The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Goals
1.2. Specific Goals
- To determine total energy intake in the Spanish population aged 9–75 years, and its distribution by age group and sex.
- To determine total energy expenditure in the Spanish population aged 9–75 years, stratified by age group and sex.
- To analyze the main food groups and subgroups contributing to energy intake and differences by age group and sex.
- To evaluate different anthropometric measurements of special interest for the energy balance hypothesis.
- To describe the perception and understanding of different items in relation to EB for the Spanish population.
2. Experimental Section
2.1. Pilot Studies
2.2. Study Design and Sampling Procedure

{kind=link}
{kind=link}
{kind=link}
| Base | Sample (n) | |||
|---|---|---|---|---|
| Initial targeted Sample | Final Sample | Final + Boost | ||
| 2634 | 2009 | 2285 | ||
| sex | Men | 1309 | 1013 | 1160 |
| Women | 1325 | 996 | 1125 | |
| age (years) | Infants 9–12 | 240 | 100 | 213 |
| Adolescents 13–17 | 246 | 124 | 211 | |
| Adults 18–64 | 1911 | 1588 | 1655 | |
| Elderly 65–75 | 237 | 197 | 206 | |
- -
- Age groups (in years): 9–12, 13–17, 18–64 and 65–75.
- -
- Gender: men and women.
- -
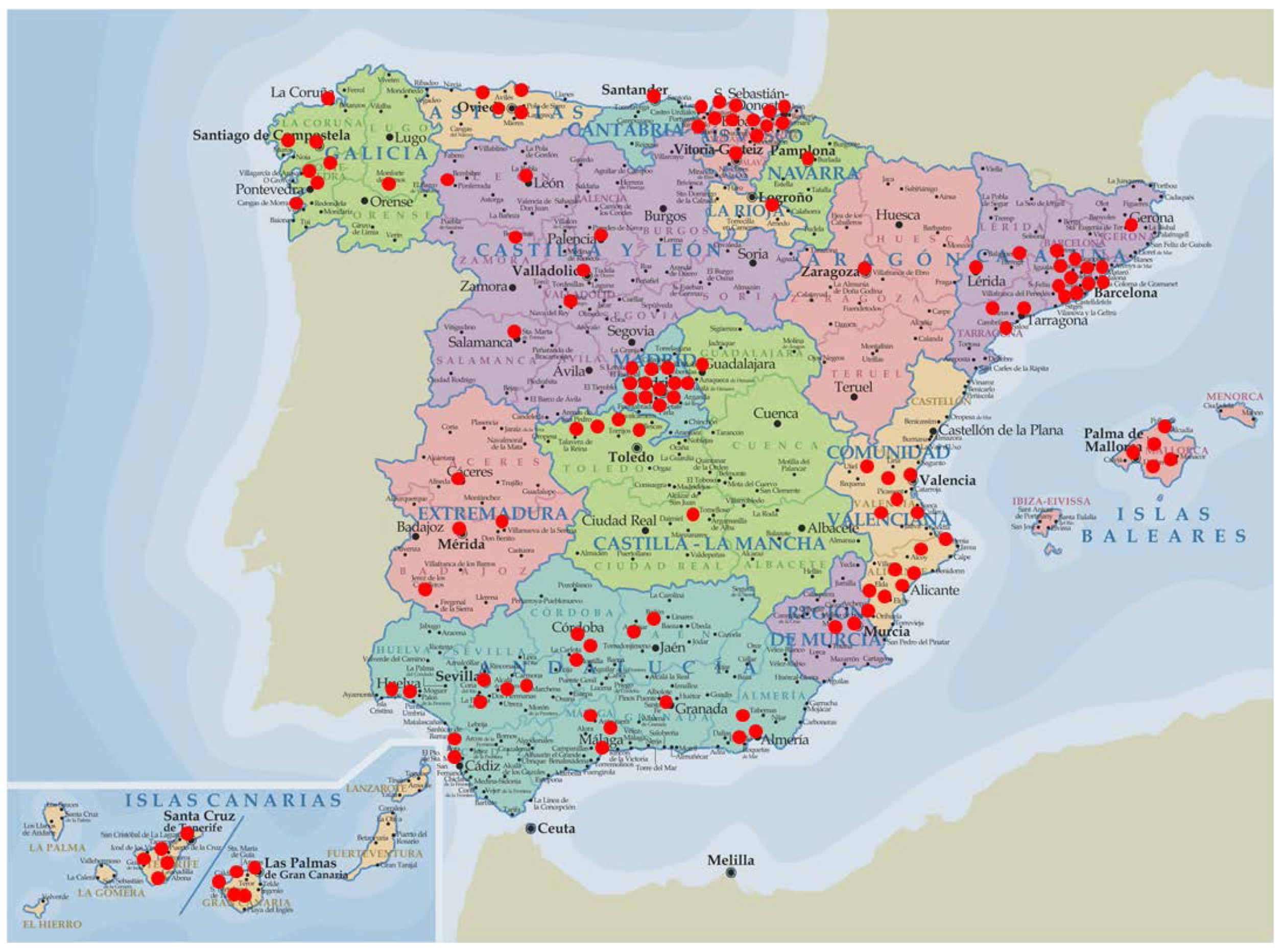
- Region: seven Nielsen areas (Northeast, Levant, South, West, North Central, Barcelona, Madrid) and Canary Islands.
- -
- Habitat size: 2000 to 30,000 inhabitants (rural population); from 30,000 to 200,000 inhabitants (semi-urban population) and over 200,000 inhabitants (city/town population).
- -
- Other factors that were considered: rate of unemployment; % of foreigners (immigrant population), level of physical activity, and education/economical level.

2.3. Final Fieldwork
- 1–10 units, only one potential participant.
- 11–20 units, two potential participants as maximum.
- 21–50 units, three potential participants maximum.
- >50 units, four participants.
2.4. Stages
2.4.1. Stage 1: The Interviewer Visits

- (a)
- Identification of the trained interviewer, as a collaborator of the FEN. The interviewer explained the main goals of the study, the design and stages, the novelty of the tools to be used for collecting food intake and recording physical activity, as well as offered to have a feedback report at the end of the study that included main results, dietary and physical activity advice, etc. The potential participant also received a letter from the principal investigator of the ANIBES Study, and was informed about the stipend for participation in the study. At this point, the potential participant was asked to sign the letter of consent for participation in the study.
