1. Introduction
Soy protein-based infant formulas (SF) currently comprise about 13% of total infant formula use in the US [
1]. The indication for use of SF includes management of IgE-mediated cow’s milk protein allergy (CMPA), lactose malabsorption or sensitivity, galactosemia, acute diarrhea, and general gastrointestinal discomfort (gas, fussiness and spit-ups); and as a source of nutrition for infants of vegetarian families [
1,
2]. Despite these SF benefits, studies [
3,
4,
5,
6] have demonstrated a firmer stool consistency in infants fed SF compared to those fed milk-based formulas. Dietary ingredients capable of modulating stool consistency may potentially help improve gastrointestinal tolerance and acceptance of SF in infants.
Fructooligosaccharides (FOS) is a non-digestible carbohydrate found in several plant-based foods, including bananas. Oligosaccharides, including FOS and galactooligosaccharides (GOS) are generally considered to be prebiotics because they promote the growth of healthy and beneficial gut
Bifido and
Lactobacilli bacteria in the colon [
7]. Several clinical studies [
8,
9,
10,
11,
12,
13,
14,
15] have demonstrated that the supplementation of milk-protein based infant formulas (MF) and infant cereal formulas with FOS and or GOS yielded softer stool consistency compared to non-supplemented formulas. In contrast, there is no reported clinical evaluation of SF supplemented with FOS or GOS. Experts [
16] have recommended clinical evaluation of water balance in infants fed formulas with supplemental FOS or GOS as a measure of safety because of the propensity of the supplementation to produce watery stools. Therefore, the supplementation of SFs with FOS and subsequent clinical assessment of GI tolerance and water balance in infants might provide an opportunity to improve soft stool consistency and tolerance of SF. The supplementation of SF with GOS is not advisable so as to avoid the addition of lactose and galactose inherent to GOS ingredients, which are contraindicated in infants with galactosemia or lactose sensitivity.
Most currently available SF contains a minimal amount of sucrose to help enhance palatability, acceptability and compliance by infants in need of the formula. In addition, sucrose masks the beany taste and flavor to help reduce rejection by infants consuming soy-based formula for nutritional or medical purposes. Clinical evidence suggests that sucrose has positive calming and analgesic effects [
17,
18] on infants. However, it is unclear if sucrose affects GI or stool tolerance in infants.
Dietary carotenoids are lipid soluble compounds found in abundance in fruits and vegetables, and are suggested to be important in immune function, skin and eye health [
19,
20]. Carotenoids are higher in human milk compared to most infant formulas, and are believed to contribute to the various protection benefits attributed to the breastfed infants [
21,
22]. Clinical studies have reported a normal growth and tolerance [
23,
24] in term infants fed milk-based formulas supplemented with carotenoids. One of the studies [
23] has demonstrated comparable levels of plasma carotenoids in infants fed milk-based formulas supplemented with carotenoids similar to levels in those fed human milk (HM). However, clinical assessment of a soy-based infant formula with supplemental carotenoids is lacking.
In view of the above, the primary goal of this study was to assess the comparative GI tolerance in healthy term infants fed the two experimental soy-based powdered formulas versus a standard commercial control soy-based formula with history of safe use. The experimental formulas were supplemented with scFOS and mixed carotenoids (MC; beta-carotene, lutein and lycopene) while the control formula was not. One of the experimental soy formulas also contains sucrose versus none in the other experimental formula.
4. Discussion
The primary goal of the study was to assess GI tolerance to soy based infant formulas with supplemental scFOS using measures of stool tolerance in infants. To our knowledge, this study is the first reported clinical evaluation of a soy protein-based infant formula, supplemented with FOS. Clinical studies in infants and young children have suggested that foods with supplemental FOS modulate stool consistency. Moore
et al. [
8] demonstrated softer stools, increased stool frequencies; fewer complaints of hard stools or constipation, and good GI tolerance in infants consuming FOS supplemented baby cereals. Euler
et al. [
9] evaluated the effect of 1.5 and 3.0 g/L FOS supplementation of milk-based infant formulas in a randomized crossover study in normal infants for one week. The 3.0 g/L FOS supplementation resulted in more frequent and significantly softer stools compared to the control. Both levels of FOS supplementation were reported by the authors to be safe and well tolerated. Paineau
et al. [
14] compared milk-based formulas supplemented with 4.0 g/L scFOS
versus placebo supplemented with 4.0 g/L maltodextrins in healthy infants. They reported significantly higher change in bifido bacteria population in stools of infants fed the scFOS compared to the placebo group. Other investigators have conducted studies on milk-based infant formulas with combination of FOS and GOS in both term [
10] and preterm infants [
11]. The addition of GOS to milk-based infant formulas, fed alone [
12] or in combination with oligofructose at a 9:1 ratio [
13,
15], resulted in normal growth, stool softening, and beneficial effects on health and development of newborn infants.
