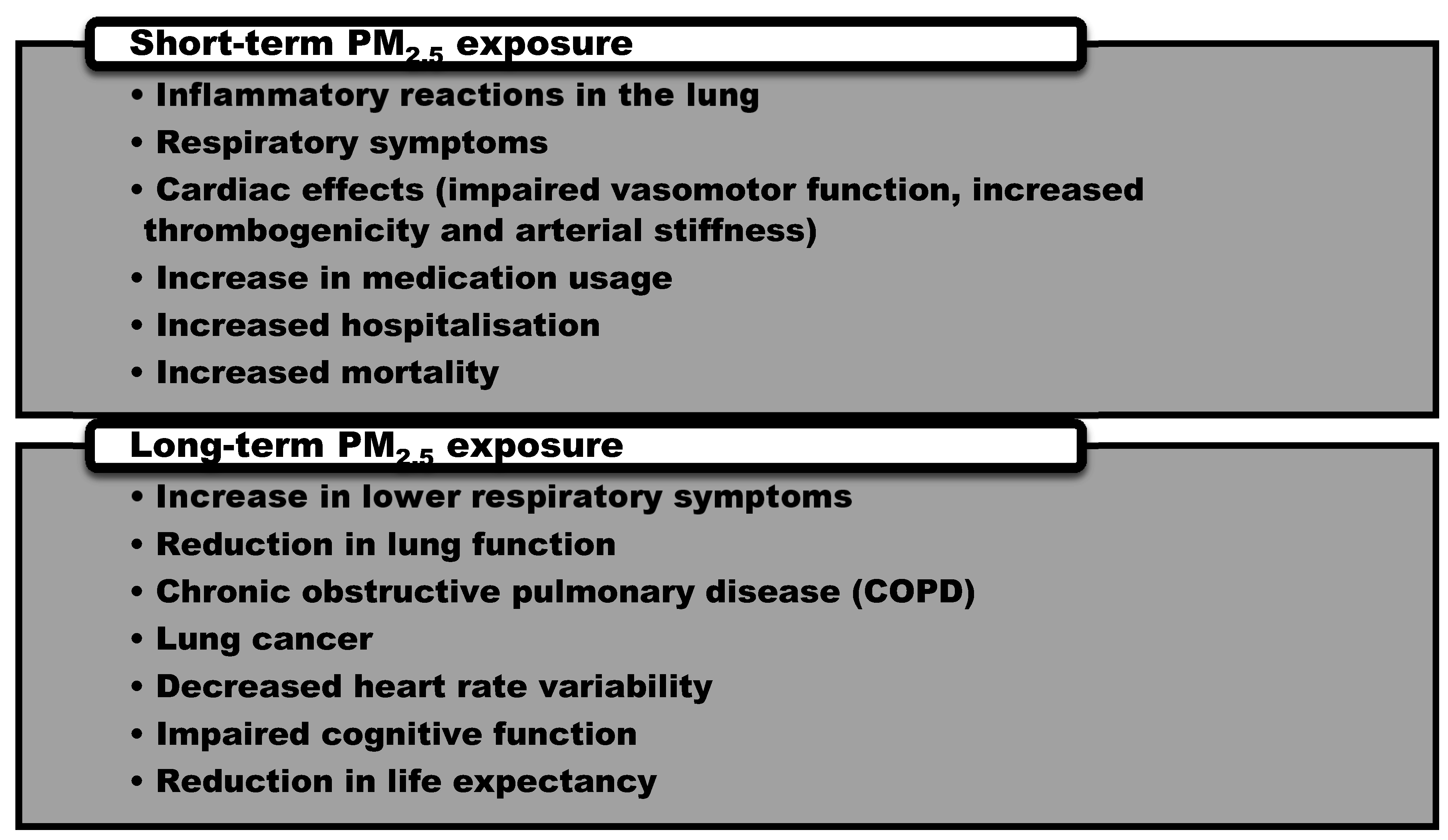
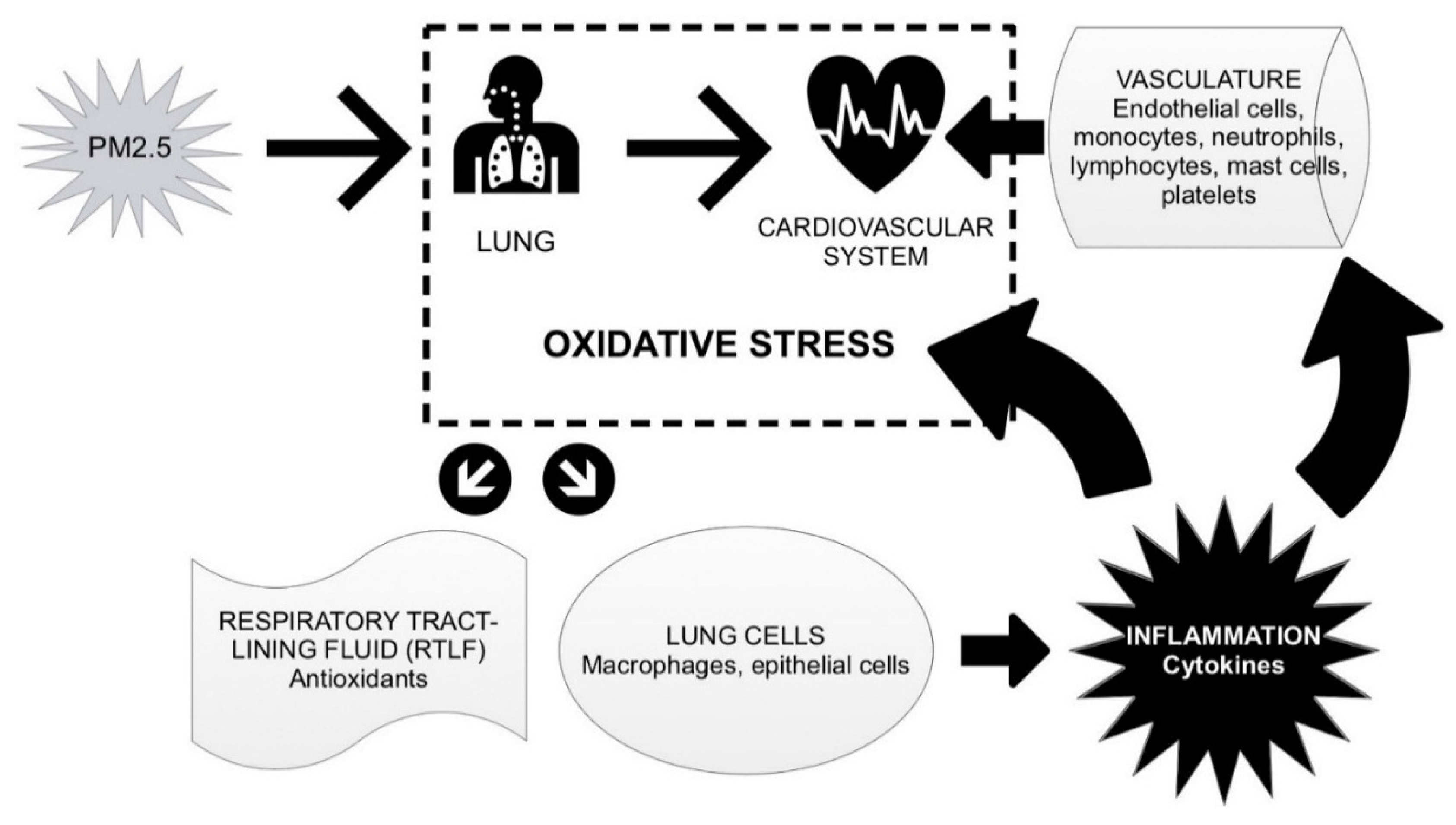
3. Impact of PM2.5 Exposure on Human Health


4. Effect of Nutrients on Air Pollution-Induced Health Damage

{kind=link}
{kind=link}
| Reference | Design | Population | Sample Size | Air Pollutant | Nutrient Intervention | Objectives | Main Outcome Measures | Interpretation |
|---|---|---|---|---|---|---|---|---|
| Mohsenin (1987) [60] | Randomized, double-blinded, placebo-controlled | Healthy adults | N = 11 | Nitrogen dioxide (NO2) | Vitamin C (4 × 500 mg/day) | To determine the effect of vitamin C on NO2-induced airway hyperresponsiveness in normal subjects | Lung mechanics and airway responsiveness to methacholine aerosol | Airway hyperresponsiveness induced by NO2 in normal subjects is completely prevented by pretreatment with ascorbic acid |
| Romieu et al. (1998) [61] | Randomized, double-blinded, placebo-controlled | Street workers | N = 47 | Ozone (O3) | Vitamin C (650 mg/day), Vitamin E (75 mg/day), β-carotene (15 mg/day) | To evaluate whether acute effects of ozone on lung functions could be attenuated by antioxidant vitamin supplementation | Pulmonary function tests | Supplementation above the recommended allowance provided additional protection against the acute effect of high ozone exposure on lung functions |
| Grievink et al. (1999) [62] | Randomized, double-blinded, placebo-controlled | Bicyclists | N = 38 | Ozone (O3) | Vitamin C (500 mg/day), Vitamin E (100 mg/day) | To investigate whether the acute effects of ozone on lung function could be modulated by antioxidant vitamin supplementation | Pulmonary function tests | Supplementation with the antioxidant vitamins C and E confers partial protection against the acute effects of ozone on FEV, and forced vital capacity in cyclists |
| Trenga et al. (2001) [63] | Double-blind crossover study | Adults with asthma | N = 17 | Ozone (O3) | Vitamin C (500 mg), Vitamin E (400 IU) | To evaluate the effects of dietary antioxidants on ozone-induced bronchial hyperresponsiveness in adult subjects with asthma | Pulmonary function tests | Dietary supplementation with vitamins E and C benefits asthmatic adults who are exposed to air pollutants |
| Romieu et al. (2002) [64] | Randomized, double-blinded, placebo-controlled | Children with asthma | N = 158 | Ozone (O3) | Vitamin C (250 mg/day), Vitamin E (50 mg/day) | To evaluate whether acute effects of ozone, nitrogen dioxide, and particulates with mass median diameter less than 10 µm could be attenuated by antioxidant vitamin supplementation | Pulmonary function tests | Supplementation with antioxidants modulated the impact of ozone exposure on the small airways of children with moderate to severe asthma |
| Sienra-Monge et al. (2004) [65] | Randomized, double-blinded, placebo-controlled | Children with asthma | N = 117 | Ozone (O3) | Vitamin C (250 mg/day), Vitamin E (50 mg/day) | To investigate the impact of antioxidant supplementation on the nasal inflammatory response to ozone exposure in atopic asthmatic children | Nasal lavage | Vitamin C and E supplementation above the minimum dietary requirement in asthmatic children with a low intake of vitamin E provided some protection against the nasal acute inflammatory response to ozone |