- (b)
- Inclusion/exclusion questionnaire: the interviewer verified through a filter questionnaire that the participant was eligible for the ANIBES Study. Several exclusion criteria were applied:
- Those individuals living in an institution (e.g., colleges; nursing homes, hospitals, etc.)
- Individuals following a therapeutic diet due to a recent surgery or any medical prescription.
- If they were suffering a transitory pathology (i.e., flu, gastroenteritis, chicken pox, etc.) at the time of the fieldwork.
- Individuals employed in areas related to consumer science, marketing or the media.
- Those following dietary advice such as for prevention of hypertension, diabetes, hypercholesterolemia or hyperuricemia.
- Pregnant and lactating women.
- With diagnosed allergy and/or food intolerance.
- Suffering a metabolic disease such as hyperthyroidism or hypothyroidism.
- (c)
- Anthropometric measurements: the trained interviewer collected the different measures following the procedures tested before at the two pilot studies:
- Height: by triplicate using a Stadiometer model Seca 206 (Seca, Hamburg, Germany).
- Weight: one determination in a weighing scale model Seca 804 (Seca, Hamburg, Germany). This scale provide information about body mass index (BMI), percentage of body fat and percentage of body water.
- Waist circumference: by triplicate using a tape measure model Seca 201 (Seca, Hamburg, Germany). The volunteer was asked to stand and placed the tape measure around his/her middle, just above the hipbones. Measure was taken just after breathing out.
- (d)
- 24-h Dietary Recall: no prior notification was given to the subjects about whether or when they would be interviewed about their food intake. An ad hoc questionnaire was designed and previously checked and modified at the already explained pilot studies. The participant recalled the food intake for the past 24 h. Food quantities were assessed by using of household measures, food models, pictures, or the brands. The 24-h dietary recall was designed for further verification of the information collected at the Tablet, but also to make the participant more familiar with the type of information to be recorded during the three-day period.
- (e)
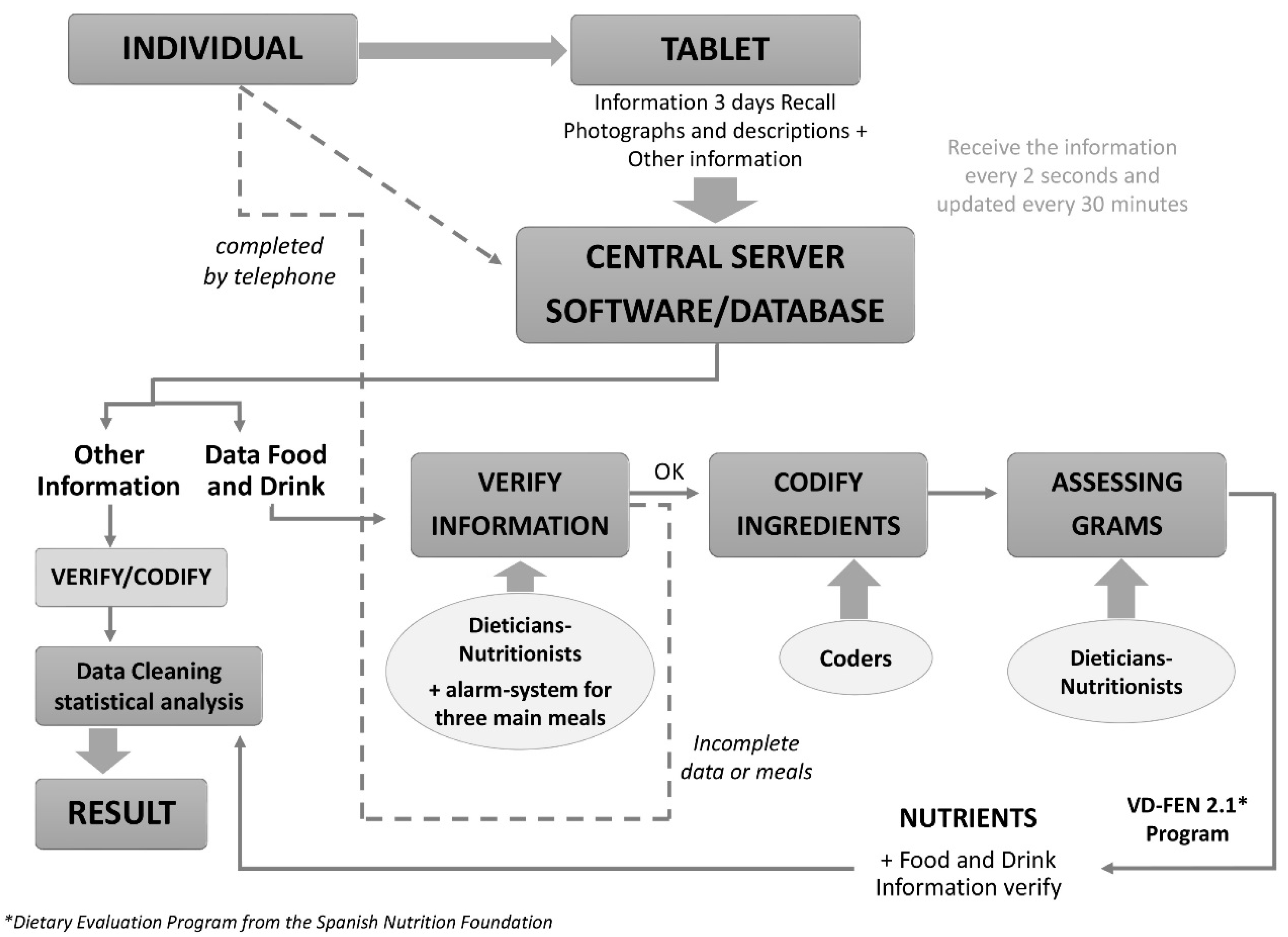
- Tablet device for collection of dietary data: the three-day food diary: All the participants were provided with a tablet device (Samsung Galaxy Tab27.0.) and instructed on how to record by taking pictures of all foods and beverages consumed, both at home and outside. Pictures had to be taken before and after finishing the meals. Additionally, a brief description of the meals, recipes, brands, etc. had to be also recorded with the device. The tablet was designed only to be used to collect information related to the ANIBES Study and no other uses were allowed.