In our current study, we did not see any effect of the supplemental scFOS at 2.5 g/L on stool softening as indicated by the absence of a significant difference in the MRSC among the 3 study formulas. It is quite possible that a higher level of scFOS supplementation maybe needed for the soy-based formulas to produce a softer stool consistency compared to the level required for the milk-based formulas. It is well known that soy-based formulas tend to produce firmer stools compared to milk-based formulas or HM [
3,
4,
5,
6]. This could be partly due to the higher levels of inherent fiber and raffinose and starchyose in soy protein isolate components of soy formulas and the need for a higher calcium fortification rate in soy formulas relative to milk-based formulas. A modest level of scFOS supplementation was used in this pilot study to avoid a possible excessive watery stools and water balance issues when a higher level of oligosaccharides is used in infant formulas as recommended against by Experts [
16].
The results of the current study indicated that the two experimental formulas were generally well tolerated and were favorably comparable to the established control formula. This is supported by the absence of significant differences (
p > 0.05) in many of the GI tolerance measures evaluated in this study. Nonetheless, there were some measures that slightly favored the experimental formulas
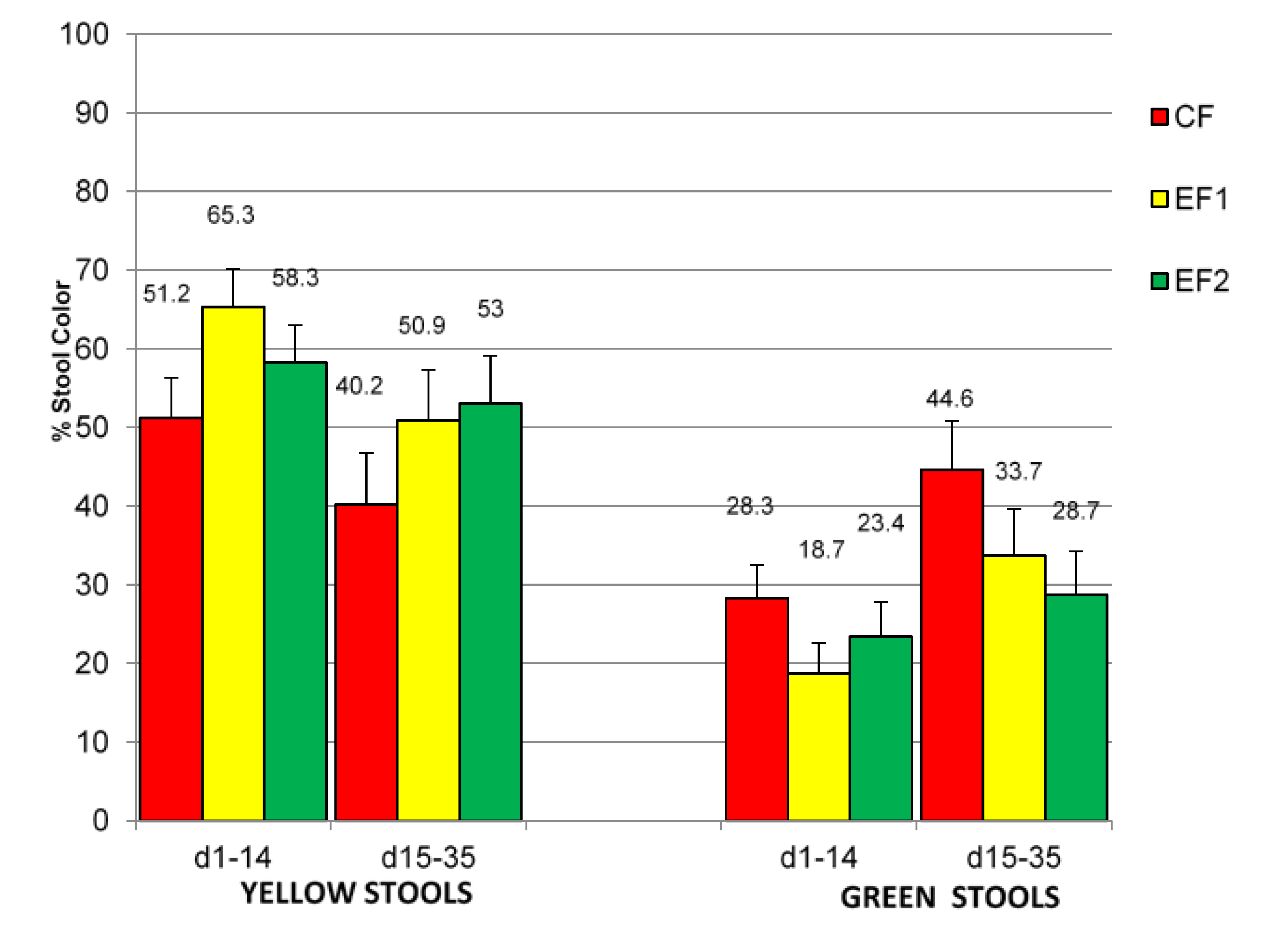