| Romieu et al. (2005) [8] | Randomized double-blinded | Nursing home residents older than 60 years | N = 50 | Particulate matter (PM) | Omega-3 fatty acid | To evaluate the effect of supplementation with omega-3 polyunsaturated fatty acids on the reduction of HRV associated with PM2.5 exposure | The association between HRV and 1 SD change in PM2.5 (8 µg/m3) | Supplementation with 2 g/day of fish oil prevented HRV decline related to PM2.5 exposure in the study population |
| Romieu et al. (2008) [66] | Randomized, double-blinded, controlled | Nursing home residents older than 60 years | N = 52 | Particulate matter (PM) | Omega-3 fatty acid (2 g fish oil/day) Soy oil | To evaluate whether n-3 PUFA supplementation could protect against the cardiac alterations linked to PM exposure | Cu/Zn SOD activity, LPO products, GSH | Supplementation with n-3 PUFA modulated the adverse effects of PM (2.5) |
| Riedl et al. (2009) [67] | Placebo-controlled dose escalation | Healthy nonsmokers ≥18 years of age | N = 65 | n/a | Oral sulforaphane doses contained in a standardized broccoli sprout homogenate | To investigate the in vivo effects of sulforaphane on the expression of glutathione-s-transferase M1 (GSTM1), glutathione-s-transferase P1 (GSTP1), NADPH quinone oxidoreductase (NQO1), and hemoxygenase-1 (HO-1) in the upper airway of human subjects | RNA expression for selected Phase II enzymes in nasal lavage cells | This study demonstrates the potential of antioxidant Phase II enzymes induction in the human airway as a strategy to reduce the inflammatory effects of oxidative stress |
| Possamai et al. (2010) [68] | Randomized, controlled | Subjects exposed to emissions from a coal electric-power plant | N = 80 | Particulate matter (PM) | Vitamin C (500 mg/day), Vitamin E (800 mg/day) | To better understand the relations between PM exposure derived from a coal electric-power plant and the oxidative damage in subjects directly or indirectly exposed to airborne contamination | Biomarkers of oxidative stress | Antioxidant intervention was able to confer a protective effect of vitamins C and E against the oxidative insult associated with airborne contamination derived from coal burning of an electric-power plant |
| Tong et al. (2012) [69] | Randomized, double-blinded, controlled | Healthy middle-aged adults | N = 29 | Particulate matter (PM) | Omega-3 fatty, acid (3 g fish oil/day), Olive oil (3 g/day) | To evaluate the efficacy of fish oil supplements in attenuating adverse cardiac effects of exposure to concentrated ambient fine and ultrafine particulate matter (CAP) | Heart rate variability (HRV) and electrocardiographic (ECG) repolarization changes. Plasma lipids changes | Omega-3 fatty acid supplements offer protection against the adverse cardiac and lipid effects associated with air pollution exposure |
| Heber et al. (2014) [70] | Controlled | Healthy subjects over age 18 | N = 29 | Diesel exhaust particle (DEP) | Sulforaphane (100 μmol) | To evaluate whether the administration of a standardized broccoli sprout extract could be used to suppress the nasal inflammatory response in human subjects challenged with 300 mg of an aqueous DEP suspension | White blood cell (WBC) counts | The study demonstrates the potential preventive and therapeutic potential of broccoli or broccoli sprouts rich in glucoraphanin for reducing the impact of particulate pollution on allergic disease and asthma |