- (f)
- If the participant declared or demonstrated that he/she was unable to use the tablet device, other possibilities were offered: photo camera plus paper or telephone interview.
- (g)
- At the end of the first visit, the date for the second interviewer visit was agreed, as well as the telephone calls to be made for check up at the end of the collection of the data.
- (h)
- Accelerometer device to quantify physical activity level: The physical activity measurements was obtained with an accelerometer ActiGraph (model GT3x y GT3x+; ActiGraph, Pensacola, FL, USA). This provided a measure of the frequency, intensity, and duration of physical activity and allowed classification of activity levels as sedentary, light, moderate and vigorous. Individuals were asked to wear the ActiGraph on a belt above the right hip, during three consecutive full days including its cycle of the three days food and beverages diary record by the tablet.
3. Results
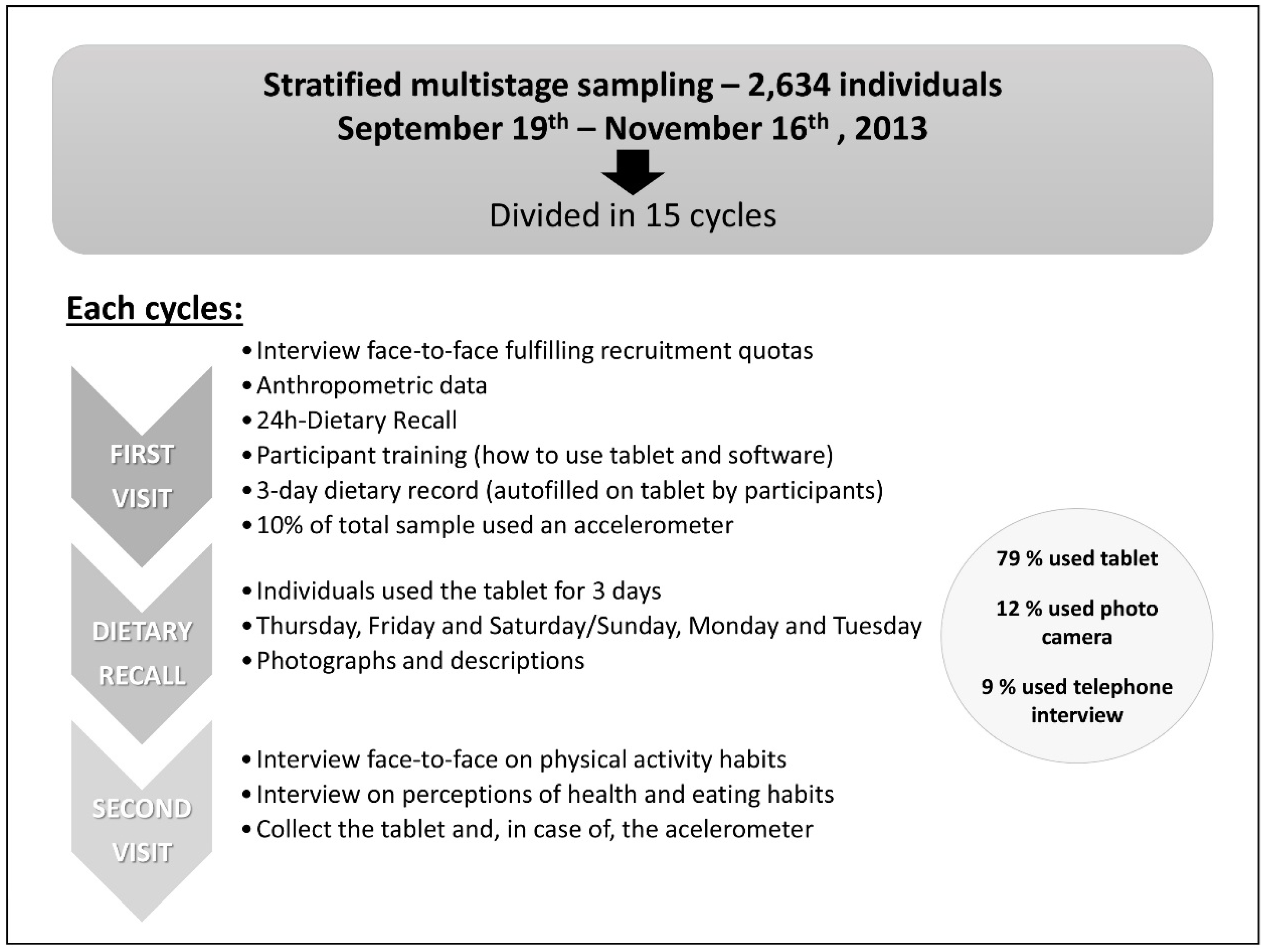
- Fieldwork dates: 19 September through 16 November 2013, structured in 15 different cycles/stages.
- 90 interviewers and 12 coordinators.
- Equipment:
- ○
- 426 Tablet devices
- ○
- 90 devices for anthropometric measurements (weighing scales, stadiometers, tape measures).
- ○
- 87 accelerometers.