versus the control formula. The EF1 and EF2 groups produced significantly more yellowish stools
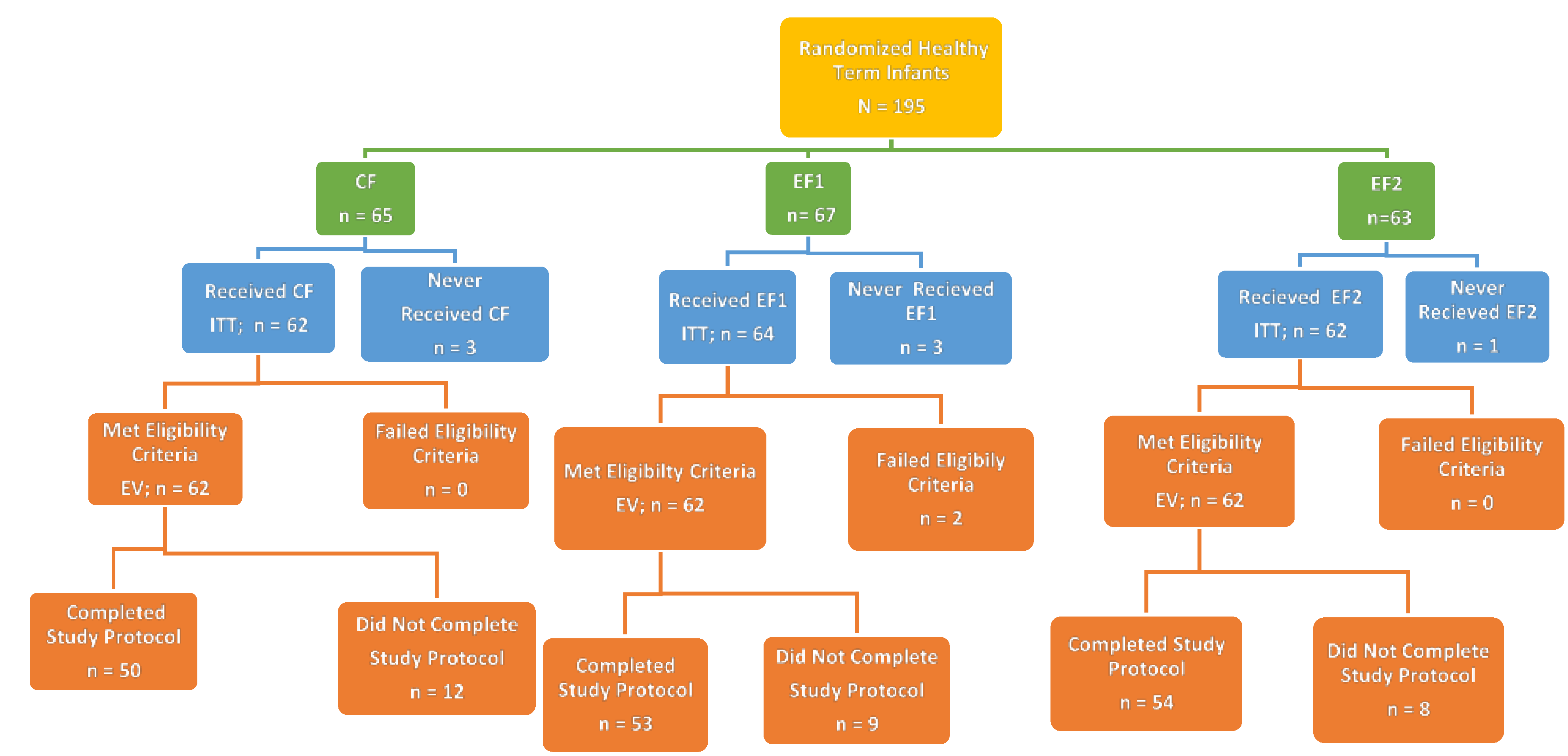
versus the CF group throughout the study; although statistically significant differences were noted only at d1–14 and not at d15–35 periods. The study period differences could be possibly due to adaptation with the progression in feeding and age of the infant subjects and the diminishing subjects’ sample size towards the end of study. The EV group had 142 subjects at d14, which was reduced to 120 subjects at d35. Notwithstanding, the yellowish stool trend was present and consistent throughout the study periods. The production of yellowish stools may be desirable for infant formula-fed infants, because stools produced by human milk-fed infants are predominantly yellowish compared to those produced by formula-fed infants [
4,
33]. Other studies which evaluated infant formulas supplemented with a combination of GOS and FOS [
15], and rice starch [
30] have similarly noted an increase in yellowish stools when compared to formulas that were not supplemented. The rationale for the production of yellowish stools is unclear. However, it is likely related to the prebiotic effects of oligossacharides on bifidogenic bacteria in the GI tract. Study completion rates were slightly better for EF1 and EF2 groups compared to the CF group despite a lack of statistically significant differences (CF, EF1 and EF2 were 81%, 86% and 87%, respectively).