| Egner et al. (2014) [71] | Randomized, placebo-controlled | Adults in good general health | N = 291 | n/a | Glucoraphanin (600 µmol), Sulforaphane (40 µmol) | To evaluate the magnitude and duration of pharmacodynamic action of a broccoli sprout-derived beverage | Urinary excretion of the mercapturic acids of the pollutants, benzene, acrolein, and crotonaldehyde | Intervention with broccoli sprouts enhances the detoxication of some airborne pollutants and may provide a frugal means to attenuate their associated long-term health risks |
5. The Asthma Case
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Kahn, R.; Levy, R.; Verduzco, C.; Villeneuve, P.J. Global Estimates of Ambient Fine Particulate Matter Concentrations from Satellite-Based Aerosol Optical Depth: Development and Application. Environ. Health Perspect. 2010, 118, 847–855. [Google Scholar] [CrossRef] [PubMed]
- WHO. Who Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Aphekom. Available online: http://www.Aphekom.Org/Web/Aphekom.Org/Home (accessed on 6 April 2015).
- Brook, R.D. Cardiovascular Effects of Air Pollution. Clin. Sci. 2008, 115, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Peters, A. Particulate Matter and Heart Disease: Evidence from Epidemiological Studies. Toxicol. Appl. Pharmacol. 2005, 207, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Castro-Giner, F.; Kunzli, N.; Sunyer, J. Air Pollution, Oxidative Stress and Dietary Supplementation: A Review. Eur. Respir. J. 2008, 31, 179–197. [Google Scholar] [CrossRef] [PubMed]
- Hennig, B.; Ettinger, A.S.; Jandacek, R.J.; Koo, S.; Mcclain, C.; Seifried, H.; Silverstone, A.; Watkins, B.; Suk, W.A. Using Nutrition for Intervention and Prevention Against Environmental Chemical Toxicity and Associated Diseases. Environ. Health Perspect. 2007, 115, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Tellez-Rojo, M.M.; Lazo, M.; Manzano-Patino, A.; Cortez-Lugo, M.; Julien, P.; Belanger, M.C.; Hernandez-Avila, M.; Holguin, F. Omega-3 Fatty Acid Prevents Heart Rate Variability Reductions Associated with Particulate Matter. Am. J. Respir. Crit. Care Med. 2005, 172, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Mudway, I.; Blomberg, A.; Frew, A.; Sandstrom, T. Altered Lung Antioxidant Status in Patients with Mild Asthma. Lancet 1999, 354, 482–483. [Google Scholar] [CrossRef]
- Wood, L.G.; Gibson, P.G.; Garg, M.L. Biomarkers of Lipid Peroxidation, Airway Inflammation and Asthma. Eur. Respir. J. 2003, 21, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Garg, M.L.; Smart, J.M.; Scott, H.A.; Barker, D.; Gibson, P.G. Manipulating Antioxidant Intake in Asthma: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2012, 96, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Su, J.G.; Apte, J.S.; Lipsitt, J.; Garcia-Gonzales, D.A.; Beckerman, B.S.; de Nazelle, A.; Texcalac-Sangrador, J.L.; Jerrett, M. Populations Potentially Exposed to Traffic-Related Air Pollution in Seven World Cities. Environ. Int. 2015, 78, 82–89. [Google Scholar] [CrossRef] [PubMed]
- USEP. National Ambient Air Quality Standards (Naaqs). Available online: http://www.Epa.Gov/Air/Criteria.Html (accessed on 13 November 2015).