- Percentages of users for the different devices to collect food and beverages information was:
- ○
- 79% of the sample used a Tablet
- ○
- 12% used photo camera
- ○
- 9% used telephone interview
3.1. Data Processing
| SAMPLE | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial Targeted Sample | Final Sample | Final Sample + Boost | |||||||||||
| Device | Device | Device | |||||||||||
| Base | Tablet | Photo Camera | Telephone | Base | Tablet | Camera | Telephone | Base | Tablet | Camera | Telephone | ||
| Sex | Base | 2634 | 2077 | 320 | 237 | 2009 | 1568 | 253 | 188 | 2285 | 1804 | 279 | 202 |
| 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | ||
| Men | 1309 | 1038 | 156 | 115 | 1013 | 800 | 124 | 89 | 1160 | 922 | 143 | 95 | |
| 50% | 50% | 49% | 49% | 50% | 51% | 49% | 47% | 51% | 51% | 51% | 47% | ||
| Women | 1325 | 1039 | 164 | 122 | 996 | 768 | 129 | 99 | 1125 | 882 | 136 | 107 | |
| 50% | 50% | 51% | 51% | 50% | 49% | 51% | 53% | 49% | 49% | 49% | 53% | ||
| Age (years) | Base | 2634 | 2077 | 320 | 237 | 2009 | 1568 | 253 | 188 | 2285 | 1804 | 279 | 202 |
| 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | ||
| Children 9–12 | 240 | 201 | 29 | 10 | 100 | 82 | 15 | 3 | 213 | 178 | 27 | 8 | |
| 9% | 10% | 9% | 4% | 5% | 5% | 6% | 2% | 9% | 10% | 10% | 4% | ||
| Adolescents 13–17 | 246 | 221 | 21 | 4 | 124 | 113 | 8 | 3 | 211 | 190 | 18 | 3 | |
| 9% | 11% | 7% | 2% | 6% | 7% | 3% | 2% | 9% | 11% | 6% | 1% | ||
| Adults 18–64 | 1911 | 1571 | 207 | 133 | 1588 | 1300 | 176 | 112 | 1655 | 1361 | 180 | 114 | |
| 73% | 76% | 65% | 56% | 79% | 83% | 70% | 60% | 72% | 75% | 65% | 56% | ||
| Elderly 65–75 | 237 | 84 | 63 | 90 | 197 | 73 | 54 | 70 | 206 | 75 | 54 | 77 | |
| 9% | 4% | 20% | 38% | 10% | 5% | 21% | 37% | 9% | 4% | 19% | 38% | ||

3.2. Quality Control
- (a)
- The same dietician-nutritionist was responsible for checking the food records included by the participant during the three-day dietary food record study.
- (b)
- The initial quality control was based on the photographs and descriptions sent by the participants, but also the brief description that was asked before/after each meal and/or intake. Special care was given to validate some variables such as ingredients, brands of the processed and ready-to-eat foods, portion size or culinary technique in order to obtain accurate information for further codification.
- (c)
- The final approval of the received information was given by a dietician-nutritionist and supervisor.
- ○
- Level 1–16 food and beverage groups;
- ○
- Level 2–29 food and beverage subgroups;
- ○
- Level 3–761 food and beverages entries;
- ○
- Company and brand;
- ○
- Culinary treatment;
- ○
- Household measure (tablespoons, glasses, cups, plates); typical/most used portion sizes and recipes from Spain; or conventional units/measures (e.g., 1 yogurt, 1 apple piece, half tomato, 1 slice of bread, 1 soda can, 1 biscuit, butter portion, etc.).
3.3. Data Cleaning
- -
- If a participant only had records from two or less days, he/she was considered as not valid and eliminated from the final sample.
- -
- If a participant was registered four or more days, valid data were for those three collected days corresponding to the specific cycle of the participant, but always under the same scheme: 2 working days + 1 weekend day.
- −
- Unexplained behavior in energy intake and large intra-individual variations between days were observed. When the known meal pattern of the participant was 3–5 intakes per day, but missing data was clearly observed in the register (i.e., only breakfast and/or one meal per day), he/she was removed from the final sample.
- −
- When extremely low energy intakes were recorded:
- ○
- Less than 500 kcal/day in two or three days of the period.
- ○
- Less than 500 kcal/day in one day, and <800 kcal/day in the remaining days.
- Having fulfilled previous data cleaning stages.
- Having completed successfully both visits during the fieldwork.
- If the participants had valid data on: weight, height, waist circumference.
4. Discussion
4.1. Dietary Assessment Methodologies
4.2. 24-h Dietary Recall
4.3. Dietary Record
4.4. Interview Options
4.5. Physical Activity
4.6. Anthropometry
5. Conclusions
- -
- The first dietary survey in Spain that looked specifically on the “energy balance” paradigm at the population level.
- -
- Included a representative age sample (9–75 years old) of the Spanish population.
- -
- The first study carried out in the same individuals which allow information collection on diet, physical activity, anthropometry and body composition.
- -
- Employed for the first time in Spain new technology to collect information on intake and physical activity (using tablet devices in nearly real time) to avoid the well known and common problems of under/over reporting.
- -
- The new ANIBES software (food and beverage database) allowed the most detailed information (not only by the usual food groups included in food composition tables) to be obtained, also for subgroups which are much more accurate and adjusted to the current “real” food market.
- -
- A precise quantification of physical activity was achievable nationwide (combined use of self-validated questionnaires plus objective accelerometers), to avoid the key problem of underreporting and to evaluate factors such as type, duration, amount, and intensity, which are rarely reported in population nutrition surveys.
Acknowledgments
Author Contributions
- Emma Ruiz-Moreno (E.R.M.) conceived the protocol, methodology to be employed, and designed the training procedures for interviewers and dieticians-nutritionists. ERM analyzed the data (collection, quality control), and also contributed to the general discussion.
- José Manuel Ávila (J.M.A.) conceived the overall design, protocol, and methodology. J.M.A. contributed to the interpretation and discussion of the results.
- Marcela González-Gross (M.G.G.) contributed to the design, protocol and methodology of the physical activity part. M.G.G. and Adrián Castillo (A.C.) were responsible of analysis of physical activity procedures, derived data and interpretation.
- Teresa Valero, Susana del Pozo, and Paula Rodriguez, were responsible for instruments to be used, training, and cleaning of the data.
- Javier Aranceta (J.A.), Ángel Gil (A.G.), Marcela González-Gross (M.G.G.), Rosa M. Ortega (R.M.O.), and Lluis Serra-Majem (L.S.M.), are members of the Scientific Advisory Board of the ANIBES Study. They were responsible for careful review of the protocol, design and methodology; J.A., A.G., M.G.G., R.M.O., and L.S.M. gave continuous scientific advice to the study, and for the interpretation of the results. They critically reviewed the manuscript.
- Gregorio Varela-Moreiras (G.V.M.), Principal Investigator, was responsible for design, protocol, methodology, and follow/check-up of the study. G.V.M. wrote the paper.
- All authors approved the final version of the manuscript.