There were no statistically significant differences between the study groups in the safety measures (AEs, SAEs, hydration status and physical examinations) assessed in this study. Despite the observed numerically higher (but no statistically significant differences) parental report of the occurrence of diarrhea in the EF1 group relative to the CF or EF2 group, the hydration status as denoted by the USG for the subjects with diarrhea were normal. The observation of a lower oral candidiasis infection in the EF1 group
versus EF2 and CF groups is interesting but its clinical relevance is unclear. It is unknown if this observed difference in infection rate is related to the higher vaginal births noted with subjects in the EF1
versus EF2 and CF groups. Nonetheless, this finding is consistent with studies [
34,
35] which have reported a higher risk of infection in infants who were born by caesarean compared to those born by vaginal routes.
Human milk and some infant formulas have introduced carotenoids into the infant diets. A recent study [
23] of milk-based formulas supplemented with similar levels of mixed carotenoid (MC) in our current study demonstrated comparable blood levels of lutein, lycopene and beta-carotene as in human milk-fed infants. The milk-based formulas supplemented with MC were well tolerated and supported normal growth. To our knowledge, our current study is the first study to report the supplementation of a soy-based infant formula with MC. The supplementation of EF1 and EF2 formulas with MC did not negatively impact GI tolerance.
An additional secondary interest of the current study was to evaluate the impact of sucrose inclusion in soy-based formula on formula tolerance in normal infants. Clinical evidence suggests that sucrose has positive calming and analgesic effects [
17,
18] on infants, especially infants with tolerance issues; however, it is unclear if sucrose affects stool patterns in infants. For the most part, in this study, tolerance responses were similar between the two experimental formulas, which only differ by having (EF1) or not having sucrose (EF2). The few differences observed between EF1 and EF2 included a significantly higher percentage of hard stools with EF1
versus EF2 at d14 but not at d35 of age, which suggests a possible transient effect; and a significantly more parental response favoring an “intent to continue to use study formula” for the EF2
versus EF1 group. In contrast, the parental questionnaire response indicated that the EF1 group was significantly less gassy compared to EF2 at only 14 days of age and not at 35 days of age. EF1 also had a slightly higher (non-statistically significant) percentage of yellowish stool color compared to EF2 group. Nonetheless, both formulas were well tolerated, using the CF formula as the standard comparator. The true impact of sucrose on GI tolerance in infants can best be evaluated in infants experiencing GI intolerance or colic symptoms. In our current study, we only enrolled normal infant subjects who were not having tolerance issues.
The strength of this current study includes being the first clinical study to assess the GI tolerance and short-term safety impact of soy protein-based infant formula supplemented with FOS in healthy term infants, and also the first clinical study to provide documented clinical GI tolerance feeding experience for soy protein-based infant formulas supplemented with MC. Among the weakness of the study are the absence of an assessment of varying levels of supplemental scFOS, which might potentially have a robust effect on GI tolerance; the absence of human milk and or milk protein-based formula group(s) to serve as a reference in the current study; the non-assessment of stool chemistry and probiotic colonization effects of the supplemental scFOS in the study; the shorter feeding duration of feeding in the study; and that the study did not address the efficacy of these types of formulas in infants experiencing tolerance issues. However, the intent of the current study was a pilot study in scope. These identified weaknesses are likely to be addressed by future studies.


{kind=link}
{kind=link}