- AGDOT. National Standards for Criteria Air Pollutants in Australia. Available online: http://www.Environment.Gov.Au/Protection/Publications/Factsheet-National-Standards-Criteria-Air-Pollutants-Australia (accessed on 16 November 2015).
- Sampson, P.D.; Richards, M.; Szpiro, A.A.; Bergen, S.; Sheppard, L.; Larson, T.V.; Kaufman, J.D. A Regionalized National Universal Kriging Model Using Partial Least Squares Regression for Estimating Annual Pm Concentrations in Epidemiology. Atmos. Environ. 2013, 75, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Novotny, E.V.; Bechle, M.J.; Millet, D.B.; Marshall, J.D. National Satellite-Based Land-Use Regression: NO2 in the United States. Environ. Sci. Technol. 2011, 45, 4407–4414. [Google Scholar] [CrossRef] [PubMed]
- Clougherty, J.E.; Kheirbek, I.; Eisl, H.M.; Ross, Z.; Pezeshki, G.; Gorczynski, J.E.; Johnson, S.; Markowitz, S.; Kass, D.; Matte, T. Intra-Urban Spatial Variability in Wintertime Street-Level Concentrations of Multiple Combustion-Related Air Pollutants: The New York City Community Air Survey (Nyccas). J. Expo. Sci. Environ. Epidemiol. 2013, 23, 232–240. [Google Scholar] [CrossRef] [PubMed]
- De Hoogh, K.; Wang, M.; Adam, M.; Badaloni, C.; Beelen, R.; Birk, M.; Cesaroni, G.; Cirach, M.; Declercq, C.; Dedele, A.; et al. Development of Land Use Regression Models for Particle Composition in Twenty Study Areas in Europe. Environ. Sci. Technol. 2013, 47, 5778–5786. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.I.; Clougherty, J.E.; Baxter, L.K.; Houseman, E.A.; Paciorek, C.J. Evaluating Heterogeneity in Indoor and Outdoor Air Pollution Using Land-Use Regression and Constrained Factor Analysis. Res. Rep. 2010, 5–91. [Google Scholar]
- Nel, A.E.; Diaz-Sanchez, D.; Li, N. The Role of Particulate Pollutants in Pulmonary Inflammation and Asthma: Evidence for the Involvement of Organic Chemicals and Oxidative Stress. Curr. Opin. Pulm. Med. 2001, 7, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Schauer, J.J.; Lough, G.C.; Shafer, M.M.; Christensen, W.F.; Arndt, M.F.; Deminter, J.T.; Park, J.S. Characterization of Metals Emitted from Motor Vehicles. Res. Rep. 2006, 133, 1–88. [Google Scholar]
- Lanki, T.; de Hartog, J.J.; Heinrich, J.; Hoek, G.; Janssen, N.A.; Peters, A.; Stolzel, M.; Timonen, K.L.; Vallius, M.; Vanninen, E.; et al. Can We Identify Sources of Fine Particles Responsible for Exercise-Induced Ischemia on Days with Elevated Air Pollution? The Ultra Study. Environ. Health Perspect. 2006, 114, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Clougherty Je, K.I.; Johnson, S.; Pezeshki, G.; Jacobson, J.B.; Eisl, H.; Gorczynski, J.; Ross, Z.; Kitson, H.; Benson, A.; Camacho, A.; et al. The New York City Community Air Survey Supplemental Report: Nickel Concentrations in Ambient Fine Particles: Winter Monitoring, 2008–2009; New York City Department of Health and Mental Hygiene, and Nyc Mayor’s Office for Long-Term Planning and Sustainability: New York, NY, USA, 2010. [Google Scholar]
- Krewski, D.B.R.; Goldberg, M.S.; Hoover, K.; Siemiatycki, J.; Jerrett, M. Reanalysis of the Harvard Six Cities Study and the American Cancer Society Study of Particulate Air Pollution and Mortality; Health Effects Institute (Hei): Cambridge, MA, USA, 2000. [Google Scholar]
- Jerrett, M.; Burnett, R.T.; Brook, J.; Kanaroglou, P.; Giovis, C.; Finkelstein, N.; Hutchison, B. Do Socioeconomic Characteristics Modify the Short Term Association between Air Pollution and Mortality? Evidence from A Zonal Time Series in Hamilton, Canada. J. Epidemiol. Commun. Health 2004, 58, 31–40. [Google Scholar] [CrossRef]
- Shmool, J.L.; Kubzansky, L.D.; Newman, O.D.; Spengler, J.; Shepard, P.; Clougherty, J.E. Social Stressors and Air Pollution Across New York City Communities: A Spatial Approach for Assessing Correlations Among Multiple Exposures. Environ. Health A Glob. Access Sci. Sour. 2014, 13, 91. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., 3rd; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate Matter Air Pollution and Cardiovascular Disease: An Update to the Scientific Statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R. The Role of Oxidative Stress in the Cardiovascular Actions of Particulate Air Pollution. Biochem. Soc. Trans. 2014, 42, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; O’neill, M.S.; Wright, R.O.; Hu, H.; Vokonas, P.S.; Sparrow, D.; Suh, H.; Schwartz, J. Hfe Genotype, Particulate Air Pollution, and Heart Rate Variability: A Gene-Environment Interaction. Circulation 2006, 114, 2798–2805. [Google Scholar] [CrossRef] [PubMed]