Conflicts of Interest
References
- World Health Organization. The European Health Report 2009. Health and Health Systems; World Health Organization: Copenhagen, Denmark, 2009. [Google Scholar]
- World Health Organization (WHO) Regional Office for Europe. Action Plan for Implementation of the European Strategy for the Prevention and Control of Non-Communicable Diseases 2012–2016. World Health Organization: Copenhagen, Denmark, 2012. [Google Scholar]
- Elmadfa, I. European Nutrition and Health Report. Forum of Nutrition; Elmadfa, I., Ed.; Karger: Vienna, Austria, 2009; Volume 62. [Google Scholar]
- Varela-Moreiras, G.; Alguacil Merino, L.F.; Alonso Aperte, E.; Aranceta Bartrina, J.; Avila Torres, J.M.; Aznar Laín, S.; Belmonte Cortés, S.; Cabrerizo García, L.; dal Re Saavedra, M.Á.; Delgado Rubio, A.; et al. Obesity and sedentarism in the 21st century: What can be done and what must be done? Nutr. Hosp. 2013, 28, 1–12. [Google Scholar] [CrossRef]
- World Health Organization. Vienna Declaration on Nutrition and Noncommunicable Diseases in the Context of Health 2020. In WHO Ministerial Conference on Nutrition and Noncommunicable Diseases in the Context of Health 2020; World Health Organization: Vienna, Austria, 2013. [Google Scholar]
- Varela-Moreiras, G.; Ávila, J.M.; Cuadrado, C.; del Pozo, S.; Ruiz, E.; Moreiras, O. Evaluation of food consumption and dietary patterns in Spain by the Food Consumption Survey. Eur. J. Clin. Nutr. 2010, 64, S37–S43. [Google Scholar] [CrossRef] [PubMed]
- Varela-Moreiras, G. Libro Blanco de la Nutrición en España (White Book on Nutrition in Spain); Spanish Foundation on Nutrition/Spanish Agency on Food Safety and Nutrition (AESAN, MSSSI): Madrid, Spain, 2013. [Google Scholar]
- Bach-Faig, A.; Serra-Majem, L.; Carrasco, J.L.; Roman, B.; Ngo, J.; Bertomeu, I. The use of indexes evaluating the adherence to the Mediterranean diet in epidemiological studies: A review. Public. Health Nutr. 2006, 9, 132–146. [Google Scholar] [CrossRef] [PubMed]
- FAO. FAOSTAT-PC, Food Balance Sheets 1997. FAO: Rome, Italy, 1998. [Google Scholar]
- Moreno, L.A.; Sarria, A.; Popkin, B.M. The nutrition transition in Spain: A European Mediterranean country. Eur. J. Clin. Nutr. 2002, 56, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Fouskakis, D.; Oikonomou, E.; Almeida, M.D.V.; Berg, M.A.; Gedrich, K.; Moreiras, O.; Nelson, M.; Trygg, K.; Turrini, A.; et al. Dietary patterns and their socio-demographic determinants in 10 European countries: Data from the DAFNE databank. Eur. J. Clin. Nutr. 2006, 60, 181–190. [Google Scholar]
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-Analysis. BMJ 2008, 28, 337–344. [Google Scholar]
- Montoye, H.J.; Taylor, H.L. Measurement of physical activity in population studies: A review. Hum. Biol. 1984, 56, 195–216. [Google Scholar] [PubMed]
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- European Food Safety Authority (EFSA). General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar]
- Acheson, K.J.; Campbell, I.T.; Edholm, O.G.; Miller, D.S.; Stock, M.J. The measurement of food and energy intake in man-an evaluation of some techniques. Am. J. Clin. Nutr. 1980, 33, 1147–1154. [Google Scholar] [PubMed]
- Biró, G.; Hulshof, K.F.; Ovesen, L.; Amorim Cruz, J.A. Selection of methodology to assess food intake. Eur. J. Clin. Nutr. 2008, 56, 25–32. [Google Scholar]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [PubMed]
- Laporte, R.E.; Montoye, H.J.; Caspersen, C.J. Assessment of physical activity in epidemiologic research: Problems and prospects. Public Health Rep. 1985, 100, 131. [Google Scholar] [PubMed]
- Martin-Moreno, J.; Gorgojo, L. Valoración de la ingesta dietética a nivel poblacional. Mediante cuestionarios individuales: Sombras y luces metodológicas. Rev. Esp. Salud Pública 2007, 81, 507–518. [Google Scholar]
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostálová, J.; Dlouhý, P.; et al. European Nutrition and Health Report 2009. Ann. Nutr. Metab. 2009, 55, 1–40. [Google Scholar]
- Bingham, S.A. The dietary assessment of individuals: Methods, accuracy, new techniques and recommendations. Nutr. Abstr. Rev. 1987, 57, 705–742. [Google Scholar]
- Becker, W.; Foley, S.; Shelley, E.; Gibney, M. Energy under-reporting in Swedish and Irish dietary surveys: Implications for food-based dietary guidelines. Br. J. Nutr. 1999, 81, S127–S131. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E.; Cole, T.J. Biased over- or under-reporting is characteristic of individuals whether over time or by different assessment methods. J. Am. Diet. Assoc. 2001, 101, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, P.; Slimani, N.; Ciampi, A.; Trichopoulou, A.; Naska, A.; Lauria, C.; Veglia, F.; Riboli, E. Evaluation of under- and overreporting of energy intake in the 24-h diet recalls in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2002, 5, 1329–1345. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Solvoll, K.; Bjørneboe, G.E.A.; Drevon, C.A. Under- and overreporting of energy intake related to weight status and lifestyle in a nationwide sample. Am. J. Clin. Nutr. 1998, 68, 266–274. [Google Scholar] [PubMed]
- Stumbo, P.J. New technology in dietary assessment: A review of digital methods in improving food record accuracy. Proc. Nutr. Soc. 2013, 72, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Bosch, M.; Woo, I.; Kim, S.; Boushey, C.J.; Ebert, D.S.; Delp, E.J. The use of mobile devices in aiding dietary assessment and evaluation. IEEE J. Sel. Top. Signal Process. 2010, 4, 756–766. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Bosch, M.; Boushey, C.J.; Delp, E.J. An image analysis system for dietary assessment and evaluation. In Proceedings of the Image Processing (ICIP), 2010 17th IEEE International Conference, Hong Kong, China, 26–29 September 2010; pp. 1853–1856.
- Puri, M.; Zhu, Z.; Yu , Q.; Divakaran, A.; Sawhney, H. Recognition and Volume Estimation of Food Intake Using a Mobile Device. In Presented at the Applications of Computer Vision (WACV), 2009 Workshop, Utah, UT, USA, 7–8 December 2009.
- Nelson, M.; Atkinson, M.; Darbyshire, S. Food photography II: Use of food photographs for estimating portion size and the nutrient content of meals. Br. J. Nutr. 1966, 76, 31–49. [Google Scholar] [CrossRef]
- De Henauw, S.; Brants, H.A.; Becker, W. Operationalization of food consumption surveys in Europe: Recommendations from the European Food Consumption Survey Methods (EFCOSUM) Project. Eur. J. Clin. Nutr. 2002, 56, 75–88. [Google Scholar] [CrossRef]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy balance and obesity. Circulation 2012, 126, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Using the energy gap to address obesity: A commentary. J. Am. Diet. Assoc. 2009, 109, 1848–1854. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Wyatt, H.R. Role of physical activity in preventing and treating obesity. J. Appl. Phyisol. 2005, 99, 765–770. [Google Scholar]
- Varela, G.; García, D.; Moreiras-Varela, O. La Nutrición de los Españoles. Diagnóstico y Recomendaciones; Escuela Nacional de Administración Pública: Madrid, Spain, 1971. [Google Scholar]
- Varela, G.; Moreiras, O.; Carbajal, A.; Campo, M. Encuesta de Presupuestos Familiares 1990–1991; Spanish National Statistical Institute: Madrid, Spain, 1991; Volume I. [Google Scholar]
- Varela-Moreiras, G. La Dieta Mediterránea en la España actual. Nutr Hosp. 2014, 30 (Suppl. 2), 21–28. [Google Scholar]
- Varela, G.; Moreiras, O.; Carbajal, A.; Campo, M. Encuesta de Presupuestos Familiares 1990–91; Estudio Nacional de Nutrición y Alimentación 1991; INE: Madrid, Spain, 1995; Volume 1. [Google Scholar]
- Varela-Moreiras, G.; Ávila, J.M.; Cuadrado, C.; del Pozo, S.; Ruiz, E.; Moreiras, O. Valoración de la Dieta Española de Acuerdo al Panel de Consumo Alimentario; Ministerio de Medio Ambiente y Medio Rural y Marino/Fundación Española de la Nutrición: Madrid, Spain, 2008. [Google Scholar]
- Del Pozo, S.; García, V.; Cuadrado, C.; Ruiz, E.; Valero, T.; Ávila, J.M.; Varela-Moreiras, G. Valoración Nutricional de la Dieta Española de acuerdo al Panel de Consumo Alimentario; Fundación Española de la Nutrición (FEN): Madrid, Spain, 2012. [Google Scholar]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Encuesta Nacional de Ingesta Dietética Española 2011. Available online: http://www.aesan.msc.es/AESAN/docs/docs/notas_prensa/Presentacion_ENIDE.pdf (accessed on 2 October 2014).
- Serra-Majem, L.; Ribas Barba, L.; Aranceta-Bartrina, J.; Pérez-Rodrigo, C.; Saavedra Santana, P.; Peña- Quintana, L. Obesidad en la infancia y adolescencia en España. Resultados del estudio enKid (1998–2000). Med. Clin. 2003, 121, 725–732. [Google Scholar]
- González-Gross, M.; Castillo, M.J.; Moreno, L.; Nova, E.; Gonzalez-Lamuño, D.; Perez-Llamas, F.; Gutiérrez, A.; Garaulet, M.; Joyanes, M.; Leyva, A.; et al. Alimentación y Valoración del Estado Nutricional de los Adolescentes Españoles (Proyecto AVENA). Evaluación de riesgos y propuesta de intervención. I. Descripción metodológica del estudio. Nutr. Hosp. 2003, 18, 15–27. [Google Scholar]
- Aranceta, J.; Pérez, C.; Amela, C.; García, R. Encuesta de Nutrición de la Comunidad de Madrid. Documentos Técnicos de Salud Pública No. 18; Dirección General de Prevención y Promoción de la Salud; Comunidad de Madrid: Madrid, Spain, 1994. [Google Scholar]
- Ruiz, E.; del Pozo, S.; Cuadrado, C.; Valero, T.; Ávila, J.M.; Varela-Moreiras, G. Encuesta de Nutrición de la Comunidad de Madrid (ENUCAM). Documentos Técnicos de Salud Pública; Consejería de Sanidad de la Comunidad de Madrid: Madrid, Spain, 2014. [Google Scholar]
- Serra Majem, L.; Ribas Barba, L.; Salvador Castell, G.; Román Viñas, B.; Castell Abat, C.; Cabezas Peña , C.; Pastor Ferrer, M.C.; Raidó, B.; Ngo de la Cruz, N.; García Álvarez, A.; et al. Tendencias del estado nutricional de la población española: Resultados del sistema de monitorización nutricional de Cataluña (1992–2003). Rev. Esp. Salud Pública 2007, 81, 559–570. [Google Scholar]
- Vioque, J.; Quiles, J. Encuesta de Nutrición y Salud de la Comunidad Valenciana, 1994; Departamento de Salud Pública-Universidad Miguel Hernández: España, Alicante, 2003. [Google Scholar]
- Muñiz, J.; Pérez, T.; del Pozo, S.; Cuadrado, C.; Moreiras, O. Encuesta Sobre los Hábitos Alimentarios de la Población Adulta Gallega, 2007; Dirección Xeneral de Saúde Pública: Santiago de Compostela, Spain, 2008. [Google Scholar]
- Aranceta, J.; Pérez, C.; Marzana, I.; Eguileor, I.; González de Galdeano, L.; Saenz de Buruaga, J. Food consumption patterns in the Basque Country: The EINUT-I study. Public Health Nutr. 1998, 1, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales. Encuesta Nacional de Salud 2011–2012; Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales: Madrid, Spain, 2013. [Google Scholar]
- Livingstone, M.B.E.; Robson, P.J.; Wallace, J.M. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, 213–222. [Google Scholar] [CrossRef]
- Cuenca-García, M.; Ortega, F.B.; Ruiz, J.R.; González-Gross, M.; Labayen, I.; Jago, R.; Martínez-Gómez, D.; Dallongeville, J.; Bel-Serrat, S.; Marcos, A.; et al. HELENA study group. Combined influence of healthy diet and active lifestyle on cardiovascular disease risk factors in adolescents. Scand. J. Med. Sci. Sports 2012, 12. [Google Scholar] [CrossRef]