- Oftedal, B.; Brunekreef, B.; Nystad, W.; Madsen, C.; Walker, S.E.; Nafstad, P. Residential Outdoor Air Pollution and Lung Function in Schoolchildren. Epidemiology 2008, 19, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Martinez, R.; Perez-Padilla, R.; Olaiz-Fernandez, G.; Mendoza-Alvarado, L.; Moreno-Macias, H.; Fortoul, T.; Mcdonnell, W.; Loomis, D.; Romieu, I. Lung Function Growth in Children with Long-Term Exposure to Air Pollutants in Mexico City. Am. J. Respir. Crit. Care Med. 2007, 176, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., 3rd; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung Cancer, Cardiopulmonary Mortality, and Long-Term Exposure to Fine Particulate Air Pollution. Jama J. Am. Med. Assoc. 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air Pollution and Lung Cancer Incidence in 17 European Cohorts: Prospective Analyses from the European Study of Cohorts for Air Pollution Effects (Escape). Lancet. Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Ranft, U.; Schikowski, T.; Sugiri, D.; Krutmann, J.; Kramer, U. Long-Term Exposure to Traffic-Related Particulate Matter Impairs Cognitive Function in the Elderly. Environ. Res. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Brunekreef, B.; Goldbohm, S.; Fischer, P.; Van Den Brandt, P.A. Association Between Mortality and Indicators of Traffic-Related Air Pollution in the Netherlands: A Cohort Study. Lancet 2002, 360, 1203–1209. [Google Scholar] [CrossRef]
- Pope, C.A., 3rd; Burnett, R.T.; Turner, M.C.; Cohen, A.; Krewski, D.; Jerrett, M.; Gapstur, S.M.; Thun, M.J. Lung Cancer and Cardiovascular Disease Mortality Associated with Ambient Air Pollution and Cigarette Smoke: Shape of the Exposure-Response Relationships. Environ. Health Perspect. 2011, 119, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Haryanto, B.; Suksmasari, T.; Wintergerst, E.; Maggini, S. Multivitamin Supplementation Supports Immune Function and Ameliorates Conditions Triggered By Reduced Air Quality. Vitam. Miner. 2015, 4. [Google Scholar] [CrossRef]
- Zeka, A.; Sullivan, J.R.; Vokonas, P.S.; Sparrow, D.; Schwartz, J. Inflammatory Markers and Particulate Air Pollution: Characterizing the Pathway to Disease. Int. J. Epidemiol. 2006, 35, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, T. Role of Oxygen Radicals on Bronchial Asthma. Curr. Drug Targets Inflam. Allergy 2005, 4, 505–509. [Google Scholar] [CrossRef]
- Kelly, F.J.; Fussell, J.C. Linking Ambient Particulate Matter Pollution Effects with Oxidative Biology and Immune Responses. Ann. N. Y. Acad. Sci. 2015, 1340, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Holguin, F.; Tellez-Rojo, M.M.; Hernandez, M.; Cortez, M.; Chow, J.C.; Watson, J.G.; Mannino, D.; Romieu, I. Air Pollution and Heart Rate Variability Among the Elderly in Mexico City. Epidemiology 2003, 14, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Sarnat, J.A.; Holguin, F. Asthma and Air Quality. Curr. Opin. Pulm. Med. 2007, 13, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Fussell, J.C. Air Pollution and Airway Disease. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2011, 41, 1059–1071. [Google Scholar] [CrossRef] [PubMed]
- Ko, F.W.; Hui, D.S. Air Pollution and Chronic Obstructive Pulmonary Disease. Respirology 2012, 17, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Kunzli, N.; Jerrett, M.; Garcia-Esteban, R.; Basagana, X.; Beckermann, B.; Gilliland, F.; Medina, M.; Peters, J.; Hodis, H.N.; Mack, W.J. Ambient Air Pollution and the Progression of Atherosclerosis in Adults. PLos ONE 2010. [Google Scholar] [CrossRef]
- Kunzli, N.; Jerrett, M.; Mack, W.J.; Beckerman, B.; Labree, L.; Gilliland, F.; Thomas, D.; Peters, J.; Hodis, H.N. Ambient Air Pollution and Atherosclerosis in Los Angeles. Environ. Health Perspect. 2005, 113, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; Mcconnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E.; et al. The Effect of Air Pollution on Lung Development from 10 to 18 Years of Age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Mccreanor, J.; Cullinan, P.; Nieuwenhuijsen, M.J.; Stewart-Evans, J.; Malliarou, E.; Jarup, L.; Harrington, R.; Svartengren, M.; Han, I.K.; Ohman-Strickland, P.; et al. Respiratory Effects of Exposure to Diesel Traffic in Persons with Asthma. N. Engl. J. Med. 2007, 357, 2348–2358. [Google Scholar] [CrossRef] [PubMed]
- Mcconnell, R.; Berhane, K.; Yao, L.; Jerrett, M.; Lurmann, F.; Gilliland, F.; Kunzli, N.; Gauderman, J.; Avol, E.; Thomas, D.; et al. Traffic, Susceptibility, and Childhood Asthma. Environ. Health Perspect. 2006, 114, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Holguin, F.; Flores, S.; Ross, Z.; Cortez, M.; Molina, M.; Molina, L.; Rincon, C.; Jerrett, M.; Berhane, K.; Granados, A.; et al. Traffic-Related Exposures, Airway Function, Inflammation, and Respiratory Symptoms in Children. Am. J. Respir. Crit. Care Med. 2007, 176, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; von Klot, S.; Heier, M.; Trentinaglia, I.; Hormann, A.; Wichmann, H.E.; Lowel, H.; Cooperative Health Research in the Region of Augsburg Study Group. Exposure to Traffic and the Onset of Myocardial Infarction. N. Engl. J. Med. 2004, 351, 1721–1730. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.S.; Powell, K.E.; Hutwagner, L.; Graham, L.M.; Teague, W.G. Impact of Changes in Transportation and Commuting Behaviors During the 1996 Summer Olympic Games in Atlanta on Air Quality and Childhood Asthma. Jama 2001, 285, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Mu, L.; Deng, F.; Tian, L.; Li, Y.; Swanson, M.; Ying, J.; Browne, R.W.; Rittenhouse-Olson, K.; Zhang, J.J.; Zhang, Z.F.; et al. Peak Expiratory Flow, Breath Rate and Blood Pressure in Adults with Changes in Particulate Matter Air Pollution During the Beijing Olympics: A Panel Study. Environ. Res. 2014, 133, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhu, T.; Kipen, H.; Wang, G.; Huang, W.; Rich, D.; Zhu, P.; Wang, Y.; Lu, S.E.; Ohman-Strickland, P.; et al. Cardiorespiratory Biomarker Responses in Healthy Young Adults to Drastic Air Quality Changes Surrounding the 2008 Beijing Olympics. Res. Rep. 2013, 174, 5–174. [Google Scholar]