- Biro, G.; Hulshof, K.F.; Ovesen, L.; Amorim, C.J. Selection of methodology to assess food intake. Eur. J. Clin. Nutr. 2002, 56, S25–S32. [Google Scholar] [CrossRef] [PubMed]
- Hagstromer, M.; Bergman, P.; de Bourdeaudhuij, I.; Ortega, F.B.; Ruiz, J.R.; Manios, Y.; Rey-López, J.P.; Phillipp, K.; von Berlepsch, J.; Sjöstrom, M.; et al. Concurrent validity of a modified version of the International Physical Activity Questionnaire (IPAQ-A) in European adolescents: The HELENA Study. Int. J. Obes. 2008, 32, S42–S48. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar]
- Harris, J.A.; Benedict, F.G. A Biometric Study of Basal Metabolism in Man; Publication No. 279; Carnegie Institute of Washington: Washington, DC, USA, 1919. [Google Scholar]
- Freedson, P.; Pober, D.; Janz, K.F. Calibration of accelerometer output for children. Med. Sci. Sports Exerc. 2005, 37 (Suppl. 11), S523–S530. [Google Scholar] [CrossRef]
- Freedson, P.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Application, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 15ª ed.; Pirámide: Madrid, Spain, 2011. [Google Scholar]
- Kroes, R.; Muller, D.; Lambe, J.; Lowik, M.R.; van Klaveren, J.; Kleiner, J.; Massey, R.; Mayer, S.; Urieta , I.; Verger, P.; et al. Assessment of intake from the diet. Food Chem. Toxicol. 2002, 40, 327–385. [Google Scholar] [CrossRef]
- Hoffmann, K.; Boeing, H.; Dufour, A.; Volatier, J.L.; Telman, J.; Virtanen, M.; Becker, W.; de Henauw, S.; EFCOSUM Group. Estimating the distribution of usual dietary intake by short-term measurements. Eur. J. Clin. Nutr. 2002, 56, S53–S62. [Google Scholar]
- Leclercq, C.; Arcella, D.; Piccinelli, R.; Sette, S.; le Donne, C.; Turrini, A. On behalf of the INRAN SCAI 2005–06 study group. The Italian National Food Consumption Survey INRAN-SCAI 2005–06. Main results in terms of food consumption. Public Health Nutr. 2009, 12, 2504–2532. [Google Scholar]
- Voedingscentrum. Zoe et Nederland, Resultaten van de Voedselconsumptiepeiling 1997–1998. Voedingscentrum: Den Haag, The Netherlands, 1998. [Google Scholar]
- Pekkarinen, M. Methodology in the collection of food consumption data. World Rev. Nutr. Diet. 1970, 12, 145–171. [Google Scholar] [PubMed]
- Riboli, E.; Kaaks, R. The EPIC Project: Rationale and study design. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26, S6–S14. [Google Scholar]
- Van Staveren, W.A.; de Groot, L.C.; Blauw, Y.H.; van der Wielen, R.P. Assessing diets of elderly people: Problems and approaches. Am. J. Clin. Nutr. 1994, 59, 221–323. [Google Scholar]
- Thompson, F.E.; Subar, A.F. Dietary assessment methodology. In Nutrition in the Prevention and Treatment of Disease, 2nd ed.; Coulson, A., Boushey, C., Eds.; Elsevier: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Van Staveren, W.A.; Ocke, M.C. Dietary assessment. In ILSI, Present Knowledge in Nutrition, 9th ed.; Bowman, B.A., Russell, R.M., Eds.; ILSI: Washington, DC, USA, 2006. [Google Scholar]
- Slimani, N.; Deharveng, G.; Charrondiere, R.U.; van Kappel, A.L.; Ocke, M.C.; Welch, A.; Lagiou, A.; van Liere, M.; Agudo, A.; Pala, V.; et al. Structure of the standardized computerized 24-h diet recall interview used as reference method in the 22 centres participating in the EPIC project. Comput. Methods Progr. Biomed. 1999, 8, 251–256. [Google Scholar]
- Todd, K.S.; Hudes, M.; Calloway, D.H. Food intake measurement: Problems and approaches. Am. J. Clin. Nutr. 1983, 37, 139–146. [Google Scholar] [PubMed]
- Kohlmeier, L.; Mendez, M.; McDuffie, J.; Miller, M. Computer-assisted self-interviewing: A multimedia approach to dietary assessment. Am. J. Clin. Nutr. 1997, 65, 1275–1281. [Google Scholar]
- Beasley, J.M.; Davis, A.; Riley, W.T. Evaluation of a web-based, pictorial diet history questionnaire. Public Health Nutr. 2008, 12, 1–9. [Google Scholar]
- Foster, E.; Matthews, J.N.; Nelson, M.; Harris, J.M.; Mathers, J.C.; Adamson, A.J. Accuracy of estimates of food portion size using food photographs—The importance of using age-appropriate tools. Public Health Nutr. 2006, 9, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.; Haraldsdottir, J. Food photographs: Practical guidelines I. Design and analysis of studies to validate portion size estimates. Public Health Nutr. 1998, 1, 219–230. [Google Scholar]
- Livingstone, M.B.E.; Robson, P.J.; Black, A.E.; Coward, W.A.; Wallace, J.M.W.; McKinley, M.C.; Strain, J.J.; McKenna, P.G. An evaluation of the sensitivity and specificity of energy expenditure measured by heart rate and the Goldberg cut-off for energy intake: Basal metabolic rate for identifying mis-reporting of energy intake by adults and children: A retrospective analysis. Eur. J. Clin. Nutr. 2003, 57, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Gersovitz, M.; Madden, J.P.; Smiciklas-Wright, H. Validity of the 24-h. dietary recall and seven-day record for group comparisons. J. Am. Diet. Assoc. 1978, 73, 48–55. [Google Scholar]
- Bingham, S.A.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Sneyd, M.J.; Key, T.J.A.; Roe, L.; Day, N.E.; et al. Comparison of dietary assessment methods in nutritional epidemiology: Weighed records v. 24 h recalls, food-frequency questionnaires and estimated-diet records. Br. J. Nutr. 1994, 72, 619–643. [Google Scholar]
- Beaton, G.H.; Burema, J.; Ritenbaugh, C. Errors in the interpretation of dietary assessments. Am. J. Clin. Nutr. 1997, 65, 1100–1107. [Google Scholar]
- Casey, P.H.; Goolsby, S.L.; Lensing, S.Y.; Perloff, B.P.; Bogle, M.L. The use of telephone interview methodology to obtain 24-h dietary recalls. J. Am. Diet. Assoc. 1999, 99, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Brustad, M.; Skeie, G.; Braaten, T.; Slimani, N.; Lund, E. Comparison of telephone vs. face-to-face interviews in the assessment of dietary intake by the 24 h recall EPIC SOFT program-the Norwegian calibration study. Eur. J. Clin. Nutr. 2003, 57, 107–113. [Google Scholar]
- Bogle, M.; Stuff, J.; Davis, L.; Forrester, I.; Strickland, E.; Casey, P.H.; Ryan, D.; Champagne, C.; McGee, B.; Mellad, K.; et al. Validity of a telephone-administered 24-h dietary recall in telephone and non-telephone households in the rural Lower Mississippi Delta region. J. Am. Diet. Assoc. 2001, 101, 216–222. [Google Scholar]
- Bakker, I.; Twisk, J.W.; van Mechelen, W.; Mensink, G.B.; Kemper, H.C. Computerization of a dietary history interview in a running cohort; evaluation within the Amsterdam Growth and Health Longitudinal Study. Eur. J. Clin. Nutr. 2003, 57, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.L.; Murtaugh, M.A.; Schumacher, M.C.; Johnson, J.; Edwards, S.; Edwards, R.; Benson, J.; Tom-Orme, L.; Lanier, A.P. Development, implementation, and evaluation of a computerized self-administered diet history questionnaire for use in studies of American Indian and Alaskan native people. J. Am. Diet. Assoc. 2008, 108, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Probst, Y.C.; Faraji, S.; Batterham, M.; Steel, D.G.; Tapsell, L.C. Computerized dietary assessments compare well with interviewer administered diet histories for patients with type 2 diabetes mellitus in the primary healthcare setting. Patient Educ. Couns. 2008, 72, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Turconi, G.; Guarcello, M.; Berzolari, F.G.; Carolei, A.; Bazzano, R.; Roggi, C. An evaluation of a colour food photography atlas as a tool for quantifying food portion size in epidemiological dietary surveys. Eur. J. Clin. Nutr. 2005, 59, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Wolper, C.; Heshka, S.; Heymsfield, S.B. Measuring Food Intake: An Overview; Sage Publishing: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Guthrie, H.A. Selection and quantification of typical food portions by young adults. J. Am. Diet. Assoc. 1984, 84, 1440–1444. [Google Scholar] [PubMed]
- Chambers, I.V.E.; McGuire, B.; Godwin, S.L.; McDowell, M.; Vecchio, F.A. Quantifying portion sizes for selected snack foods and beverages in 24-h dietary recalls. Nutr. Res. 2000, 20, 315–326. [Google Scholar] [CrossRef]
- Frobisher, C.; Maxwell, S.M. The estimation of food portion sizes: A comparison between using descriptions of portion sizes and a photographic food atlas by children and adults. J. Hum. Nutr. Diet. 2003, 16, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Wrieden, W.L.; Momen, N.C. Workshop 3: Novel approaches for estimating portion sizes. Eur. J. Clin. Nutr. 2009, 63, 80–81. [Google Scholar] [CrossRef]
- Foster, E.; Adamson, A.J.; Anderson, A.S.; Barton, K.L.; Wrieden, W.L. Estimation of portion size in children’s dietary assessment: Lessons learnt. Eur. J. Clin. Nutr. 2009, 63, 45–49. [Google Scholar] [CrossRef]
- Moran, M.; Cauwenberg, J.V.; Hercky-Linnewiel, R.; Cerin, E.; Deforche, B.; Plaut, P. Understanding the relationships between the physical environment and physical activity in older adults: A systematic review of qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, J.R. Research Methods in Physical Activity; Human Kinetics: Leeds, UK, 2005. [Google Scholar]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry; WHO Technical Report Series 854; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Ferrari, P.; Friedenreich, C.; Matthews, C.E. The role of measurement error in estimating levels of physical activity. Am. J. Epidemiol. 2007, 166, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Couneya, K.S.; Neilson, H.K.; Matthews, C.E.; Willis, G.; Irwin, M.; Troiano, R.; Ballard-Barbash, R. Reliability and validity of the past year total physical activity questionnaire. Am. J. Epidemiol. 2006, 163, 959–970. [Google Scholar] [CrossRef] [PubMed]
- Wareham, N.J.; Jakes, R.W.; Rennie, K.L.; Mitchell, J.; Hennings, S.; Day, N.E. Validity and repeatability of the EPIC-Norfolk physical activity questionnaire. Int. J. Epidemiol. 2002, 31, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Conner Gorber, S.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct measures for assessing height, weight and body mass index: A systematic review. The international association for the study of obesity. Obes. Rev. 2007, 8, 307–326. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz, E.; Ávila, J.M.; Castillo, A.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Bartrina, J.A.; Gil, Á.; González-Gross, M.; Ortega, R.M.; et al. The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology. Nutrients 2015, 7, 970-998. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7020970
Ruiz E, Ávila JM, Castillo A, Valero T, Del Pozo S, Rodriguez P, Bartrina JA, Gil Á, González-Gross M, Ortega RM, et al. The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology. Nutrients. 2015; 7(2):970-998. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7020970
Chicago/Turabian StyleRuiz, Emma, José Manuel Ávila, Adrián Castillo, Teresa Valero, Susana Del Pozo, Paula Rodriguez, Javier Aranceta Bartrina, Ángel Gil, Marcela González-Gross, Rosa M. Ortega, and et al. 2015. "The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology" Nutrients 7, no. 2: 970-998. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7020970