- Chiuve, S.E.; Sampson, L.; Willett, W.C. The Association Between A Nutritional Quality Index and Risk of Chronic Disease. Am. J. Prev. Med. 2011, 40, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Hoeft, B.; Weber, P.; Eggersdorfer, M. Micronutrients—A Global Perspective on Intake, Health Benefits and Economics. Int. J. Vitam. Nutr. Res. 2012, 82, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Landete, J.M. Dietary Intake of Natural Antioxidants: Vitamins and Polyphenols. Crit. Rev. Food Sci. Nutr. 2013, 53, 706–721. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Sung, B.; Aggarwal, B.B. Age-Associated Chronic Diseases Require Age-Old Medicine: Role of Chronic Inflammation. Prevent. Med. 2012, 54, S29–S37. [Google Scholar] [CrossRef] [PubMed]
- Poljsak, B.; Fink, R. The Protective Role of Antioxidants in the Defence Against Ros/Rns-Mediated Environmental Pollution. Oxid. Med. Cell. Longev. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Mohsenin, V. Effect of Vitamin C on No2-Induced Airway Hyperresponsiveness in Normal Subjects. A Randomized Double-Blind Experiment. Am. Rev. Respir. Dis. 1987, 136, 1408–1411. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Meneses, F.; Ramirez, M.; Ruiz, S.; Perez Padilla, R.; Sienra, J.J.; Gerber, M.; Grievink, L.; Dekker, R.; Walda, I.; et al. Antioxidant Supplementation and Respiratory Functions Among Workers Exposed to High Levels of Ozone. Am. J. Respir. Crit. Care Med. 1998, 158, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Grievink, L.; Zijlstra, A.G.; Ke, X.; Brunekreef, B. Double-Blind Intervention Trial on Modulation of Ozone Effects on Pulmonary Function By Antioxidant Supplements. Am. J. Epidemiol. 1999, 149, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Trenga, C.A.; Koenig, J.Q.; Williams, P.V. Dietary Antioxidants and Ozone-Induced Bronchial Hyperresponsiveness in Adults with Asthma. Arch. Environ. Health 2001, 56, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Sienra-Monge, J.J.; Ramirez-Aguilar, M.; Tellez-Rojo, M.M.; Moreno-Macias, H.; Reyes-Ruiz, N.I.; Del Rio-Navarro, B.E.; Ruiz-Navarro, M.X.; Hatch, G.; Slade, R.; et al. Antioxidant Supplementation and Lung Functions Among Children with Asthma Exposed to High Levels of Air Pollutants. Am. J. Respir. Crit. Care Med. 2002, 166, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Sienra-Monge, J.J.; Ramirez-Aguilar, M.; Moreno-Macias, H.; Reyes-Ruiz, N.I.; Del Rio-Navarro, B.E.; Ruiz-Navarro, M.X.; Hatch, G.; Crissman, K.; Slade, R.; Devlin, R.B.; et al. Antioxidant Supplementation and Nasal Inflammatory Responses Among Young Asthmatics Exposed to High Levels of Ozone. Clin. Exp. Immunol. 2004, 138, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Garcia-Esteban, R.; Sunyer, J.; Rios, C.; Alcaraz-Zubeldia, M.; Velasco, S.R.; Holguin, F. The Effect of Supplementation with Omega-3 Polyunsaturated Fatty Acids on Markers of Oxidative Stress in Elderly Exposed to Pm (2.5). Environ. Health Perspect. 2008, 116, 1237–1242. [Google Scholar] [CrossRef] [PubMed]
- Riedl, M.A.; Saxon, A.; Diaz-Sanchez, D. Oral Sulforaphane Increases Phase Ii Antioxidant Enzymes in the Human Upper Airway. Clin. Immunol. 2009, 130, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Possamai, F.P.; Junior, S.A.; Parisotto, E.B.; Moratelli, A.M.; Inacio, D.B.; Garlet, T.R.; dal-Pizzol, F.; Filho, D.W. Antioxidant Intervention Compensates Oxidative Stress in Blood of Subjects Exposed to Emissions from A Coal Electric-Power Plant in South Brazil. Environ. Toxicol Pharmacol. 2010, 30, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.; Rappold, A.G.; Diaz-Sanchez, D.; Steck, S.E.; Berntsen, J.; Cascio, W.E.; Devlin, R.B.; Samet, J.M. Omega-3 Fatty Acid Supplementation Appears to Attenuate Particulate Air Pollution-Induced Cardiac Effects and Lipid Changes in Healthy Middle-Aged Adults. Environ. Health Perspect. 2012, 120, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Heber, D.; Li, Z.; Garcia-Lloret, M.; Wong, A.M.; Lee, T.Y.; Thames, G.; Krak, M.; Zhang, Y.; Nel, A. Sulforaphane-Rich Broccoli Sprout Extract Attenuates Nasal Allergic Response to Diesel Exhaust Particles. Food Funct. 2014, 5, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Egner, P.A.; Chen, J.G.; Zarth, A.T.; Ng, D.; Wang, J.; Kensler, K.H.; Jacobson, L.P.; Munoz, A.; Johnson, J.L.; Groopman, J.D.; et al. Rapid and Sustainable Detoxication of Airborne Pollutants By Broccoli Sprout Beverage: Results of A Randomized Clinical Trial in China. Cancer Prev. Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V.; Mehra, M.R.; Ventura, H.O. Omega-3 Polyunsaturated Fatty Acids and Cardiovascular Diseases. J. Am. Coll. Cardiol. 2009, 54, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Kris-Etherton, P.M.; Harris, K.A. Intakes of Long-Chain Omega-3 Fatty Acid Associated with Reduced Risk for Death from Coronary Heart Disease in Healthy Adults. Curr. Atheroscler. Rep. 2008, 10, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Geelen, A.; Brouwer, I.A.; Geleijnse, J.M.; Zock, P.L.; Katan, M.B. Effect of Fish Oil on Heart Rate in Humans: A Meta-Analysis of Randomized Controlled Trials. Circulation 2005, 112, 1945–1952. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Mudway, I.S. Protein Oxidation At the Air-Lung Interface. Amino Acids 2003, 25, 375–396. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J. Dietary Antioxidants and Environmental Stress. Proc. Nutr. Soc. 2004, 63, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Fiorito, G.; Guarrera, S.; Valle, C.; Ricceri, F.; Russo, A.; Grioni, S.; Mattiello, A.; di Gaetano, C.; Rosa, F.; Modica, F.; et al. B-Vitamins Intake, Dna-Methylation of One Carbon Metabolism and Homocysteine Pathway Genes and Myocardial Infarction Risk: The Epicor Study. Nutr. Metab. Cardiovasc. Dis. Nmcd 2014, 24, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Abbenhardt, C.; Miller, J.W.; Song, X.; Brown, E.C.; Cheng, T.Y.; Wener, M.H.; Zheng, Y.; Toriola, A.T.; Neuhouser, M.L.; Beresford, S.A.; et al. Biomarkers of One-Carbon Metabolism Are Associated with Biomarkers of Inflammation in Women. J. Nutr. 2014, 144, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Baccarelli, A.; Cassano, P.A.; Litonjua, A.; Park, S.K.; Suh, H.; Sparrow, D.; Vokonas, P.; Schwartz, J. Cardiac Autonomic Dysfunction: Effects from Particulate Air Pollution and Protection By Dietary Methyl Nutrients and Metabolic Polymorphisms. Circulation 2008, 117, 1802–1809. [Google Scholar] [CrossRef] [PubMed]
- Manicourt, D.H.; Devogelaer, J.P. Urban Tropospheric Ozone Increases the Prevalence of Vitamin D Deficiency Among Belgian Postmenopausal Women with Outdoor Activities During Summer. J. Clin. Endocrinol. Metab. 2008, 93, 3893–3899. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, K.S.; Mughal, M.Z.; Upadhyay, P.; Berry, J.L.; Mawer, E.B.; Puliyel, J.M. The Impact of Atmospheric Pollution on Vitamin D Status of Infants and Toddlers in Delhi, India. Arch. Dis. Child. 2002, 87, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpanah, F.; Pour, S.H.; Heibatollahi, M.; Moghbel, N.; Asefzade, S.; Azizi, F. The Effects of Air Pollution on Vitamin D Status in Healthy Women: A Cross Sectional Study. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency in 2010: Health Benefits of Vitamin D and Sunlight: A D-Bate. Nat. Rev. Endocrinol. 2011, 7, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Albanes, D.; Heinonen, O.P.; Taylor, P.R.; Virtamo, J.; Edwards, B.K.; Rautalahti, M.; Hartman, A.M.; Palmgren, J.; Freedman, L.S.; Haapakoski, J.; et al. Alpha-Tocopherol and Beta-Carotene Supplements and Lung Cancer Incidence in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study: Effects of Base-Line Characteristics and Study Compliance. J. Natl. Cancer Inst. 1996, 88, 1560–1570. [Google Scholar] [CrossRef] [PubMed]
- Omenn, G.S.; Goodman, G.E.; Thornquist, M.D.; Balmes, J.; Cullen, M.R.; Glass, A.; Keogh, J.P.; Meyskens, F.L., Jr.; Valanis, B.; Williams, J.H., Jr.; et al. Risk Factors for Lung Cancer and for Intervention Effects in Caret, the Beta-Carotene and Retinol Efficacy Trial. J. Natl. Cancer Inst. 1996, 88, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Virtamo, J.; Pietinen, P.; Huttunen, J.K.; Korhonen, P.; Malila, N.; Virtanen, M.J.; Albanes, D.; Taylor, P.R.; Albert, P.; Group, A.S. Incidence of Cancer and Mortality Following Alpha-Tocopherol and Beta-Carotene Supplementation: A Postintervention Follow-Up. Jama 2003, 290, 476–485. [Google Scholar] [PubMed]
- Blaylock, R.L. Methodological Problems with Population Cancer Studies: The Forgotten Confounding Factors. Surg. Neurol. Int. 2015. [Google Scholar] [CrossRef] [PubMed]
- Masoli, M.; Fabian, D.; Holt, S.; Beasley, R. Global Initiative for Asthma (Gina) Program. The Global Burden of Asthma: Executive Summary of the Gina Dissemination Committee Report. Allergy 2004, 59, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Baines, K.J.; Fu, J.; Scott, H.A.; Gibson, P.G. The Neutrophilic Inflammatory Phenotype Is Associated with Systemic Inflammation in Asthma. Chest 2012, 142, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.P.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations: Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef] [PubMed]
- European Respiratory Society. Ers White Book. Available online: http://www.Erswhitebook.Org/Chapters/Outdoor-Environment/ (accessed on 8 October 2015).
- Troesch, B.; Hoeft, B.; Mcburney, M.; Eggersdorfer, M.; Weber, P. Dietary Surveys Indicate Vitamin Intakes Below Recommendations Are Common in Representative Western Countries. Br. J. Nutr. 2012, 108, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Garg, M.L.; Simpson, J.L.; Mori, T.A.; Croft, K.D.; Wark, P.A.; Gibson, P.G. Induced Sputum 8-Isoprostane Concentrations in Inflammatory Airway Diseases. Am. J. Respir. Crit. Care Med. 2005, 171, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Garg, M.L.; Blake, R.J.; Garcia-Caraballo, S.; Gibson, P.G. Airway and Circulating Levels of Carotenoids in Asthma and Healthy Controls. J. Am. Coll. Nutr. 2005, 24, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Garg, M.L.; Blake, R.J.; Simpson, J.L.; Gibson, P.G. Oxidized Vitamin E and Glutathione As Markers of Clinical Status in Asthma. Clin. Nutr. 2008, 27, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Garg, M.L.; Powell, H.; Gibson, P.G. Lycopene-Rich Treatments Modify Noneosinophilic Airway Inflammation in Asthma: Proof of Concept. Free Radic. Res. 2008, 42, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.; Hart, A.; Milan, S.J.; Sugumar, K. Vitamins C and E for Asthma and Exercise-Induced Bronchoconstriction. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Saedisomeolia, A.; Wood, L.G.; Garg, M.L.; Gibson, P.G.; Wark, P.A. Anti-Inflammatory Effects of Long-Chain N-3 Pufa in Rhinovirus-Infected Cultured Airway Epithelial Cells. Br. J. Nutr. 2009, 101, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Hazlewood, L.C.; Foster, P.S.; Hansbro, P.M. Lyprinol Reduces Inflammation and Improves Lung Function in A Mouse Model of Allergic Airways Disease. Clin. Exp. Allergy 2010, 40, 1785–1793. [Google Scholar] [CrossRef] [PubMed]
- Thien, F.C.; Woods, R.K.; Abramson, M.J. Dietary Marine Fatty Acids (Fish Oil) for Asthma in Adults and Children (Cochrane Review). Cochrane Librar. 2004. [Google Scholar] [CrossRef]
- Saedisomeolia, A.; Wood, L.G.; Garg, M.L.; Gibson, P.G.; Wark, P.A.B. Supplementation of Long Chain N-3 Polyunsaturated Fatty Acids Increases Utilisation of Lycopene in Cultured Airway Epithelial Cells. J. Food Lipids 2008, 15, 421–432. [Google Scholar] [CrossRef]
- Castro, M.; King, T.S.; Kunselman, S.J.; Cabana, M.D.; Denlinger, L.; Holguin, F.; Kazani, S.D.; Moore, W.C.; Moy, J.; Sorkness, C.A.; et al. Effect of Vitamin D3 on Asthma Treatment Failures in Adults with Symptomatic Asthma and Lower Vitamin D Levels: The Vida Randomized Clinical Trial. Jama 2014, 311, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Péter, S.; Holguin, F.; Wood, L.G.; Clougherty, J.E.; Raederstorff, D.; Antal, M.; Weber, P.; Eggersdorfer, M. Nutritional Solutions to Reduce Risks of Negative Health Impacts of Air Pollution. Nutrients 2015, 7, 10398-10416. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7125539
Péter S, Holguin F, Wood LG, Clougherty JE, Raederstorff D, Antal M, Weber P, Eggersdorfer M. Nutritional Solutions to Reduce Risks of Negative Health Impacts of Air Pollution. Nutrients. 2015; 7(12):10398-10416. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7125539
Chicago/Turabian StylePéter, Szabolcs, Fernando Holguin, Lisa G. Wood, Jane E. Clougherty, Daniel Raederstorff, Magda Antal, Peter Weber, and Manfred Eggersdorfer. 2015. "Nutritional Solutions to Reduce Risks of Negative Health Impacts of Air Pollution" Nutrients 7, no. 12: 10398-10416. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7125539